
Abstract
Purpose:
Current guidelines provide weak recommendations for starting enteral nutrition (EN) in patients with septic shock (on vasopressor support). Outcomes of patients receiving EN in septic shock on vasopressor support have not been well studied. We hypothesize that early trophic EN in mechanically ventilated patients with septic shock is associated with improved outcomes.
Methods:
Single-center retrospective study of mechanically ventilated patients admitted with septic shock to identify patients receiving (1) no EN, (2) <600 kcal/d within 48 hours, and (3) ≥600 kcal/d within 48 hours. Outcomes studied included in-hospital mortality, length of intensive care unit stay (LOS), duration of mechanical ventilation (DOMV), and complications of feeding intolerance.
Results:
Sixty-six patients were identified. In all, 15 received no EN, 37 received <600 kcal/d, and 14 received ≥600 kcal/d EN daily. Median LOS was 12, 5, and 13 days, respectively. The LOS was lower in patients receiving <600 kcal/d when compared to either no EN (P < .001) or those receiving ≥600 kcal/d (P < .001). Median DOMV was lower in patients receiving <600 kcal/d (median 3, P < .001) as compared to no EN (median 7, P < .001) or those receiving ≥600 kcal/d (median 7.5, P < .001). Mortality was not different. There were no significant complications among groups.
Conclusion:
In patients with septic shock, those receiving <600 kcal/d EN within 48 hours had lower DOMV and LOS when compared to those who did not receive EN or those who received ≥600 kcal/d. These observations provide strong justification for prospective evaluation of the effect of early trophic EN in patients with septic shock.
Introduction
Severe sepsis is defined as the systemic inflammatory response syndrome (SIRS) with a source of infection and evidence of end-organ damage. 1 Between 2000 and 2007, the number of admissions in the United States for severe sepsis has increased from 143 per 100 000 to 343 per 100 000 and mortality has decreased from 39% to 27%. 2 The 2004 and 2008 Surviving Sepsis guidelines do not provide recommendations for enteral nutrition (EN). 3,4 In the 2012 guidelines, weak recommendations are made for initiating early nutrition, defined as within 48 hours, in patients with severe sepsis and septic shock. 5 The 2012 guidelines state “no clinical trial has specifically addressed early feeding in septic patients.” 5(p197)
The American Society of Parenteral and Enteral Nutrition also provides a weak (grade E) recommendation to withhold EN in patients with hemodynamic instability requiring significant hemodynamic support. 6 The guidelines state “EN intended to be infused into the small bowel should be withheld in patients who are hypotensive (mean arterial blood pressure <60 mm Hg), particularly if clinicians are initiating use of vasopressor agents or escalating the dose of such agents to maintain hemodynamic stability.” 6(p284)
The lack of a strong recommendation results in our supposition of a heterogeneity in clinical practice regarding the initiation and dose of EN in patients with septic shock. We hypothesized that early trophic EN in mechanically ventilated patients with septic shock would be associated with improved mortality, reduced length of intensive care unit stay (LOS), shorter duration of mechanical ventilation (DOMV), and a lack of significant complications.
Methods
Study Population
We conducted a retrospective study of patients using the Department of Nutrition Services’ database of patients referred for enteral feeding in our medical intensive care unit (MICU). The nutrition services’ database includes all MICU patients referred for EN support. The study was approved by the Medical College of Wisconsin institutional review board (ID#PRO00018076) and met all national guidelines for protection of human studies. We collected data on patients ≥18 years of age between the time period of April 1, 2011, through March 31, 2012, meeting with the following inclusion criteria: (1) MICU admission diagnosis of septic shock requiring vasopressor support and (2) mechanical ventilation on admission or within 24 hours of admission and for >48 hours. We excluded those patients who had a documented contraindication for enteral feeding, including (1) bowel obstruction, (2) protracted ileus, (3) intractable vomiting, (4) major upper gastrointestinal bleed, and (5) bowel surgery within the previous 30 days. These patients were excluded so as not to confound the study. Severe sepsis was defined by consensus criteria as 2 or more criteria of the SIRS with known or suspected infection plus end-organ damage. 1 Septic shock was defined as severe sepsis with persistent hypotension (mean arterial pressure < 70 mm Hg) despite intravenous (IV) fluid resuscitation. 5 All charts were independently reviewed by one of the study authors.
Definition of Variables
We collected 31 variables, including demographic, clinical and biochemical data, duration and quantity of therapies, and outcomes (Table 1). We identified patients who had received EN versus no EN within 48 hours of MICU admission. In patients who had received EN within 48 hours of MICU admission, we a priori separated these patients into those receiving trophic feeding and those receiving full EN. Trophic feeding has been usually defined as 10 to 30 mL/h. 6 Our intensive care unit (ICU) predominantly uses a 1.2-kcal/mL low fiber formula. Using the median trophic feeding rate of 20 mL/h, this correlates with 576 kcal/d. Thus, we considered trophic to be <600 kcal/d (but more than 1 kcal/d). We divided patients into 3 groups: (1) those receiving no enteral feeding, (2) those receiving <600 kcal/d, and (3) those receiving ≥600 kcal/d. Daily kilocalories of EN were collected for the first 7 days of ICU admission.
Baseline Patient Characteristics Based on Stratification of Quantity of Enteral Nutrition.
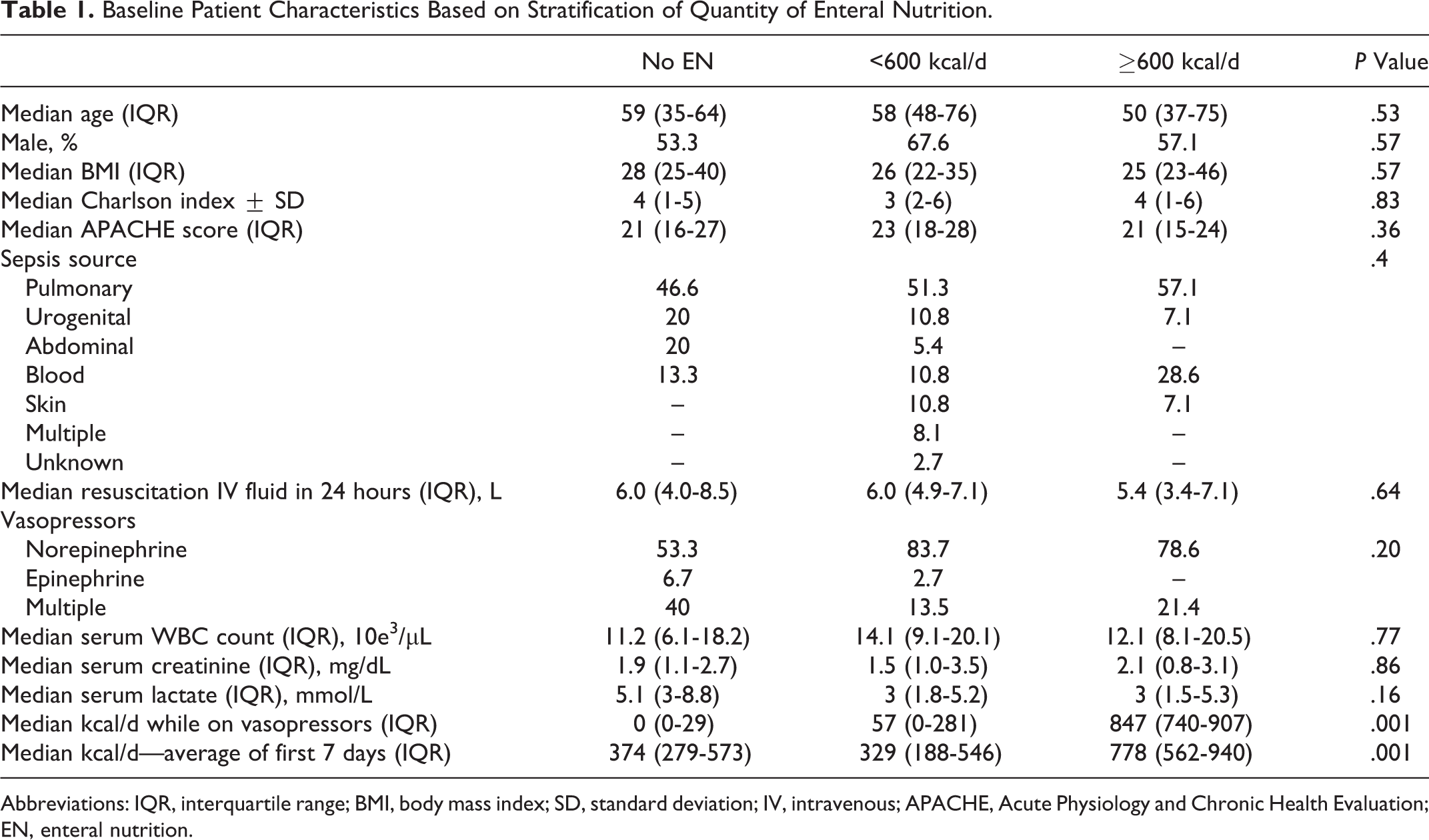
Abbreviations: IQR, interquartile range; BMI, body mass index; SD, standard deviation; IV, intravenous; APACHE, Acute Physiology and Chronic Health Evaluation; EN, enteral nutrition.
Acute Physiology and Chronic Health Evaluation (APACHE) II scores were calculated for the first 24 hours as an assessment of severity of illness. We adapted the Charlson-Deyo comorbidity index to define the burden of preexisting comorbidities. The Charlson-Deyo index uses 17 comorbid conditions with differential weighting, with scores ranging from 0 to 33, and higher scores representing a greater comorbidity burden. 7
Outcomes
Outcomes of interest were in-hospital mortality, DOMV, LOS, and feeding intolerance from EN. Feeding intolerance is a general term indicating intolerance of EN for clinical reasons of diarrhea, vomiting, gastrointestinal bleeding, ileus, and high gastric residual volume. 8 The most feared complications are nonocclusive mesenteric ischemia and nonocclusive bowel necrosis. 9 Aspiration pneumonia was defined as a clinical and radiographic diagnosis of pneumonia with findings of any volume of tube feeding on airway suctioning.
Statistical Analysis
We performed all statistical analyses using STATA IC 11.0 (Stata-Corp, College Station, Texas). Categorical variables were compared using the Pearson chi-square test. We compared mortality of those receiving no enteral feeds to those receiving <600 kcal/d and those receiving ≥600 kcal/d to those receiving <600 kcal/d using Pearson chi-square test. Bonferroni correction was applied for the 2 comparisons. The P value was therefore kept at .025. Continuous variables in Table 1 are presented as median and interquartile range and were compared with the Kruskal-Wallis test since these were not normally distributed.
For Table 2, the outcomes LOS and DOMV were not distributed normally, therefore we log transformed these 2 variables. Comparisons were then made between those receiving no enteral feeds and those receiving ≥600 kcal/d to those receiving <600 kcal/d using both t test and Wilcoxan rank test. The P value was kept at .025 since 2 comparisons were made (Bonferroni correction).
Patient Outcomes Based on Stratification of Quantity of Enteral Nutrition.
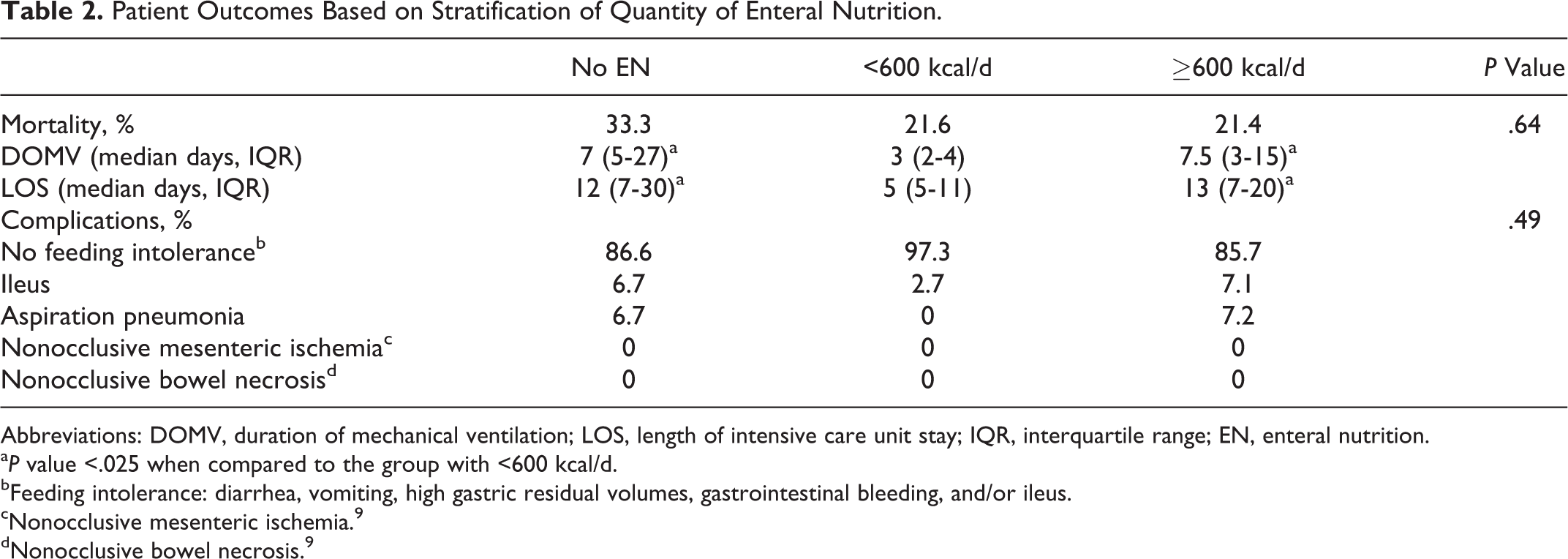
Abbreviations: DOMV, duration of mechanical ventilation; LOS, length of intensive care unit stay; IQR, interquartile range; EN, enteral nutrition.
aP value <.025 when compared to the group with <600 kcal/d.
bFeeding intolerance: diarrhea, vomiting, high gastric residual volumes, gastrointestinal bleeding, and/or ileus.
cNonocclusive mesenteric ischemia. 9
dNonocclusive bowel necrosis. 9
We then performed linear regression on natural log-transformed LOS and DOMV to examine the association of no feeding and >600 kcal/d feeds on LOS and DOMV as compared to trophic feeds. The antilogs of the regression coefficients show the proportion change in LOICU and LOMV and are reported as such. Similarly, multivariable logistic regression model was constructed to examine association of no feeding on mortality when compared to those with <600 kcal/d. A second multivariable logistic regression model was constructed to examine association of >600 kcal/d on mortality when compared to those with <600 kcal/d. The P value was kept at .025 since 2 comparisons were made.
The above-mentioned models were adjusted for age, APACHE II score, Charlson comorbidity index, and amount of fluids received in first 24 hours. We further used propensity score to further adjust for differences in patients who received trophic feeds. We used a logistic regression model to calculate the likelihood that a person would undergo trophic feeding than otherwise. We included age, gender, body mass index (BMI), fever, total fluids received in first 24 hours, type of vasopressor used, the highest dose of vasopressor on the first day of MICU admission, APACHE II score, Charlson comorbidity index, and highest serum lactic acid on the first day of MICU admission. We then divided the propensity score into quintiles and used it as a continuous variable in the previously developed model.
Results
Between April 1, 2011, and March 31, 2012, there were 2413 admissions to the MICU. Of these, 490 were referred to nutrition services for EN. Of the 490 patients, 424 were excluded due to failure to meet the criteria of septic shock and/or mechanical ventilation. Sixty-six patients were ultimately included for analysis (Figure 1).
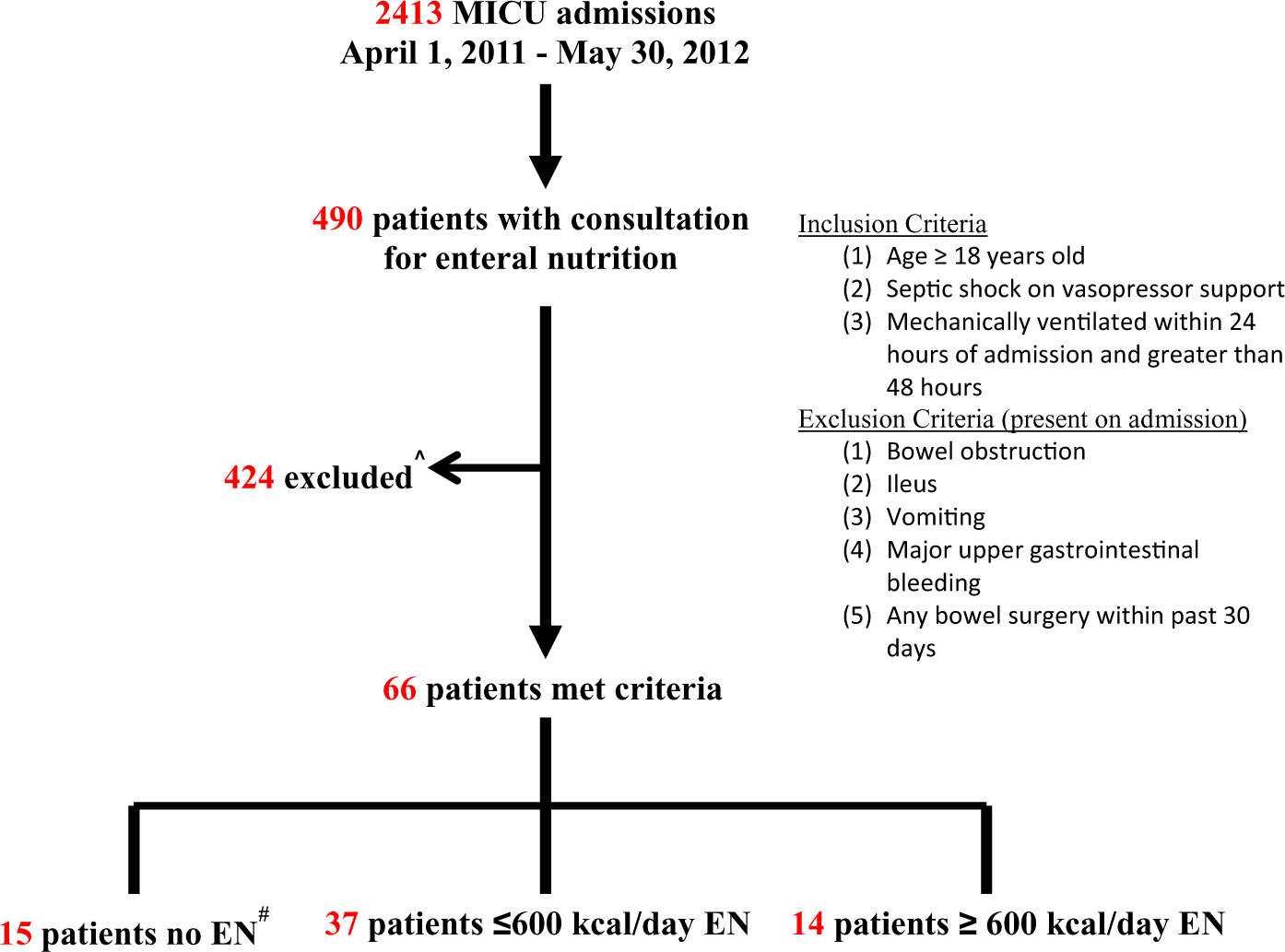
Overview of patient selection. ^ indicates did not meet inclusion and/or met exclusion criteria; #, enteral nutrition (within 48 hours).
Fifteen patients received no EN within 48 hours of MICU admission. In all, 37 patients received <600 kcal/d within 48 hours of admission and 14 patients received ≥600 kcal/d within 48 hours of admission.
Demographic and Clinical Characteristics
The 3 cohorts were similar with respect to age, gender, mean Charlson index, and APACHE II scores. The mean BMI in the <600 kcal/d group was not different as compared to that of the no feeding group or ≥600 kcal/d group. A pulmonary source was the predominant cause of sepsis in all groups (Table 1).
Processes of Care
The no EN group received a median of 0 kcal while on vasopressors, the <600 kcal/d group received a median of 57 kcal/d while on vasopressors, and the ≥600 kcal/d group received a median of 847 kcal/d while on vasopressors. The no EN group received EN after 48 hours. The median quantity of EN received by the no EN group and <600 kcal/d group was 374 and 329 kcal/d, respectively, over the first 7 days.
Norepinephrine was the most commonly used vasopressor in all groups (Table 1). Multiple vasopressors were used in 40% of the no EN group and in 21.4% of the ≥600 kcal/d group, compared to 13.5% of the <600 kcal/d group.
Among the patients who received EN, 86% in the <600 kcal/d group and 36% in the ≥600 kcal/d group had an oral-gastric tube as the route of EN. Overall, >50% of both groups were fed into an end-gastric tube.
The median volume of IV fluids received in the first 24 hours of sepsis diagnosis was 6.0 L in the <600 kcal/d group compared to 6.0 and 5.4 L in the no EN and ≥600 kcal/d groups, respectively. The choice of vasopressor, route of EN, and amount of IV fluid received were not statistically different between groups.
Outcomes
In-hospital mortality was 33.3%, 21.6%, and 21.4% for no EN, <600 kcal/d, and ≥600 kcal/d groups, respectively (Table 2). These values were not statistically different. On adjusted analysis, the mortality was not significantly different between <600 kcal/d and the other 2 groups.
Median LOS (Table 2) was 12, 5, and 13 days, respectively. On adjusted analysis, the LOS was lower in patients receiving <600 kcal of EN/d when compared to either no EN (P < .001) or those receiving ≥600 kcal/d (P < .001). Median DOMV (Table 2) was lower in those receiving <600 kcal/d (median 3) as compared to those receiving no EN (median 7, P < .001) or those receiving ≥600 kcal (median 7.5, P < .001).
On adjusted analysis, the LOS was longer by 2.33 times (95% confidence interval [CI] 1.36-3.97, P = .003) in the no EN group and 1.58 times (95% CI 1.28-1.97, P < .001) in those receiving ≥600 kcal/d when compared to those receiving <600 kcal/d. Similarly, the DOMV was 2.41 times longer (95% CI 1.20-4.08, P = .014) in the no EN group and 1.49 times (95% CI 1.14-1.95, P = .004) in those receiving ≥600 kcal/d when compared to those receiving trophic feeds.
Feeding tolerance was documented in 87%, 97%, and 86% of the no EN, <600 kcal/d group, and >600 kcal/d group, respectively. Ileus associated with enteral feeding was similar between the 3 groups. Nonocclusive mesenteric ischemia was absent in all groups. There were no aspiration pneumonia events in the <600 kcal/d group. Aspiration pneumonia was found in 6.7% and 7.2% in the no EN and >600 kcal/d groups, respectively.
Discussion
Our study demonstrates a decreased LOS and DOMV among mechanically ventilated patients with septic shock in those receiving <600 kcal/d within 48 hours, as compared to those receiving no EN or ≥600 kcal/d within 48 hours of MICU admission. Importantly, we cannot determine the reason some patients with septic shock on vasoactive support were started on EN, while in others it was withheld. Our observation of heterogeneity in clinical practice that leads us to speculate the decision to withhold EN in this population is based on a paucity of data in this particular population.
Large randomized controlled trials of EN support have excluded patients on “high” doses of vasoactive support. 10,11 Rice et al performed a randomized controlled trial of trophic versus full feeding in critically ill patients. 10 They found similar benefits of early trophic feeding as compared to full EN support; however, only 35% and 41% of trophic and full EN groups, respectively, received vasopressors. 10 In a subsequent study of EN in acute lung injury (EDEN), 37% and 39% in the trophic and full feeding groups, respectively, were treated with vasoactive support. 11 Notably, both studies excluded patients requiring “high” doses of vasoactive support (eg, norepinephrine >30 μg/min). 10,11 A secondary analysis of the International Nutrition Survey evaluated the effect of energy and protein intake given by EN on clinical outcomes in a large cohort of critically ill patients with sepsis receiving only EN. 12 The analysis suggests calorie and protein delivery closer to recommended amounts by EN in the early phase of ICU stay were associated with more favorable outcomes; however, the study included a heterogenous population of medical and surgical patients; and data on the type, frequency, and dosing of vasoactive support were not available. 12
Furthermore, without guidelines and given theoretical reasons to withhold EN (discussed subsequently), ICU clinicians have widely varying practices with respect to enteral feeding patients with this condition. The current recommendations to withhold EN in patients with shock are based on 2 observations, both of which could increase risk of intestinal and vital organ ischemia–reperfusion injury in a patient with hypotension. First, blood flow to the small bowel is such that the artery and vein of the villus run parallel, but their blood flows are in opposite directions. This anatomical arrangement allows countercurrent exchange of oxygen from the artery to the vein along the course within the villus. The result is a descending gradient of tissue P
The second observation that gives rise to a theoretical objection to enteral feeding in a patient with hypotension on vasopressors is the fact that feeding may lead to a “steal” phenomenon by splanchnic circulation without an increase in total blood flow. 14
Despite these theoretical concerns, animal and human studies show conflicting results. Rats that provided luminal nutrients during hypotension exhibited increased jejunal hypoxia and mucosal permeability as well as decreased glucose absorption and metabolism. 15 Clamping of the superior mesenteric artery established intestinal ischemia prior to institution of enteral nutrients. 15 Physiology in this model is different than feeding a patient with risk factors for, but not established intestinal ischemia (since gastrointestinal ischemia occurs when blood flow is <50% the basal value).
Human studies of cardiogenic shock have demonstrated tolerance to EN. 16,17 Revelly and colleagues evaluated the hemodynamic and metabolic adaptations to EN. Nine cardiothoracic surgery patients requiring hemodynamic support received isoenergetic postpyloric EN. 16 Enteral nutrition increased cardiac index, splanchnic blood flow, and metabolic responses demonstrating that nutrients were utilized. 16 Berger and colleagues demonstrated tolerance of >1200 kcal/d EN in 70 postcardiac surgery patients with circulatory failure requiring vasoactive support. 17
These latter studies provide observations in cardiogenic shock where a reduction in splanchnic blood flow occurs in proportion to a reduction in cardiac output, putting the patient at risk for splanchnic ischemia. In septic conditions, the impact of blood flow reduction is unpredictable. 18 The addition of norepinephrine could lead to hepatosplanchnic vasoconstriction, placing the small bowel at risk for ischemia, but this mechanism might be off-set by norepinephrine and increases venous return by constriction of venous capacitance beds, thus increasing cardiac output. 19
Our data indicate the <600 kcal/d group received more IV fluid resuscitation in the first 24 hours (as compared to the ≥600 kcal/d group), and perhaps adequate fluid resuscitation maintains >50% basal value flow and oxygen delivery to the small bowel, which attenuates the risk of intestinal ischemia by maintaining adequate oxygen delivery to small bowel villus. An intact villus preserves intestinal epithelium, maintains brush border enzyme activity, maintains barrier function to enhance immune function, and preserves tight cell junctions to prevent bacterial translocation. 20
Human studies of EN in septic shock are limited. Rai and colleagues retrospectively studied 43 patients with sepsis (33 with shock) to determine the adequacy of EN in this population. 21 Enteral nutrition was initiated at a mean of 1.3 days to 33 patients in shock with no difference in ICU or hospital mortality. The 33 patients with shock did have a larger mean residual volume, but this did not affect the success of feeding, and complications were not reported. 21 Khalid and colleagues demonstrated improved ICU and hospital survival in the sickest of medical ICU patients (ie, those on multiple vasopressors) who had early EN as compared to those with late EN. 22 In a secondary analysis of the Intensive Insulin Therapy and Pentastarch Resuscitation in Severe Sepsis trial, 353 patients with severe sepsis or septic shock were evaluated to analyze the effect of 3 nutritional strategies. 23 Those receiving EN alone had improved 90-day mortality. 23
Apart from the timing of EN, quantity of EN may be important. Rokyta and colleagues demonstrated the initiation of low-dose postpyloric EN in ICU patients with severe sepsis led to the parallel increase in systemic and hepatosplanchnic blood flow and hepatosplanchnic energy metabolic, oxygen kinetics, and gastric mucosal energy did not deteriorate during EN. 24 Using a definition of trophic feeding of 10 to 30 mL/h, delivery of 1.0 kcal/mL as opposed to a 1.5-kcal/mL formula would provide a substantially different daily caloric intake. Our small observational study suggests that <600 kcal/d as a trophic value is associated with improved outcomes and no increased risk of complications secondary to EN.
We acknowledge several limitations to our study. First, our study is limited by the small sample size, especially small numbers in the cohort with ≥600 kcal/d enteral feeding. These limitations preclude us from estimating the true width of CIs surrounding our estimates of mortality risk. Second, due to the retrospective nature of our study, we are unable to investigate the mechanisms of our findings. Third, although we used physiological and biochemical data to adjust for severity of illness, it is possible residual confounding factors reflecting unmeasured severity of illness directed clinician’s decisions to feed or withhold nutrition. Specifically feeding might not have been initiated in patients who were the sickest or had reasons for withholding that are not reflected in severity of illness scores. Along the same lines, other unmeasured imbalances amid cohorts may have confounded our results. Particularly, use of prokinetic agents and/or opiates may interfere with gastrointestinal intolerance to EN. Although our cohort did not include patients on PN, we are not able to quantify calories obtained from other sources such as propofol or dextrose infusions. Next, patients were excluded based on inclusion and exclusion criteria for the purpose of not introducing confounding risk factors. However, there is potential in limiting the external validity of our study to other shock states. The BMI of our population was high (means of 33, 28, and 33 for no EN, <600, and ≥600 kcal/d, respectively), further limiting external validity. Finally, whether our observations apply equally to surgical patients is also unclear. Our results should not be extrapolated to patients who are not mechanically ventilated, have bowel ischemia, or have abnormal bowel motility at presentation.
Our study demonstrates that administration of <600 kcal/d compared to no EN and ≥600 kcal/d is associated with a shorter LOS and DOMV without an increased risk of complications in patients with septic shock requiring mechanical ventilation. Our data also document heterogeneity in clinical practice regarding the provision and quantity of EN in mechanically ventilated patients with septic shock, perhaps a consequence of the heterogeneity and lack of strong guidelines observed in clinical guidelines. Thus, current guidelines may underestimate the tolerability or benefit of EN of patients with septic shock. Prospective research in larger numbers of patients is needed to provide evidence on the potential of trophic feeding in mechanically ventilated patients with septic shock to favorably affect outcomes and to explore mechanisms underlying the impact of feeding on clinical outcomes in patients with this disorder.
Footnotes
Authors’ Note
Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the National Center for Research Resources and The National center for Advancing Translational Sciences, National Institute of Health, through Grant Number 8UL1TR000055.