
Abstract
Objective:
The objective was to investigate the benefits of supplementing enteral feeding with omega-3 fatty acids in children with mild to moderate sepsis and its effects on acute-phase reactants and interleukin 6 (IL-6) level.
Methods:
The study was a prospective randomized, double-blind, placebo-controlled study from January 2012 to June 2014, which included 2 groups of children with mild to moderate sepsis tolerating enteral feeding. Group A included 60 children supplemented with omega-3 fatty acids, whereas group B included 60 children who received enteral feeding without omega-3 supplementation. Both groups had complete blood pictures, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), serum albumin, and IL-6 before and after 7 days from supplementation.
Results:
There was a significant improvement in hemoglobin percentage (P < .0001), total white blood cell (WBC) count (P < .0001), and platelet count (P < .0001) and significant decrease in CRP (P < .0001), ESR (P < .0001), IL-6 (P < .0001), and albumin level (P < .001) in the supplemented group than the nonsupplemented group. The supplemented group also had a significantly shorter duration of stay in pediatric intensive care unit (PICU; P < .01) and decreased death rate than the nonsupplemented group.
Conclusion:
Children with mild to moderate sepsis showed significant improvement in inflammatory markers and had shorter PICU admission when enteral feeding was supplemented with omega-3 essential fatty acids.
Introduction
Sepsis is an inflammatory-mediated condition in response to infection and is one of the most common causes of death in hospitalized patients including children, with mortality rate reaching 28.3% to 41.1% in developed countries and a much higher figure in developing countries. 1 According to World Health Organization statistics, 80% of death in children <4 years can be classified as sepsis-related deaths. 2 Patients who survive sepsis have an underrecognized risk of physical and cognitive impairment with more than doubled risk of dying in the following 5 years. 3 Pathogenic invasion of the blood stream during sepsis induces inflammatory response syndrome (systemic inflammatory response syndrome) as a result of the circulation of high concentrations of inflammatory cytokines such as tumor necrosis factor (TNF) α, interleukin (IL) 1β, IL-6, and IL-8. Interleukin 6 and other cytokines induce the release of C-reactive protein (CRP) from the liver, which is a strong proinflammatory and anti-inflammatory acute-phase protein that helps meditating the elimination of pathogens. 4
Interleukin 6 is one of the most prominent sepsis markers and involved with the activation of cytokine cascade in sepsis. 5 It has both proinflammatory and anti-inflammatory effects, and its release is induced by the primary cytokines of sepsis, TNF, and IL-1. It increases early in sepsis and peaks within 2 hours after the onset of infections and persists in the bloodstream for longer duration than TNF and IL-1. 5,6 Interleukin 6 is proved to be a good marker of sepsis and is correlated with the severity and outcome of sepsis. Decreasing the level of IL-6 after initial increase in patients with sepsis coincides with controlling the sepsis and is a good predictor of survival with close relation to the outcome. 7,8
The immune system is responsible for host protection against the effects of infectious agents as well as plays a pivotal role in triggering sepsis manifestations. Adequate functioning of immune system is critically determined by nutrition. Immune nutrition is the modulation of the immune system response by nutritional supplement or modification. 9 In critical conditions such as sepsis, it is known that omega-3 supplementation has positive effects on the immune system as well as the patient’s prognosis due to anti-inflammatory properties. 10 Studies in adult population showed beneficial effects of omega-3 supplementation to the enteral feeding in reducing ICU length of stay and new organ failure and in significantly reducing the mortality rate. 11,12 According to our best knowledge, most of the studies concerned with the use of immune nutrition were performed on adult patients, with few studies done on pediatric patients with sepsis. This study was designed to investigate the potential benefits of supplementing enteral feeding with omega-3 fatty acids on children with sepsis who needed pediatric intensive care unit (PICU) care and its effects on acute-phase reactants and the level of IL-6.
Patients and Methods
Study Design
The study was conducted as a prospective randomized, double-blind, placebo-controlled study from January 2012 to June 2014 in the PICU, Pediatric Department in a tertiary care hospital. The study included children diagnosed to have various grade of sepsis due to various causes who needed intensive care support and who tolerated enteral feeding within a maximum 2 days of admission. The children were divided by computer randomization into 2 groups. Group A received omega-3 fatty acids with their enteral feeding, while group B received enteral feeding without omega-3 fatty acids supplement. All cases included in the study received the appropriate treatment immediately according to their primary diseases (eg, fluids, inotropes, antibiotics for sepsis and pneumonia, mechanical ventilation when needed, etc). The study was approved by the Ethics Committee of the Faculty of Medicine, Tanta University, and conducted in accordance with the Helsinki Declaration. Written informed consent was obtained from each child’s guardian prior to any study procedure, with assurance of patient privacy.
Patient Selection
Children included in the study were between 1 and 5 years of age who were diagnosed as having sepsis by a PICU physician according to the criteria set by Critical Care Consensus Conference of Intensive Care Society of the Union of the American Physicians. 13
Exclusion criteria included any child with contraindication to enteral feeding; history or clinical evidence of malnutrition according to the updated World Health Organization child growth charts 14 ; cases with severe sepsis, septic shock, or any systemic organ failure; or any child who cannot tolerate enteral feeding within the first 2 days of admission. Children who stopped enteral feeding before completing the study and those who succumbed before the end of the study were also excluded. All children had thorough medical and nutritional history and thorough clinical examination including general and systemic examination as well as nutritional assessment. Complete blood count, biochemistry, and coagulation were routinely assessed. The liver and renal functions were done on admission to exclude organ failure. Complete blood pictures, markers of inflammation, including acute-phase reactants (CRP, erythrocyte sedimentation rate [ESR], and serum albumin), and IL-6 were measured on admission and after 1 week of the starting supplement.
Outcome Measures
There were 2 domains targeted as primary outcomes in the study: clinical outcome of the cases and changes in inflammatory markers and IL-6.
Nutritional Intervention
Enteral feeding was done through nasogastric tubes after ensuring tolerance to the enteral feeding. Tolerance to the enteral feeding was tried when the child was hemodynamically stable and had functioning gastrointestinal tract and done according to European Society for Parenteral and Enteral Nutrition (ESPEN) guidelines on enteral nutrition. 15 Children were randomly divided into 2 groups by a computerized program based on a randomization schedule produced by the study biostatistician. Group A was supplemented by omega-3 fatty acid in a dose of 350 mg twice daily for children between 1 and 3 years and 450 mg twice daily for children between 4 and 5 years during 7 days after admission to the intensive care unit and standard treatment per the American Institute of Medicine of the National Academies guidelines for maximum dose for this age group. 16
Group B received enteral feeding without omega-3 fatty acid support. Both the patient families and the investigators were blinded to the supplement. The omega-3 was used as syrup containing 395 mg of omega-3 fatty acids for every 5 mL in the form of 140 mg docosahexanoic acid (DHA) and 35 mg eicosapentaenoic acid (EPA). The protein, carbohydrate, fat, water, mineral, and vitamin contents were the same for both groups, except for the omega-3 contents. Basal energy requirements were calculated with the Schofield equation. Monitoring of enteral feeding was done according to the recommended rules for all forms of nutritional support, including the risk of refeeding syndrome as well as daily assessment of the position of nasally inserted tubes, and the possible occurrence of the development of erosions. 15,16
Statistical Analysis
The power level of the primary end point of the study was more than 90% when using 60 patients for each group (using Power and Precision V3; http://www.Power-Analysis.com/). The statistical analysis was performed using WINKS SDA Software (sixth edition, 2007; TexaSoft, Cedar Hill, Texas). Data were presented as mean ± standard deviation (SD) values. Comparison between the studied groups was performed with Student t test, with P < .05 considered statistically significant. Wilcoxon signed rank test was used to assess the normality of distributions of the data.
Results
The study included 120 children with sepsis who needed PICU admission, divided into 2 groups: group A had 60 children supplemented with omega-3 and group B had 60 children without omega-3 supplementation. The demographic characteristic of the 2 groups did not have any significant statistical difference, as shown in Table 1. The most common organisms implicated in sepsis were the viral sepsis in both groups followed by Streptococcus pneumoniae, and underlying medical conditions were present in more than half of the patients in both groups.
Demographic and Clinical Data of the 2 Patient Groups.
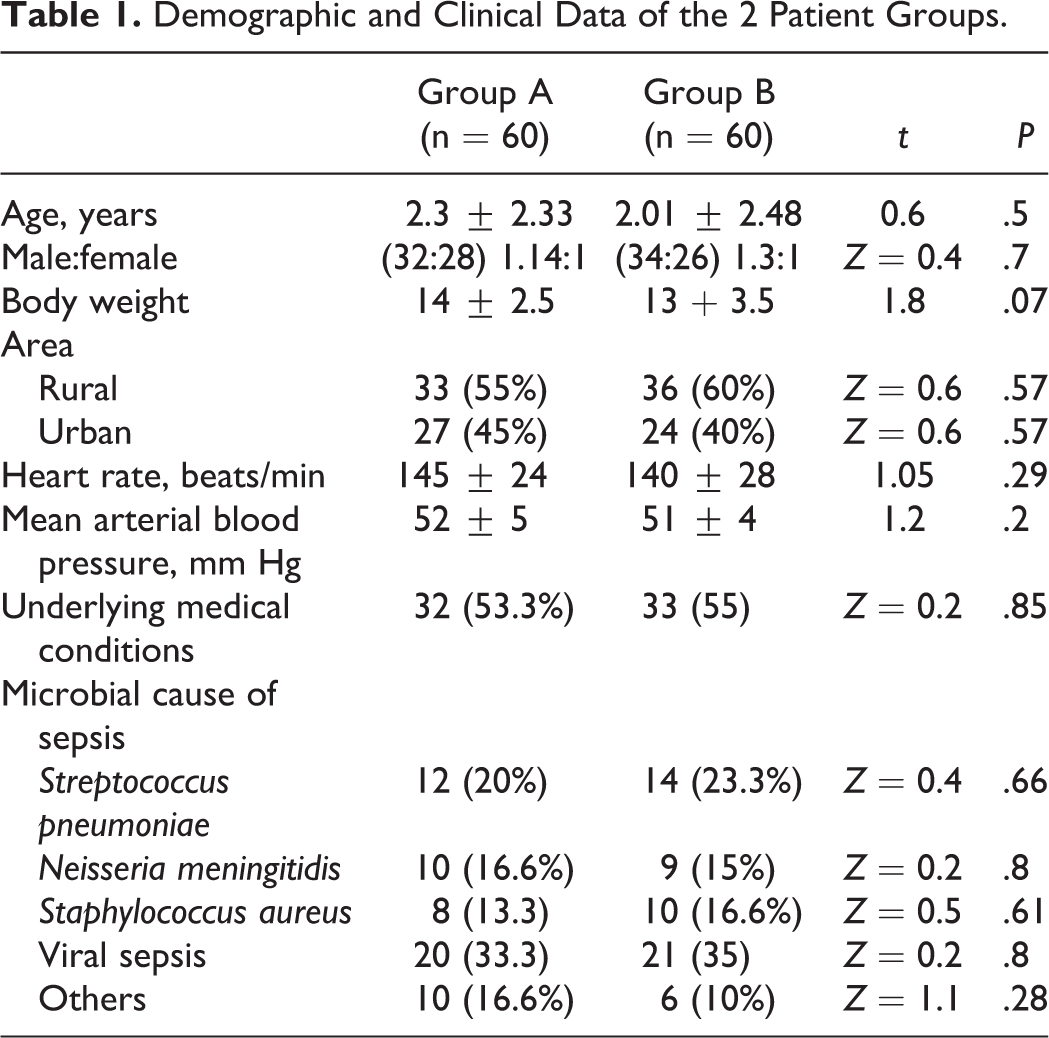
Table 2 shows the laboratory data of the 2 groups before the nutritional intervention. It showed no significant difference in hemoglobin percentage (Hb%), total white blood cell (WBC) count, platelet count, CRP, ESR, IL-6, and serum albumin between the 2 patient groups. After 1 week from supplementation with omega-3, Hb% showed significant increase (P < .0001), total WBC counts showed significant reduction (P < .0001), and the platelet count showed significant improvement in the supplemented group than the nonsupplemented group (P < .0001). The acute-phase reactants (CRP and ESR) also showed significant improvement in the supplemented group than the nonsupplemented group (P < .01 and P < .0001, respectively). At the same time, IL-6 showed significant reduction (P < .0001), and serum albumin showed significant increase (P < .01) in the supplemented group than the nonsupplemented group. Despite the death rate showed no significant difference in the 2 groups, the duration of PICU admission was significantly shorter in the supplemented group than the nonsupplemented group (P < .01), as shown in Table 3.
Laboratory Data of the 2 Groups Before Nutritional Intervention.a
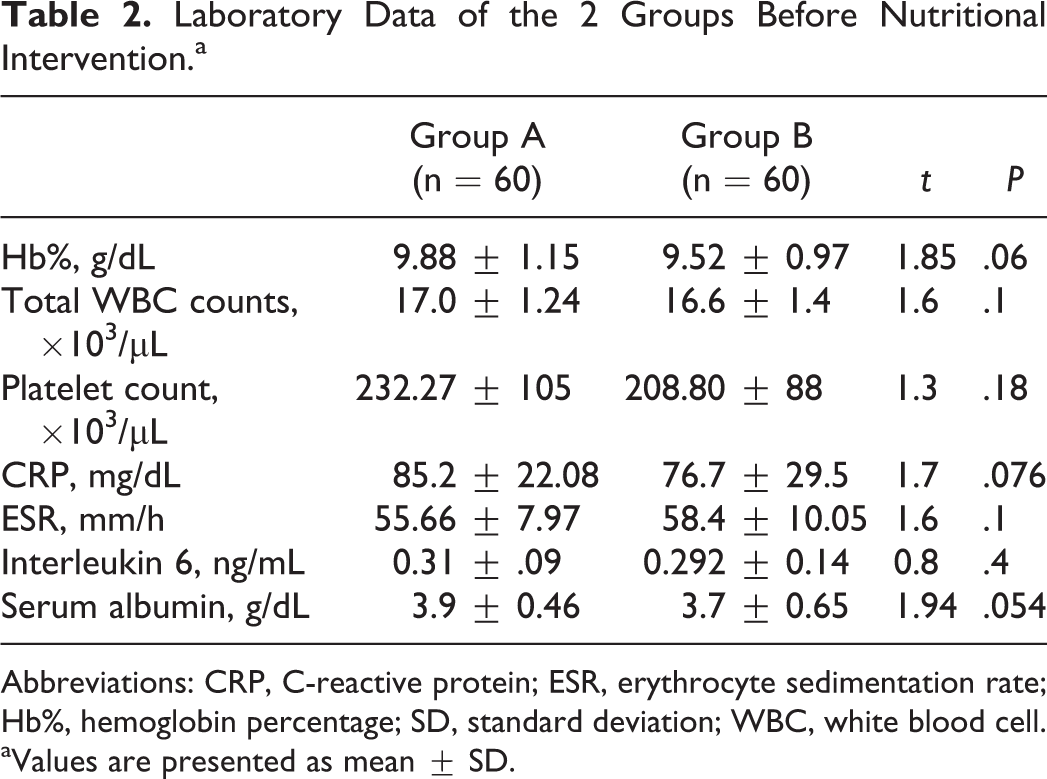
Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Hb%, hemoglobin percentage; SD, standard deviation; WBC, white blood cell.
aValues are presented as mean ± SD.
Laboratory Data of the 2 Groups After Nutritional Intervention.a

Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Hb%, hemoglobin percentage; PICU, pediatric intensive care unit; SD, standard deviation; WBC, white blood cell.
aValues are presented as mean ± SD.
bSignificant.
Tables 4 and 5 showed comparison between the patient groups before and after the nutritional intervention. Table 4 showed significant improvement in Hb%, total WBC counts, platelet count, acute phase reactants (CRP and ESR), as well as IL-6 levels and albumin levels in the supplemented group after than before supplementation. On the other hand, the nonsupplemented group did not have significant improvement except for total WBCs, CRP, and ESR.
Laboratory Data of the Omega-3 Supplemented Group Before and After Nutritional Intervention.a
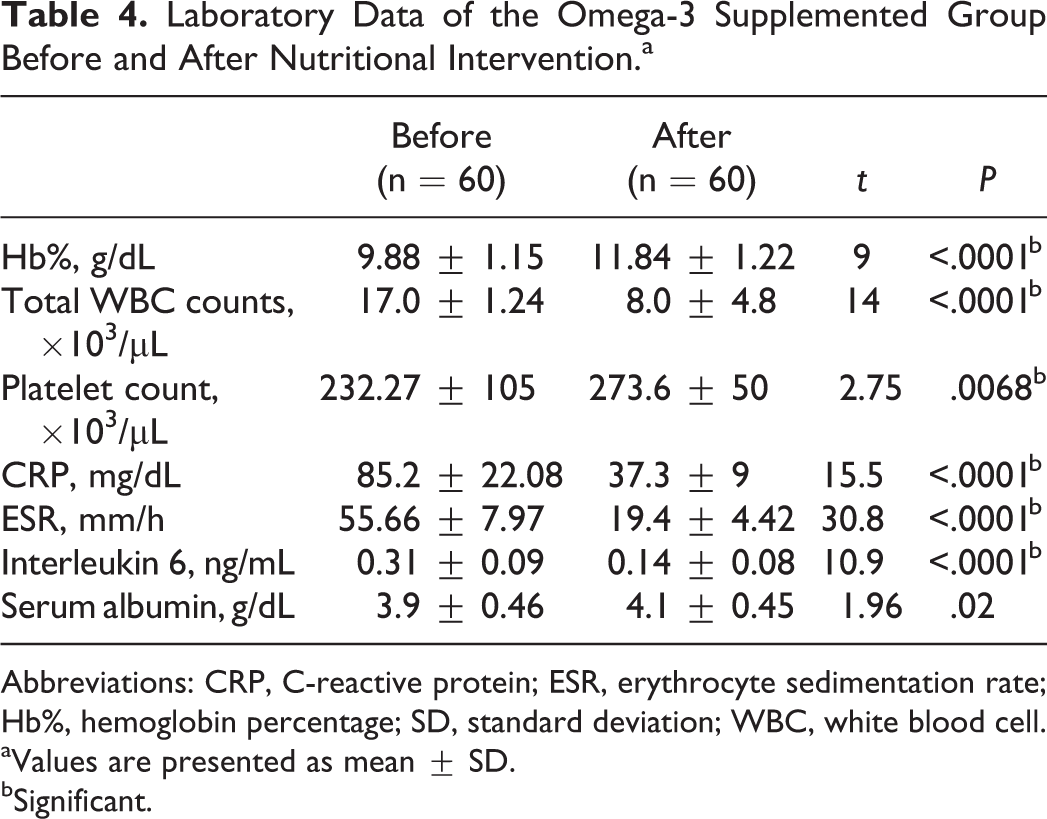
Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Hb%, hemoglobin percentage; SD, standard deviation; WBC, white blood cell.
aValues are presented as mean ± SD.
bSignificant.
Laboratory Data of the Nonsupplemented Group at the Beginning and at the End of the Study.a
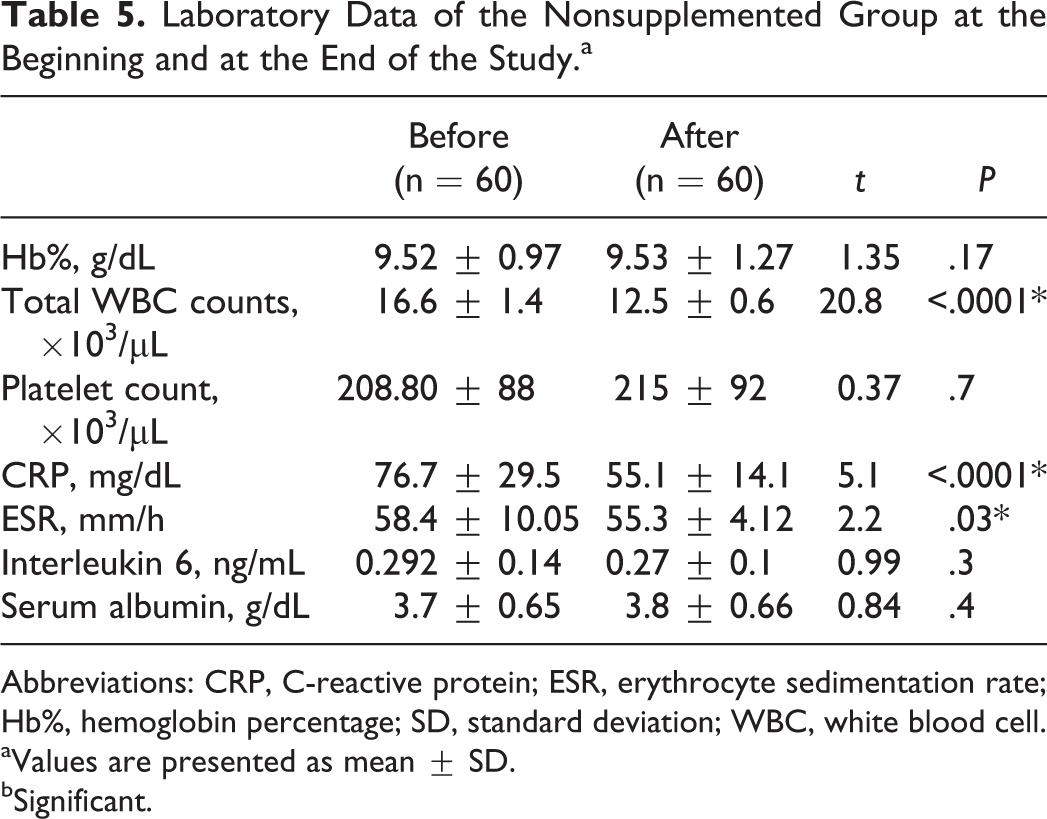
Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Hb%, hemoglobin percentage; SD, standard deviation; WBC, white blood cell.
aValues are presented as mean ± SD.
bSignificant.
Discussion
Sepsis is an uncontrolled and overwhelming systemic immune response to an infection. Inflammation is the hallmark of sepsis and characterized by oxidative stress, mitochondrial dysfunction, and massive cytokine release, which caused cellular damage and organ dysfunction. 17 In the current study, there were significant increased levels of acute-phase reactants (CRP and ESR) and IL-6 in both patient groups. C-reactive protein is increased in a try of the body to eliminate the pathogens and to inhibit the interaction between endothelial cells and leukocytes to reduce the deteriorating inflammatory response. However, CRP is a marker of inflammation and cannot distinguish between infectious and noninfectious causes of inflammation. 18 In the current study, CRP showed significant reduction after 1 week from treatment of sepsis in both patient groups. C-reactive protein levels usually decrease over the first 48 hours when successful antimicrobial therapy is initiated, 19 which is matching with our results. However, CRP has poor predictability of mortality. 20 On the same way, ESR showed significant increase in both patient groups. However, ESR has relatively low sensitivity and specificity for sepsis, which could be increased when combined with other markers such as immature and total neutrophil (I–T) ratio. 21 Interleukin 6 was found to be significantly high in both patient groups in our study. Interleukin 6 was found to increase fast in sepsis so that it could serve as a good sepsis biomarker and is a well-known predictor of blood culture positivity in patients with sepsis. Direct measurement of the serum IL-6 level can help rapidly detect bacterial infection, thus allowing for early therapeutic decisions and prognostic predictions. 22
Current guidelines of sepsis management recommend that anti-infectious therapy such as antimicrobial therapy and surgical source control should be initiated as soon as possible to optimize outcome. 23 Although antibiotics are the keystone in the management of sepsis, numerous various treatment modalities were tried to improve the outcome in different centers all over the world. Immune modulation and targeting inflammatory cytokines production are among these modalities, for example, Toll-like receptor 4 inhibition and modulation of the endocannabinoid system. 24 Nutrition is a critical determinant of immune responses. Nutrients act as antioxidants and cofactors at the level of cytokine regulation. Nutrition can affect cell-mediated immunity, phagocyte function, complement system, secretory immunoglobulin A antibody concentrations, and cytokine production. Specific food components can enhance immune functions or alternatively dampen the inflammatory processes. Micronutrients such as zinc, selenium, iron, copper, vitamins A, C, E, and B6, and folic acid have important influences on immune responses. 25
In our study, there was a significant improvement in Hb%, WBCs, platelet count, CRP, ESR, and IL-6 in the patient group supplemented with omega-3 than the nonsupplemented group. Omega-3 polyunsaturated fatty acids are essential dietary constituents. Besides their importance as a source of energy, structural components of cell membranes, and signaling molecules, they demonstrated potent modulating effects of the immune response through modification of eicosanoid production and by direct or indirect modification of the intracellular signal transduction pathways, including the alteration of gene transcription, in various tissues as well as by induction of apoptosis in primary lymphocytes, monocytes, colonic mucosal cells, and various cell lines, thus inhibiting the inflammatory process at different levels. 26 –28 Supplementation with omega-3 also alters the profile of lipid mediators generated during inflammation, with production of the newly identified, DHA-derived inflammation-resolving mediator classes (in addition to the formation of less proinflammatory eicosanoids from EPA). It also modulates the vagal tone with potential anti-inflammatory effects by activating nicotinic receptors upon infiltrating and resident macrophages. Stimulation of the efferent vagus is therapeutic in experimental septic shock. Fish oil supplementation increases vagal tone following myocardial infarction and in experimental human endotoxinemia. 29
Many studies showed that diet supplementation with omega-3 fatty acids was associated with a reduction in the release of prostaglandin E2, thromboxane B2, leukotriene B4, and leukotriene E4 from inflammatory cells. 30 Mayer et al showed that omega-3 acids EPA and DHA significantly improve neutrophil functions. 31 Gultekin et al showed that omega-3–enriched total parenteral nutrition solution contributes to a decrease in the levels of inflammatory mediators and to an improvement in the biochemical parameters in patients with sepsis. 32 Barbosa et al also showed that parenteral fish oil in patients with sepsis increases plasma EPA, modifies inflammatory cytokine levels, significantly decreases IL-6, and improves gas exchange, which are associated with a tendency toward shorter length of hospital stay. 33
In our study, children supplemented with omega-3 had a significantly shorter duration of PICU admission days than the nonsupplemented group. Grau-Carmona et al showed that adult patients with sepsis who received enteral diet enriched with EPA, γ-linolenic acid (GLA), and antioxidants had a shorter length of stay in the ICU than the nonsupplemented patients. However, they did not find any differences in infectious complications. 34 In addition, Heller et al showed that administration of omega-3 fatty acid may reduce mortality, antibiotic use, and length of hospital stay in different diseases. 35 Pontes-Arruda et al showed that adult patients with severe sepsis or septic shock who required mechanical ventilation and tolerated enteral nutrition supplemented with EPA, GLA, and elevated antioxidants had significant increases in ICU-free days, ventilator-free days, oxygenation status, and 28-day survival than the nonsupplemented patients. 12 However, although Singer et al showed in patients with acute lung injury that a diet enriched with EPA + GLA may be beneficial for gas exchange, respiratory dynamics, and requirements for mechanical ventilation, they showed that the hospital length of stay was not different between the 2 groups. 36
There are a number of limitations in our study. We excluded many diseases associated with sepsis such as malnutrition from the study to decrease the effects of confounding factors. However, this may lead to the need for another study for the effects of omega-3 supplement in such cases. Also, despite the keen to decrease the effects of various confounding factors, the only effective way is to do a large-scale multicenter study adequately powered and well controlled for confounding factors to show beneficial or harmful effects of such interventions. We also examined mild to moderate cases with sepsis and excluded severe cases. So, we also need to extend the study to include severe sepsis.
Conclusion
Inflammatory response is the hallmark of sepsis. Omega-3 supplementation of the enteral feeding showed significant improvement in WBCs, platelet number, Hb%, acute phase reactants, and IL-6, with a shorter length of stay in PICU in children with mild to moderate sepsis. Further studies are needed to show the efficacy of omega-3 supplementation in severe sepsis and systemic organ failure.
Footnotes
Authors’ Note
Work done in Pediatric ICU, Pediatric Department, Faculty of Medicine. All the authors affirm that the manuscript is an honest, accurate, and transparent account of the study being reported. We declare that no important aspects of the study have been omitted. All the authors are responsible for data sharing and to make raw research data available to everyone upon request for free.
Ethical Approval
The study was approved by the Ethics Committee of the Faculty of Medicine, Tanta University, and conducted in accordance with the Helsinki Declaration. Written informed consent was obtained from each child’s guardian prior to any study procedure, with assurance of patient privacy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.