
Abstract
Purpose:
To test the hypothesis that fever was more frequent in critically ill patients with brain injury when compared to nonneurological patients and to study its effect on in-hospital case fatality.
Methods:
Retrospective matched cohort study utilizing a single-center prospectively compiled registry. Critically ill neurological patients ≥18 years and consecutively admitted to the intensive care unit (ICU) with acute ischemic stroke (AIS), intracerebral hemorrhage (ICH), and traumatic brain injury (TBI) were selected. Patients were matched by sex, age, and Acute Physiology and Chronic Health Evaluation II (APACHE-II) to a cohort of nonneurological patients. Fever was defined as any temperature ≥37.5°C within the first 24 hours upon admission to the ICU. The primary outcome measure was in-hospital case fatality.
Results:
Mean age among neurological patients was 65.6 ± 15 years, 46% were men, and median APACHE-II was 15 (interquartile range 11-20). There were 18% AIS, 27% ICH, and 6% TBI. More neurological patients experienced fever than nonneurological patients (59% vs 47%, P = .007). The mean hospital length of stay was higher for nonneurological patients (18 ± 20 vs 14 ± 15 days, P = .007), and more neurological patients were dead at hospital discharge (29% vs 20%, P < .0001). After risk factor adjustment, diagnosis (neurological vs nonneurological), and the probability of being exposed to fever (propensity score), the following variables were associated with higher in-hospital case fatality: APACHE-II, neurological diagnosis, mean arterial pressure, cardiovascular and respiratory dysfunction in ICU, and fever (odds ratio 1.9, 95% confidence interval 1.04-3.6, P = .04).
Conclusion:
These data suggest that fever is a frequent occurrence after brain injury, and that it is independently associated with in-hospital case fatality.
Introduction
Brain injuries from stroke and head trauma are leading causes of morbidity and mortality in the world. 1,2 Identification and implementation of strategies to optimize acute physiologic derangements are important goals for improving overall mortality and long-term clinical outcomes. To this end, recognition and advanced temperature modulation for the management of fever in the intensive care unit (ICU) are strategies used by critical care specialists to limit secondary neuronal injury in this patient population. 3,4
The adverse effects of fever after brain injury have been recognized in animal models 5,6 and observational studies. 7 –10 The chance for adverse functional outcome increases with exposure to fever after acute ischemic stroke (AIS), 11,12 intracerebral hemorrhage (ICH), 13 subarachnoid hemorrhage (SAH), 14,15 and traumatic brain injury (TBI). 9,10 Fever has been associated with increased ICU length of stay (LOS), hospital LOS, and overall case fatality in critically ill neurological patients, even after adjusting for other predictors of poor outcome. 16 In the most comprehensive meta-analysis of fever in patients with brain injury, a consistent association between fever and poor outcome was found, suggesting that fever is a potential therapeutic target in this patient population. 7 Although there is substantial animal and clinical data implicating fever as a predictor of poor outcome in brain injury, there is little observational data assessing the prevalence and risk factors for this phenomenon and its effect on outcome as compared to other critically ill nonneurological patients in whom fever, as part of the systemic inflammatory response syndrome (SIRS), is also prevalent.
Overall, the primary aim of this analysis was to determine the occurrence of fever within 24 hours of admission to the ICU in a cohort of patients with brain injury when compared to a matched cohort of critically ill nonneurological patients. Specifically, we sought to determine: (1) to determine whether fever was a common occurrence after brain injury when compared to nonneurological patients with similar critical-illness severity; (2) to determine whether the presence of fever was associated with lower survival at hospital discharge; (3) to determine whether the exposure to early fever remained significantly associated with in-hospital case fatality after adjustment for confounding variables in a multivariate analysis; and (4) to identify independent predictors of fever in the setting of critical illness. We hypothesized that fever, upon admission to the ICU, would be more frequent in critically ill neurological patients and associated with lower survival rate at hospital discharge when compared to a matched cohort of nonneurological patients.
Materials and Methods
Study Design and Patient Population
Our study was a retrospective matched cohort study. Patients older than 18 years and consecutively admitted to the ICU within 24 hours of brain injury from January 1, 2003, to December 31, 2008, with AIS, ICH, and TBI were selected. These patients were individually matched by sex, age (±2 year), and disease severity using the Acute Physiology and Chronic Health Evaluation II (APACHE-II) score (±5 points) to a cohort of nonneurological patients, which included medical (nonoperative) and surgical (emergent or elective postsurgical) patients that were also consecutively admitted to the ICU within 24 hours of onset of critical illness. All patients were treated according to the local ICU protocols. A description of our ICU setting has been described elsewhere. 17 This study was approved and in accordance with local institutional review board regulations (Cooper University Hospital).
Definition of Patient Variables and Outcome
The following variables were recorded for all patients admitted to our ICU during the study period: demographic variables, clinical variables (within 24 hours), comprehensive serum chemistries and blood work, indices of disease severity: the Glasgow Coma Scale (GCS) and APACHE-II score, admission do not resuscitate (DNR) status, emergency department (ED) boarder status,
18
cardiopulmonary resuscitation before admission, and admission and hospital discharge status (alive independent, alive partially dependent, alive fully dependent, or dead). To assess for the effect of medical complications, we collected data on the following acute organ dysfunctions in the ICU: cardiovascular (systolic blood pressure [SBP] <90 mm Hg, or mean arterial pressure (MAP) <60 mm Hg, or vasopressor requirement to keep SBP >90 mm Hg or MAP >60 mm Hg, and duration >1 hour), metabolic (lactic acidosis >2.0 mmol/dL), respiratory (acute lung injury Pa
Definition of Temperature Variables
The exposure variable was temperature. For the purpose of this analysis, Tmax was defined as the highest temperature within the first 24 hours of admission to ICU. Fever was defined as any Tmax > 37.5°C, and normothermia defined as patients not classified as fever. These cutoffs were defined a priori by consensus and conform to published results from clinical observations 13,19,20 and practice guidelines. 21
Statistical Analysis
Continuous data are presented as means and standard deviations or medians and interquartile ranges (IQRs) as appropriate based on the distribution of the data. We used the Shapiro-Wilk test to determine whether variables were normally distributed. Categorical data are reported as number of patients and proportions. The initial univariate analysis was performed with the t test for means or the Mann-Whitney U test for nonnormally distributed data and chi-square or Fisher exact tests for proportions. In addition, to determine the differences in admission physiologic variables within diagnostic groups (nonneurological vs AIS, ICH, or TBI), the analysis of variance was performed and the Tukey-Kramer honestly significant difference post hoc test was used to determine the differences within means (Table 1). For days to primary outcome (in-hospital case fatality) analysis, Kaplan-Meier survival estimates and log-rank tests were used to compare the fever and normothermia groups within neurological and nonneurological patients.
Components of Systemic Inflammatory Response Syndrome and Lowest MAP Within 24 Hours Based on ICU Admission Diagnosis.
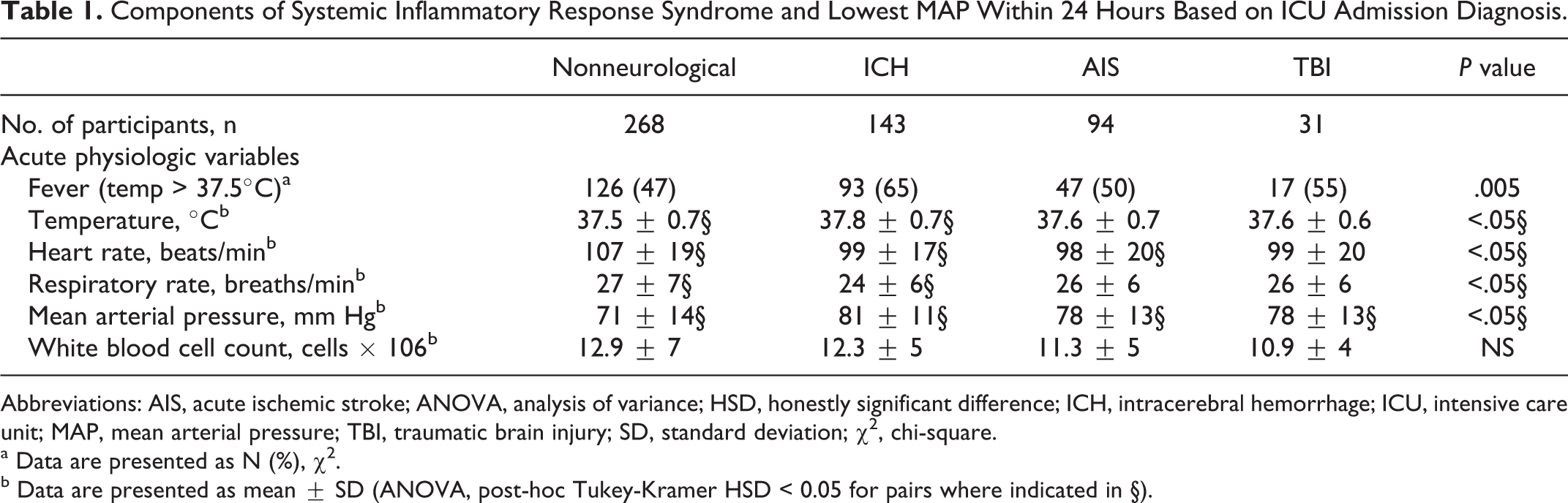
Abbreviations: AIS, acute ischemic stroke; ANOVA, analysis of variance; HSD, honestly significant difference; ICH, intracerebral hemorrhage; ICU, intensive care unit; MAP, mean arterial pressure; TBI, traumatic brain injury; SD, standard deviation; χ 2 , chi-square.
a Data are presented as N (%), χ 2 .
b Data are presented as mean ± SD (ANOVA, post-hoc Tukey-Kramer HSD < 0.05 for pairs where indicated in §).
Multivariable analysis of predictors of in-hospital case fatality was performed by means of a logistic regression and included matching variables to limit the introduction of bias in the results. 22 Significant risk factors were identified from the candidate variables with P value <.2 at the univariable level or from those believed to be clinically relevant. All variables in Tables 2 and 3 were considered potential candidates. In all multivariable analyses, all factors of interest were included, and parsimonious models were found by systematically removing the least significant factor and recalculating the model. To explore the possibility of an effect modification in our data, interaction terms were defined a priori and tested for in the multivariable model. Interaction terms between the exposure variable of interest (fever) and the following variables were included in the models, diagnosis (neurological vs nonneurological), age, gender, and APACHE-II. Finally, in a separate multivariable logistic regression analysis, we evaluated the predictors of fever upon admission to the ICU. We then calculated each individual’s probability of being exposed to fever (propensity score). To test whether fever exposure remained a significant independent predictor of in-hospital case fatality, when the propensity of individuals to be exposed to fever was adjusted for, a sensitivity analysis was performed using the propensity scores and adding the result into the final multivariate model. 23 Statistical analyses were conducted using JMP for Macintosh Version 8.0.2 (SAS Institute, Cary, North Carolina), and significance was set at P < .05. Our reporting of observational data conforms with Strengthening the Reporting of Observational Studies in Epidemiology STROBE guidelines. 24
Baseline Characteristics of Study Population Within First 24 Hours of Hospitalization.a
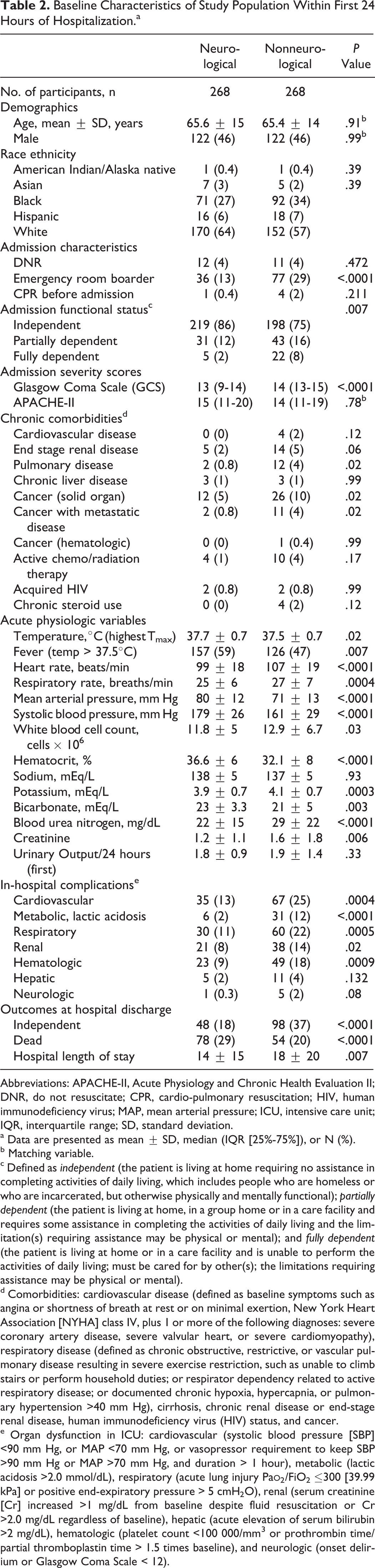
Abbreviations: APACHE-II, Acute Physiology and Chronic Health Evaluation II; DNR, do not resuscitate; CPR, cardio-pulmonary resuscitation; HIV, human immunodeficiency virus; MAP, mean arterial pressure; ICU, intensive care unit; IQR, interquartile range; SD, standard deviation.
a Data are presented as mean ± SD, median (IQR [25%-75%]), or N (%).
b Matching variable.
c Defined as independent (the patient is living at home requiring no assistance in completing activities of daily living, which includes people who are homeless or who are incarcerated, but otherwise physically and mentally functional); partially dependent (the patient is living at home, in a group home or in a care facility and requires some assistance in completing the activities of daily living and the limitation(s) requiring assistance may be physical or mental); and fully dependent (the patient is living at home or in a care facility and is unable to perform the activities of daily living; must be cared for by other(s); the limitations requiring assistance may be physical or mental).
d Comorbidities: cardiovascular disease (defined as baseline symptoms such as angina or shortness of breath at rest or on minimal exertion, New York Heart Association [NYHA] class IV, plus 1 or more of the following diagnoses: severe coronary artery disease, severe valvular heart, or severe cardiomyopathy), respiratory disease (defined as chronic obstructive, restrictive, or vascular pulmonary disease resulting in severe exercise restriction, such as unable to climb stairs or perform household duties; or respirator dependency related to active respiratory disease; or documented chronic hypoxia, hypercapnia, or pulmonary hypertension >40 mm Hg), cirrhosis, chronic renal disease or end-stage renal disease, human immunodeficiency virus (HIV) status, and cancer.
e Organ dysfunction in ICU: cardiovascular (systolic blood pressure [SBP] <90 mm Hg, or MAP <70 mm Hg, or vasopressor requirement to keep SBP >90 mm Hg or MAP >70 mm Hg, and duration > 1 hour), metabolic (lactic acidosis >2.0 mmol/dL), respiratory (acute lung injury Pa
Univariate Predictors of Case Fatality.a
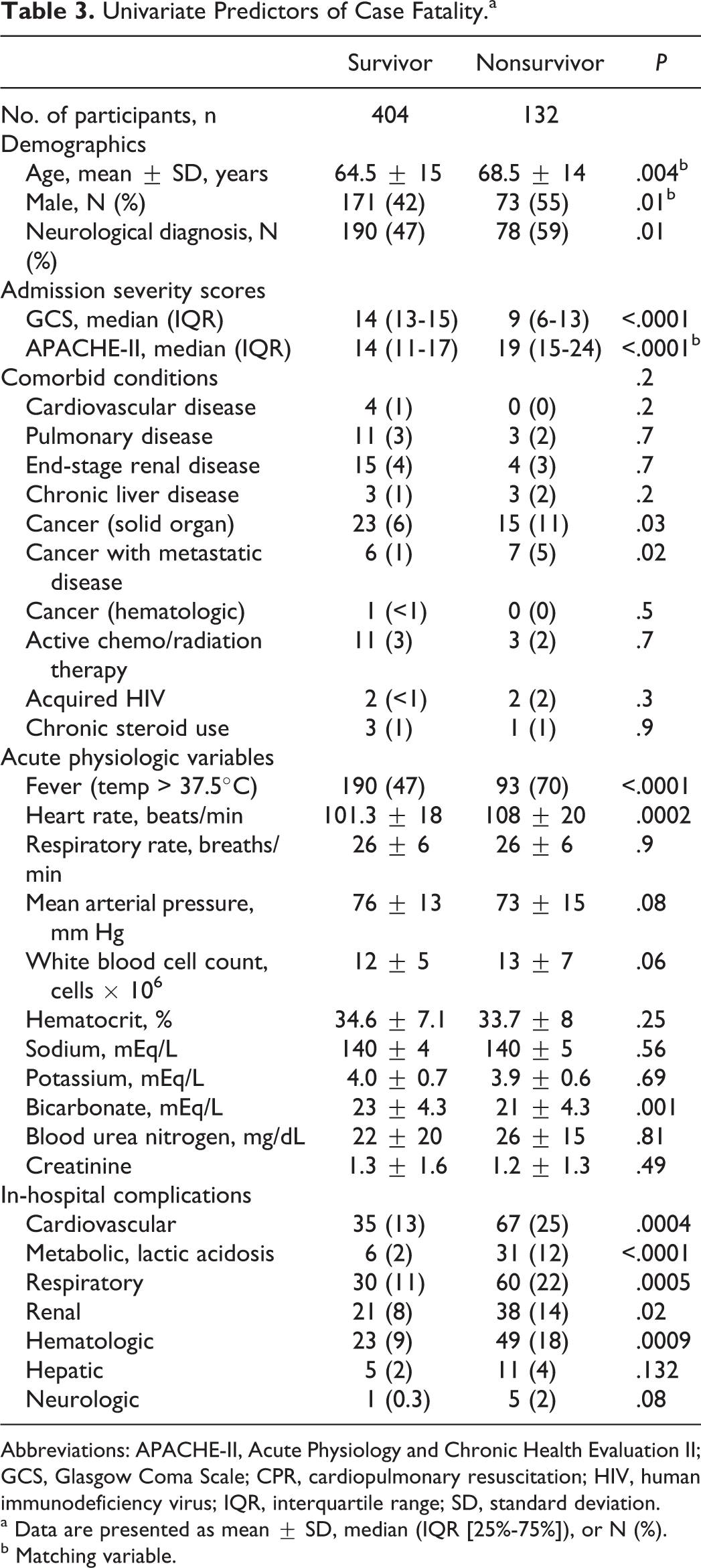
Abbreviations: APACHE-II, Acute Physiology and Chronic Health Evaluation II; GCS, Glasgow Coma Scale; CPR, cardiopulmonary resuscitation; HIV, human immunodeficiency virus; IQR, interquartile range; SD, standard deviation.
a Data are presented as mean ± SD, median (IQR [25%-75%]), or N (%).
b Matching variable.
Results
Over the 5-year period, 296 patients met the inclusion criteria. Of this group, only 268 patients had complete data suitable for analysis. These patients were subsequently matched to 268 nonneurological patients. Mean age was 65.6 ± 15 years, 46% were men, and median APACHE-II score was 15 (IQR 11-20). Within neurological group, there were 53% ICH, 35% AIS, and 12% TBI. Patients were predominantly of white race and were living independently prior to hospital admission. Within nonneurological group, 95% were medical (primarily sepsis, diabetic ketoacidosis, or coronary patients), 3% were emergency postsurgical cases, and 2% were elective surgical cases. Comorbid conditions were seen more commonly in nonneurological patients, and the most frequent comorbidity was cancer. More nonneurological patients remained in ED in boarder status. Acute physiologic data and additional baseline characteristics are shown in Table 2.
In-hospital complications were more frequent in nonneurological patients, with cardiovascular complications being more prevalent and followed by respiratory, hematological, and renal. The case fatality at hospital discharge was higher in neurological patients, and more nonneurological patients were independent at discharge (Table 2).
On Kaplan-Meier analysis, the survival fractions for the fever group and normothermia groups diverged significantly over time in neurological patients (log-rank P = .0002) but not on nonneurological patients (log-rank P = NS; Figure 1). The mean hospital LOS was higher for nonneurological patients (Table 2).
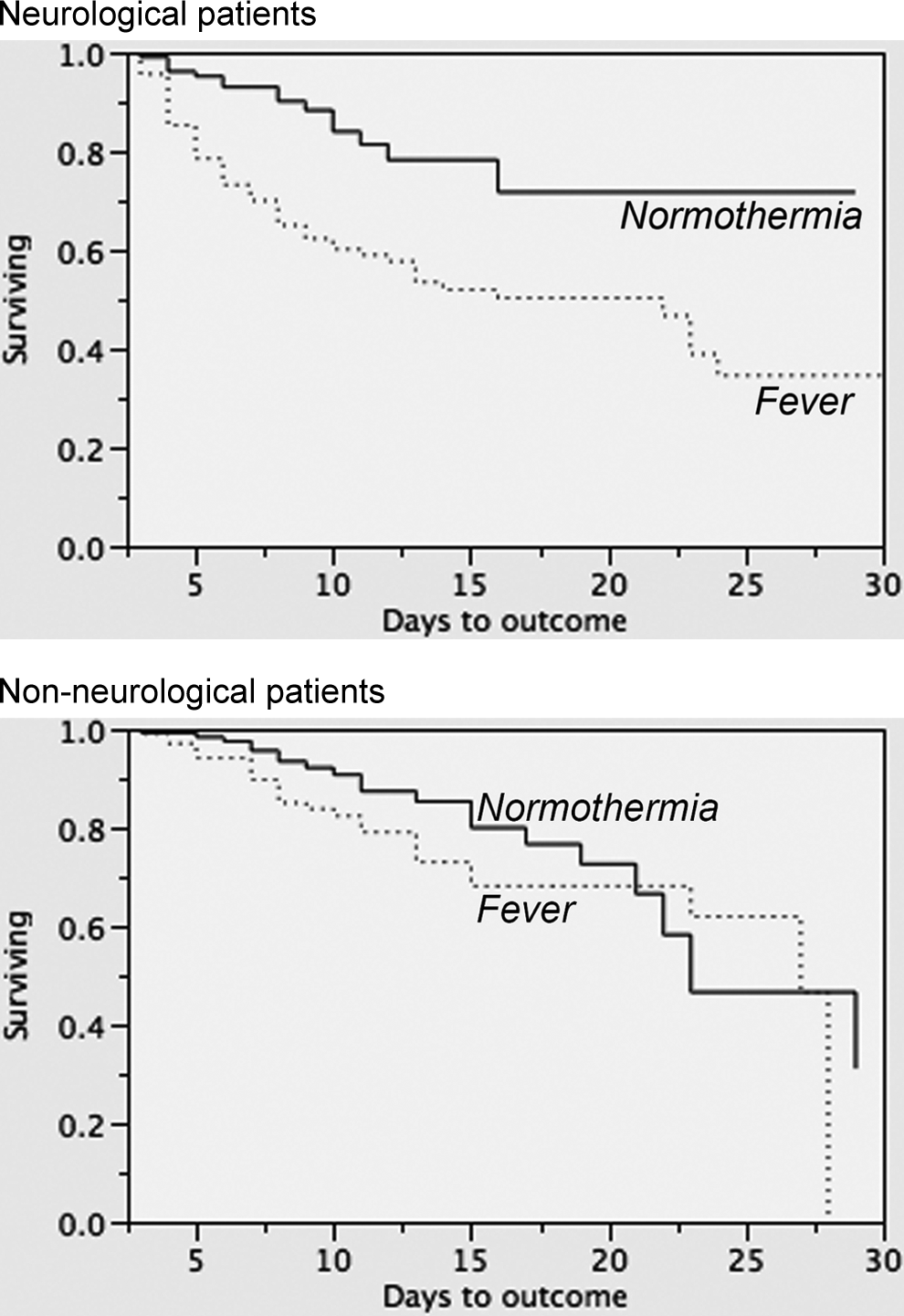
Kaplan-Meier analysis of 30-day mortality between fever and normothermia in neurological (log-rank < .0001) and nonneurological patients (log-rank = NS).
The mean Tmax for critically ill neurological patients was higher when compared to nonneurological patients, and more critically ill neurological patients experienced fever upon admission to the ICU than nonneurological patients (Table 2). Although neurological patients were more febrile on admission to the ICU, Tmax varied among subgroups being higher in ICH than in AIS and TBI and significantly different from nonneurological patients (Table 1). Overall, fever was more frequent after ICH followed by TBI, AIS, and nonneurological patients (Table 1).
In the initial univariate analysis, fever upon admission to the ICU conferred a higher risk of in-hospital case fatality (unadjusted odds ratio [OR] 2.6, 95% confidence interval (CI) 1.8-4.1, P < .0001). Additional variables associated with case fatality at the univariate level are presented in Table 3. In the multivariable analysis, APACHE-II, neurological diagnosis, MAP, cardiovascular and respiratory dysfunction, and fever were associated with increased odds of in-hospital case fatality (Table 4). We did not observe significant interactions in the variables retained in the model.
Multivariable Analysis of Predictors of In-Hospital Case Fatality.
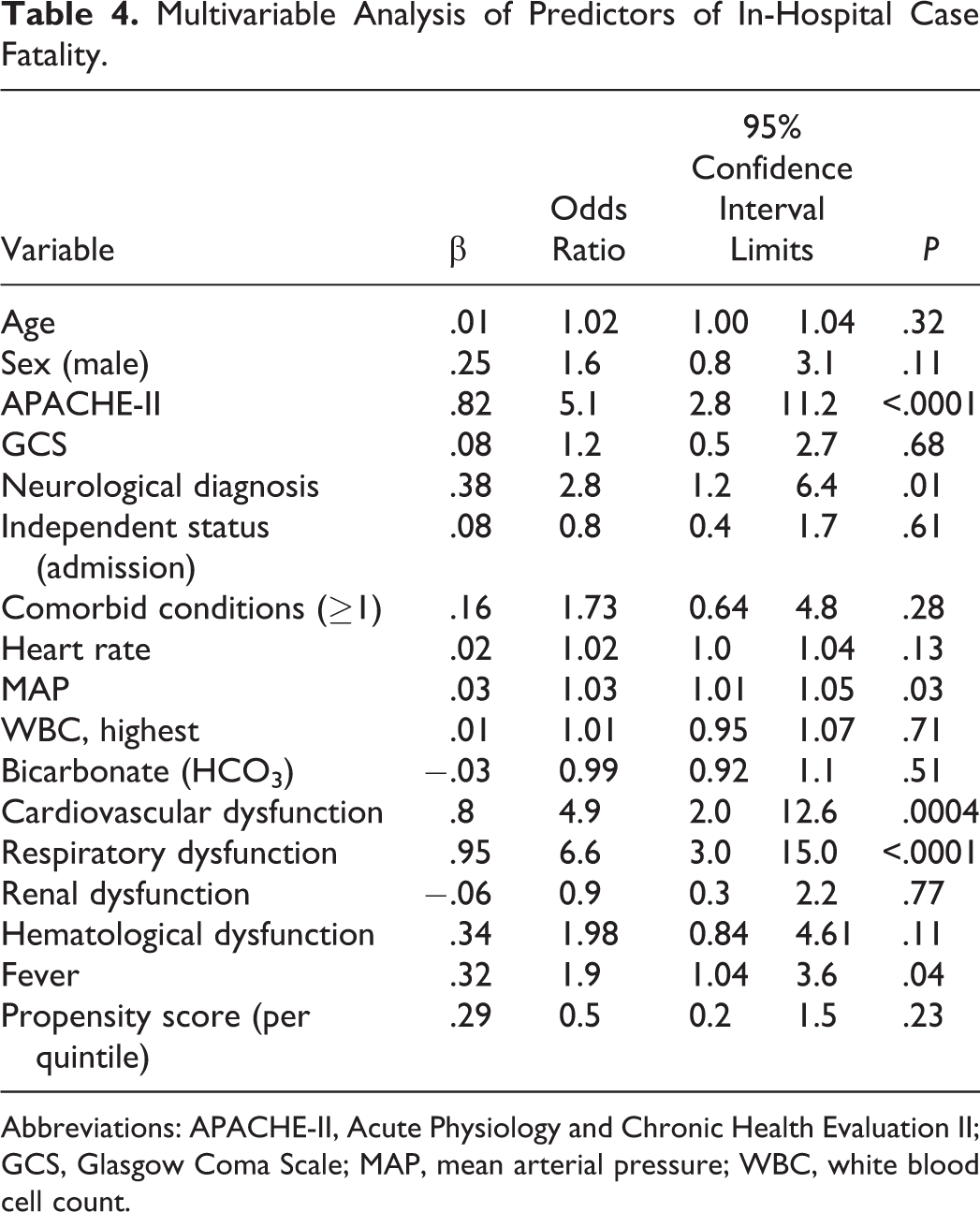
Abbreviations: APACHE-II, Acute Physiology and Chronic Health Evaluation II; GCS, Glasgow Coma Scale; MAP, mean arterial pressure; WBC, white blood cell count.
Finally, we performed a sensitivity analysis to test whether fever remained a significant independent predictor of in-hospital case fatality when adjusted for a propensity score (ie, probability of fever exposure). We calculated each patient’s probability of fever exposure by fitting a logistic regression with fever as the dependent variable. Independent predictors of fever upon admission to the ICU were younger age, heart rate, respiratory rate, and neurological diagnosis (Table 5). The probabilities, expressed in quintiles, were included in the final logistic regression model (Table 4). In the absence of the calculated propensity score, the odds for in-hospital case fatality related to fever did not change significantly (OR 1.8, 95% CI 1.01-3.5, P = .04).
Multivariate Analysis of Predictors of Fever Upon Admission to the ICU.
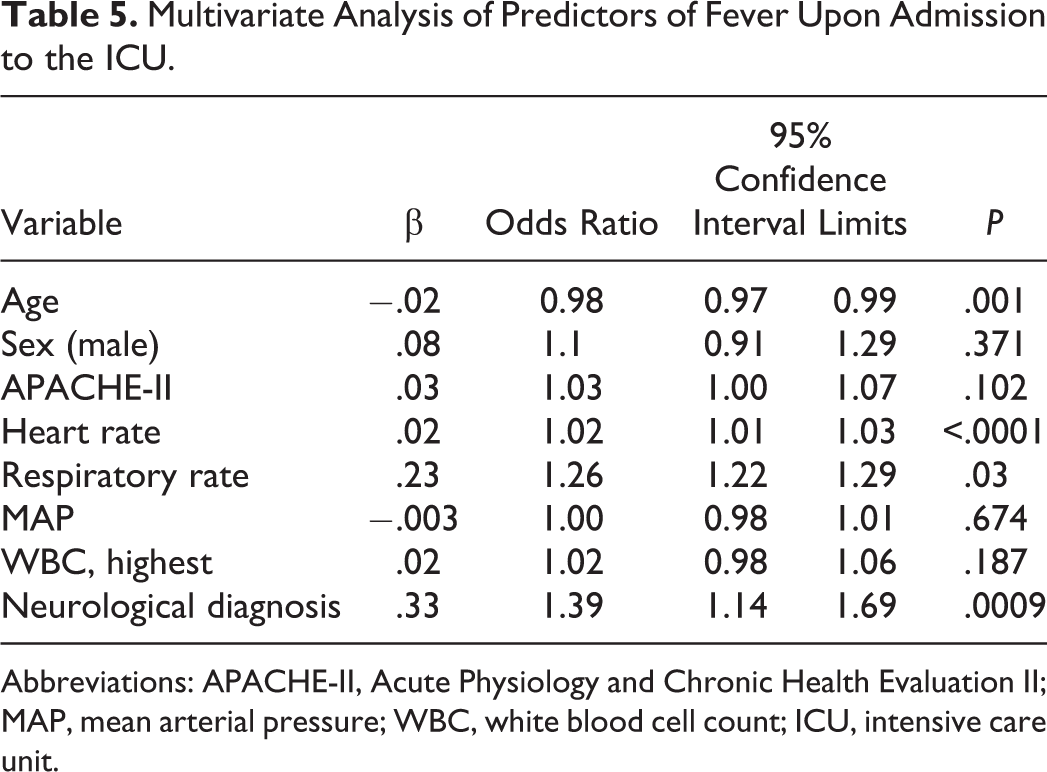
Abbreviations: APACHE-II, Acute Physiology and Chronic Health Evaluation II; MAP, mean arterial pressure; WBC, white blood cell count; ICU, intensive care unit.
Discussion
In this study, we demonstrated that fever upon admission to the ICU was a common occurrence in patients with brain injury when compared to matched nonneurological patients with similar severity of illness. Fever was associated with lower survival rates at hospital discharge. Most importantly, the effect of fever on in-hospital case fatality was only significant in critically ill neurological patients, and this effect remained after adjustment for additional predictors of hospital case fatality including prior comorbidities, acute physiologic derangements, critical illness severity score, in-hospital complications, and the probability of being exposed to fever. We did not observe a significant effect of admission DNR status, ED boarder status, or prior to admission cardiopulmonary resuscitation on in-hospital case fatality. 18,25,26 We acknowledge that although association does not necessarily imply causation, these data support our hypothesis that fever upon admission to the ICU is also associated with poor outcome.
Fever is a common response following trauma and critical illness, and this phenomenon has been attributed to a systemic response to the initial event or a defensive reaction to protect the body from ensuing infections. 27 In our study, neurological patients had higher temperatures and slightly higher proportion of fever on admission than nonneurological patients. This phenomenon was independent of age, gender, APACHE-II score, and elements of SIRS, suggesting that the occurrence of fever may be an independent event in neurological patients and not just a phenomenological occurrence in the setting of critical illness. In our study, the presence of neurological injury increased the odds of fever when compared to nonneurological patients with similar disease severity. This finding is in agreement with prior studies in critically ill neurological patients and suggests that brain injury, independent of etiology, is an important risk factor for the development of fever. 28
Numerous studies in patients with brain injury have shown that fever within 24 hours and sustained fever after admission are associated with poor neurological outcomes. 7,8,11,13 –16,20,29 –35 Fever increases the metabolism of the brain and exacerbates neuronal injury by several physiopathologic mechanisms, excitotoxicity amino acid and free radical production, blood–brain barrier breakdown, cytoskeletal proteolysis, and inhibition of protein kinases, acting as an important factor causing secondary brain injury. 35 According to different studies, the effect of fever persists even after controlling for other predictors of poor outcome, and this effect applies to both infectious and noninfectious causes. 8,14,15,36 Most of the data on fever and neurological outcome are derived from the AIS population, 7,8,11,30,31,34 but there are data suggesting that the effects of fever are also important after ICH, 13,20 SAH, 14,15 TBI, 9,10 and cardiac arrest. 32
Our study also demonstrates no effect of fever on case fatality in the nonneurological group, providing further support to the notion that fever may confer a biological benefit when the brain is intact, but once it is primarily injured, any protective benefits of fever may be outweighed by a “presumed” vulnerability of the brain to further damage by higher systemic temperatures. 37,38 We acknowledge that the approach to targeted temperature modulation may be different in subgroups of critically ill neurological patients based on different physiopathologic mechanisms. However, until convincing results from prospective randomized suggest otherwise, it may be prudent to attempt achieving normothermia in these patient population. Currently, American Heart Association (AHA) guidelines, the Brain Trauma Foundation (BTF) guidelines, and the results of some studies advocate for the achievement of normothermia, particularly after AIS and some sort of fever control in patients with AIS, ICH, SAH, or TBI. 39 –42
The strengths of our study are related to the methodology used to test our hypothesis and our sensitivity analysis to investigate our internal validity. However, our study has limitations. First, our analysis was observational in nature, which limits the inferences that can be made about etiological or causal relationships. Second, the inherent nature of the database used to perform our analysis, which was not originally designed to collect other end points commonly used in neurological outcome research such as the National Institutes of Health Stroke Scales (NIHSS), ICH scores, radiological variables (volumes, presence of intraventricular hemorrhage, contusions, hydrocephalus, etc), surrogates of brain damage such as pupillary abnormalities, and long-term functional outcomes; therefore, identification of associations or interactions within those variables could not be substantiated, suggesting the possibility of some unmeasured confounding that may have influenced the association between fever and case fatality. Third, we acknowledge our modest sample size and that we were underpowered to detect meaningful differences in the effects of fever and our proposed outcome among different subgroups of critically ill neurological patients. However, we did not detect an interaction between fever and neurological diagnosis in our data. Fourth, based on the nature of our database, we were unable to determine the effect of additional abnormal temperature elevation beyond 24 hours (fever burden), and its effect on our prespecified outcomes. However, our data analysis is robust and indicates that the effect of fever could be significant as early as 24 hours. Finally, whether our results are generalizable to other hospital settings can always be argued as a potential limitation based on the single-academic center setting of our study. To this end, our results may not be generalizable to other settings, where patients’ characteristics, management strategies and outcomes may differ substantively. However, our study provides important information about the effects of early fever after acute brain injury in comparison to nonneurological patients.
In summary, these data suggest that fever upon admission to the ICU is a frequent occurrence after brain injury and that it is independently associated with in-hospital case fatality. Future research is needed to determine whether maintenance of normothermia by an early targeted temperature management protocol would improve in-hospital case fatality after brain injury.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Rincon has received salary support from the American Heart Association (AHA 12CRP12050342).