
Abstract
Introduction:
Sedation with dexmedetomidine may facilitate ventilator liberation and limit the occurrence of delirium. No trial has assessed patient recall or the development of psychological outcomes after dexmedetomidine sedation. This pilot study evaluated whether transitioning benzodiazepine sedation to dexmedetomidine alters patient recall and the incidence of anxiety, depression, or acute stress disorder (ASD).
Methods:
This investigation was a randomized, double-blind, single-center study. Existing continuous benzodiazepine sedation was converted to dexmedetomidine or midazolam when patients qualified for daily awakenings. Sedation was titrated to achieve Riker sedation agitation scores of 3 to 4. The intensive care unit (ICU) Stressful Experiences Questionnaire, hospital anxiety and depression scale, and the impact of event scale-revised were administered before hospital discharge to assess recall, anxiety, depression, and manifestations of ASD.
Results:
A total of 11 patients received dexmedetomidine, and 12 patients received midazolam. Median dosing was 0.61 µg/kg/h for 3.5 days for dexmedetomidine and 3.7 mg/h for 3 days for midazolam. Attainment of goal sedation and analgesia was similar; however, more dexmedetomidine patients experienced agitation and pain. The median duration of mechanical ventilation from study drug initiation to extubation was 3.4 days in dexmedetomidine patients and 2.9 days in midazolam patients. Dexmedetomidine patients remembered 18.5 experiences compared with 8.5 in midazolam patients (P = .015). Rates of anxiety and depression were similar. In all, 5 (62.5%) dexmedetomidine patients and 1 (12.5%) midazolam patient manifested ASD (P = .063), and 1 dexmedetomidine patient and 5 midazolam patients developed new-onset delirium (P = .07). Hypotension occurred in 10 (90.9%) dexmedotomidine patients and 6 (50%) midazolam patients (P = .069).
Conclusions:
Transitioning benzodiazepine sedation to dexmedetomidine when patients qualify for daily awakenings may reduce the development of delirium and facilitate remembrance of ICU experiences but may lead to manifestations of ASD. Monitoring hypotension is required for both the sedatives. Additional comparative studies focusing on the long-term impact of ICU recall and psychological outcomes are needed.
Keywords
Introduction
Appropriate sedative use in critically ill patients should optimize comfort and minimize adverse events. 1–3 Dexmedetomidine is a selective α2-adrenoceptor agonist that produces sedation, anxiolysis, and partial analgesia. 4 Dexmedetomidine sedation is unique, because it is less sedating than the commonly used agents and does not suppress the respiratory drive. 4 However, its use is limited because hypotension and bradycardia are frequent side effects. 4
Recent studies show that dexmedetomidine effectively maintains goal sedation and may facilitate ventilator liberation. 4–7 Patients in these studies required light sedation prior to enrollment and were transitioned to dexmedetomidine within 24 to 96 hours of intensive care unit (ICU) admission. Although dexmedetomidine limited the occurrence of acute brain dysfunction (delirium and coma) and improved the ability of patients to communicate while sedated, 4–7 none of these studies assessed psychological outcomes. This is important because anxiety, depression, acute stress disorder (ASD), and posttraumatic stress disorder (PTSD) in ICU patients may be related to several interconnected parameters, including the sedation regimen, the occurrence of delirium, the duration of mechanical ventilation, and the ability of patients to remember their ICU experiences. 8,9
Dexmedetomidine’s pharmacologic and clinical properties suggest it may be an ideal bridging sedative when extubation is approaching since it minimizes neurologic compromise and respiratory depression (to facilitate liberation) and lessens acute brain dysfunction to possibly enhance recall. It is unknown, however, whether these beneficial outcomes reduce the occurrence of deleterious psychological outcomes. The goals of this randomized, double-blind pilot study were to evaluate the utility and safety of transitioning patients from benzodiazepines to dexmedetomidine once they qualified for daily awakenings and to specifically assess patient recall of their ICU experiences and the incidence of anxiety, depression, and ASD manifestations.
Materials
Patients
The protocol was approved by the University of Colorado Anschutz Medical Center institutional review board. Patients were enrolled in the medical or surgical ICUs. Written informed consent and Health Insurance Portability and Accountability Act authorization were obtained from legally authorized next of kin.
Critically ill patients requiring mechanical ventilation and receiving a benzodiazepine infusion with an anticipated need of at least 12 additional hours of sedation at a Riker sedation agitation score of 3 to 4 were recruited once they qualified for daily awakenings. Exclusion criteria were age less than 18 or greater than 85 years; administration of benzodiazepines for purposes other than sedation (eg, seizure control); administration of neuromuscular blockers for more than 12 hours; administration of epidural medications; active myocardial ischemia; second- or third-degree heart block; hemodynamic instability; active neuromuscular disease; Childs-Pugh class C liver disease; alcohol abuse within 6 months of study eligibility; baseline dementia; solid organ transplant; pregnancy; moribund state with planned withdrawal of life support; enrollment in another therapeutic study; or known or suspected severe adverse reactions to any benzodiazepines, dexmedetomidine, or clonidine.
Intensive Care Unit Sedation, Analgesia, and Ventilator Liberation Practices
Sedation was provided using a protocol that preferentially administers benzodiazepines. This protocol is incorporated into the computerized provider order entry system and applied across all ICUs. According to the protocol, infusions are titrated by the ICU nurse to the desired Riker sedation-agitation score. Analgesia is provided with fentanyl infusion titrated to a Pain Assessment Behavioral Scale (PABS) score of ≤3. Infusion rates of these agents are increased by 25% when goal comfort is not achieved after 2 bolus doses equivalent to half the current infusion rate. Sedation is held when patients are oversedated until a Riker score of 3 is achieved at which time sedation is resumed at half the previous rate. Assessments of Riker scores and PABS measurements occur hourly during dosage adjustments and at least every 4 hours thereafter.
Daily awakenings are performed by bedside nurses when the following conditions are met: patient is hemodynamically stable, patient is not receiving neuromuscular blockade, and patient is on ≤70% for fraction of inspired oxygen and ≤14 cmH2O-positive end expiratory pressure. A spontaneous breathing trial (SBT) is performed at the discretion of the medical team or by the respiratory therapist if predefined conditions are met. The respiratory therapist may extubate the patient if the tidal volume is ≥5 mL/kg ideal body weight, vital capacity is ≥10 mL/kg ideal body weight, and/or the rapid shallow breathing index is ≤105. Failure of the SBT is determined by any of the following: respiratory rate >35, minute ventilation >20 L/min, oxygen saturation <90%, systolic blood pressure >180 or <90 mm Hg, or respiratory distress.
Study Design
This prospective, randomized, double-blind pilot study compared substituting continuous benzodiazepine sedation with dexmedetomidine when patients were eligible for daily awakenings. Within 24 hours of qualifying for daily awakenings, patients were randomized by a computer-generated random numbers table to receive dexmedetomidine or midazolam continuous sedation. Dexmedetomidine (0.075 µg/kg/mL) and midazolam (0.5 mg/mL) were prepared in 0.9% sodium chloride in clear infusion bags indistinguishable from one another. Both the agents were titrated by the bedside nurse for a Riker score of 3 to 4. Dexmedetomidine was started at 0.15 µg/kg/h and adjusted by 0.15 µg/kg/h to a maximum of 1.5 µg/kg/h, while midazolam was started at 1 mg/h and adjusted by 1 mg/h to a maximum of 10 mg/h. All infusions were adjusted by increments of 2 mL/h to maintain blinding. Existing sedation and analgesia were weaned after the study sedative was infused for 2 hours by decreasing lorazepam by 0.5 mg/h, midazolam by 1 mg/h, and fentanyl by 10 µg/h for every incremental 2 mL/h rate increase in study sedative assuming sedation and analgesia were maintained. Open-label midazolam or fentanyl were permitted according to the sedation and analgesia protocol if agitation or pain were present or if the maximum study drug dose was reached. Intravenous haloperidol and oral neuroleptics were used at the discretion of the medical team only after delirium was identified.
Outcomes
The primary outcomes were the rates of post-ICU anxiety, depression, and ASD manifestations. Recall, anxiety, depression, and ASD were evaluated at least 72 hours after extubation or tracheostomy but before hospital discharge. The ICU recall was assessed using the ICU Stressful Experiences Questionnaire (ICU-SEQ). 10–12 This questionnaire assesses 29 potentially stressful experiences of ICU patients who received mechanical ventilation, each on a 5-point scale. Anxiety and depression were assessed using the hospital anxiety and depression scale (HADS). 8,9 The HADS consists of 14 questions, 7 for anxiety and 7 for depression, with each question scored on a 3-point scale. A total score of 11 for each subscale is indicative of the presence of manifestations representing anxiety or depression. The ASD-related traits were assessed using the impact of event scale-revised (IES-R). 13 The IES-R has 3 subscales, 8 questions on intrusion, 8 questions on avoidance, and 6 questions on hyperarousal. Each item is scored on a 4-point scale with a cumulative score of 30 indicative of the presence of ASD. All 3 questionnaires are easily administered and possess good reliability and validity. 8–13 Positive screenings, however, should be considered as traits representative of anxiety, depression, and ASD with definitive diagnosis of each requiring evaluation by trained providers. Although the IES-R is commonly used to screen for PTSD at least 1 month following a traumatic event, it was applied in this study to assess for ASD and should not be interpreted as manifestations of PTSD.
A secondary outcome was successful ventilator liberation, defined as at least 72 hours of tracheal extubation. Patients received their previously randomized study medication if they were reintubated within 72 hours of extubation. These patients were analyzed only if successful extubation subsequently occurred. Patients reintubated after 72 hours were excluded from continuing the study, and sedation and analgesia were managed by the medical team. Tracheostomy and death were not considered extubation, and these patients were excluded from the analysis of ventilator liberation. Other outcomes included hourly and cumulative doses of conventional sedatives and analgesics; percentage of Riker scores at various sedation levels; percentage of PABS scores indicating minimal pain (≤3); delirium during each 12-hour nursing shift as measured by an investigator using the Intensive Care Unit Delirium Screening Checklist (ICDSC); ICU and hospital lengths of stay; and hypotension (systolic blood pressure ≤90 mm Hg or a decrease in systolic blood pressure of 40 mm Hg), bradycardia (heart rate ≤55 beats/min or a decrease of 20 beats/min), or tachycardia (heart rate ≥120 beats/min or an increase of 20 beats/min). Lorazepam doses were converted to midazolam using a ratio of 1 mg lorazepam to 2 mg midazolam. 3
Statistical Analysis
Data from multiple studies were used to determine the number of patients needed to show a difference in time to ventilator liberation. 5–7,14,15 Additionally, based on a power of 0.8 and a significance of 0.05, 16 patients were required per group to show a desired absolute difference of 30% in the occurrence rates of anxiety, depression, and ASD manifestations. It was anticipated that an additional 9 patients per group would be required secondary to study withdrawal or persistent intubation. An independent data and safety monitoring board was not convened for this study, and an interim analysis was not conducted.
Mean, median, standard deviation, and interquartile ranges (IQRs) were determined for all continuous data. Statistical analysis of continuous data (acute physiologic and chronic health evaluation III score, age, time to ventilator liberation, sedative and analgesic doses, and ICU length of stay) used the Student t test or Mann-Whitney U test for parametric and nonparametric data, respectively. Statistical analysis of proportions (diagnoses, race, gender, Riker, and PABS; presence of delirium, agitation, and depression, or ASD; and occurrence of adverse events) used a chi-square test or Fisher exact test. All analyses were 2 tailed. A P value <.05 was considered significant, and P values ≤.10 are reported.
Results
Patient Population
From September 2009 to May 2012, 23 mechanically ventilated patients were enrolled from 469 consecutive patients screened (Figure 1). Of the 23 patients, 11 were randomized to dexmedetomidine and 12 to midazolam (Table 1). The study was stopped early due to slow enrollment as sedation practices changed to favor intermittent benzodiazepine administration. Therefore, the number of patients expected to require an additional 12 hours of continuous sedation decreased significantly over the study period.
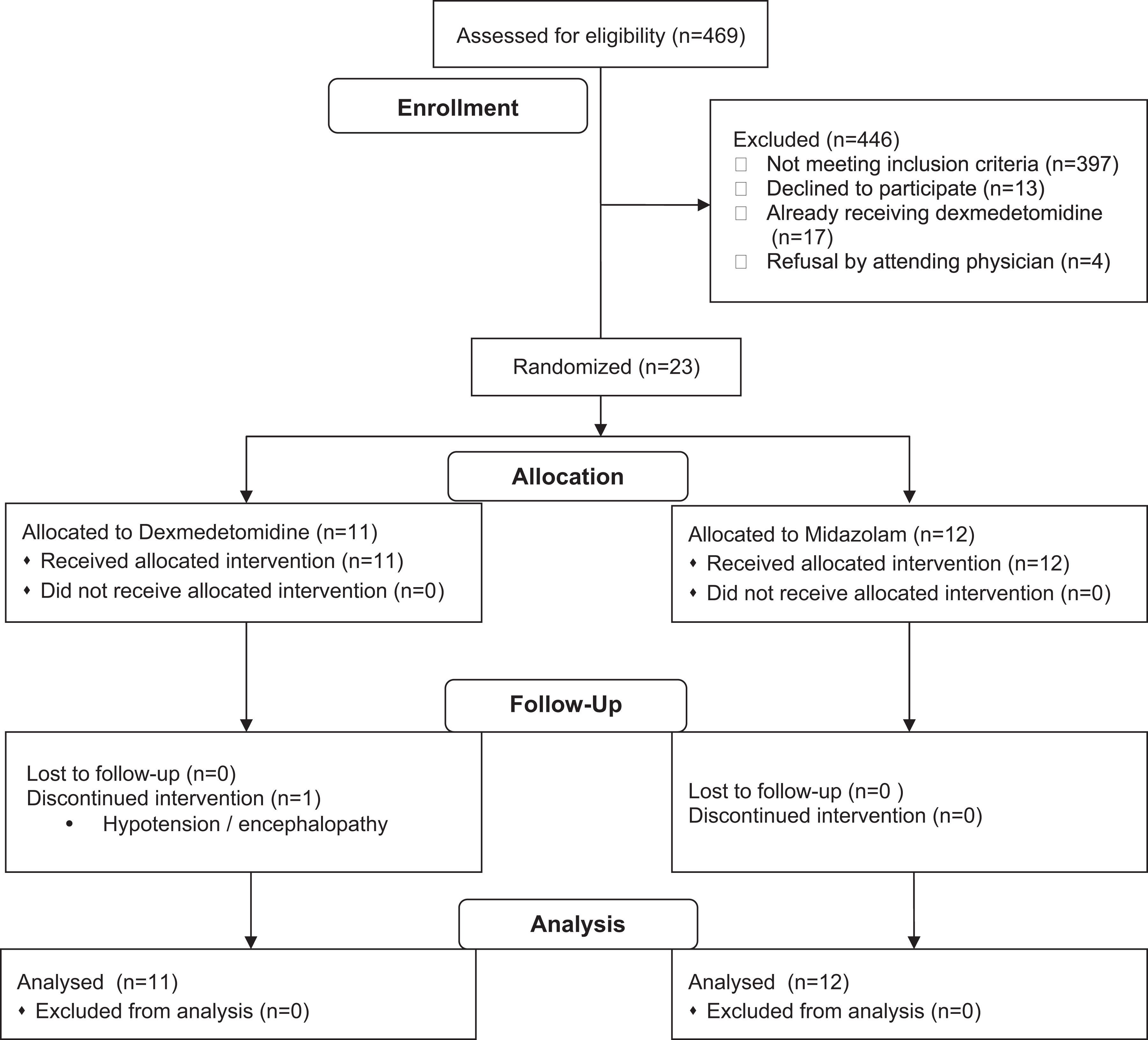
Patient enrollment, randomization, and study flow.
Baseline Demographics and Characteristics of Study Population.a
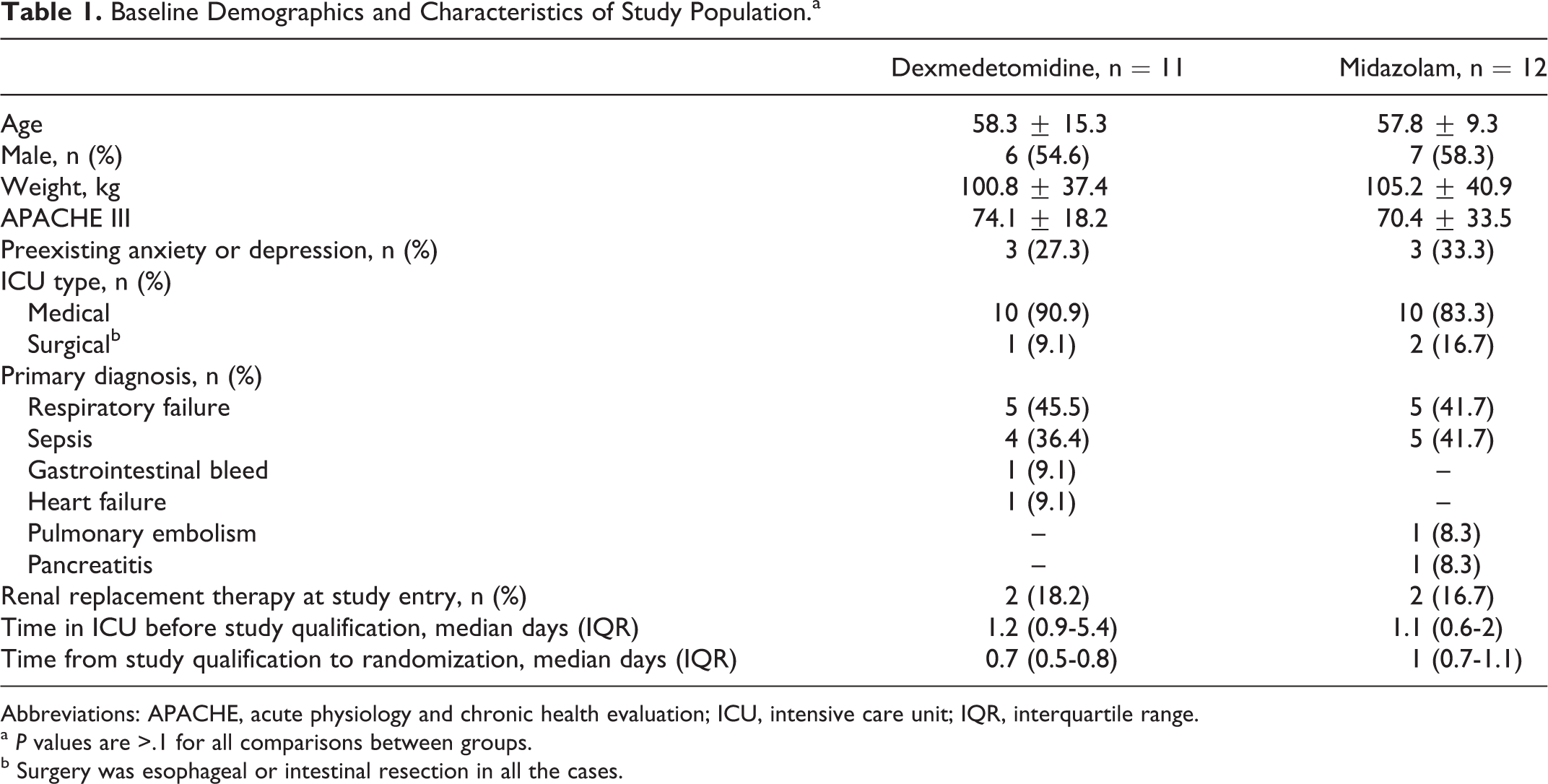
Abbreviations: APACHE, acute physiology and chronic health evaluation; ICU, intensive care unit; IQR, interquartile range.
a P values are >.1 for all comparisons between groups.
b Surgery was esophageal or intestinal resection in all the cases.
Study Drug Administration and Sedation Efficacy
Dexmedetomidine patients required slightly more open-label midazolam though the midazolam group received more total midazolam (Table 2). All patients received fentanyl by continuous infusion at baseline, and the cumulative amounts administered over the study period were similar between groups. Riker scores indicating agitation occurred about 4-fold more frequently in the dexmedetomidine group. Similarly, PABS scores indicating pain occurred approximately twice as often in the dexmedetomidine group despite similar fentanyl requirements. Daily awakenings were used in 74% and 77% of eligible opportunities in the dexmedetomidine group and midazolam group, respectively.
Study Drug Administration and Sedation and Analgesia Parameters.a
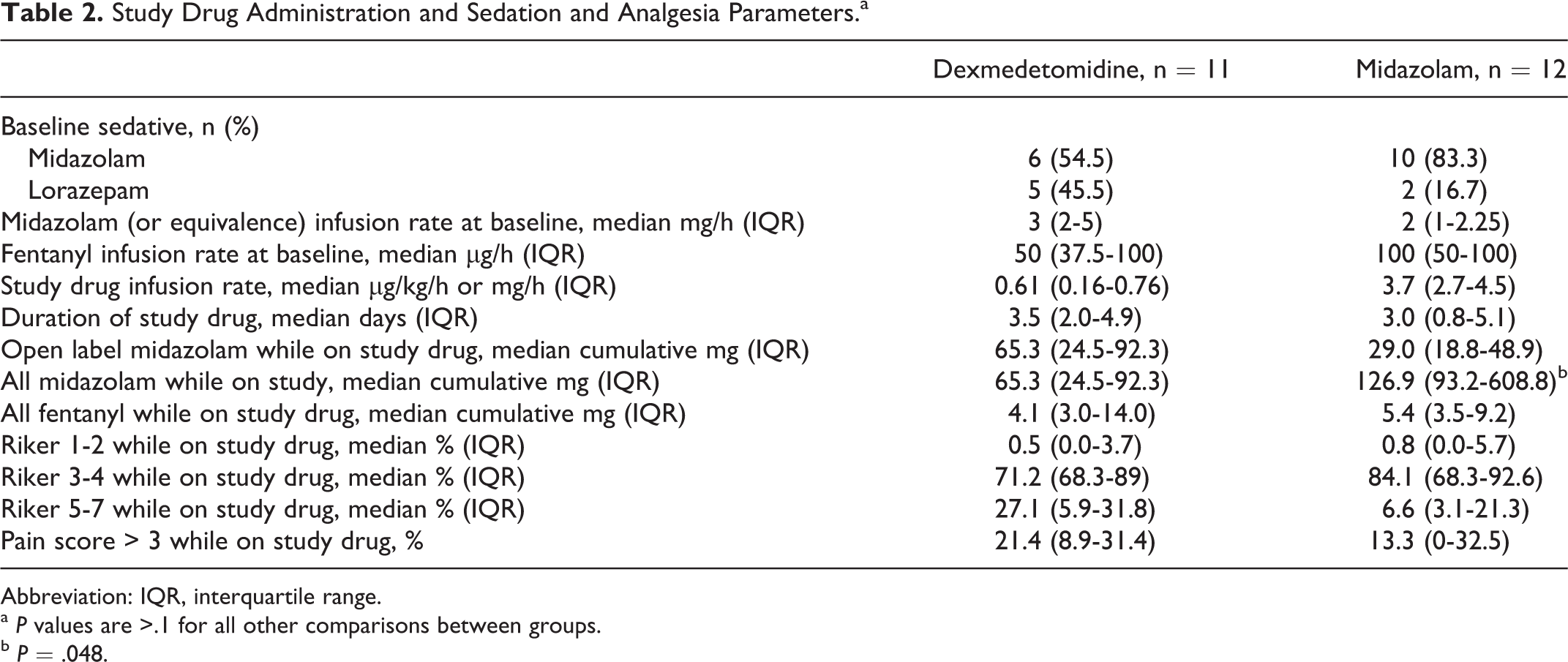
Abbreviation: IQR, interquartile range.
a P values are >.1 for all other comparisons between groups.
b P = .048.
Patient Disposition, ICU Length of Stay, and Ventilator Liberation
Two (18.2%) dexmedetomidine patients and 1 midazolam patient died before extubation. Four patients in each group were discharged home; the remainder were transferred to a long-term care facility. There were no significant differences between total ICU length of stay, ICU length of stay after randomization, or total duration of mechanical ventilation. Median ICU length of stay was 18.4 days (IQR, 11.5-33.9) and 16.1 days (IQR, 6.5-28.1) for dexmedetomidine and midazolam, respectively. The ICU length of stay after randomization was 10.2 days (IQR, 6.8-25.2) and 12 days (IQR, 4.8-14.8), respectively. Median total duration of mechanical ventilation was 9.4 days (IQR, 5.9-15.5) and 9.5 days (4.2-11.7), respectively. Total duration of mechanical ventilation for ICU survivors was 8.2 days (IQR, 5.7-15.5) and 10.9 days (4.4-12.6), respectively. In all, 4 (36.4%) dexmedetomidine patients and 3 (25%) midazolam patients failed extubation. In all, 1 dexmedetomidine patient was reintubated after 72 hours, but the other 6 patients resumed their study drug allocation. In all, 3 (27.3%) dexmedetomidine patients and 2 midazolam (16.7%) patients required tracheostomy. The median duration of mechanical ventilation from study drug initiation to extubation was 3.4 days (IQR, 2.6-14.2) in 7 dexmedetomidine patients and 2.9 days (IQR, 2-4.4) in 8 midazolam patients.
Recall, Anxiety, Depression, and ASD
Of 8 patients in each group that completed the questionnaires, preexisting anxiety or depression was present in 2 dexmedetomidine patients and 3 midazolam patients. Prior to admission, all these patients were receiving a selective serotonin reuptake inhibitor, and 1 patient in each group was receiving scheduled benzodiazepine therapy. None of these patients was taking a neuroleptic agent, prazosin, or clonidine at the time of admission. One dexmedetomidine patient was reintubated after completing the questionnaires. The median number of experiences remembered by dexmedetomidine patients was 18.5 compared with 8.5 for the midazolam patients (P = .015; Table 3). Of the 29 possible memories, 18 (62.1%) were more likely to be recalled in the dexmedetomidine group and 4 (13.8%) were more likely to be recalled in the midazolam group (P < .001). In general, patients rated the extent of their memory of each experience as moderate to extreme. Manifestations of anxiety and depression were similar between the groups (Table 4). Specific question items of the HADS that rated statistically more frequent in the dexmedetomidine group were “I have troubles falling or staying asleep,” “I stay away from reminders of the ICU,” “Any reminder brings back feelings about the ICU,” “My feelings are kind of numb,” and “I get a frightening feeling as if something awful is going to happen.” Positive IES-R screenings occurred in 5 dexmedetomidine patients and 1 midazolam patient (P = .063) and were consistent across the 3 subscales of intrusion, avoidance, and hyperarousal (Table 4).
Patient Recall of ICU Experience (ICU-SEQ).a
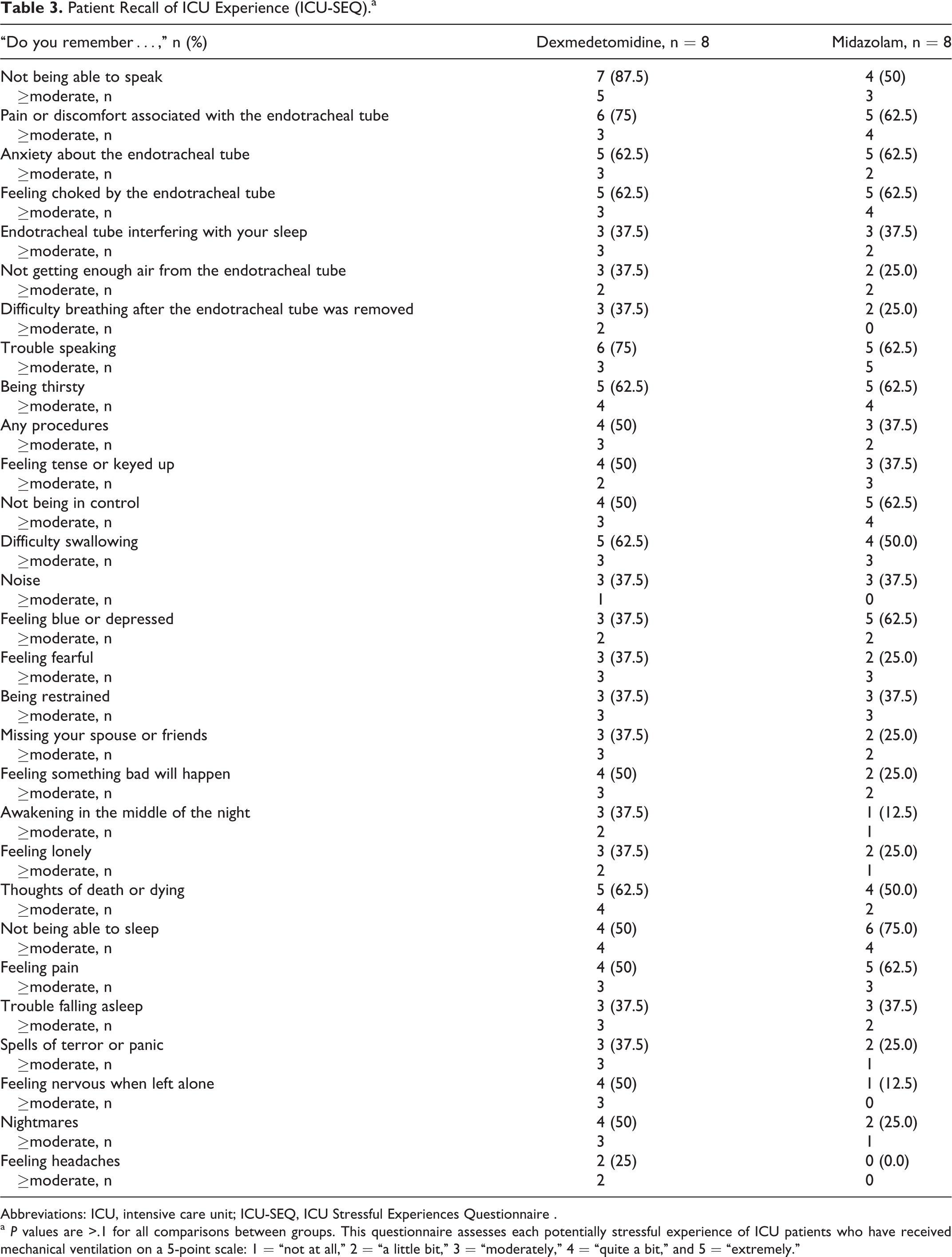
Abbreviations: ICU, intensive care unit; ICU-SEQ, ICU Stressful Experiences Questionnaire .
a P values are >.1 for all comparisons between groups. This questionnaire assesses each potentially stressful experience of ICU patients who have received mechanical ventilation on a 5-point scale: 1 = “not at all,” 2 = “a little bit,” 3 = “moderately,” 4 = “quite a bit,” and 5 = “extremely.”
Manifestations of Anxiety, Depression, and ASD.a
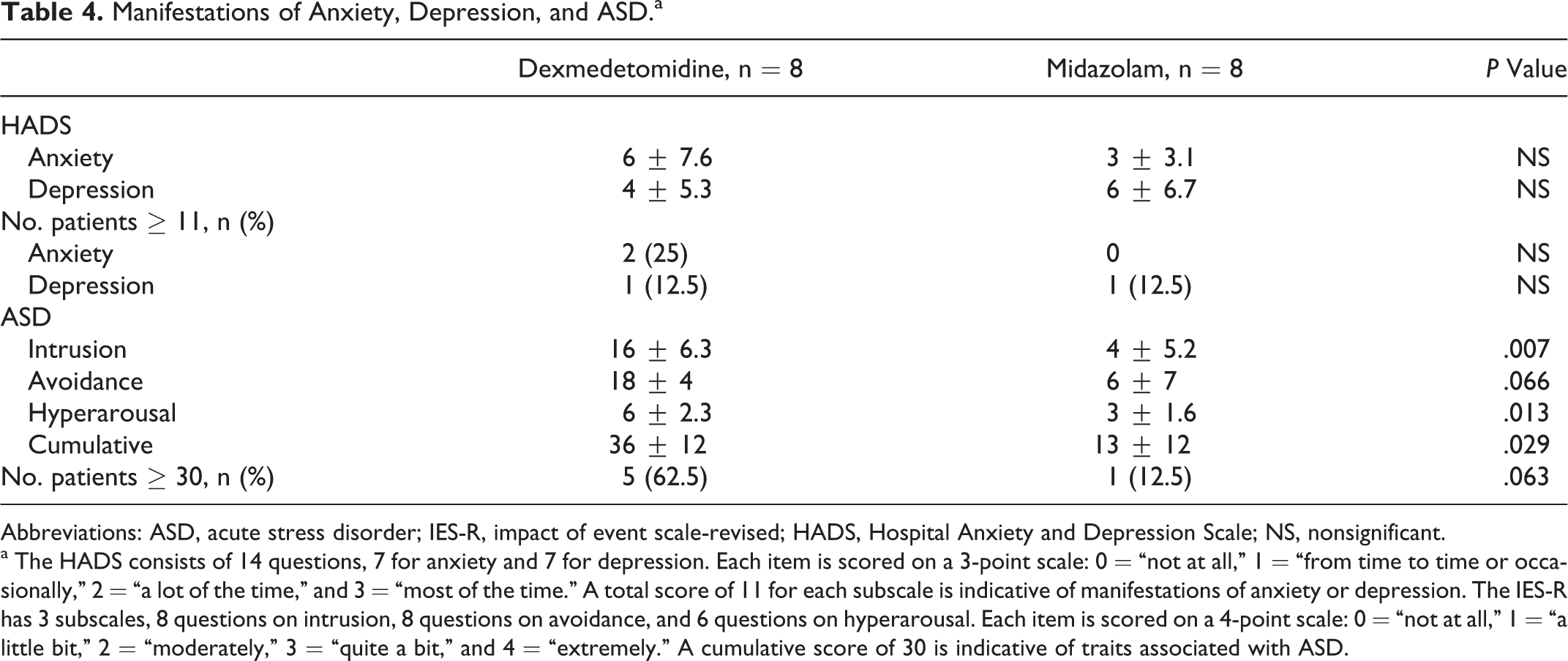
Abbreviations: ASD, acute stress disorder; IES-R, impact of event scale-revised; HADS, Hospital Anxiety and Depression Scale; NS, nonsignificant.
a The HADS consists of 14 questions, 7 for anxiety and 7 for depression. Each item is scored on a 3-point scale: 0 = “not at all,” 1 = “from time to time or occasionally,” 2 = “a lot of the time,” and 3 = “most of the time.” A total score of 11 for each subscale is indicative of manifestations of anxiety or depression. The IES-R has 3 subscales, 8 questions on intrusion, 8 questions on avoidance, and 6 questions on hyperarousal. Each item is scored on a 4-point scale: 0 = “not at all,” 1 = “a little bit,” 2 = “moderately,” 3 = “quite a bit,” and 4 = “extremely.” A cumulative score of 30 is indicative of traits associated with ASD.
Adverse Events
One dexmedetomidine patient developed hypertension and encephalopathy within 2 hours of starting the study drug, necessitating the permanent discontinuation of all continuous infusion sedatives (Table 5). Blood pressure and neurologic status improved within 6 hours of discontinuing all sedatives. This patient eventually required a tracheostomy and was transferred to a long-term care facility. Another 3 dexmedetomidine patients developed hypotension to the extent that the study drug was temporarily stopped by the medical team. Delirium was present at baseline in 3 patients in each group, but fewer dexmedetomidine patients developed delirium over the course of study drug administration. All patients with delirium received haloperidol, and two patients with delirium in each group received olanzapine.
Adverse Events During Study Drug Administration.a
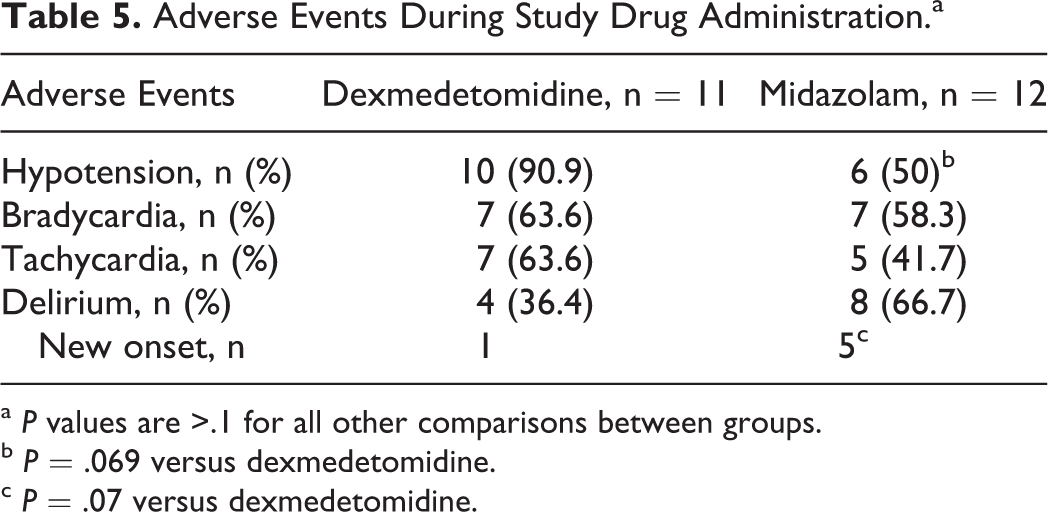
a P values are >.1 for all other comparisons between groups.
b P = .069 versus dexmedetomidine.
c P = .07 versus dexmedetomidine.
Discussion
This randomized, double-blind study was stopped early due to slow enrollment that was the result of institutional sedation practices changing during recruitment. Whether the study influenced these changes is unknown. Despite the enrollment of only 23 patients, some meaningful results were obtained that warrant further investigation. Dexmedetomidine did not expedite ventilator liberation, but its use was associated with less midazolam administration, more hypotension, less delirium, and greater recall of ICU experiences. Patients receiving dexmedetomidine were no more likely to develop traits of anxiety or depression but were more likely to manifest ASD symptoms before hospital discharge. These results should be interpreted as hypothesis generating and may serve as pilot data for future studies.
Like most other studies, our results suggest that dexmedetomidine effectively maintains light-to-moderate sedation 5–7,14,15 ; however, the occurrence rates of Riker and PABS scores reflecting discomfort or pain were 2- to 4-fold higher with dexmedetomidine. Other studies suggest that additional sedatives or analgesics may be required to maintain comfort while using dexmedetomidine, possibly because the lighter level of sedation provided by dexmedetomidine may require supplementation when deeper sedation is desired or the lighter level of sedation facilitates the ability of patients to communicate discomfort or request additional sedatives or analgesics. 4–7 We found the use of open-label midazolam was approximately doubled with dexmedetomidine, but total midazolam exposure was reduced. Less overall benzodiazepine administration should have facilitated extubation. We speculated that the lack of respiratory suppression associated with dexmedetomidine would facilitate ventilator liberation when patients met daily awakening criteria. We were unable to verify this hypothesis likely because the duration of mechanical ventilation is dependent upon many factors other than sedation, and our sample size was small. Nonetheless, further studies are warranted to investigate whether dexmedetomidine facilitates ventilator liberation while providing comfort.
We found that dexmedetomidine reduced new-onset delirium as measured by the ICDSC. While this is consistent with previous studies comparing dexmedetomidine and benzodiazepines that measured delirium with the Confusion Assessment Method ICU, some of these studies also showed reduced duration of mechanical ventilation which itself may affect the occurrence of delirium. 4–7 We found less delirium with dexmedetomidine despite similar length of ventilation. These data support minimizing the use of benzodiazepines to reduce the occurrence of delirium.
Our study is the first investigation to compare patient recall after sedation with dexmedetomidine or a benzodiazepine. We found that dexmedetomidine increased recall associated with mechanical ventilation. Although the ICU-SEQ is validated for this purpose, it only assesses negative perceptions associated with mechanical ventilation. Whether the recall of pleasurable events (eg, interacting with family and friends) is enhanced with dexmedetomidine is unknown. Two short-term postoperative studies found greater recall of pain or discomfort with dexmedetomidine compared to propofol. 16,17
Although several specific question items of the HADS were rated higher by patients receiving dexmedetomidine, the occurrence of anxiety and depression manifestations was similar between the groups. In contrast, dexmedetomidine patients were more likely to manifest traits of ASD across all subscales (intrusion, avoidance, and hyperarousal). Therefore, while dexmedetomidine patients were more likely to remember the unpleasant experiences associated with mechanical ventilation, this did not alter manifestations of anxiety or depression but acutely increased perceptions of traumatic stress. Manifestations of ASD traits may be related to delirium and recall, both of which are affected by sedation. 8–12 Increased manifestations of ASD in the dexmedetomidine group were surprising since these patients experienced less delirium. 18,19 The development of ASD-associated symptoms, however, may be related to enhanced discomfort and pain assessed in this group. These results also contrast with other studies that found lighter sedation or limited benzodiazepine administration enhanced recall and reduced deleterious cognitive or psychological outcomes after discharge. 12,20–32 This may be related to methodological differences as we assessed these outcomes while patients were in the hospital, whereas other studies conducted these assessments weeks to months after hospital discharge or as post hoc analyses. Whether ASD leads to PTSD and the association of dexmedetomidine with ASD manifestations and possibly PTSD clearly require further study, especially since dexmedetomidine is recommended in critically ill patients at high risk of developing delirium. 1 Also, ASD manifestations shortly after ICU discharge may not confer PTSD. It may be that greater remembrance of negative ICU experiences leads to traits of ASD, but the occurrence of PTSD is unaffected or lessened because these memories provide patients with context to cope.
Despite starting dexmedetomidine at a low dose, hypotension occurred in all, but 1 dexmedetomidine patient and required temporary study drug discontinuation in 3 patients. This is consistent with the results of other studies. 4–7,14,15 Hypotension also occurred frequently in the midazolam group. Vigilant monitoring for hypotension is needed for both the sedatives, especially early in therapy or when the dosage is increased.
This study is not without limitations. Early termination resulted in fewer patients than required for predefined statistical power. This study is an example of how research may alter practice in a favorable manner for patient care to the extent that recruitment is affected. The occurrence of anxiety, depression, and ASD used screening tools, but definitive diagnosis of each requires patient assessment by trained clinicians. Also, the IES-R is a screening tool for PTSD, and its application as an assessment tool for ASD has not been validated despite research reports of its use for this indication. 13 The order of administering the surveys may have influenced the results as patients were first asked to assess their recall of mostly negative perceptions that were more likely to occur in the dexmedetomidine group and may have promoted manifestations of ASD.
Conclusion
Dexmedetomidine did not expedite ventilator liberation, but its use was associated with less midazolam administration, more hypotension, less delirium, and greater recall of ICU experiences. Patients receiving dexmedetomidine were no more likely to develop symptoms of anxiety or depression, but they were more likely to manifest traits of ASD before hospital discharge. Further studies are warranted to investigate the appropriate application of dexmedetomidine in mechanically ventilated patients.
Footnotes
Authors’ Note
All authors participated in the design of the study, data interpretation, and manuscript preparation. RM is the principal investigator and was responsible for budget management, regulatory compliance, patient recruitment, data collection, entry, and analyses, and manuscript preparation. CRP, SWM, THK, and DNF aided in patient recruitment, study coordination; and data collection, entry, and analyses. JCL and SPM aided in patient recruitment, study coordination, and patient assessments for study purposes. Data were presented at the Society of Critical Care Medicine’s Annual Congress; January 22, 2013; San Juan, PR and the European Society of Intensive Care Medicine Meeting; October 9, 2013; Paris, France. Abstracts were published in Critical Care Medicine 2012;40:1111, and Intensive Care Medicine 2013;39(suppl2):S469.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Financial support was obtained by an investigator-initiated research grant from Hospira. Trial registration: clinicaltrials.gov identifier NCT00744380.