
Abstract
Introduction:
A new strain of human influenza A (H1N1) virus originated from Mexico in 2009 and spread to more than 190 countries and territories. The World Health Organization (WHO) declared it a level 6 (highest level) pandemic. In August 2010, WHO announced that the H1N1 2009 influenza virus had moved into the postpandemic period. The WHO also declared that this flu strain is expected to continue to circulate as a seasonal virus “for some years to come.” The objective of this study is to describe the chest radiographic and computed tomography (CT) findings of patients with severe H1N1 pneumonia admitted to the intensive care unit (ICU) during the 2009 pandemic.
Hypothesis:
Patients with severe H1N1 pneumonia requiring ICU admission have extensive radiographic and CT abnormalities.
Methods:
Eighteen patients, aged 23 to 62 (mean 41), admitted to the ICU at UCLA-Olive View Medical Center with a primary diagnosis of pandemic H1N1 infection, confirmed either via rapid influenza detection test or by real-time reverse transcriptase polymerase chain reaction assay, formed the study population. All patients had chest x-ray (CXR) within 24 hours of admission and 5 patients had CT examinations. In this retrospective study, images were evaluated for the pattern (ground-glass opacities, consolidation, reticular opacities, and nodular opacities), distribution (unilateral/bilateral, upper/middle/lower lung zone, and central/peripheral/peribronchovascular), and extent (focal/multifocal/diffuse; number of lung zones) of abnormalities.
Results:
All (100%) patients had abnormal CXR and CT studies. The predominant radiographic findings were ground-glass opacities (16 of 18; 89%), consolidation (16 of 18; 89%), and reticular opacities (6 of 18, 33%). The radiographic abnormalities were bilateral in 17 (94%) patients; involved lower lung distribution in 18 (100%) patients, and mid and lower lung distribution in 16 (89%) patients. Radiographic abnormalities were peribronchovascular in 11 (61%) patients and multifocal in 10 (56%). Sixteen (89%) patients had extensive abnormalities involving 3 or more lung zones. The patients requiring mechanical ventilation had a higher incidence of bilateral, diffuse consolidation in a peribronchovascular distribution on chest radiographs. The predominant CT abnormalities were consolidation (5 of 5; 100%), ground-glass opacities (5 of 5; 100%), and nodular opacities (3 of 5, 60%). The CT findings were peribronchovascular and multifocal in 4 (80%) patients and extensive and bilateral in all (100%) patients.
Conclusions:
Patients with H1N1 pneumonia admitted to the ICU had bilateral, extensive CXR, and CT abnormalities. Consolidations and ground-glass opacities were the most common imaging findings, predominantly affecting mid and lower lung zones. Imaging abnormalities were peribronchovascular and multifocal in a majority of patients.
Introduction
A new strain of human influenza A (H1N1) virus originated from Mexico in 2009 and spread to more than 190 countries and territories. The World Health Organization (WHO) declared it a level 6 (highest level) pandemic. The pandemic H1N1 influenza virus contained 2 swine strains, 1 avian strain and 1 human strain of influenza viruses. 1 Although mostly self-limited, an estimated 61 million cases of H1N1 pneumonia were diagnosed from April 2009 to April 2010, resulting in 274 000 hospitalizations and 12 500 deaths. 2,3
Compared with seasonal influenza, pandemic H1N1 infection was more virulent in younger adults, patients with obesity, and pregnant patients. Symptoms at presentation included fever, cough, dyspnea, diarrhea, and vomiting. Within a few months of the pandemic, the Centers for Disease Control (CDC) reported that 25% of hospitalized patients with H1N1 were admitted to the pneumonia intensive care unit (ICU), 60% of which required mechanical ventilation. 4 The median age of those who were admitted to an ICU was 29 years.
About one-third of the patients admitted to the ICU were previously healthy without underlying medical conditions. 3,5 Asthma, chronic obstructive pulmonary disease, obesity, immunosuppression (including from medications and HIV), diabetes, chronic kidney disease, and cardiovascular disease were common comorbidities among those who were admitted to the ICU. Respiratory failure and refractory shock from primary viral pneumonia or secondary bacterial infections were the most common causes of death in these patients. 6
Three factors were found to be independently associated with death in H1N1-infected patients: requirement of invasive ventilation at the time of ICU admission, any coexisting medical conditions, and older age. 2 In August 2010, the WHO declared the postpandemic period for the H1N1 influenza virus with the caveat that this strain is expected to continue to circulate as a seasonal virus “for some years to come.” 7 In fact, the 2013 to 2014 influenza seasons witnessed a resurgence of the H1N1 subtype resulting in significant morbidity and mortality. According to the Centers of Disease Control data, H1N1 has been the predominant virus reported in the 2013 to 2014 seasons, with 88% of viruses causing influenza-like illness characterized as H1N1. 8
The radiographic findings in viral pneumonias include poorly defined nodules, peribronchial ground-glass opacities, airspace consolidation, and hyperinflation due to associated bronchiolitis. 9,10 There are a limited number of studies describing exclusively the radiologic findings of patients with H1N1 influenza A admitted to the ICU. 11 –14 In this study, we retrospectively reviewed the chest radiographic and computed tomographic findings of patients with a primary diagnosis of H1N1 influenza infection admitted to the ICU at UCLA-Olive View Medical Center during the 2009 season.
Materials and Methods
Study Population
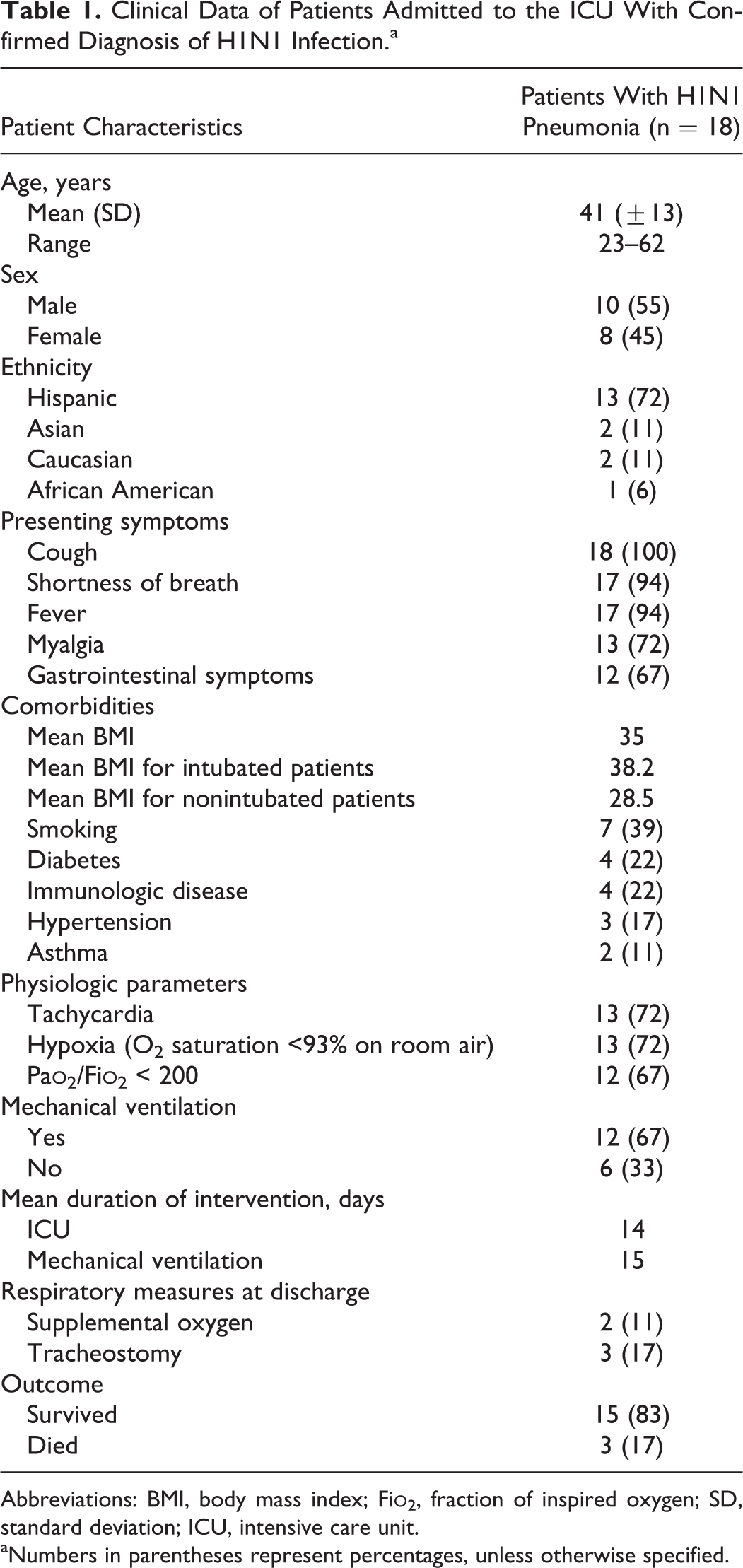
The institutional review board at UCLA-Olive View Medical Center approved this retrospective study and waived informed consent due to its observational nature. From June 2009 until November 2009, 19 adult patients with a primary diagnosis of H1N1 influenza were admitted to the ICU at UCLA-Olive View Medical Center. All patients presented with influenza-like symptoms, with diagnoses confirmed via rapid influenza detection test or by real-time reverse transcriptase polymerase chain reaction assay for H1N1. One patient who tested positive for H1N1 was excluded because his primary diagnosis was pancreatitis. Thus, a total of 18 patients were included in our study (Table 1). The selected charts were reviewed for patient demographics, presenting signs and symptoms, comorbidities (including obesity, diabetes, smoking status, asthma, chronic obstructive lung disease, autoimmune diseases, cardiovascular conditions, and renal failure), length of hospitalization and ICU stay, mechanical ventilation, need for tracheostomy or supplemental oxygen at discharge, and outcome.
Clinical Data of Patients Admitted to the ICU With Confirmed Diagnosis of H1N1 Infection.a
Abbreviations: BMI, body mass index; Fi
aNumbers in parentheses represent percentages, unless otherwise specified.
Image Acquisition and Analysis
All chest radiographs included in this study were obtained within 24 hours of admission to the hospital, with the exception of 1 radiographic study, which was obtained after 48 hours. Five patients had posteroanterior and lateral chest radiographs and 13 patients had portable chest radiographs. Admission radiographs were compared with baseline images, when available, to assess the presence of new findings. Computed tomography (CT) scans of the chest were obtained in 5 (28%) patients, within 24 hours of admission to hospital for 4 patients and on the 11th day of hospital stay for 1 patient. Computed tomography scans were obtained using a 64-slice multidetector CT scanner (Somatom Sensation or Somatom Definition; Siemens Healthcare: Malvern Inc, Pennsylvania, USA) using 120 kV, 150 to 400 mAs, and 3 mm reconstructed slice thickness. Automatic exposure control was utilized for all CT studies. Four patients received 100 mL of intravenous contrast (Omnipaque 350 or Visipaque 320; GE Healthcare). Coronal and sagittal reformations were provided. A thoracic radiologist with 10 years of experience and a pulmonologist with 13 years of experience retrospectively reviewed all chest radiographic and CT studies. Decisions on final interpretations were reached by consensus.
Imaging studies were evaluated for the type of radiologic pattern (ground-glass opacities, consolidation, reticular opacities, nodular opacities and lymphadenopathy), distribution (unilateral/bilateral, upper/middle/lower, and central/peripheral/peribronchovascular), and extent (focal/multifocal/diffuse; number of lung zones) of abnormalities. Radiographic images and CT scans were interpreted using the descriptors defined by the Fleischner Society Nomenclature Committee. 15 Ground-glass opacity is defined as an area of hazy increased lung opacity with indistinct margins of pulmonary vessels on radiograph but with preserved bronchial and vascular margins on CT. Consolidation is defined as a homogeneous increase in parenchymal attenuation that obscures vessel margins and airway walls. Reticular pattern is defined as small linear opacities forming a net pattern. Nodular opacity is defined as a rounded opacity, well or poorly defined, measuring up to 3 cm in diameter. The distribution of abnormalities was characterized as central (<4 cm from the hila), peripheral, or peribronchovascular. Each lung was divided into upper, middle, and lower lung zones comprising a third of the long axis of each lung. The presence, laterality, and size of pleural effusions were noted.
Results
Our patient population consisted of 10 men and 8 women aged between 23 and 62 years (mean 41 ± 13; Table 1). Thirteen (72%) patients were Hispanic. The mean body mass index (BMI) was 35 kg/m2, and 6 (33%) patients had obesity as their only comorbid condition. The mean BMI for patients requiring mechanical ventilation was 38.2, and the mean BMI of patients that did not require intubation was 28.5. Other comorbidities in our patient population included smoking (39%), diabetes (22%), immunologic diseases (22%), hypertension (17%), and asthma (11%). The most common presenting symptoms were cough (100%), shortness of breath (94%), fever (94%), myalgia (72%), and gastrointestinal symptoms (67%). Most patients arrived to the emergency department with tachycardia (72%) and hypoxia (72%), with arterial oxygen saturation less than 93% on room air.
16
Twelve (67%) patients had a ratio of Pa
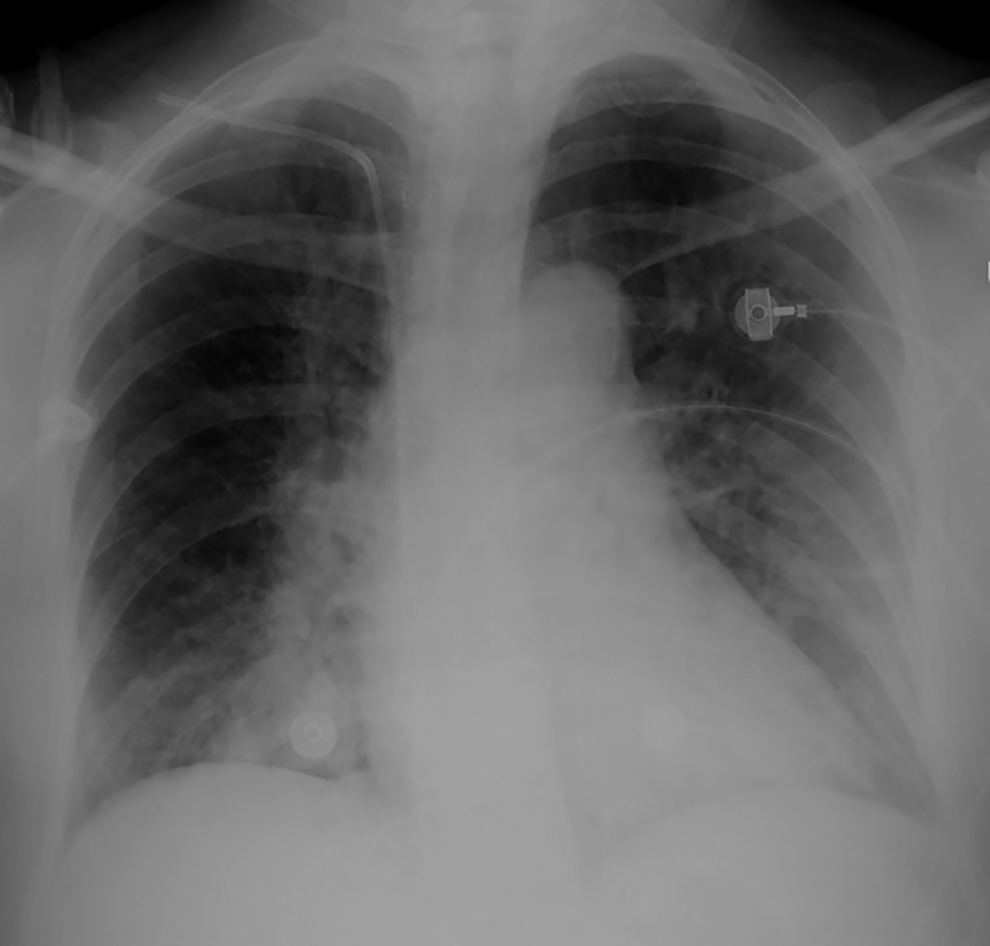
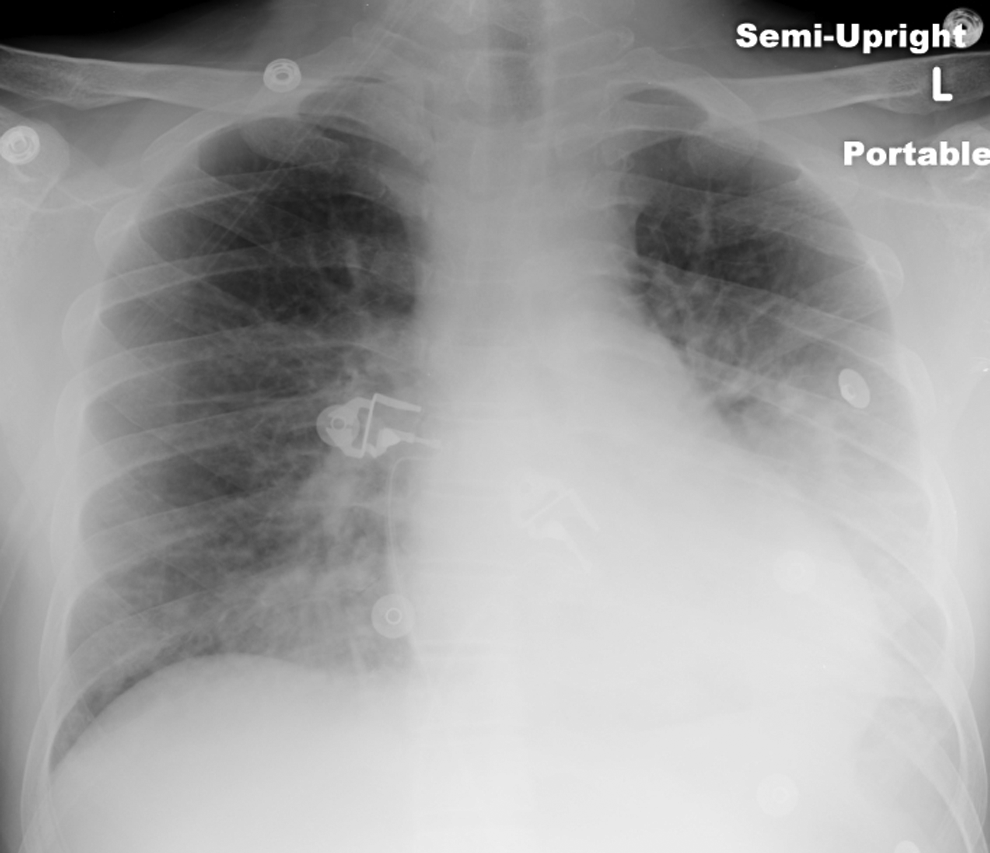
All (100%) patients had abnormal chest x-ray (CXR) radiography and CT studies (Table 2). The predominant radiographic findings were ground-glass opacities (16 of 18; 89%; Figure 1), consolidation (16 of 18; 89%; Figure 2), and reticular pattern (6 of 18; 33% Figure 3). A combination of ground-glass opacities and consolidation were noted in 9 (50%) patients. The radiographic abnormalities were bilateral in 17 (94%) patients. All patients had lower lung involvement (100%); 12 (67%) patients demonstrated middle and lower lung zone abnormalities (Figure 4); 4 (22%) patients showed involvement of all lung zones; and 2 (11%) patients showed only lower lung involvement. In all, 14 (78%) patients had both central and peripheral findings; 3 (17%) patients had central distribution of abnormalities. Eleven (61%) patients had a peribronchovascular distribution of abnormalities. In all, 10 (56%) patients had multifocal abnormalities (Figure 5) and 7 (39%) had diffuse involvement. Sixteen (89%) patients had extensive abnormalities involving 3 or more lung zones. Small unilateral or bilateral pleural effusions were seen in 16 (89%) patients (Figure 6), not requiring thoracentesis or drainage.
Chest Radiographic and CT Findings of H1N1 Patients Requiring ICU Admission.a
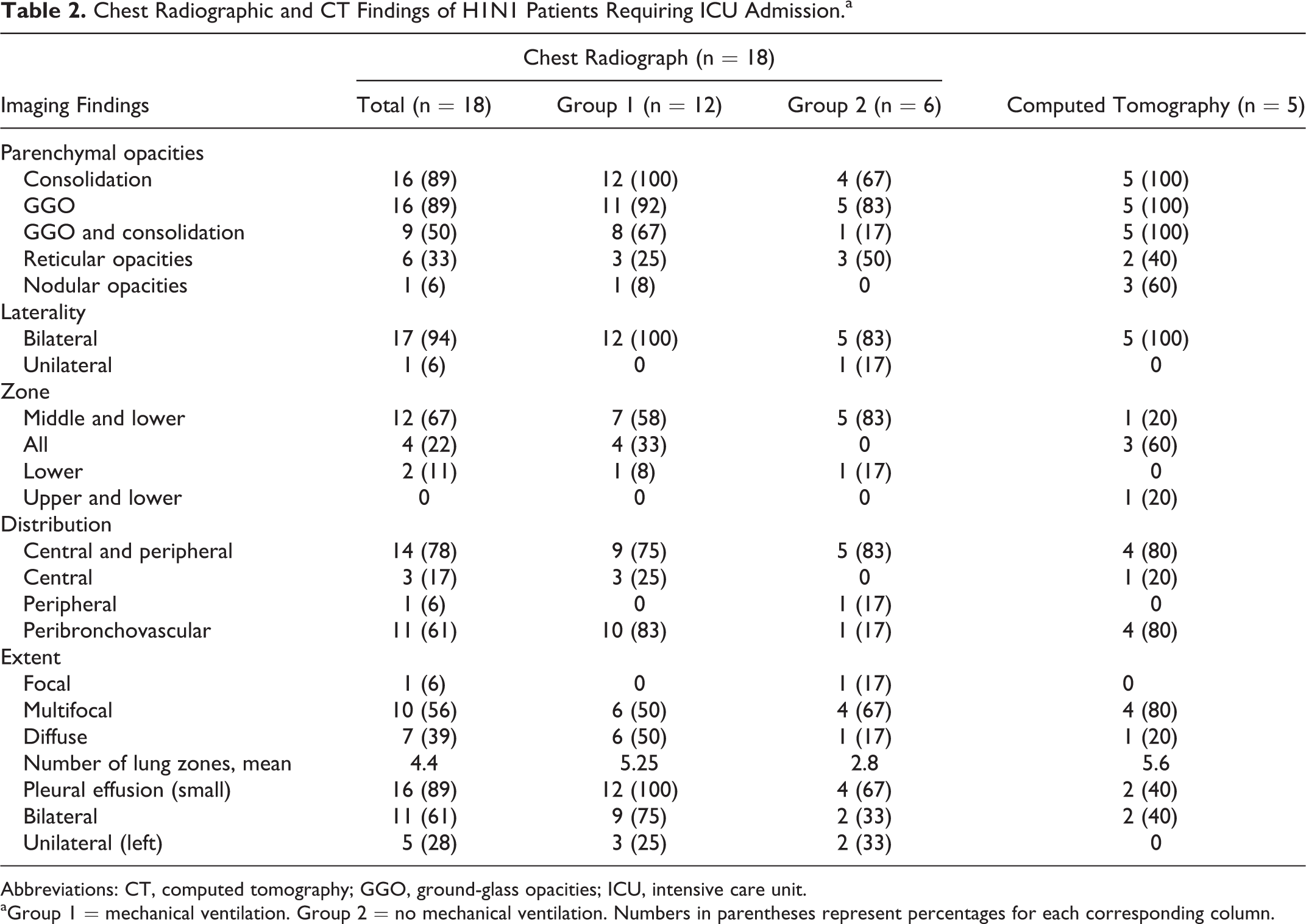
Abbreviations: CT, computed tomography; GGO, ground-glass opacities; ICU, intensive care unit.
aGroup 1 = mechanical ventilation. Group 2 = no mechanical ventilation. Numbers in parentheses represent percentages for each corresponding column.
Frontal chest radiograph in a 62-year-old woman shows bilateral ground-glass and reticular opacities in the right lower lung zone and left lung, and right lower lobe consolidation.

Frontal chest radiograph in a 34-year-old man shows bilateral diffuse consolidation and ground glass.
Frontal chest radiograph in a 20-year-old man shows bilateral diffuse reticular opacities and lower lobe consolidation.
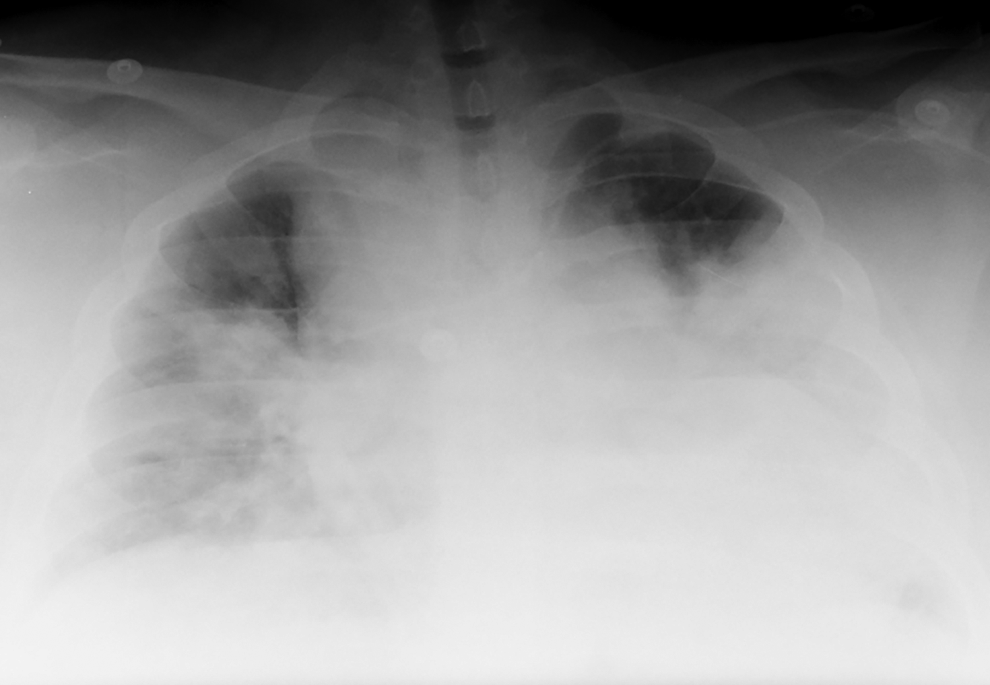
Frontal chest radiograph in a 23-year-old man shows bilateral consolidation and ground glass in the mid and lower lung zones.

Frontal chest radiograph in a 52-year-old man shows bilateral, multifocal ground-glass, and patchy consolidation with peribronchovascular distribution, involving all 6 lung zones.

Frontal chest radiograph in a 52-year-old woman shows bilateral lower lung zone ground-glass and reticular opacities, left lower lobe consolidation, and small pleural effusions, left greater than right.
All 5 patients who had thoracic CT examinations had consolidations and ground-glass opacities (100%); 3 (60%) patients had nodular opacities; and 2 (40%) patients demonstrated a reticular pattern. The thoracic CT findings were bilateral in all (100%) patients. In all, 3 (60%) patients had abnormalities involving all lung zones; 1 (20%) had mid and lower lung zone findings; and 1 (20%) patient had upper and lower lung zone abnormalities. In all, 4 (80%)patients had peribronchovascular distribution of abnormalities (Figure 7); 4 (80%) patients had central and peripheral involvement, while 1 (20%) patient had only central abnormalities. Four (80%) patients had multifocal abnormalities (Figure 8), while 1 (20%) patient had diffuse involvement. All (100%) patients demonstrated extensive CT abnormalities involving 4 or more lung zones. Two (40%) patients had small bilateral pleural effusions. Mediastinal lymph node enlargement (>1 cm on short axis) was seen in only 1 patient.
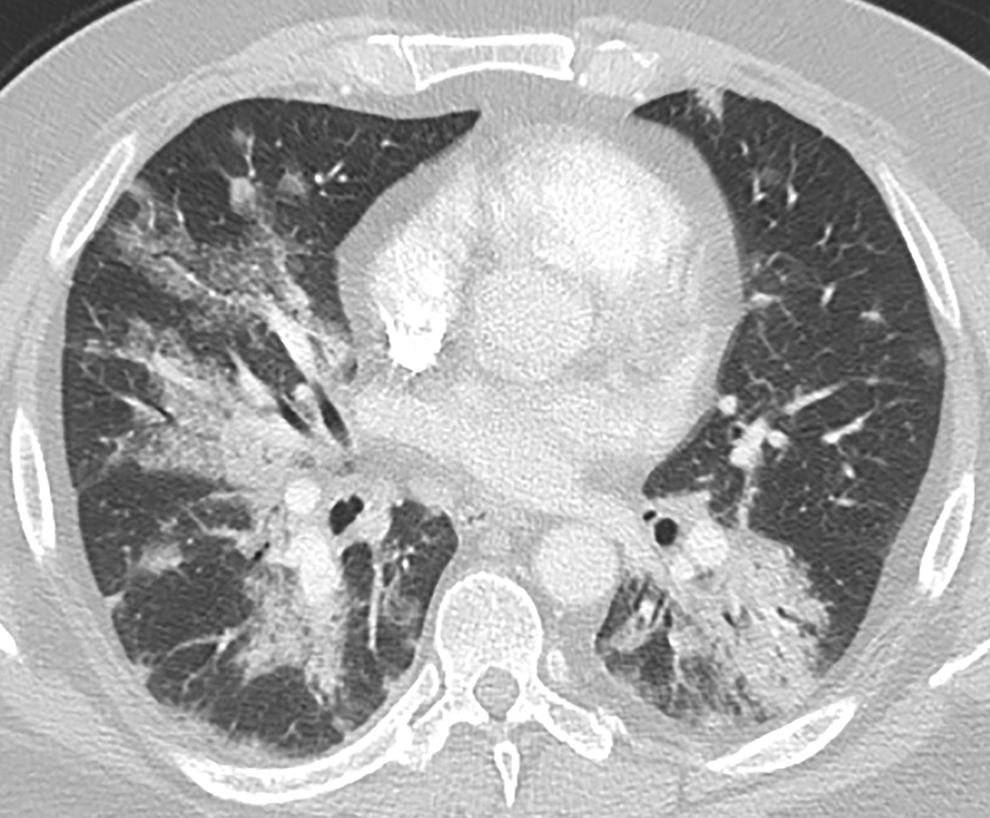
Axial computed tomography (CT) image in a 52-year-old man shows bilateral multifocal consolidation and ground-glass opacities in the middle and lower lung zones, with peribronchovascular distribution. The upper lung zones were also involved (not shown).
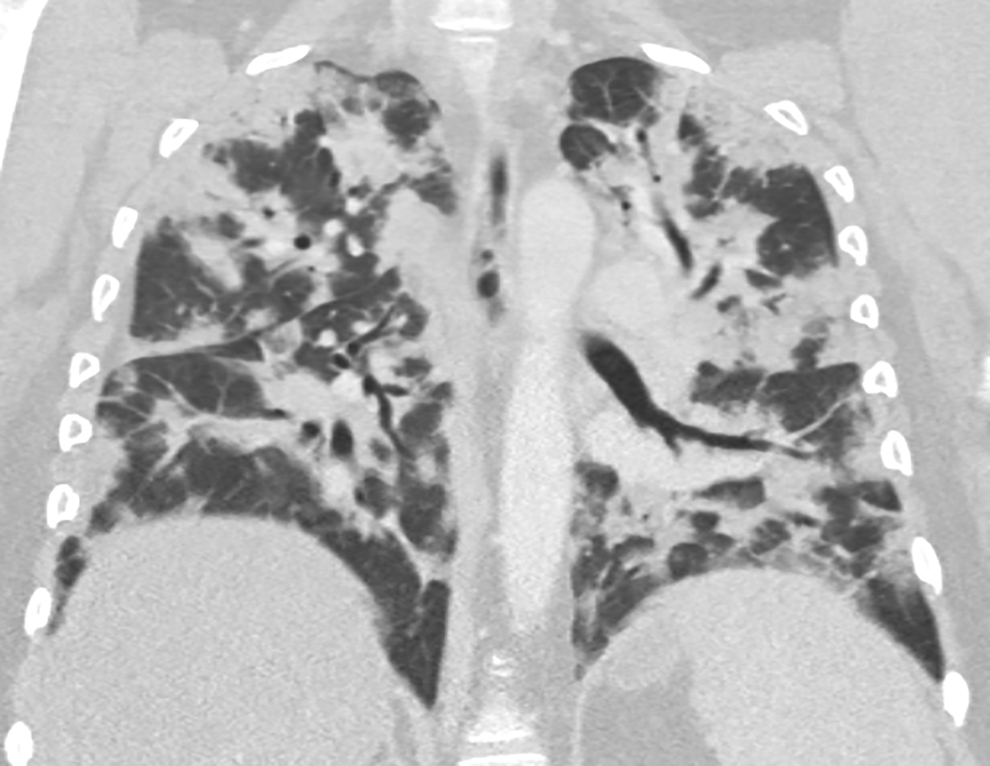
Coronal chest computed tomography (CT) in a 42-year-old woman shows bilateral multifocal nodular and consolidative pattern with both central and peripheral distribution, involving all 6 lung zones.
Twelve (67%) patients in our study were intubated for respiratory failure (Table 2). Four of these patients had chest CT examinations. Eleven (92%) intubated patients had ground-glass opacities, and all (100%) patients had consolidations on their CXR. Examinations demonstrated ground-glass opacities and consolidations in 8 (67%) of the CXR studies and all (100%) of the CT studies of intubated patients. All (100%) intubated patients had bilateral abnormalities and greater than 3 lung zones involvement on CXR and CT scans (Figure 9). In all, middle and lower lung zone abnormalities were seen in 11 (92%) of the x-rays and all (100%) of the CT scans in this group of patients. All (100%) intubated patients had lower lung zone abnormalities on CXR and CT scans. The abnormalities had a peribronchovascular distribution in 10 (83%) intubated patients on CXR and 4 (80%) on thoracic CT. In all, 6 (50%) intubated patients had diffuse radiographic abnormalities and 4 (80%) had multifocal CT involvement.
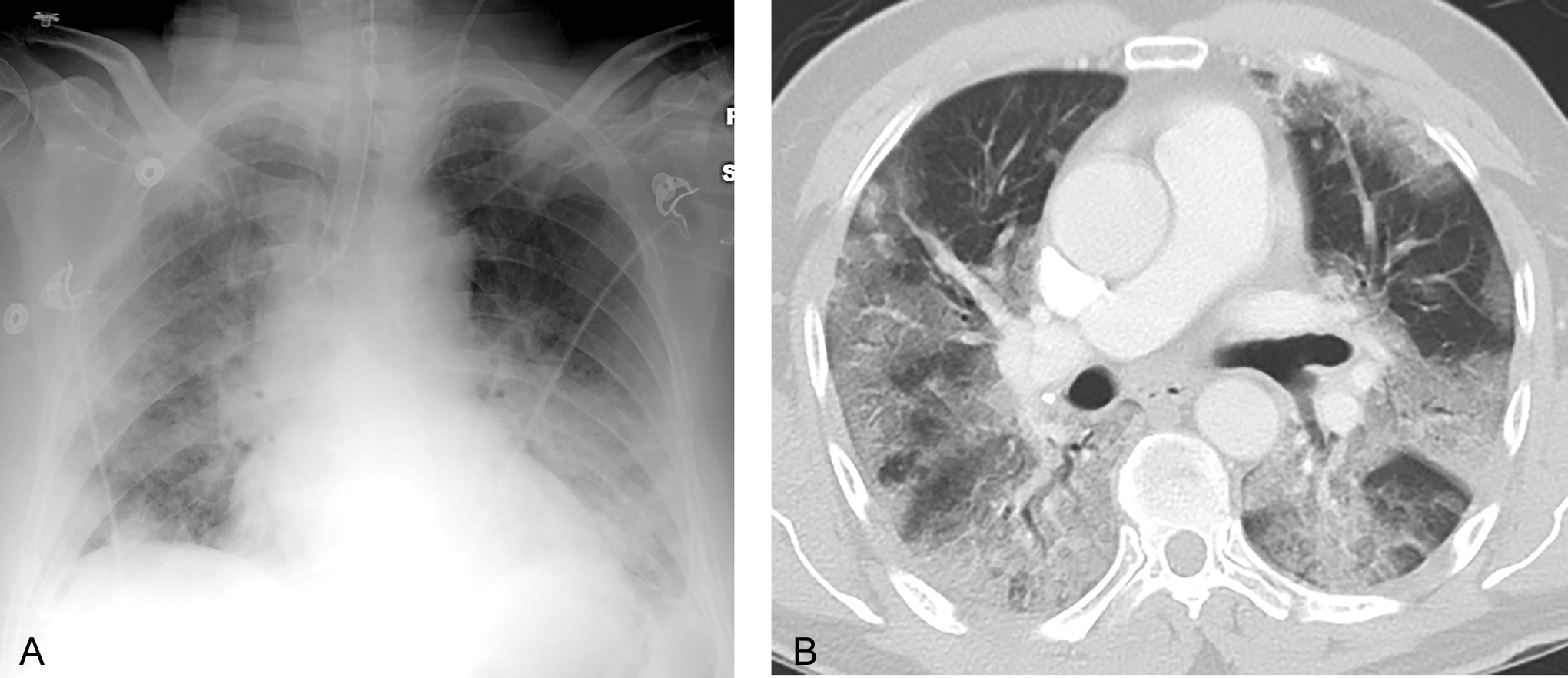
Frontal chest radiograph (A) and axial (B) chest computed tomography (CT) images in a 56-year-old man shows bilateral diffuse ground glass and consolidation, involving all 6 lung zones.
Discussion
Our patient population was admitted to the hospital beginning in the summer months, which is unusual for typical seasonal pneumonia. In contrast to seasonal influenza, which tends to affect patients at the extremes of age, H1N1 influenza affected middle-age patients among our cohort, a pattern that was observed in other studies as well (Table 3). In the United States, 77% of patients with H1N1 infection were less than 50 years of age, 45% of which were non-Hispanic whites and 20% were Hispanic.
2
Seventy-two percent of our study population was Hispanic, deviating from the national trend since UCLA-Olive View Medical Center serves a large, low-income, predominantly Hispanic population. Compared with seasonal influenza, obesity and gastrointestinal symptoms including nausea, diarrhea, and abdominal pain were seen more frequently in our patients with H1N1 influenza. The mean BMI of our patients was 35 kg/m2, with the mean BMI of 38.2 for patients requiring mechanical ventilation, compared to 28.5 for patients not requiring intubation (Table 1). The association between H1N1 influenza and obesity was also observed in other studies, with obesity making up as much as 90% of the study population in some series.
17
Other symptoms of H1N1 in our patients were similar to typical seasonal influenza. These symptoms included cough, shortness of breath, fever, myalgia, and headache. All 12 (67%) patients who required mechanical ventilation met criteria for acute respiratory distress syndrome with Pa
Summary of Studies on CXR and CT Findings of Patients With H1N1 Infection.a
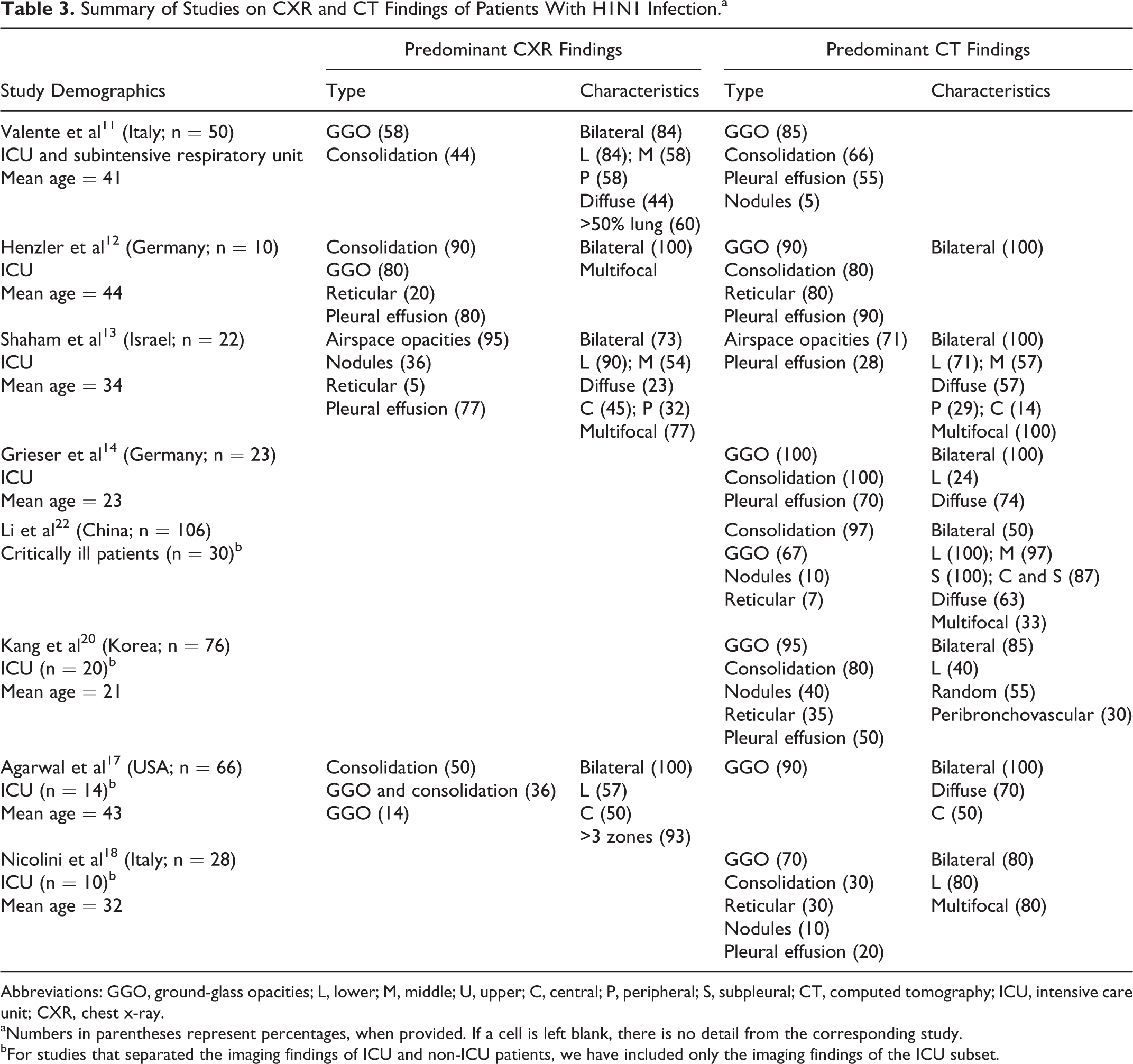
Abbreviations: GGO, ground-glass opacities; L, lower; M, middle; U, upper; C, central; P, peripheral; S, subpleural; CT, computed tomography; ICU, intensive care unit; CXR, chest x-ray.
aNumbers in parentheses represent percentages, when provided. If a cell is left blank, there is no detail from the corresponding study.
bFor studies that separated the imaging findings of ICU and non-ICU patients, we have included only the imaging findings of the ICU subset.
From a broad perspective, plain chest radiographic and CT findings of H1N1 influenza pneumonia are similar to those noted for other viral pneumonias. Radiographic findings of viral pneumonia consist of patchy or diffuse ground-glass opacities with or without consolidation, reticular opacities, and nodules. 10 Computed tomography findings of viral pneumonia consist of centrilobular nodules, ground-glass attenuation with a diffuse or lobular distribution, and segmental consolidation. Centrilobular nodules and ground-glass attenuation with a lobular distribution tend to be seen frequently in influenza pneumonia, whereas pleural effusions are rare. 10 Despite some similarities, there were certain radiographic findings in our patients that set these images apart from those noted in traditional seasonal influenza.
In our study, all 18 patients admitted to the ICU had abnormal CXR and thoracic CT findings. Ground-glass opacities and consolidations were the most common imaging findings in our study, occurring in 89% of CXR and in 100% of CT studies. Nodular opacities were seen in 60% of CT studies. In all, 16 (89%) patients had radiographic abnormalities involving 3 or more lung zones, and all 5 (100%) patients who underwent CT had extensive CT involvement of 4 or more lung zones. The 12 patients who required mechanical ventilation had a higher radiographic incidence of ground-glass opacities (92% vs 83%) and consolidation (100% vs 67%) than the ones that did not require intubation and mechanical ventilation. Mechanically ventilated patients had a combination of ground-glass opacities and consolidation in 67% of patients, compared to only 17% in nonintubated patients. In these patients, the radiographic abnormalities were more likely to be peribronchovascular (83% vs 17%) and diffuse (50% vs 17%). Intubated patients also had more extensive abnormalities involving an average of 5.25 lung zones on CXR, compared to 2.8 lung zones for those not requiring mechanical ventilation. Additionally, all 6 lung zones were noted to be involved on thoracic CT scans. Other studies have found that the pattern and extent of CXR and CT abnormalities may be determining factors in the clinical course of H1N1 infection. 11,14,17 –19
Bilateral lung involvement was seen in greater than 94% of the patients. Abnormal findings had lower (100% on CXR and CT) and middle (67% on CXR, 80% on CT) lung distribution. A majority (78%) of patients had both central and peripheral radiographic and CT findings. Peribronchovascular distribution was present in 61% of patients on CXR and 80% on CT. Imaging abnormalities were multifocal in 56% of CXRs and 80% of CTs and diffuse in 39% of CXRs and 20% of CTs. These imaging abnormalities and patterns of distribution are consistent with other published studies (Table 3). 9,11 –14,18 –22
There are a limited number of studies describing imaging findings exclusively in patients admitted to the ICU. 12 –14 In a study of imaging findings in 50 patients with H1N1 admitted to the ICU or subintensive care, Valente et al described ground glass as the most common CXR (58%) and CT (85%) abnormality, followed by consolidation in 44% of CXR and 66% of CT studies. 11 In all, 84% of CXR abnormalities were bilateral, 86% with lower lung predominance, and 58% peripheral. Of the patients, 60% had more than 50% of lung volume involved, and the extent of the disease correlated with the severity of hypoxia and patient outcome. 11 Henzler et al also identified consolidation and ground-glass opacities as the most common CXR and CT findings of H1N1 pneumonia in mechanically ventilated patients. 12 Consolidation was present in 90% of CXRs and 80% of CTs, while ground-glass opacities were seen in 80% of CXRs and 90% of CTs scans. Ground glass or consolidation was seen bilaterally and multifocally in 100% of patients. 12 Shaham et al described bilateral airspace opacities in 73% of CXRs and 100% of CTs of 22 patients with severe H1N1 infection requiring ICU admission, with abnormalities seen in the lower lobes on 90% of CXR and 71% of CT studies. 13 In a study by Grieser and colleagues, ground-glass opacities and consolidation were seen in all (100%) thoracic CT studies of patients with H1N1 who required mechanical ventilation. 14 Abnormalities were bilateral in 100% of patients, with diffuse distribution in 74% of patients. A CT score based on the extent of ground glass and consolidation had prognostic value in predicting mortality. 14
Other investigators have described imaging findings in the subsets of patients with H1N1 requiring mechanical ventilation or intensive care, often comparing them with less severely affected patients. 18,20,22 In a study of 66 patients with H1N1, Agarwal et al described radiographic and CT abnormalities in 100% of the subset of 14 patients who required mechanical ventilation. 17 Radiographic abnormalities included consolidation in 50% of patients, a combination of ground glass and consolidation in 36%, and ground-glass opacities in 14% of patients; 90% of the patients had a combination of ground glass and consolidation on CT. Bilateral radiographic abnormalities were seen in 100% of patients, with a lower zone distribution in 57% of patients and central zone predominance in 50%. In all, 93% of patients requiring mechanical ventilation had radiographic abnormalities involving more than 3 lung zones, compared to only 10% of patients who were not admitted to the ICU. 17 A high incidence of consolidation and/or ground glass on CT examinations was reported by other investigators, as well as a correlation between multifocal and bilateral distribution with severity of disease and frequency of mechanical ventilation. 20,22 Aviram et al reported a higher CXR incidence of ground-glass opacities and consolidation, with bilateral involvement of 4 or more lung zones, in the subset of patients requiring intensive care, compared with patients who did not require mechanical ventilation. 19 Jartti et al also reported a correlation between the extent of radiographic involvement and disease severity in her study. 21
A reticular pattern was seen in 33% of chest radiographs and 40% of CT scans in our patients, which falls within the range seen in other series. 12,18,22 Nicolini et al described reticular opacities on CT scan in 30% of patients with H1N1 requiring mechanical ventilation, while Kang et al identified a similar pattern in 35% of such patients. 18,20 Henzler et al reported reticular opacities in 20% of CXR; however, in his study increased interstitial markings were seen in 80% of CT. 12
In seasonal influenza pneumonia, pleural effusions tend to be a rare finding. However, small pleural effusions were present in many of our radiographic images (89%). Presence of pleural effusion has been variably reported in radiographic and CT studies of patients with H1N1; however, the incidence of pleural effusion is higher in studies describing subsets of patients requiring intensive care or mechanical ventilation (Table 3). Henzler et al described pleural effusions in 80% of CXR and 90% of CT for H1N1 mechanically ventilated patients, 12 Shaham et al identified pleural effusions in 77% of CXR, 13 while Grieser et al found pleural effusions in up to 70% of CT of such patients. 14 Kang et al reported pleural effusions on CT scans in 50% of patients with H1N1 requiring mechanical ventilation, compared to only 14% of patients treated as outpatients. 20 Despite these reports, the relevance of pleural effusions in our study and other studies of H1N1 influenza is unclear.
Although small airway abnormalities such as centrilobular nodules are frequently seen in seasonal influenza pneumonia, our study did not demonstrate such a pattern, which is consistent with other studies (Table 3). This pattern may be due to propensity of the H1N1 virus to involve the alveolar epithelium more than the bronchiolar epithelium. 11 Some investigators, however, have reported centrilobular nodules in up to 40%, and tree-in-bud bronchiolar pattern in 15%, of patients with H1N1 pneumonia requiring intensive care. 13,19,21 We also did not observe any pulmonary emboli in our patients, although other studies document an increased incidence of pulmonary emboli in up to 36% of patients with H1N1 requiring mechanical ventilation. 17,21 Our finding of ground-glass opacities and consolidation as the predominant radiographic finding in severe H1N1 pneumonia is consistent with other studies investigating this strain of influenza.
In our study, we present the imaging findings of severe cases of H1N1 pneumonia leading to ICU admission. Our study has several limitations. It is a single-center retrospective study and is thus subject to selection bias. Only 28% of our patients had CT scans, which is a more accurate modality for assessing the patterns and distributions we described. Although our study population was relatively large compared to other imaging studies of confirmed patients with H1N1 admitted to ICU, a larger sample would have resulted in greater generalizability of our findings.
In conclusion, severe cases of H1N1 pneumonia requiring ICU admission demonstrate extensive bilateral CXR and thoracic CT abnormalities. The most common radiographic findings are ground-glass opacities and consolidation, followed by reticular pattern. Computed tomography demonstrates additional findings of nodular opacities. Additionally, radiographic findings of severe cases of H1N1 pneumonia are predominantly bilateral and affect mostly the lower and the mid lung fields, usually involving greater than 3 lung zones. Patients requiring mechanical ventilation had a higher BMI and a higher incidence of bilateral, diffuse consolidation in a peribronchovascular distribution on chest radiographs, compared to patients who did not require intubation. Small pleural effusions are present in many of these patients, a finding not uncommonly observed in seasonal influenza pneumonia. In late 2013, the CDC recognized a reemergence of H1N1 as the predominant influenza subtype resulting in significant morbidity and mortality nationwide. The findings presented herein add to the body of literature characterizing radiographic patterns of severe H1N1 pneumonia in patients requiring intensive care, which is now particularly relevant, given the resurgence of this worrisome influenza strain.
Footnotes
Authors’ Note
This manuscript is an original contribution of the authors listed earlier and has not been previously published. It has not been submitted for publication elsewhere. All authors have participated in writing this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.