
Abstract
Background:
Interhospital transportation of critically ill patients is challenging. The risk incurred by the patient is compounded when stabilization and application of appropriate therapies are delayed. The purpose of this study was to first develop an interhospital intensive care unit (ICU) transfer instrument to systematize communication and determine feasibility of use. Then, the transfer instrument was tested for effects on patient mortality, stability on arrival, and recommended therapy implementation.
Method:
The instrument was developed and pilot tested for 6 months to optimize function and applicability. Then, a before-and-after quasi-experimental study tested this instrument by assessing several key outcomes. Outcomes measured included 48-hour mortality, ICU mortality, hospital mortality, emergent intubation, emergent central venous catheter insertion, immediate change in antibiotics, and addition of vasopressors immediately on arrival. Patients were compared by age, gender, cause for admission, and Acute Physiology and Chronic Health Evaluation (APACHE) II score. A standardized mortality ratio was calculated using the patient’s APACHE II score. Pretransport recommendations to referring physicians and adherence to recommendations were also measured.
Results:
The preintervention group consisted of 134 patients collected continuously over 6 months. The postintervention group was collected continuously over a 6-month period and included 77 patients. The interhospital ICU transfer instrument was associated with fewer emergent central venous catheter insertions and fewer changes in antibiotics on arrival. Recommendations to transferring physicians were followed 90% of the time.
Conclusions:
The interhospital ICU transfer instrument is a tool that is effective in coordinating the transfer of medical ICU patients. Implementation leads to timely critical interventions and may reduce mortality.
Introduction
Interhospital transport of severely ill patients from smaller rural or community hospitals to a tertiary medical center’s medical intensive care unit (ICU) is a common practice and is performed to enhance the prognosis of the patient. 1 The need to transport critically ill patients is projected to increase due to demographic changes in aging of the population and regionalization of specialists and critical care resources to improve efficiency. 2,3 Previous observational studies have shown transferred patients have a higher than expected mortality when compared to patients who presented at the tertiary medical center but these studies have been fairly difficult to conduct and assess, given small sample sizes and heterogeneity of confounder adjustment. 4 –8 These studies have also reported that interhospital transfer of patients to medical ICUs (MICUs) have longer ICU and overall hospital length of stay than those patients with local presentations. 5,6 The uncertainty of this risk has prompted development of administrative risk models, like that used by the University Health System, to include transfer status in their predicted patient mortality calculation. 9
Although specific causalities underpinning the increased risk of mortality among interhospital transfer patients are not well defined, previously identified associations include distance traveled, medical complications, severity of illness, and subtype of illness. 10 The proposed reasons for increased mortality include risk of complications and stressors inherent to transport process and delay in critical therapies secondary to time traveling to definitive care location. 10 These findings in medically critically ill patients run counter to the “scoop and run” approach citing time to tertiary medical center as the most important predictor of outcome. 11,12 Experts in critical care medicine actually caution against the “scoop and run” approach in the medically critically ill patient as definitive therapies can frequently be initiated at referring hospitals and continued in route. 10,13,14 This notion is supported by a retrospective review that demonstrated adult populations with critical care needs who had therapies initiated en route had longer stabilization times prior to transport but had shorter ICU and hospital length of stay at the receiving hospital. 15
The American College of Emergency Physicians guidelines endorse the use of medical evaluation and essential stabilization by the referring facility within their capabilities and use of written transfer protocols for optimal care. 16 Mirroring that precedent, most ICU guidelines on interhospital transport recommend clear communication of patient care between referring and accepting physicians guided by a protocol allowing recommendations to be made for early therapy and stabilization prior to transport. 10,13,14
It has been postulated that fidelity of communication and early institution of appropriate therapies, including adequate antibiotics and resuscitation, is critical in this fragile population. 10 The Joint Commission identified failure of communication as the most frequent cause of serious preventable adverse events and has included improved communication as a 2012 National Patient Safety Goal. 17 Current practice suggests interhospital transfer communication, which includes referring physician and contact number, patient’s name, age, nature of illness or injury, vital signs, physical findings, results of pertinent diagnostic studies, treatment, current condition, reason for transfer, and recommendations on transportation selection. 10 After discussion, the accepting critical care physician can make recommendations on method of transport and current management. 10,13,14
To date, no transfer planning instrument has been directly studied for efficacy of communication and early initiation of recommended therapies among medically critically ill patients. The purpose of this study was to first develop an interhospital ICU transfer instrument to systematize communication and determine feasibility of use. Then, the transfer instrument was tested for effects on patient mortality, stability on arrival, and emergent therapy implementation. A recommendation section specific to critically ill medical patients was also included to determine how often recommendations to outside physicians were implemented. It was hypothesized that this transfer instrument would improve patient care outcomes by clarifying communication and initiating critical therapies earlier in the transfer process.
Methods
The University of Virginia institutional review board approved the study prior to initiation and gave approval for waiver of consent due to the minimal risk imposed to patients. This study was conducted in 3 phases: ICU transfer instrument development, pilot testing of ICU transfer instrument, and outcome ascertainment prior to and following the patient transfer instrument intervention.
Study Design
ICU transfer instrument
Development
A patient transfer instrument was developed (Figure 1) with 4 main sections: (1) patient data, (2) reason for transfer, (3) treatment recommendations, and (4) condition on arrival. The patient data section was based on previous expert opinion, consultation with the research and practice literature, and discussion with the institution’s critical care physicians and our emergency medicine colleagues. 10 The instrument included physician and hospital contact information, past medical history, a history of present illness narrative highlighting complicating problems, the patient’s current vital signs, and essential test results. Vital signs were focused around the “ABC’s” (airway, breathing, and circulation) including notation of ventilator setting paired with the ABG, blood pressure paired with vasopressor, and vascular access. Additional fields included pertinent laboratory test results, current antibiotics with culture data, and radiology data with a prompt to ensure the original films are sent. The second section prompted the user to notify key services that will be involved in the patient’s care so that the full care team is ready to act on the patient’s arrival. The third section prompted and documented recommendations made to referring physician. This section was divided into the core recurring components of medical ICU patient’s treatment: ventilator support, antibiotics, resuscitation, and central vascular access for that resuscitation. The instrument user was asked to identify the reasoning behind therapy choices to facilitate dialog and identify opportunities for intervention delivery before or during transport. The final section provided feedback to the process by collecting data on the patient’s status on arrival to the receiving hospital.
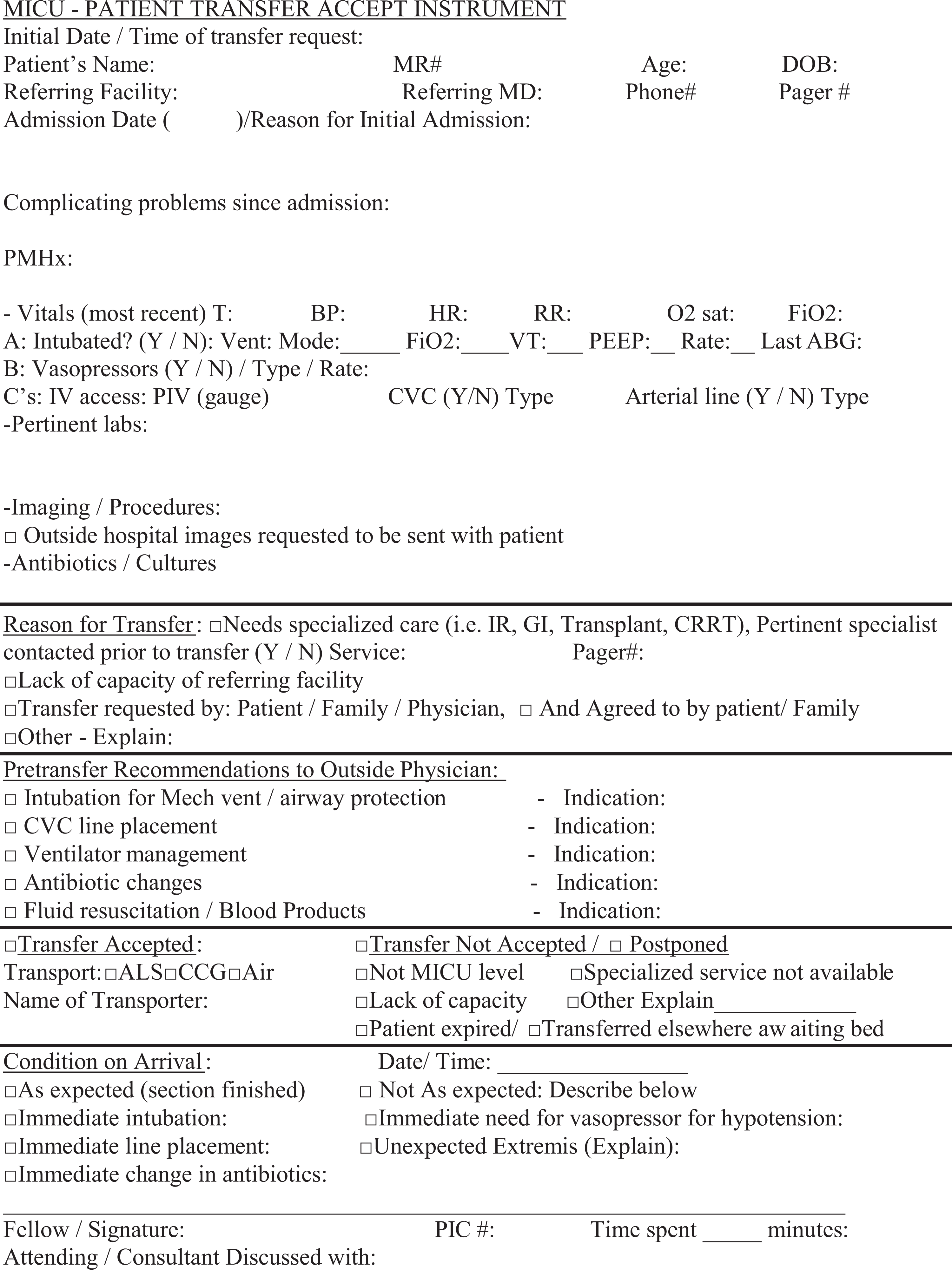
Medical intensive care unit—patient transfer accept instrument.
Pilot testing
Prior to the instrument implementation, a training session on interhospital patient transfer instrument was conducted among fellow physicians who would be utilizing the instrument. The instrument was initiated and pilot tested for the last 6 months of 2010 by physicians accepting outside hospital transfers to a closed medical ICU in a single academic tertiary referral center. The accepting physicians were all pulmonary critical care fellow physicians, at different years of training, who remained in close communication with the attending physicians. Following the 6-month testing period, all of the participating physicians completed a survey to assess functionality prior to further testing (Figure 2). Questions were measured on a Likert-type scale with 1 = strongly disagree and 5 = strongly agree.
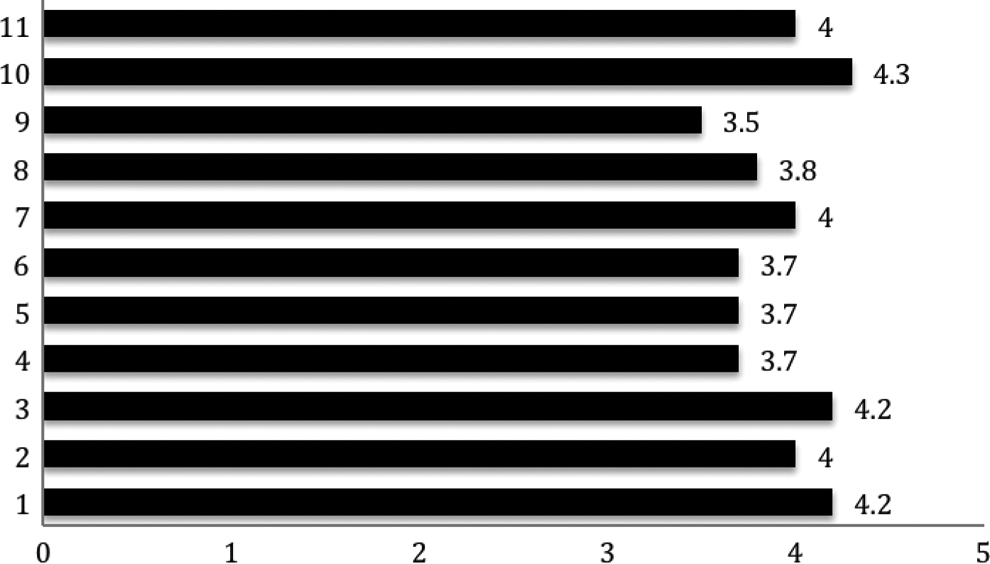
Likert-Type scale scoring of the questions listed subsequently assessed by physicians accepting transfer requests after 6 months of instrument implementation. (x-axis the Likert score 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree. y-axis denotes the question number from Appendix A).
Outcome ascertainment
A quasi-experimental study was performed after implementation of the instrument. The preintervention group included all patients admitted to the medical ICU team who were transferred from outside hospitals for 6 months starting in January 2009. The postintervention group included all patients admitted to the medical ICU team transferred from outside hospitals for 6 months starting January 2011 (after implementation of the transfer instrument). Patients in both the groups were compared using age, gender, and Acute Physiology and Chronic Health Evaluation (APACHE) II scores. Outcome measures included early patient mortality within 48 hours, ICU mortality, hospital mortality, APACHE II risk-adjusted hospital mortality, need for urgent intervention at time of arrival denoted by antibiotics changed (specifically the need for broader coverage than currently provided), need for immediate central venous catheter, additional vasopressors, and immediate intubation. The intervention variables were chosen for analysis because they were all clear definitive actions. These variables were postulated by the study team, attending physicians in the MICU, and conferred by the literature to have the greatest potential impact on patient outcomes.
Statistical Analysis
Descriptive statistics were calculated to describe all survey responses and patient and outcome variables using either mean/standard deviation for continuous variables or frequency/percentage for categorical variables. Standardized mortality ratios (SMRs) were calculated based on APACHE II-predicted mortality. The postintervention group was then compared to the preintervention group using the chi-square statistic (and Fisher exact test when n < 10) for dichotomous variables and t test for continuous variables with normal distributions. Independent associations between use of transfer instrument and outcome variables were then calculated. Odds ratios (ORs) and confidence intervals (CIs) were reported to determine the impact of instrument use (yes/no) on risk associated with adverse patient-related outcomes. Statistics were calculated with SPSS version 19, IBM.
Results
Intensive Care Unit Transfer Instrument Development and Pilot Testing
After the initial 6 months trial basis, the pulmonary critical care fellow physicians using the instrument (n = 6) reported their impressions through the 5-point Likert-type scale. Questions and responses are shown in Appendix A and tabulated in Figure 2. All users were either in agreement, strong agreement, or neutral to all the question prompts. The statements with the most consistent agreement are as follows: (1) the MICU transfer instrument is an efficient method for gathering needed data (mean score 4); (2) by listing specific recommendations and relaying this information to the MICU resident physician is there a more formulated plan in place when the patient arrives (mean score 4.3); (3) the MICU transfer instrument has made me consider more the potential decompensations during transport (mean score 4); and (4) the detail of information you collect has increased (mean score 4.2).
Intensive Care Unit Transfer Instrument Testing
The preintervention group included 134 patients. The postintervention group included 77 patients where the checklist was performed for a total 110 transfers from outside hospitals (70% compliance using the checklist). In 42 (55%) patients in the postintervention group, explicit recommendations on treatment were made and documented on the form prior to transport and all of these recommendations were followed in 38 (90%) patients.
As shown in Table 1, the 2 groups were similar in age and gender occurring in equal distribution. The postintervention group had a higher APACHE II score (19.2 in the postintervention group vs 16.3 in the preintervention group, P = .048). The postintervention group had fewer emergent central lines placed on arrival (2.4% vs 24%, P < .01) and fewer changes to antibiotics (33.8% vs 51.5% in the preintervention group, P value .01). The unadjusted mortality between the groups in the first 48 hours and during their ICU and hospital stay was not statistically different. However, after hospital mortality was adjusted for severity of illness by APACHE II scoring, there was a significant improvement in SMR for the postintervention group (preintervention SMR 1.05, postintervention SMR 0.71, P < .01).
Comparison of Patient and Outcome Variables Among Pre- and Postimplementation Cohorts.
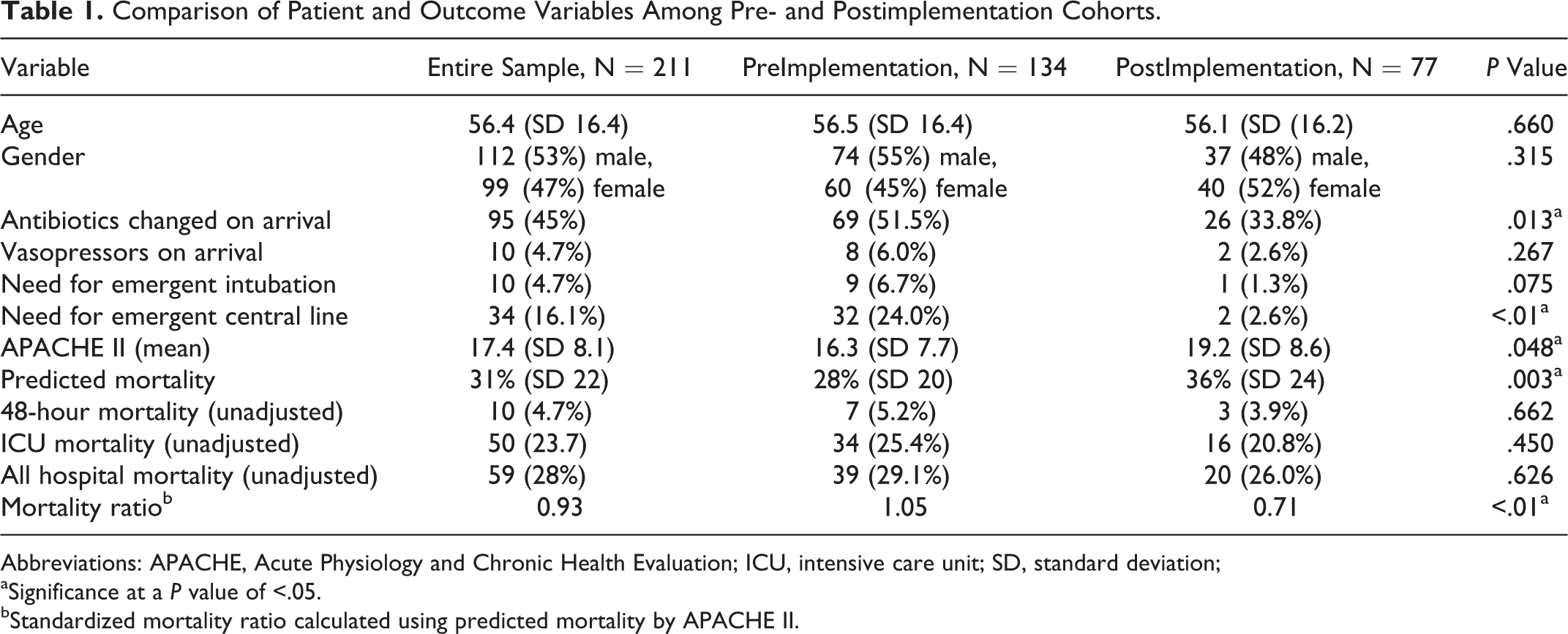
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; ICU, intensive care unit; SD, standard deviation;
aSignificance at a P value of <.05.
bStandardized mortality ratio calculated using predicted mortality by APACHE II.
Odds ratio calculation showed that the postintervention group (when transfer instrument used) demonstrated a statistically significant reduction in likelihood needing antibiotics changed (OR 0.48, CI 0.269-0.859) or needing an emergent central line placed (OR 0.085, CI 0.02-0.366) upon arrival to the tertiary hospital (Table 2).
Odds Ratio of Outcome Occurrence If the Instrument Was Used.
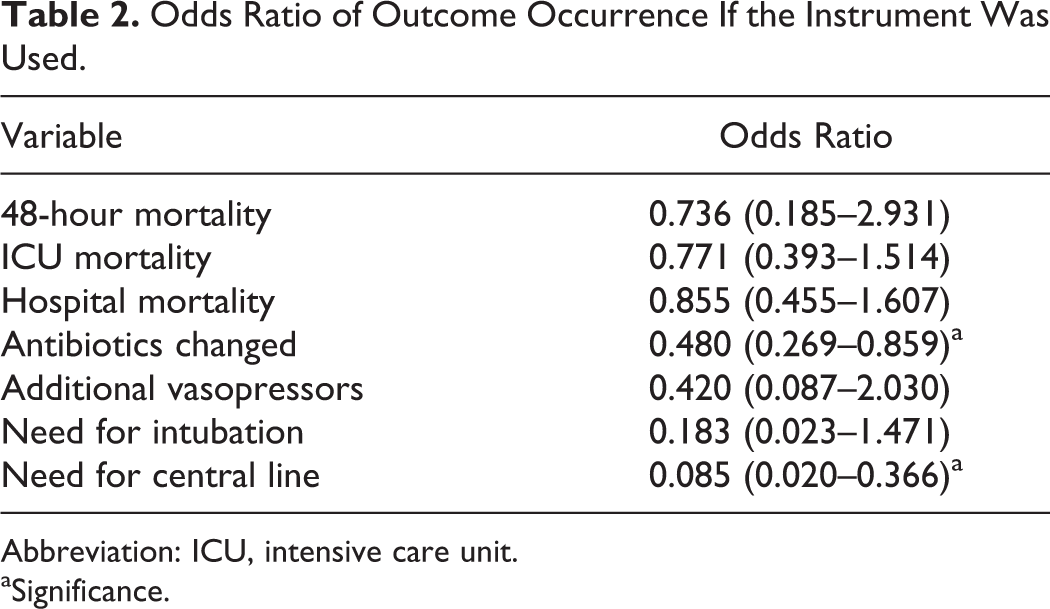
Abbreviation: ICU, intensive care unit.
aSignificance.
We reviewed the charts of the 33 patients in the postintervention group in which the transfer instrument was not used. In this group, 55% were male and 45% were female, the average age was 48, and the average APACHE II score was 14, therefore generally a healthier group. The hospital mortality for this group was 24% and after adjustment for APACHE II score the SMR was 1.00. There was no statistical difference in patient-related variables between the no-instrument group and the preintervention group or postintervention group for APACHE II score or mortality. The medical illness requiring ICU admission in all 3 groups is displayed in Table 3.
Critical Illness Requiring ICU Admission.a,b
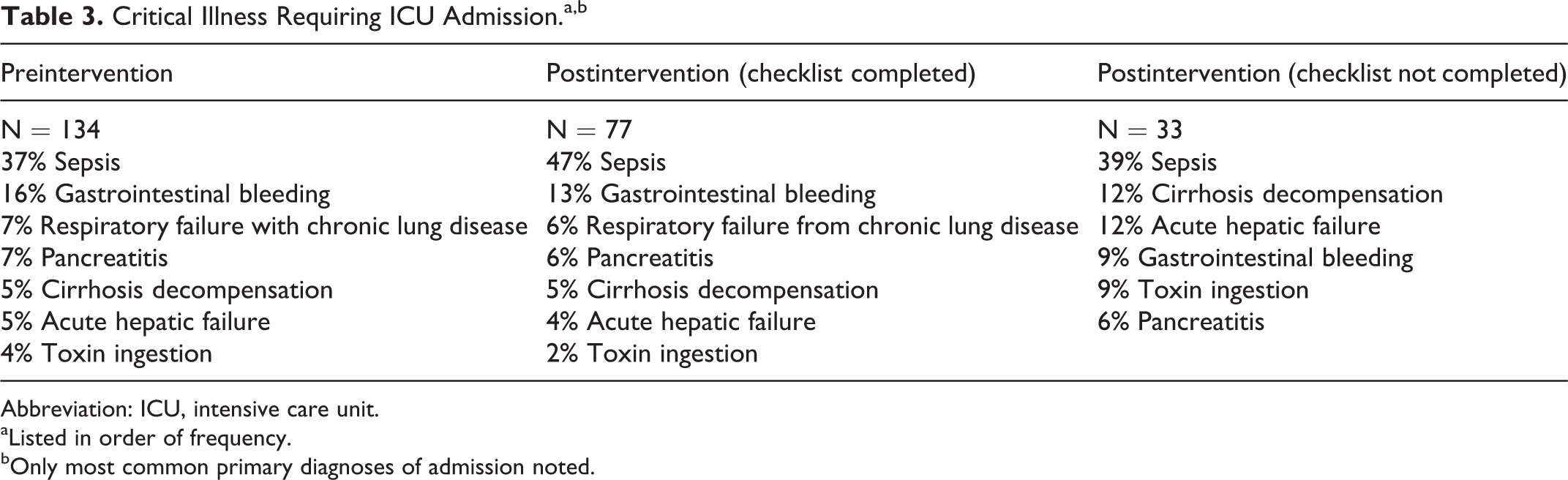
Abbreviation: ICU, intensive care unit.
aListed in order of frequency.
bOnly most common primary diagnoses of admission noted.
Discussion
The impetus for the ICU transfer instrument was born out of a desire for improving communication, timely institution of critical therapies, and preventing decompensations during transport to the receiving hospital. In our quasi-experimental study, the need for emergent central venous catheter placement and antibiotic adjustment was also significantly lower in the postintervention group. An interesting clinical finding, but 1 that lacks the ability to draw causal implications related to the transfer instrument alone, is that the SMR was significantly less in the postinstrument cohort. These findings suggest that a simple transfer instrument used to standardize communication and mitigate risk can aid intensivists and improve outcomes in the interhospital transfer of critically ill patients from one ICU to another.
Based on previous observations, our target population’s most common problems include sepsis, gastrointestinal bleeding, acute respiratory failure, acute pancreatitis, and decompensated cirrhosis. Therefore, the recommendation to outside provider’s section specifically focused on respiratory status, antibiotics, resuscitation needs, and vascular access for resuscitation and vasopressor support. The prompt for the accepting physician’s reasoning documentation was intended to facilitate open discussion with outside physicians and to identify opportunities for time-sensitive care as early as possible. We believe this is a critical element since early interventions, such as appropriate antibiotics and goal-directed resuscitation for severe sepsis, improve mortality outcomes and can be started at the outside hospital. 18 –20
When recommendations for interventions were made by the accepting physician, the implementation of proposed therapy was extremely high at 90%. The implementation was always at the discretion and final say of the outside physician. A previous study by Ligtenberg et al in the Netherlands examined referring facility compliance with the receiving hospital recommendations. 1 They found a lower level of overall compliance by outside physicians, with only 50% of transfer recommendations being followed, although the paper does not specify which and how the recommendations were requested or recorded. 1
Although changing antibiotics on arrival is not a strict surrogate of delay in adequate antibiotics, it reflects the accepting physician identifying inadequate coverage when the patient arrives. In this study, OR calculations suggest that those in the postimplementation cohort were significantly less likely to need a change in antibiotics upon arrival to the accepting hospital. These findings, in conjunction with instrument documentation of antimicrobial recommendations that were initiated, demonstrate that the transfer checklist triggers a discussion of antibiotic management prior to transfer. This intervention may have led to patients receiving adequate therapy earlier, which is central to sepsis management. 19
In addition to antibiotics, we had 3 additional themes in our postintervention group. First, emergent insertion of central venous catheters on arrival at the receiving hospital declined. Second, in review of our transfer forms collected after implementation, we observed that recommendations for antidotes for toxic ingestions, for example, acetaminophen overdose, were not always started pretransport. Thus, we added a line in the recommendations section for antidotes and therapy for intoxication. Finally, the frequency of emergent intubation on arrival did not decline significantly following implementation of the transfer instrument. Of the 134 patients, 9 required intubation immediately after transfer before implementation compared to 1 of the 77 patients after implementation of the transfer instrument. A significant difference may have not been measurable due to the inadequate sample size to detect power and low occurrence of the event in the postintervention group.
Our study is limited by the quasi-experimental design that limits the strengths of our conclusions due to the potential for biases, such as improvement in outcomes over time. We have attempted to address this by measuring mortality as described by APACHE II and use of the comparison to the preintervention cohort from a similar 6-month period (January to July). The difference in adjusted mortality between the postimplementation cohort and the preimplementation cohort supports the inference that the standardization of communication may improve mortality outcomes but a larger sample size and more robust study design are needed to address this research question. For future research, use of APACHE IV might improve the confounding measurement based on severity of illness but using the APACHE II at both time points maintained the internal consistency of our analysis. Another limitation of the instrument was the paper format. In the interim, our center has transitioned to a complete electronic medical record and we are integrating the form into this system. We hope this will enhance compliance, completeness, and usability while making the data immediately available to all caring for the patient. Continued quality improvement will be acheived through data collection and pattern recognition. Additionally, this research was conducted at 1 tertiary medical center in central Virginia; therefore, our results may not be generalizable to other tertiary centers with a large urban catchment area.
The benefits measured by implementing the transfer instrument may have been more pronounced at our center due to several characteristics. Our MICU is often full and the time to move the more stable patients to the floor or open an over flow unit can delay transit. Additionally, due to a large rural catchment area, patients may travel over 150 miles or more. This can greatly prolong the time to definitive therapy if appropriate stabilizing interventions are not initiated prior to transport.
Conclusions
To our knowledge, this is the first systematic study of an instrument for interhospital transfer of ICU patients. Instituting our ICU transfer instrument was associated with fewer immediate changes in antibiotics and a reduction in emergency insertion of central venous catheters on arrival. Recommendations to referring physicians were followed 90% of the time. Due to the benefit to patient care in our institution, we have continued to use the ICU transfer instrument and are making improvements on the model. We are currently integrating the instrument into the electronic medical record allowing easier access to all members of the treatment team.
Appendix A
Questions Posed to Physicians Accepting Transfers Using the Instrument
Communication is difficult at times with outside physicians.
The accept form has changed the way you collect information on transfers.
The detail of information you collect has increased.
Communication has improved between you and the outside physician.
Communication has improved between you and residents / charge nurses / other fellows?
The accept form has increased the number of recommendations made to outside physicians.
The accept form has made me consider more the potential decompensations during transport.
The accept form has changed what I recommend so that the decompensations are less likely.
By making the recommendations more explicit on the form outside providers have been more likely to carry them out.
By listing specific recommendations and relaying this information to the resident is there a more formulated plan in place when the patient arrives?
The MICU accept form is an efficient method gathering needed data.
Footnotes
Authors’ Note
H. Charles Malpass participated in study design, data collection and analysis, and article preparation and was Guarantor author of this article. Jessica Keim-Malpass participated in data analysis and article preparation. Kyle B. Enfield and George M. Verghese participated in study design, data analysis, and article preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.