
Abstract
Introduction:
The intensive care unit (ICU) is a dynamic and complex learning environment. The wide range in trainee’s experience, specialty training, fluctuations in patient acuity and volume, limitations in trainee duty hours, and additional responsibilities of the faculty contribute to the challenge in providing a consistent experience with traditional educational strategies. The “flipped classroom” is an educational model with the potential to improve the learning environment. In this paradigm, students gain exposure to new material outside class and then use class time to assimilate the knowledge through problem-solving exercises or discussion. The rationale and pedagogical foundations for the flipped classroom are reviewed, practical considerations are discussed, and an example of successful implementation is provided.
Methods:
An education curriculum was devised and evaluated prospectively for teaching point-of-care echocardiography to residents rotating in the surgical ICU.
Results:
Preintervention and postintervention scores of knowledge, confidence, perceived usefulness, and likelihood of use the skills improved for each module. The quality of the experience was rated highly for each of the sessions.
Conclusion:
The flipped classroom education curriculum has many advantages. This pilot study was well received, and learners showed improvement in all areas evaluated, across several demographic subgroups and self-identified learning styles.
Keywords
Introduction
The intensive care unit (ICU) is a unique learning environment where trainees have the ability to participate in the management of some of the most acutely ill patients in the hospital. Learners must acquire a broad foundation of critical care knowledge as well as develop technical and clinical problem-solving skills. 1 In addition to providing unique learning opportunities, this complex clinical setting poses unique challenges. Common challenges in trainee education include the wide range in level of training (from medical student to fellow) and experience of learners (often from a variety of specialty backgrounds including surgery, anesthesiology, internal medicine, etc). Fluctuations in patient acuity and volume, as well as the variability in disease states, may contribute to an unpredictable learning experience. Administrative responsibilities, documentation and billing requirements, or increased clinical volume also compete for the time faculty have available for teaching. 2 Limitations in duty hours of trainees have reduced clinical exposure and may allow less time for traditional methods of didactics. 3 The breadth and depth of medical knowledge and skill necessary for clinical practice continue to increase, yet the hours available for education have not. Therefore, the only realistic strategy to rectify this disparity is to make better use of our time. Innovative educational approaches for learning in the ICU, which account for the exponential growth in medical knowledge, unique learning needs, and time constraints of the learners, while adapting to the dynamic and clinically demanding environment of the ICU are needed. 4,5
The “flipped classroom” (also called “flipped teaching,” “inverted classroom,” or “blended teaching”) is one idea for improving educational efficacy that has had much recent attention in both the popular and scientific educational literature. 6 –9 The rapid increase in Internet access and advances in online technology over the last decade present an opportunity to rethink the way we teach and learn in the context of graduate medical education. The flipped classroom model is a type of learning where in-class experience is integrated with out-of-class (usually online) learning. In this paradigm, students first gain exposure to new material individually, usually via reading or watching videos, which provides a distinct advantage for learners who perform at different paces. Class time is then used for learning-centered activities that build on the preclass work rather than the traditional instructor-led lecture sessions. The overall effect is to “reverse” or “flip” the way in which material is presented to students.
The flipped classroom paradigm is particularly well suited for the ICU learning environment, where acquisition of a foundation of critical care knowledge is necessary before progressing to the more complex clinical problem solving required for patient care. There has been limited research exploring the flipped classroom model in the context of critical care education, which highlights an important knowledge gap. 10 Here, we present an overview of the flipped classroom model including its rationale and pedagogical foundations, as well as some practical considerations for implementation. An example of a successful program using the flipped classroom for teaching point-of-care echocardiography is provided.
Rationale and Pedagogical Foundations
In-class lectures remain the primary mode of didactic learning in most critical care training programs across the country. 11 The flipped classroom paradigm involves more than temporal economics by shifting content delivery outside class time. It represents a shift in how we think about the learning process. It is grounded in several interconnected educational theories and highlights many central concepts, including active learning, reflection, and collaboration.
Educators for many generations have assigned preclass reading for their students prior to a scheduled lecture. However, this notion has seen a recent revitalization due to developments in active learning theories, coupled with advancements in instructional technology. In the broadest sense, the flipped classroom may describe almost any class structure that provides content and material delivered primarily outside the classroom, whereas in-class time is used “to work through problems, advance concepts, and engage in collaborative learning.” 12 This model allows students to independently engage with materials on their own time and at their own pace, shifts the onus from the instructor to the learner, and promotes active learning and problem solving. Rather than assuming the traditional role of lecturer (“sage on the stage”), instructors act as coaches or advisors (“guide on the side”) by suggesting problem-solving approaches, clarifying content, and encouraging students’ independent thinking. 13 The real value of a flipped classroom is in the repurposing of class time into an interactive environment where students can inquire about lecture content, test their skills by applying knowledge, and interact with each other in hands-on activities.
The flipped classroom model was developed by Bergmann and Sams in 2007 who decided to use video-recorded lectures to reach a proportion of their students who had missed class. 14 Bergmann and Sams found that students were generally positive about the method; they believed that it allowed more effective use of class time and challenged them to take responsibility for their own learning. A meta-analysis from the US Department of Education in 2010 focused on K-12 education showed that blended learning, such as the flipped classroom, is more effective than either face-to-face (ie, lecture-based instruction) or online learning alone. 15 More recently, the flipped classroom idea has become more popular, and its approach has been reported in a wide variety of educational settings, including medical education. 16,17
The explicit attention to interactive and collaborative activities with the flipped classroom draws on Piaget theory of active learning. To acquire knowledge, learners must engage in active discovery learning through exploration, debate, and hands-on experiments; learning occurs not when students merely copy an idea but when they act on and apply new ideas and concepts. 18 With this theory, the instructor’s role should be to facilitate learning, not merely expound knowledge. Instead of passively listening to a lecture, students have more success when the teacher guides them through situations allowing them to explore and discover new things. Furthermore, passive learning often bores students, and they may lose motivation. Learners can read and learn information independently, but they need instructors to act as coaches and mentors to stimulate and challenge their thinking, guide their problem solving, and provide encouragement through their learning and application of the material.
The flipped classroom model also fits well with Vygotsky concept of the “zone of proximal development” (ZPD). 19,20 Vygotsky posits that learners progress through this ZPD from tasks that they can perform independently to those that they previously could not. Experienced instructors can facilitate this transition. Instructors may not be necessary for the initial steps (eg, acquisition of basal knowledge) but are integral for the refinement and application of that knowledge.
Bloom taxonomy is a widely accepted framework used to define and distinguish different levels of human cognition (Figure 1). 21,22,23 The framework classifies thinking and learning according to 6 levels of complexity, often depicted as a pyramid, leading many instructors to encourage their students to “climb to a higher (level of) thought.” The lowest 3 levels are knowledge (remembering), comprehension (understanding), and application. The highest 3 levels are analysis, synthesis (creation), and evaluation. The flipped classroom allows for progressive exposure to lower than higher levels of cognitive performance. 24 For example, students can do more basic cognitive work (ie, knowledge acquisition) independently and outside class, whereas more complex tasks (ie, knowledge application and synthesis) occur during class time with the support of their peers and instructors.
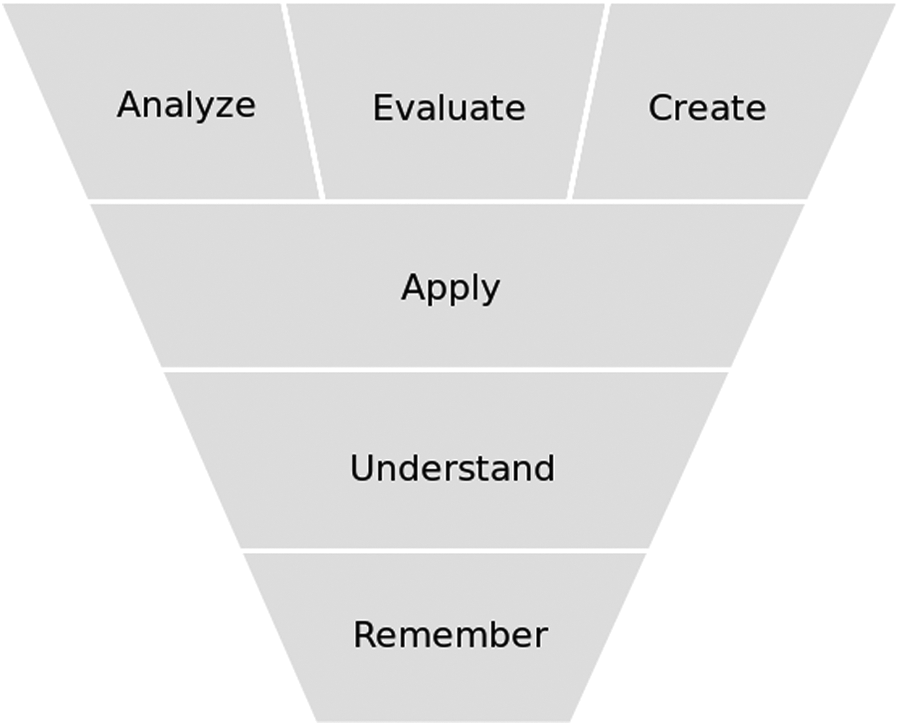
Bloom taxonomy. 21
The flipped classroom design also draws theories that emphasize the importance of reflection in the learning process. Mezirow theory of transformative learning is based on the process of reflecting back on prior learning to determine whether what we have learned is justified under present circumstances.
25
He suggests that as learners and educators we can transform our frames of reference through critical reflection on the assumptions upon which our interpretations, beliefs, and habits of mind or points of view are based. We can become critically reflective of the assumptions we or others make when we learn to solve problems instrumentally or when we are involved in communicative learning.
26
Mezirow believed critical reflection is the distinguishing characteristic of adult learning. He called rational discourse “a catalyst for transformation,” as it caused the learners to reflect on the depth and meaning of their own interpretations and forced them to articulate those values.
There is also a great deal of support for the notion of pretraining or “priming” approaches in increasing student learning and achievement. When learners are exposed to particular stimuli, their retention is improved if they have previous experience with the stimuli. 27 By providing students with direct instruction outside the classroom, they are essentially “primed” for the active learning tasks carried out in the flipped classroom. Another benefit of this sort of graded exposure is to reduce the “cognitive load” on learners, enabling them to process information more efficiently. 28 Pretraining may be an effective method of managing a large amount of material, thereby providing another mechanism for the observed positive effect of using the flipped classroom model on learning.
A growing body of literature supports the effectiveness of active learning strategies for increasing student learning and achievement. 29,30 Active learning is associated with increased engagement and critical thinking and improved outcomes and attitudes toward learning. 31 –33 Moreover, active learning stimulates higher order thinking, problem solving, and critical analysis while providing feedback to both the student and the instructor. 18,20
Another consideration in selecting the flipped classroom for ICU education focuses on the unique challenges and opportunities associated with training the “millennial generation” of learners. Characteristics of learning associated with this generation include preferring to work in groups with hands-on experiences, enjoyment of trial and error, decreased value for reading and listening to lectures, and wanting learning to be creative, interactive, and fun. 34 Although it is certainly too simplistic to ascribe these characteristics to all members of a generation, it is interesting to note that many of these attributes are consistent with trainee’s complaints of the traditional lecture structure.
Advantages of the Flipped Classroom for ICU Education
Provides scheduling flexibility and individualization
The flexibility afforded by the flipped classroom allows for an environment in which learners choose how, when, and where they learn. Learning materials may be made available to learners regardless of their particular shift schedule. The mechanism used to expose learners to new learning material can vary from simple textbook readings to lecture videos or podcasts. Preclass assignments can be varied based on differing backgrounds and training levels of the learners. If asynchronous video-recorded lectures are used, these can be paused and replayed, allowing learners to move through material at their own pace. Using a range of formats to present course content can support students’ individual learning styles and preferences. Learning is maximized via student-centered activities aimed at their readiness level or ZPD, where they can be challenged without becoming frustrated or embarrassed.
19
Flipping the classroom in this way empowers instructors to develop different learning experiences appropriate for each student.
11
2. Facilitates activities that focus on higher level cognitive skills
Capitalizing on the learner’s acquisition of basic knowledge with preclass activities in the flipped classroom, faculty can devote more face-to-face time to integrating and applying this knowledge to patient care.
1,4
The use of active learning techniques such as small group, case-based, or team-based exercises in this manner is thought to improve retention and understanding.
6
Although trainees are applying their new knowledge with supervision, they have access to immediate feedback from peers and faculty, which will help them recognize and think about their own growing understanding. The focus on active problem solving should also make learners more prepared to function independently. 3. Provides a mechanism to assess understanding and provide feedback
Preclass assignments can help both the educators and the learners assess understanding. Use of preclass quizzes can allow the faculty to practice “just-in-time teaching” in which the class activities are tailored to focus on the elements with which learners are struggling. 35 Time spent in active learning activities may strengthen the relationship between the faculty and the learners, allowing the faculty to understand even more about the learners’ strengths and weaknesses. This may give instructors a better opportunity to detect errors in thinking, especially those that are widespread throughout a class. Since faculty continually observe and provide feedback during class, it reduces the need to provide extensive commentary outside class. Learners can provide peer feedback to each other and respond to feedback they receive, encouraging a dialogue on the learner’s work and focus on the process rather than on the final product. It also gives learners practice at assessing their own work.
Faculty can obtain real-time feedback on the educational experience in an ongoing effort of quality improvement. Educational materials can be updated continuously for future iterations based on the feedback received. Lectures that have been criticized as being too long or not clinically relevant can be replaced by interactive sessions with simulations or other clinically relevant scenarios that more actively engage students in the learning process. Many educators and students have felt that the flipped classroom is a valuable way of improving learner engagement and promoting a sense of responsibility for one’s education.
Practical Considerations
Implementing a novel teaching strategy is not without potential difficulty. There is no single or standard way to design and implement the flipped classroom instructional model in practice. The means of delivering content and the ways in which face-to-face class time is used will vary with the subject matter, characteristics of the learners, background of the instructor, and available resources. Out-of-class and in-class elements must be carefully integrated to optimize the beneficial effects and encourage students to be prepared for class. Despite the potential benefits of the flipped classroom design, there are likely to be significant barriers and challenges to successful implementation. Anticipation of these potential challenges in combination with strategies to address them is most likely to ensure the project’s success. Resistance to changing the time-honored traditions of medical education
Some participants may voice objections to a new teaching model by arguing, “Despite the acknowledged problems with the existing method, we still produce well-trained physicians. Do we want to risk this success with untried methods?” To address this concern, it is important to emphasize that the goal of the flipped classroom is not to replace “what works” but rather to improve upon what doesn’t work. In this case, it is likely better to ease into the new educational program rather than abandon the existing system entirely. Early implementation may consist of changing one classroom experience per week, then expanding as success and experience grow. It is not necessary to change to a completely flipped classroom; a hybrid approach of instructional methods may be more successful and preferred by students or educators. It is important to evaluate the impact of the flipped classroom in the ICU using measures of learner satisfaction, teacher satisfaction, and knowledge acquisition. Ultimately, the goal should be to assess the impact on clinical performance. 2. Cost and time required for implementation
Educators unfamiliar with the flipped classroom are likely to require some support undertaking a novel curriculum design, as well as preparing materials and assignments (eg, video lectures and active learning classroom exercises). There may be concerns about the increased workload associated with progressing from traditional lectures to a flipped classroom. However, this “activation energy” may not be as severe as anticipated. The upfront time spent learning a new system and technology, as well as creating preclass materials for class, is largely a one-time expense, and the enduring materials produced can be reused and enhanced with future classes.
It is important to appreciate the cost–benefit ratio of this type of curriculum development when deciding how soon and how extensively it should be implemented. It will be enlightening to compare the time and effort required for faculty in preparation and project implementation with measures of educational effectiveness. Because this approach represents a comprehensive change in the class dynamic, a graduated introduction may be a less threatening approach. 3. Resistance to completing the preclass assignments
The effectiveness of in-class activities can be influenced by whether learners come to class prepared. Establishing ground rules and emphasizing expectations the faculty have for learners to view content before class are important. Explaining the rationale and creating “buy-in” from the learners may help them appreciate the importance. It may be helpful to communicate how much time is expected for each learning activity so that they can prioritize fitting them into their schedules. Finally, it is important to provide a guideline for what assignment outcomes are expected and how they will be assessed. Providing an incentive for learners to prepare for class may work in some cases. Integrating quizzes, or some other kind of activity that engages the learners with the material, may also be an effective means of getting learners to complete the assignments.
No matter how clear the explanation given in a video or written material, there will likely be learners for whom the information presented is too advanced and will need the presence of a faculty member to talk them through it. At the other end of the spectrum, if the content is too simple, the learner will not be challenged and not engaged with the material ideally. It may benefit both types of learners to provide material that can be adapted to their level of understanding. The preclass assignment might consist of both “core content” and advanced material with associated evaluative exercises such as quizzes for each group, which can serve as checks of understanding and as a departure point for class activities. 4. Resistance to active learning
Not all learners may be enthusiastic about active learning methods.
36
They may be accustomed to the traditional lecture format and find active learning approaches to be disorganized or chaotic. Or they may be more comfortable in a passive listening role and demonstrate resistance to an active environment that may require more participation. Some learners may think that faculty who practice active learning aren’t teaching, but rather shifting the instructional burden onto the learners. Others may resent having to work with (and learn from) other trainees when there is an “expert” in the room, and some may be uncomfortable taking an active role in the classroom. It is important to address these concerns by explaining the rationale for active learning while emphasizing what learners have to gain from such activities. This should occur at the beginning of the curriculum and can be repeated later if necessary. Rather than viewing complaints about active learning as a failure, they should be considered as “teachable moments” that offer opportunities to reflect on how they learn. For learners who are uncomfortable taking an active role in the class, breaking up into small groups may be less threatening. Although the flipped classroom is thought to encourage learners to take responsibility for their own learning, this will only happen if they are willing and able to do so. 5. Fear of loss of control of learning environment
Faculty may also find challenges with active learning activities. Opening the class to active learning makes it less predictable. Through a learning activity, it may become apparent that a significant number of students do not understand a concept, which prevents moving on to the next part of the planned educational activity. A heated debate on a controversial issue might erupt unexpectedly, or the faculty may find that the learners are not able to work together in a planned group activity. It is important to reinforce with the faculty that this unpredictability is an expected part of the process. The more these events happen, the more practice and skill will develop in predicting and dealing with them. Reflecting on the active learning activities ahead of time, anticipating the problems that might occur, and having a backup plan are all likely to be beneficial.
Despite these challenges, the flipped classroom model has been successfully implemented in many instances. This endeavor was designed to evaluate its effectiveness in teaching concepts and technical skills in postgraduate medical education.
Methods
A pilot study was conducted to examine the efficacy of the flipped classroom on learning outcomes for residents rotating in the surgical ICU (SICU) at the Massachusetts General Hospital. The SICU is a core educational rotation for surgery, anesthesia, and emergency medicine residents. Residents rotate through the SICU for three 1-month blocks staggered during their residency. Point-of-care echocardiography was chosen as the curriculum topic for the flipped classroom sessions because it is an increasingly important component of critical care practice and education 37 and provides an opportunity for a predictable implementation session, as it can be used in almost any clinical encounter.
The specific aims of the study were to evaluate the use of a flipped classroom approach within the SICU environment according to the first 2 levels of Kirkpatrick and Kirkpatrick effectiveness of training approach
38
: evaluate the impact of the flipped classroom approach on knowledge acquisition and evaluate residents’ perceptions of confidence with the content area, usefulness of the skills, and likelihood that they would use then in practice.
The project was approved as an educational quality improvement project by the Partners HealthCare Institutional Review Board. No patient data were collected, and all participants consented to participation.
Curriculum Design
A modular curriculum was developed to provide both core knowledge and hands-on skills to residents rotating through the SICU.
The curriculum was designed to teach the elements of basic critical care echocardiography and some components of advanced critical care echocardiography as has been suggested by the American College of Chest Physicians and La Société de Réanimation de Langue Française. 39 A series of 4 modules were designed around core concepts, each module consisting of a 5-minute video, intended to be watched prior to a “hands-on” teaching session led by experienced providers at the bedside. Videos were created using open access content from the Internet, compiled into a PowerPoint presentation, narrated, and annotated by one of the authors (C.R.T.) who is also credentialed as a registered diagnostic medical sonographer. Video files were then made available through a Dropbox link.
Modular curriculum for the flipped classroom
Part I: Principles of ultrasound
In this section, background is provided about sound wave propagation and its use for diagnostic ultrasonography. The principles are applied to the observation of respirophasic variation in the inferior vena cava, 40 which is practiced during the interactive session.
Part II: Basic views
The 4 basic views are introduced (parasternal long axis, parasternal short axis, apical 4 chamber, and subcostal), as well as evaluation for pericardial effusion. Each view is described in terms of the anatomic landmarks used to obtain it, as well as the orientation of the image. The 4 views are practiced during the interactive session.
Part III: Doppler and valves
Doppler measurements are described in terms of their use to evaluate velocity of blood flow. Distinction is made between pulsed-wave and continuous-wave Doppler for localized and higher velocities, respectively. The Bernoulli principle is applied to calculate a pressure gradient between 2 chambers, and an example of grading mitral stenosis is provided. These techniques are practiced during the interactive session.
Part IV: Functional assessment
During the final segment, ejection fraction is estimated using 2 techniques (fractional shortening and Gestalt estimation). Stroke volume is calculated through the left ventricular outflow tract. Diastolic function is measured by observing mitral inflow patterns with Doppler ultrasound, as well as tissue Doppler imaging of the mitral annulus. These measurements are practiced during the interactive session.
Assessment
Basic demographic information was collected using an online survey (SurveyMonkey). Participants were provided descriptions of the 4 Kolb learning styles (Appendix A) 41 and asked to select the one they felt best described their own learning style.
To assess the knowledge acquisition with the flipped classroom, pretesting and posttesting with multiple choice questions were performed (Appendix B). The pretest was administered via SurveyMonkey, which provided a link to the associated video after the assessment was complete. Six knowledge questions were created for each content area. These were divided into 2 test versions (3 knowledge questions per test), and learners were randomized (using an online random number generator at random.org) to receive one version as the pretest and the other as the posttest.
To assess residents’ perceptions of confidence with the content area, usefulness of the skills, and likelihood of use, a questionnaire using Likert scales was collected before and after each learning module. Evaluation of the quality of the videos and interactive sessions was also obtained, and open-ended feedback on ways to improve the curriculum was solicited.
Statistical Analysis
Continuous variables are reported as mean ± standard deviation. Categorical variables are reported as percentages or median and interquartile range as appropriate. The Wilcoxon signed rank test was used to examine changes in preintervention and postintervention scores in knowledge, perceptions of skill confidence, and likelihood of use after each module. Subgroup analyses of these changes and demographic variables including gender, specialty, postgraduate year (PGY) level, number of prior ICU months, previous ultrasound experience, and self-reported learning style were also performed. Statistical analyses were performed using STATA 10 (StataCorp 2007, College Station, Texas). Statistical significance was reached when P < .05.
Results
Baseline learner demographics are displayed in Table 1. Residents were 56.4% female, and more than half were from the department of anesthesia. Most were PGY-2 or PGY-4, and almost half identified themselves as “converging” learners based on the description provided.
Learner Demographics.
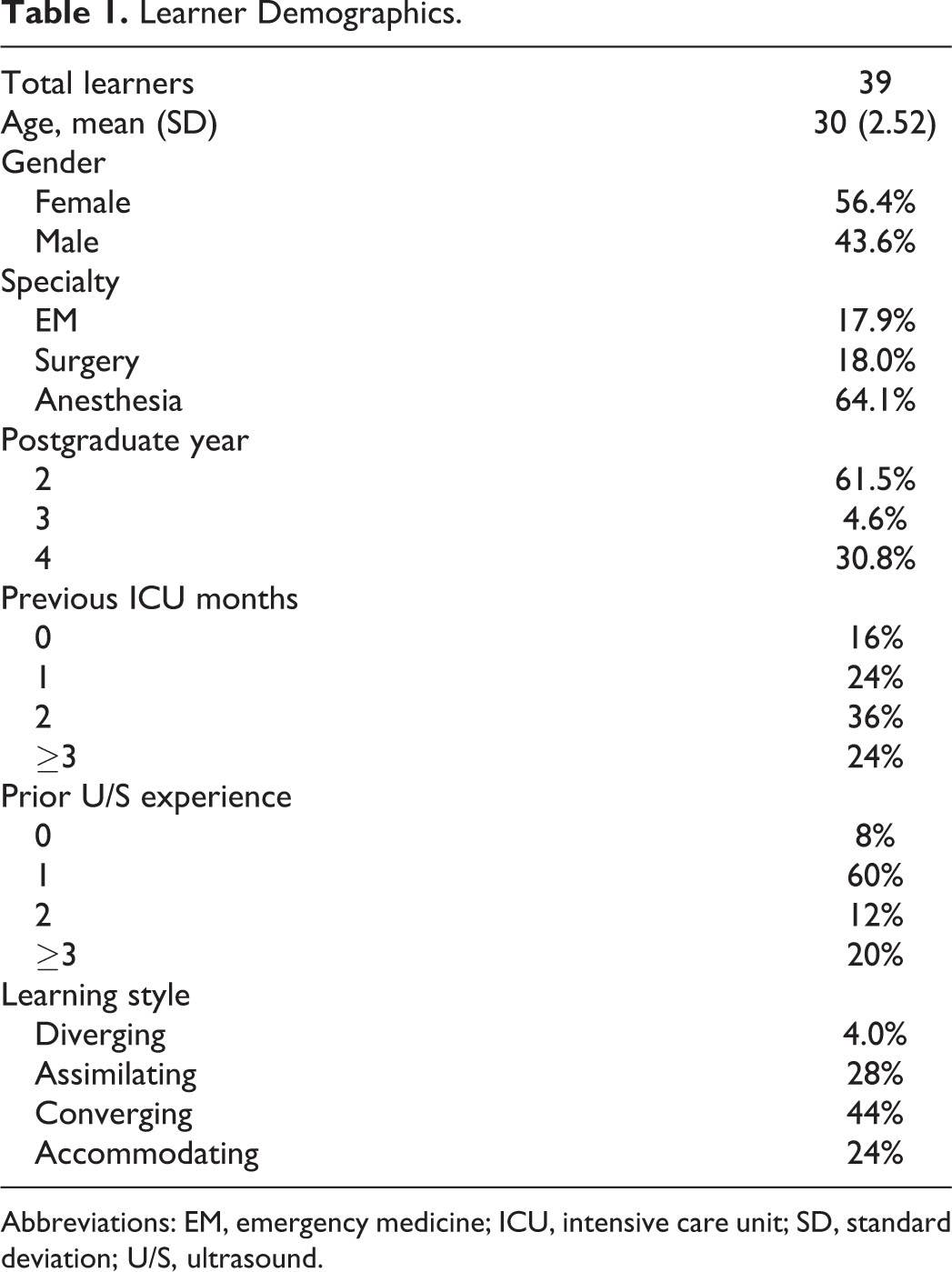
Abbreviations: EM, emergency medicine; ICU, intensive care unit; SD, standard deviation; U/S, ultrasound.
Preintervention and postintervention scores in knowledge, confidence, perceived usefulness, and likelihood of use the skills for each module are displayed in Table 2. Knowledge scores improved for all 4 modules (Table 2). There was a statistically significant improvement in residents’ perceptions of confidence with the content areas with each module. Report of usefulness of the material trended toward improvement in modules 1 and 2 and showed statistical improvements in modules 3 and 4. Likeliness to use ultrasound as reported by the residents increased after all sessions. There was no association between improvement in knowledge or residents’ perceptions of confidence, usefulness, or likelihood of use with regard to gender, self-reported learning style, level of training, or specialty area. Video quality and quality of the hands-on experience were rated highly (median “8 of 10” or higher) for each of the sessions.
Study Results.a
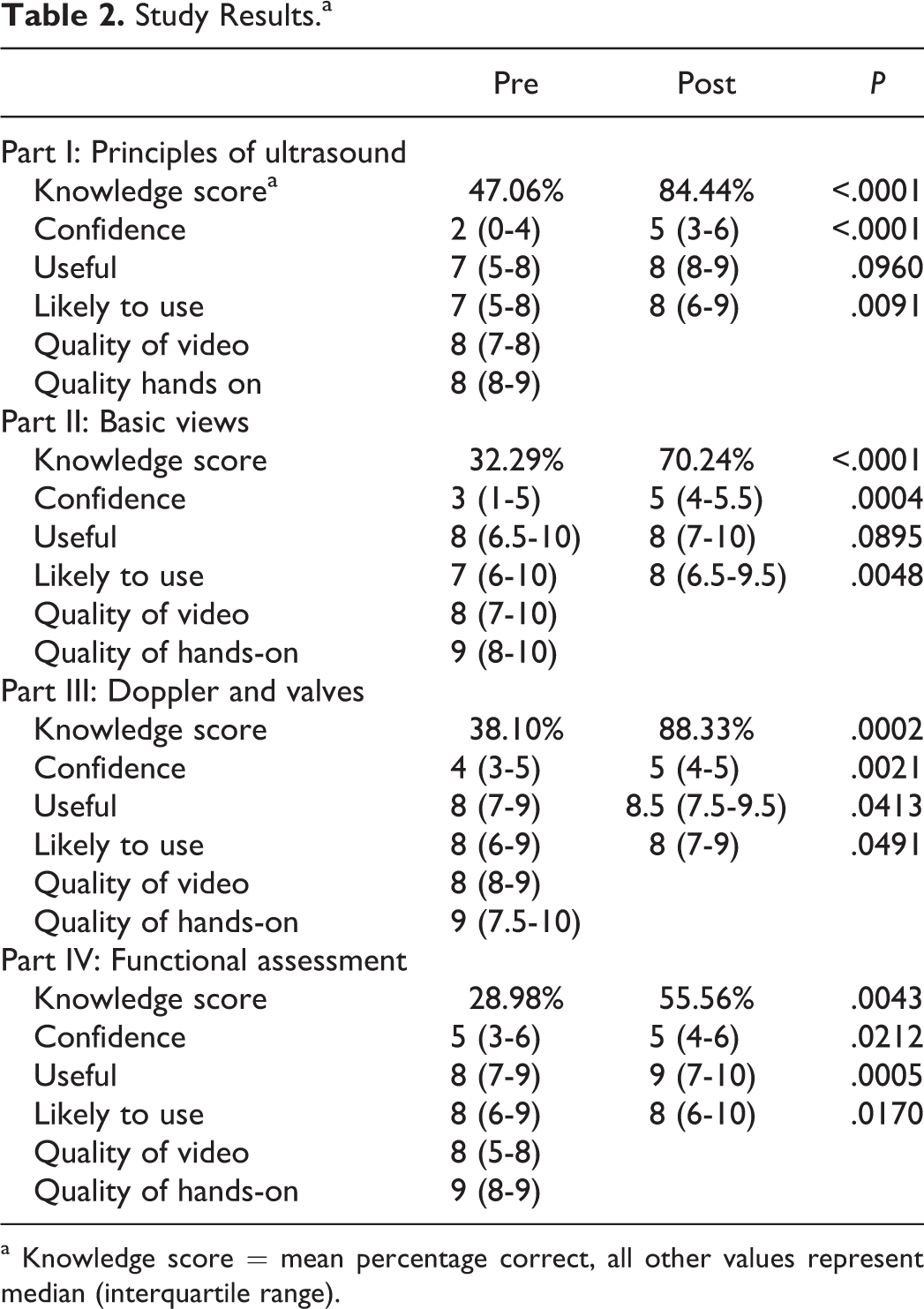
a Knowledge score = mean percentage correct, all other values represent median (interquartile range).
Discussion
The flipped classroom model appears to be effective as an education model across a range of learners when applied to a point-of-care echocardiography curriculum in the SICU. Residents showed improvement in knowledge, and their perceptions of confidence with the content area, usefulness of the skills, and likelihood that they would use then in practice attitude increased. These findings did not appear to vary based on differences in gender, self-reported learning style, level of training, or specialty area. Although the study was not designed to compare the traditional and flipped classroom models, resident’s open-ended feedback reflected a preference for the flipped classroom compared with the traditional model. This finding is consistent with current evidence. In a review of flipped classroom educational research, 11 studies examining student perceptions of the flipped classroom were identified, and all reflected overall positive opinion. 7
Limitations of this study include a limited small sample size, lack of systematic comparison to the traditional teaching model, and lack of generalizability to nonultrasound-specific course content. As this was a pilot study, the sample size was simply the number of students who participated in the class. In addition, we cannot exclude the possibility that students answered questions in a socially desirable way nor that the positive perceptions of this instructional model were attributable to merely being a different experience than other courses offered to the students. Future studies will provide additional insight into the impact of the flipped classroom on improved learner performance and attitudes as the instructional model becomes more widely adopted in medical education. In addition, studies that evaluate the use of the flipped classroom for instruction of other content areas are needed.
Conclusions
Innovative approaches that promote both educational efficiency and effectiveness are needed to meet for the challenges in educating the trainee in the ICU. The flipped classroom is an educational model with the potential to improve upon traditional educational strategies. For educators considering a flipped classroom instructional model, it is important to emphasize - as highlighted by Galway et al - that “flipping the classroom is not simply shifting lectures outside the classroom. [The method of] content delivery is just one small piece of the overall learning experience.” 24 “Flipping the classroom” also involves shifting control of both learning and the classroom from the instructor to the students, thereby promoting a focus on active learning and on higher order cognitive work. Educators should think purposefully about course design, develop effective learning activities that engage learners, complement online content, and take maximal advantage of face-to-face class time. To accomplish these tasks, it is important to think creatively about how to leverage emerging educational technologies in the flipped classroom approach. We hope that educators in the ICU environment will experiment with the flipped classroom described here to reinvent their classrooms in a way that empowers learners to develop higher order cognitive skills and to engage in meaningful learning that will ultimately improve the delivery of health care.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
{kind=link}