
Abstract
Objective:
The process of controlled donation after circulatory death (cDCD) is strongly connected with the process of withdrawal of life-sustaining therapy. In addition to impacting cDCD success, actions comprising withdrawal of life-sustaining therapy have implications for quality of palliative care. We examined pilot study data from Canadian intensive care units to explore current practices of life-sustaining therapy withdrawal in nondonor patients and described variability in standard practice.
Design:
Secondary analysis of observational data collected for Determination of Death Practices in Intensive Care pilot study.
Setting:
Four Canadian adult intensive care units.
Patients:
Patients ≥18 years in whom a decision to withdraw life-sustaining therapy was made and substitute decision makers consented to study participation. Organ donors were excluded.
Interventions:
None.
Measurements and Main Results:
Prospective observational data on interventions withdrawn, drugs administered, and timing of life-sustaining therapy withdrawal was available for 36 patients who participated in the pilot study. Of the patients, 42% died in ≤1 hour; median length of time to death varied between intensive care units (39-390 minutes). Withdrawal of life-sustaining therapy processes appeared to follow a general pattern of vasoactive drug withdrawal followed by withdrawal of mechanical ventilation and extubation in most sites but specific steps varied. Approaches to extubation and weaning of vasoactive drugs were not consistent. Protocols detailing the process of life-sustaining therapy withdrawal were available for 3 of 4 sites and also exhibited differences across sites.
Conclusions:
Standard practice of life-sustaining therapy withdrawal appears to differ between selected Canadian sites. Variability in withdrawal of life-sustaining therapy may have a potential impact both on rates of cDCD success and quality of palliative care.
Keywords
Introduction
Donation after circulatory death (DCD) has reemerged as an opportunity to improve organ donation rates. Some estimate DCD could increase the number of potential donors by up to 30%. 1 –4 Controlled DCD (cDCD) following an expected cardiac arrest (also known as Maastricht category III DCD) can occur in critically ill patients after a decision to withdraw life-sustaining therapy. 5 The process and actions of withdrawal of life-sustaining therapy influence whether consented cDCD donors actually proceed to organ procurement. In the period between the start of life-sustaining-therapy withdrawal and the declaration of death, organs are deprived of adequate oxygenation due to gradual cessation of circulation (warm ischemic time). A long warm ischemia time can be detrimental to organ graft survival, and most cDCD protocols focus on minimization of this time period. 6,7 The maximum acceptable warm ischemia time is debated; protocols set a cutoff of 1 to 3 hours. 6 –9 Up to 40% of potential cDCD donors die beyond this window and fail to donate, a loss for grieving families and potential transplant recipients. 8 Recent research suggests physiologic characteristics (e.g., heart rate, blood pressure) during the dying process may also directly impact functionality of recovered organs. 10 Withdrawal of life-sustaining therapy can impact timing of death as well as the physiologic profile of the donor during the dying period.
Withdrawal of life-sustaining therapy is also important for quality patient care in the intensive care unit. The withdrawal of life-sustaining therapy process (removal of invasive treatments, sedation/analgesia) is intended to provide comfort to dying patients. For consented organ donors, the withdrawal of life-sustaining therapy process has the additional role of influencing cDCD eligibility. Administering sedation/analgesia for relief of pain and suffering has been deemed ethically acceptable during withdrawal of life-sustaining therapy but administering sedation/analgesia to achieve successful organ donation has not. Efforts to avoid perceptions of hastening death for the purposes of organ donation can lead to changes in how life-sustaining therapies are withdrawn and how much sedation/analgesia is provided for organ donors, 11,12 contributing to prolongation of the dying process and its associated suffering. An exploration of how quality end-of-life care can be integrated with optimal cDCD eligibility has not been undertaken.
The objective of this study was to describe and analyze actions taken during the process of withdrawal of life-sustaining therapy, as it occurred in selected Canadian intensive care units. The objective of this study was to (1) describe processes of withdrawal of life-sustaining therapy as they occurred in participating Canadian adult intensive care unit sites and (2) explore whether any common pattern of life-sustaining therapy withdrawal existed between or within participating sites.
Materials and Methods
The Determination of Death Practices in Intensive Care Units (DDePICt) Pilot Study involved prospective, continued monitoring of patients undergoing withdrawal of life-sustaining therapies in the intensive care unit. 13 The primary objective of the study was to determine the feasibility of collecting physiologic data during the dying process. The study was reviewed and approved by the local Research Ethics Board. Patients’ whose families or substitute decision makers signed written consent allowing their participation had cardiovascular and respiratory monitoring continued for 30 minutes following the declaration of death. Vital sign data for a 60-minute period (30 minutes prior to and 30 minutes following declaration of death) were recorded and analyzed. During withdrawal of life-sustaining therapy, detailed information was recorded on number, type, dosing, and route of all drugs administered and withdrawn and timing and method of ventilation withdrawal. Processes of withdrawal of life-sustaining therapy were not altered in any way for the observational study. Patients who were to become organ donors were not eligible to participate. A total of 5 centers (1 pediatric and 4 adult intensive care units) participated in the pilot study.
Data Analysis
Permission was granted from the local Research Ethics Board to use data collected for the pilot study in a secondary analysis. Data were available from all 4 participating adult intensive care unit sites. Deidentified patient data were obtained in an SPSS data set, which was modified to exclude all patients <18 years. Pediatric patients were excluded due to differences in life-sustaining therapy withdrawal processes in pediatric intensive care units.
A descriptive analysis was performed using relevant variables; means, medians, and standard deviations were calculated. Univariate comparisons of means were not completed due to small sample size. Data were analyzed in six categories, namely, patient characteristics, artificial airway management, weaning of ventilation, vasoactive drug weaning, sedation/analgesia, and timing of events. Data were analyzed and compared by site. Timing data were analyzed using Microsoft Excel. All other calculations were done using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp. Armonk, New York).
Copies of withdrawal of life-sustaining-therapy protocols were obtained to further explore practice variations between hospitals. Protocols detailing processes of withdrawal of life-sustaining therapy were compared along 13 characteristics covering their content, order of steps of life-sustaining-therapy withdrawal, and physical characteristics including document length and use of checklists (see Appendix A).
Statistical significance was not calculated for any comparisons made in this analysis due to sample size limitations and the descriptive goals of the study.
Results
A total of 37 patients at 4 adult intensive care unit sites were identified in the data set as ≥18 years. One patient was excluded due to missing data (patient died before withdrawal of life-sustaining-therapy processes began). A total of 36 adult patients were included in the final analysis (see Appendix B).
Patient Demographics and Characteristics Prior to Withdrawal of Life-Sustaining Therapy
Patients included in the pilot study are described in Table 1. Patient age, sex, and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores did not seem to differ substantially between sites. Patients’ median level of consciousness, measured using the Glasgow Coma Scale, appeared dissimilar between sites. All participating intensive care units were located at university teaching hospitals. Two sites were neurotrauma centers; 2 sites were medical/surgical.
Patient Demographics.
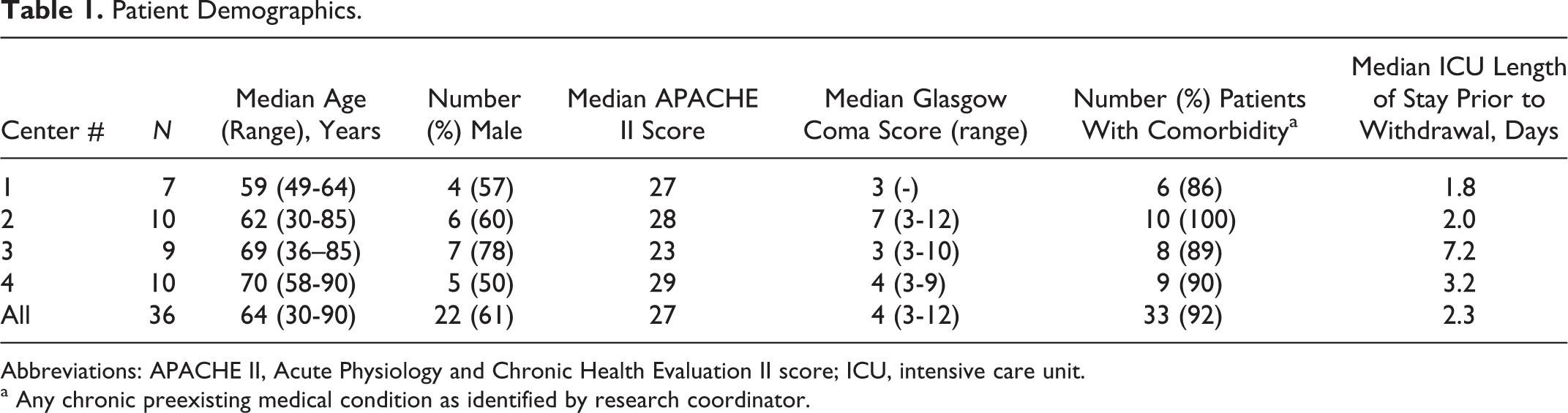
Abbreviations: APACHE II, Acute Physiology and Chronic Health Evaluation II score; ICU, intensive care unit.
a Any chronic preexisting medical condition as identified by research coordinator.
Prior to withdrawal of life-sustaining therapy, all patients (35, 97%) had an artificial airway (endotracheal intubation) and were mechanically ventilated. One (3%) patient was supported with noninvasive mechanical ventilation. All patients were administered inspired oxygen (mean FiO2 range 32%-55%). Prior to withdrawal of life-sustaining therapy, 12 (33%) patients were receiving vasoactive drugs to maintain blood pressure, ranging from 0% of patients at 2 sites to 70% of patients at 1 site (see Appendix C). Patients receiving vasoactive medications had a median of 1 vasoactive drug infusion. Thirty (83%) patients were administered sedation and/or analgesia just before withdrawal of life-sustaining therapy. The percentage of patients on any sedation/analgesia just prior to withdrawal of life-sustaining therapy varied between sites from 29% to 100%.
Airway Management
Of 36 intubated and mechanically ventilated patients, 27 (75%) had their artificial airway removed (extubation) during withdrawal of life-sustaining therapy (see Appendix D). Of the 27 patients, 15 (56%) were extubated immediately at the start of withdrawal of life-sustaining therapy. Of the 27 extubated patients, 19 (70%) had both mechanical ventilation and endotracheal tubes withdrawn without any weaning process. Median time to extubation was 0 minutes in 2 of the sites, and ranged from 46 to 60 minutes in the other 2 study centers.
Mechanical Ventilation and Oxygen Weaning
Of 36 intubated and mechanically ventilated patients, 15 (42%) had inspired oxygen percentage reduced during life-sustaining therapy withdrawal as part of a ventilation weaning process. Patterns of ventilation weaning and extubation (eg, how inspired oxygen percentage was reduced; whether protected airway was maintained) appeared to vary between sites. A table of strategies of mechanical ventilation weaning is available in Appendix E.
Withdrawal of Vasoactive Drugs
Twelve (33%) patients had vasoactive drug infusions just prior to the initiation of life-sustaining therapy withdrawal. Of these patients, 3 (25%) had the drugs withdrawn immediately when withdrawal of life-sustaining therapy began. Two study sites weaned vasoactive drugs from the remaining nine patients, with an average of 2 dose reductions before drugs were completely stopped. Median length of time for weaning vasoactive drugs was 30 minutes at both sites. While 1 site always weaned vasoactive drugs using at least 1 step down before cessation, the other site seemed to fluctuate between an abrupt stop and a gradual decrease.
Order of Withdrawal of Life-Sustaining Therapies
All 12 patients receiving vasoactive drugs just prior to initiation of life-sustaining-therapy withdrawal had these drugs withdrawn before or at the same time mechanical ventilation was removed. One site withdrew all interventions, including vasoactive drugs and all ventilation/oxygen support, simultaneously at the start of life-sustaining therapy withdrawal. In contrast, another site employed a gradual, staggered withdrawal process (weaning of vasoactive drugs followed by weaning of oxygen and ventilation mode, and final extubation) for all patients. The remaining 2 sites utilized a combination of simultaneous and staggered processes of withdrawal of life-sustaining therapy.
Administration of Analgesia and Sedation During Withdrawal of Life-Sustaining Therapy
Thirty (83%) patients in the pilot study received some form of analgesia/sedation during withdrawal of life-sustaining therapy, which varied by site (Table 2). Twenty-five (69%) patients who received analgesia/sedation during withdrawal of life-sustaining therapy were given increased doses or boluses compared to amounts received prior to life-sustaining-therapy withdrawal. Median time to first drug increase ranged from 5 to 94 minutes from the start of life-sustaining-therapy withdrawal. Drugs most commonly administered were midazolam, given to 22 (73%) patients, and fentanyl, given to 12 (40%) patients. Morphine was administered to 11 (37%) patients during life-sustaining therapy withdrawal. Other drugs administered during withdrawal of life-sustaining therapy included propofol, given to 2 (7%) patients, and lorazepam, given to 1 (3%) patient. One (3%) patient was given a glycopyrrolate injection to reduce secretions. No other drugs were administered during withdrawal of life-sustaining therapy. Six (17%) patients did not have analgesia/sedation administered during withdrawal of life-sustaining therapy. Of the 6, 5 (83%) had severe neurological injuries, all had a GCS score of 3, and 4 (67%) died less than 1 hour after the start of withdrawal of life-sustaining therapy. All six (100%) patients who did not receive any further analgesia/sedation either just prior to or during the process of life-sustaining therapy withdrawal died within 2 hours of initiation of this process.
Administration of Analgesia/Sedation During Withdrawal of Life-Sustaining Therapy.

Time to Death after Initiation of Withdrawal of Life-Sustaining Therapy
Median time to death for all sites was 1 hour and 51 minutes. Longest time to death was 2 days, 1 hour and 20 minutes, and shortest was 13 minutes (Table 3). Median times from initiation of withdrawal of life-sustaining therapy to death varied between sites. Less than half (42%) of all patients died ≤1 hour after initiation of withdrawal of life-sustaining therapy. At 2 hours after commencement of withdrawal of life-sustaining therapy, 53% of all patients had died.
Time From Withdrawal of Life-Sustaining Therapy to Death.

Withdrawal of Life-Sustaining Therapy Protocols
Of the 4 study centers, 3 (75%) used a protocol detailing the process of life-sustaining therapy withdrawal for nondonor patients (see Appendix F). One site had a protocol for cDCD patients only. This protocol was excluded, as none of the patients enrolled in this pilot study were organ donors. Included protocols varied in their descriptions of what the first action of life-sustaining therapy withdrawal should be, although all 3 began with a change to patients’ drug infusions/doses. Of the 3 protocols, 2 included statements explaining the absence of a dose limit for analgesia/sedation during life-sustaining therapy withdrawal. Of the 3 protocols, 2 described physical symptoms bedside staff might look for to determine whether increases in analgesia/sedation are needed. While 2 protocols outlined steps for ventilation withdrawal leading to extubation, 1 center’s protocol left ventilation-weaning strategies entirely up to treating physicians. All 3 protocols considered cessation of enteral feeding, laboratory testing, and medical monitoring devices part of the life-sustaining therapy withdrawal process. One protocol included an explanation of decision-making and family discussions surrounding withdrawal of life-sustaining therapy. Protocols ranged from 1 to 5 pages in total length and featured a combination of checklists and blocks of text.
Discussion
This analysis of 36 adult intensive care unit patients enrolled in the DDePICt Pilot Study provides a unique exploration of withdrawal of life-sustaining therapy practices in select Canadian intensive care units as they occur in nondonors. While previous studies describe general processes of life-sustaining therapy withdrawal in adult patients, our analysis includes more detailed observations of steps of withdrawal of mechanical ventilation, extubation, and administration and weaning of vasoactive drugs and analgesia/sedation.
Observed processes of life-sustaining therapy withdrawal involved cessation of vasoactive drugs, withdrawal of mechanical ventilation, removal of artificial airway, and increases in analgesia/sedation. The order and degree to which each life-sustaining therapy was withdrawn over time differed between sites. In general, vasoactive drugs and mechanical ventilation were withdrawn or reduced at a similar time, a pattern identified in surveys of physicians’ withdrawal of life-sustaining therapy practice. 14,15 The majority (83%) of enrolled patients received some form of analgesia and/or sedation during life-sustaining therapy withdrawal, similar to observational studies of comparable populations. 16 –19 Type, amount, and timing of drug titrations seemed to vary between sites. Just over half (53%) of all patients died within 2 hours of initiation of withdrawal of life-sustaining therapy, consistent with other studies in nonorgan donor patients where 28% to 55% die within 1 to 2 hours of initiation of life-sustaining therapy withdrawal. 17,20 Although there seemed to be a trend between administration of analgesia/sedation and increased time to death, no such conclusions can be made with such a small sample size. Median times from life-sustaining therapy withdrawal to death seemed to remain comparable between sites regardless of the pattern of therapy withdrawal. Of the 4 sites, 3 had protocols outlining procedures of life-sustaining therapy withdrawal for nondonor patients.
While sites appeared comparable in terms of patients’ illness severity, sex, and length of intensive care unit stay, intensity of patient management prior to withdrawal of life-sustaining therapy was dissimilar between sites. This may reflect inclusion of neurotrauma centers in the participating sites. Neurologically injured patients require different approaches to life-sustaining therapy due to their hemodynamic stability and need for airway protection. 21
We found contrasting patterns in the degree of staggered versus simultaneous withdrawal of life-sustaining therapies, number and types of drugs used, and methods of ventilation withdrawal. Cook et al 22 found similar levels of variability between sites in a survey of intensive care unit staff preferences regarding escalation, withholding, and withdrawing of life-sustaining therapies for 12 written case scenarios. Keenan et al 23 also observed variability in length of time from withdrawal of life-sustaining therapy to death and in vasopressor weaning strategies between community and teaching hospital intensive care units. Other prospective, multicenter observations of the withdrawal of life-sustaining therapy in adult intensive care units have found variation in the degree to which withdrawal of life-sustaining therapy is practiced but have not examined differences in specific steps of extubation, withdrawal of mechanical ventilation, weaning of vasoactive drugs, and administration of analgesia/sedation. 24 –26
A lack of consistency was also observed between protocols of withdrawal of life-sustaining therapy. In this study, 3 of 4 sites used a protocol for withdrawal of life-sustaining therapy in patients who were not organ donors. Specific steps for airway management, ventilation, and vasoactive drug weaning and administration of analgesia/sedation were different between protocols. Similarly, Dunne et al 27 found conflicting practices between guidelines collected at 27 intensive care units in Scotland, of which only 40% had protocols for the withdrawal of life-sustaining therapies available.
Practical elements of life-sustaining therapy withdrawal remain only moderately described in the current literature. Published observational studies of withdrawal of life-sustaining therapy in non-cDCD patients present different operational definitions, time periods, and life-sustaining therapies measured. 23,25,28 Studies of cDCD donation processes and cDCD protocols focus on measuring, predicting, and reducing oxygen deprivation of organs but leave applied details of the withdrawal of life-sustaining therapy process up to individual practitioners and often do not collect detailed data on the process. 29,30
Variability in the practice of withdrawal of life-sustaining therapy has a number of potential consequences. Patterns of life-sustaining therapy withdrawal may impact physiologic and hemodynamic stability of patients during the dying process. According to recent research by Reid et al, 10 physiologic characteristics of patients during withdrawal of life-sustaining therapy may be a more accurate indication of cDCD eligibility than the length of time to death. Variability in withdrawal of life-sustaining therapy patterns between sites could therefore differentially impact cDCD success and quality of procured organs. In addition to its potential impact on cDCD donation success, variability in withdrawal of life-sustaining-therapy processes may impact the quality of the dying process for all patients. With the presently observed variations, it becomes increasingly difficult to adequately assess whether pain control and breathing distress are being consistently and appropriately addressed for all patients.
Although insistence on a “tick-box” standardization approach may not be applicable in all situations, 31 the lack of consistency of a “standard care” withdrawal of life-sustaining therapy between donors and nondonors may also lead to a breakdown of trust between health care practitioners and patients. Without guidelines, physicians may be more likely to “over-” or “underpalliate” patients in a case of donation. Current cDCD protocols recommend that withdrawal proceed with “standard care” life-sustaining therapy withdrawal processes during organ donation, but this is difficult when such orders are variable and in some intensive care units may not be clearly stated. From a patient perspective, trust can be optimized if the highest quality end-of-life care is provided to all patients, regardless of the decision to donate organs. Undoubtedly, the goals of high quality end-of-life care may be different for different patients, depending on their own individual characteristics and choices (e.g., whether they choose to donate organs). The question remains whether, or how, to ensure a general guideline is consistently capable of meeting these goals in a flexible manner consistently respectful of all patients. Further research is needed to determine the relationship of certain life-sustaining therapy withdrawal patterns with physiologic results in the patient (e.g. hypotension and hypoxia) in order to determine the potential impact of the process of withdrawal of life-sustaining therapy on cDCD eligibility and also on the quality of palliative care. More information on how these goals and processes overlap (and whether they can indeed overlap) will be necessary before any common recommendations can be made.
There were limitations to this study including missing information on drug dosing during withdrawal of life-sustaining therapy, missing data on whether intravenous fluids, enteral feeding, dialysis, or laboratory testing was given, stopped, or withheld, and the small sample size which limited our ability to draw firm conclusions. In addition, the pilot study did not collect observations of patient comfort and/or suffering during the dying process, limiting our ability to comment on the social acceptability and quality of deaths resulting from certain patterns of life-sustaining therapy withdrawal. Many of these limitations are due to the retrospective nature of this analysis; initial data collection tools and pilot study design did not take into consideration an exploration of questions surrounding the withdrawal of life-sustaining therapy process. Future studies should strive to consider the process of withdrawal of life-sustaining therapy as an a priori study question and collect observations on objective measures of patient comfort.
Conclusions
Variation in practices of withdrawal of life-sustaining therapy appears to exist between 4 Canadian adult intensive care units included in the DDePICt pilot study. Sites approached and completed withdrawal of life-sustaining-therapy processes differently. Median times to death were comparable, but just under half (47%) of all patients died outside the 2-hour window recommended for organ donors. With current variability in airway management, ventilation weaning, and administration of drugs during withdrawal of life-sustaining therapies, the processes is not consistent between sites, introducing room for improvement for quality of palliation with and without organ donation potential. The impact of withdrawal of life-sustaining-therapy processes on physiologic stability and patient comfort during the dying period requires further exploration if goals of palliation and organ donation are to be optimally aligned.
Footnotes
Appendix A
Appendix B
Appendix C
Appendix D
Appendix E
Appendix F
Acknowledgments
We are grateful to the DDePICt Investigator Group for allowing us access to their data for the analysis performed in this study.
Authors’ Note
Design and implementation of the study, and manuscript development was coordinated at the Children’s Hospital of Eastern Ontario. This study used data from a pilot study supported by grants from the Children’s Hospital of Eastern Ontario Research Institute, Physician’s Services Incorporated, and Canadian Institute for Health Research. Amanda van Beinum participated in the conception, design, analysis, interpretation, drafting, and the critical revising for important intellectual content of this manuscript and that I have seen and approved the final version. Tim Ramsay participated in the conception, design, interpretation, drafting, and the critical revising for important intellectual content of this manuscript and approved the final version. Sonny Dhanani participated in the conception, design, interpretation, drafting, and the critical revising for important intellectual content of this manuscript and approved the final version. Laura Hornby participated in the conception, design, interpretation, drafting, and the critical revising for important intellectual content of this manuscript and approved the final version. Sam Shemie participated in the designing and critical revising of important intellectual content of this manuscript and approved the final version. Roxanne Ward participated in the conception, design, and critical revising for important intellectual content of this manuscript and approved the final version.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sonny Dhanani is chief medical officer of Trillium Gift of Life Network, Ontario. Sam Shemie is medical advisor for deceased donation for Canadian Blood Services; Laura Hornby is a Research Consultant for Canadian Blood Services. For the remaining authors none were declared.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.