
Abstract
Introduction:
Thiamine is an essential cofactor in carbohydrate metabolism, and deficiency can therefore cause various organ dysfunctions. Little is known about the prevalence and possible worsening of thiamine deficiency in critically ill patients. In this study, we investigated the prevalence of thiamine deficiency at admission to the intensive care unit (ICU) and hypothesized that intensive insulin therapy, aimed at regulating glucose levels, increases thiamine utilization and therefore might cause or worsen deficiency in patients with limited thiamine stores.
Materials and Methods:
An observational prospective cohort study was carried out in a medical–surgical ICU in a general teaching hospital in Apeldoorn, the Netherlands. All adults who were treated during that time with intensive insulin therapy were included. Deficiency was defined as a thiamine level <100 nmol/L. No thiamine supplementation was administered except for normal amounts present in standard enteral feeding.
Results:
A total of 58 patients were available for analysis. Median thiamine level at admission was 111 nmol/L. Deficiency was present in 39.7% of patients and was significantly associated with the presence of gastrointestinal pathology and with recent surgery. Thiamine levels increased a median of 14 nmol/L in 48 hours. Only 3.4% of patients showed a predefined relevant decline in thiamine levels.
Conclusion:
Intensive insulin therapy does not appear to cause or worsen thiamine deficiency. However, based on the high prevalence of deficiency at admission, it might be warranted to supplement thiamine in all patients admitted to the ICU, especially when there is an underlying gastrointestinal disease or recent surgery.
Introduction
Thiamine, also known as vitamin B1, is a component of thiamine pyrophosphate, which is an essential cofactor in carbohydrate metabolism. Thiamine deficiency may cause various disorders such as polyneuropathy and hyperdynamic circulatory failure (dry and wet beriberi, respectively), Wernicke encephalopathy, and lactic acidosis. 1 –4 Thiamine body stores are small, usually accepted to be 30 mg in the average adult, and depletion may therefore occur quickly. 5 Risk of deficiency is highest in patients with inadequate intake, such as those with alcoholism, unhealthy diets, or imperfectly composed total parenteral nutrition, but also in those with increased losses or utilization, such as patients with malignancy or patients undergoing prolonged periods of continuous renal replacement therapy without adequate supplementation. 3,5 –8 However, little is known about the prevalence and possible worsening of thiamine deficiency in critically ill patients admitted to the intensive care unit (ICU), especially since the introduction of intensive insulin therapy (IIT). The IIT has been advocated for several years to reduce morbidity and mortality in critically ill patients admitted to the ICU, although target levels have changed due to possible harm when overly strict regulation is pursued. 9,10 In this study, we investigated the prevalence of thiamine deficiency at ICU admission and hypothesized that the administration of insulin and glucose, aimed at regulating serum glucose levels, increases thiamine utilization and therefore might cause or worsen deficiency in patients with limited thiamine stores.
Materials and Methods
Design and Setting
An observational prospective cohort study was carried out between August 2009 and February 2010 in a 10-bed medical–surgical ICU in a general teaching hospital in Apeldoorn, the Netherlands. All adults with an expected ICU treatment of more than 48 hours (as determined by admitting attending physician) and who were thus treated during that time with IIT (see below) were included. Patients were excluded if thiamine supplementation had already been given prior to the study inclusion. During admission, no thiamine supplementation was given except for standard amounts present in enteral feeding (1.9 mg/L). The study protocol was approved by the local ethics committee (TCO 09.24), and written informed consent was obtained from the legal representative of the patient.
Data Collection
The following data were collected: age, gender, weight, height, thiamine and lactate concentration at admission and after 24 and 48 hours, diagnosis upon hospital and ICU admission, length of hospital stay before ICU admission, Acute Physiology, Age and Chronic Health Evaluation (APACHE) II score, Simplified Acute Physiology Score (SAPS) II, and hospital mortality.
Thiamine and Lactate Levels
Blood samples (EDTA and fluoride tubes, Vacutainer; Becton-Dickinson, Franklin Lakes, New Jersey, USA) for measurement of thiamine and lactate were taken at admission and at 24 and 48 hours after admission.
Whole blood thiamine diphosphate concentration was determined by ultrapressure liquid chromatography with fluorescence detection (System/column: Waters, Etten-Leur, the Netherlands; method: Chromsystems, Munich, Germany), which has been shown to be a sensitive indicator of thiamin status. 11 To exclude normal intra-assay variation, relevant change was defined as an increase or decrease of at least twice the assay variance, that is, a change of at least 20% from baseline. Thiamine deficiency was defined as <100 nmol/L based on the normal reference range supplied by the manufacturer.
We hypothesized that induced thiamine deficiency might be demasked by an increase in lactate concentration. Lactate was determined by wavelength absorbance measurement after conversion of lactate into hydrogen peroxide by lactate oxidase (Architect C8000; Abbott Diagnostics, Hoofddorp, the Netherlands), where the increase in absorbance at 548 nm is directly proportional to lactic acid concentration.
Carbohydrate Feeding and Glucose Regulation
According to the local protocol, patients received continuous intravenous glucose (5-15 mL/h glucose 50%) on admission to the ICU, combined with gastric tube feeding starting at 20 to 40 kcal/h (Nutrison Protein Plus; Nutricia, the Netherlands). Gastric residual volume was measured every 6 hours, and if it was <250 mL, enteral feeding was increased while glucose infusion was reduced to prevent an excessively high intake of carbohydrates with inherent risk of hyperglycemia. In line with the protocol in practice at the time of the study, if gastric retention was more than 250 mL, metoclopramide was started. If after another 6 hours, gastric retention was still more than 250 mL, erythromycin was added in prokinetic dosing. If this still did not lead to a gastric retention <250 mL per 6 hours, a duodenal tube was placed. Daily glucose intake was calculated by a dietician (M.G.J.R.) based on the total glucose infusion and enteral glucose intake.
Insulin infusion was adjusted according to a standardized protocol to maintain blood glucose level between 80 and 110 mg/dL, which was in line with the at that time applicable guidelines. Blood glucose was measured every hour while target levels were not reached, otherwise they were measured every 3 hours.
Statistical Analysis
All statistical analyses were performed using the Statistical package for the Social Sciences (version 16.0; SPSS, Chicago, Illinois). Between-group differences in continuous variables were tested using Wilcoxon signed rank test, Mann-Whitney U test, or Friedman analysis of variance test depending on the number and type of measurements. Between-group differences were tested by means of the relative risk (RR) and its 95% confidence interval (CI) for categorical variables. The relation between values in groups was assessed by Spearman correlation coefficient. A P value ≤.05 was considered statistically significant.
Results
Patients
Between August 2009 and February 2010, 66 patients matching inclusion criteria were identified. Eight had already received thiamine supplementation before ICU admission and were therefore excluded. Fifty-eight patients were thus available for final analysis (Table 1). The median age was 73 years (interquartile range [IQR]: 61-79), and 62% were male. Median duration of stay in hospital before admission to the ICU was 1 day (IQR 0-5); 24% were admitted directly from the emergency department. Reason for hospital admission was of gastrointestinal origin in 48% of patients. Forty-seven percent were surgical patients. The median APACHE-II and SAPS-II scores were 19 points (IQR: 12-25) and 45 points (IQR: 34-54), respectively. The median ICU stay was 7 days (IQR: 3-13), and all-cause hospital mortality was 14%.
Patient Characteristics.a
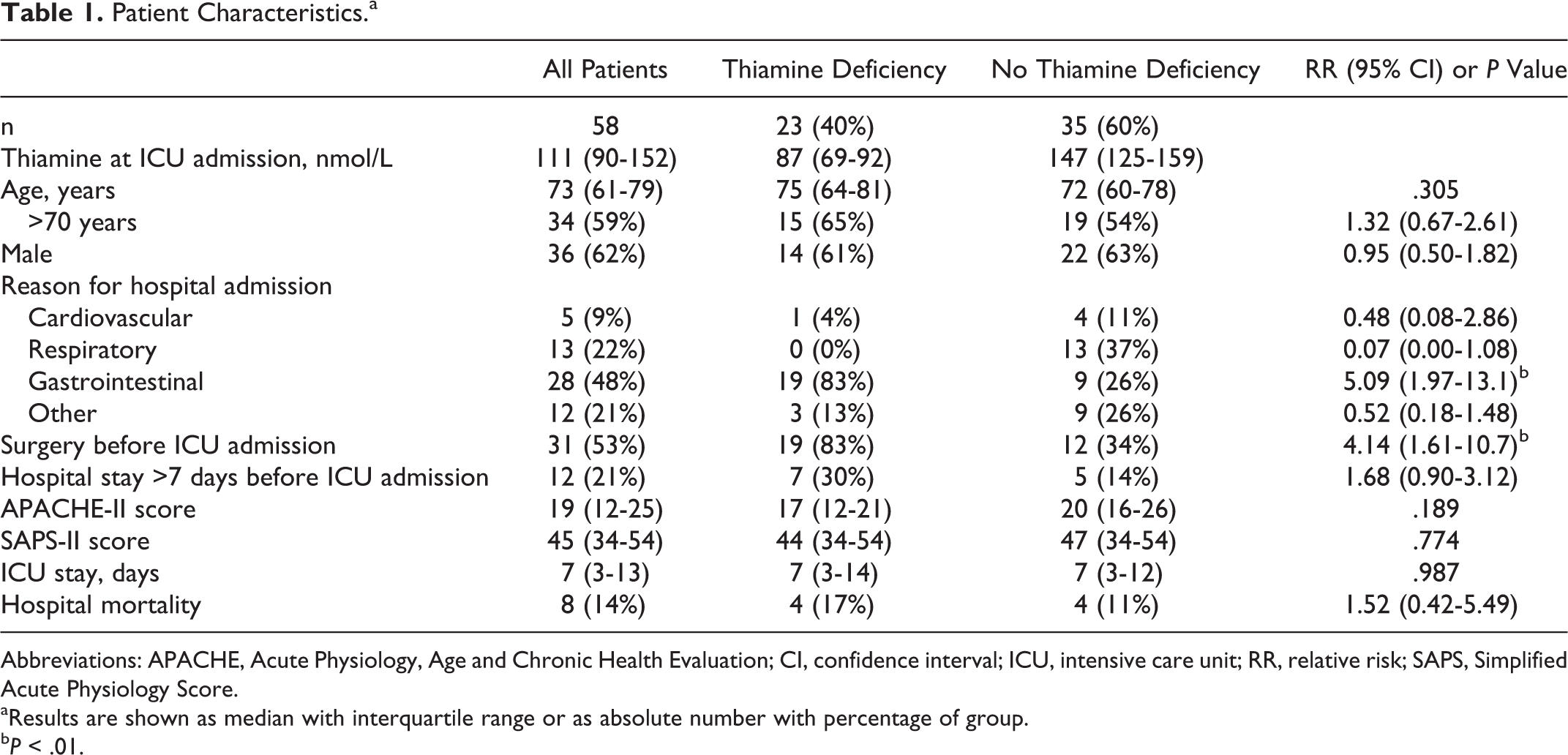
Abbreviations: APACHE, Acute Physiology, Age and Chronic Health Evaluation; CI, confidence interval; ICU, intensive care unit; RR, relative risk; SAPS, Simplified Acute Physiology Score.
aResults are shown as median with interquartile range or as absolute number with percentage of group.
b P < .01.
Thiamine Levels
The median thiamine level at ICU admission was 111 nmol/L (IQR: 90-152). Thiamine deficiency was present in 39.7% of patients at ICU admission, with a median concentration in this subgroup of 87 nmol/L (IQR: 69-92). Thiamine deficiency was associated with gastrointestinal pathology as reason for initial hospital admission (RR: 5.09; 95% CI: 1.97-13.1; P < .01) and with surgery before ICU admission (RR: 4.14; 95% CI: 1.61-10.7; P < .01).
During ICU stay, thiamine levels increased a median of 9 nmol/L (IQR: −4 to 29; P < .01) after 24 hours and 14 nmol/L (IQR: −7 to 40; P < .01) after 48 hours (Figure 1). In patients with thiamine deficiency at admission, levels increased from median 87 nmol/L (IQR: 69-92) at baseline to 99 nmol/L (IQR: 82-138; P < .01) after 48 hours. In patients without deficiency at admission, median level both at admission and after 48 hours was 147 nmol/L (P = .56).
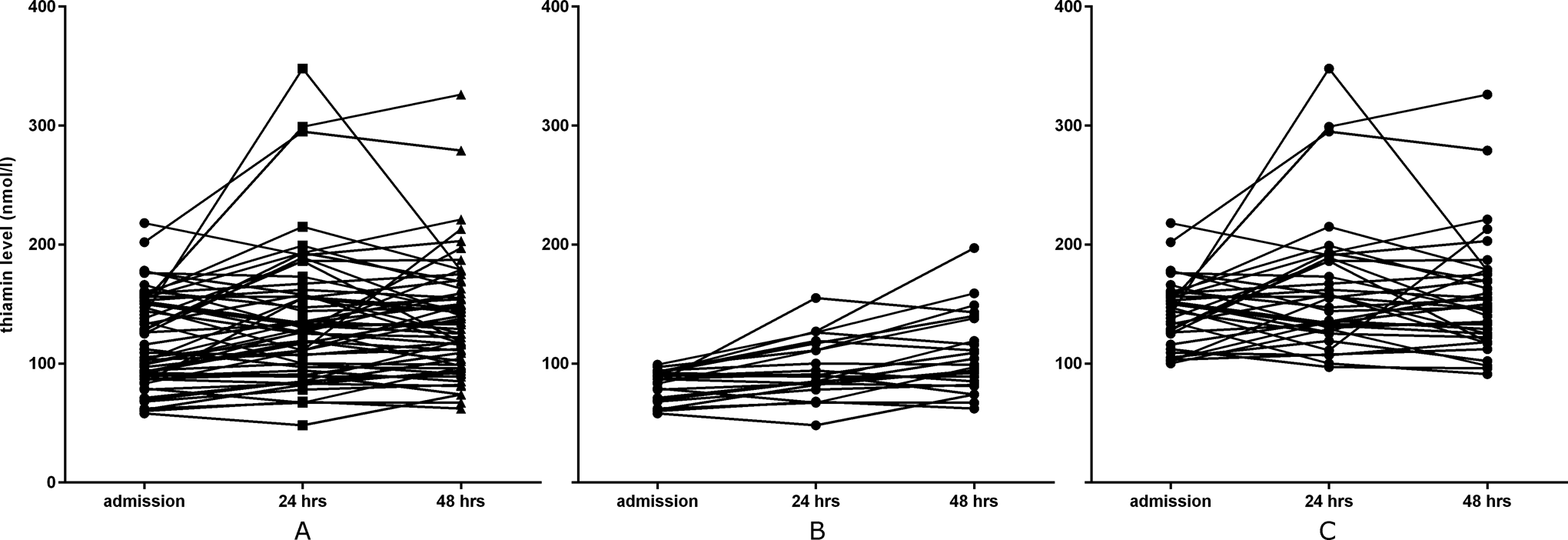
Change in thiamine levels. Panel A, Change in thiamine levels of all 58 patients. Panel B, Change in thiamine levels of 23 patients with thiamine deficiency (<100 nmol/L) at admission. Panel C, Change in thiamine levels of 35 patients in whom thiamine was normal (100 nmol/L) at admission.
An increase or decrease in thiamine level of at least 20% was seen in 37.9% and 3.4%, respectively. Thus, levels did not change in 58.6%. A rise in thiamine levels occurred more frequently in patients with thiamine deficiency at admission than in patients with normal baseline thiamine levels (RR: 2.20; 95% CI: 1.13-4.28; P = .02). The occurrence of change in thiamine concentration was not associated with any other individual patient characteristics nor was the absolute increase in whole blood thiamine correlated with the absolute amount of thiamine present in the total amount of enteral feeding (r = −.05; P = .83). Thiamine deficiency was still present in 25.7% of patients after 48 hours. The presence of thiamine deficiency during ICU admission was not associated with hospital mortality (RR: 1.52; 95% CI: 0.42-5.49; P = .52).
Lactate Levels
The median lactate level at admission was 2.2 mmol/L (IQR: 1.5-3.1), which decreased to 1.4 mmol/L (IQR: 1.1-2.0; P < .001). The median baseline lactate in patients with thiamine deficiency at admission was 3.0 mmol/L compared to 2.0 mmol/L in nondeficient patients (P = .01). The median lactate levels at 24 and 48 hours after admission were not statistically different between these groups. Median increase in thiamine levels was 10.6% (IQR: −6.5% to 43.2%), whereas median decrease in lactate levels was 32.8% (IQR: −55.8 to −4.7%). Change in lactate was inversely related to change in thiamine (r = −.31; P = .017; Figure 2).
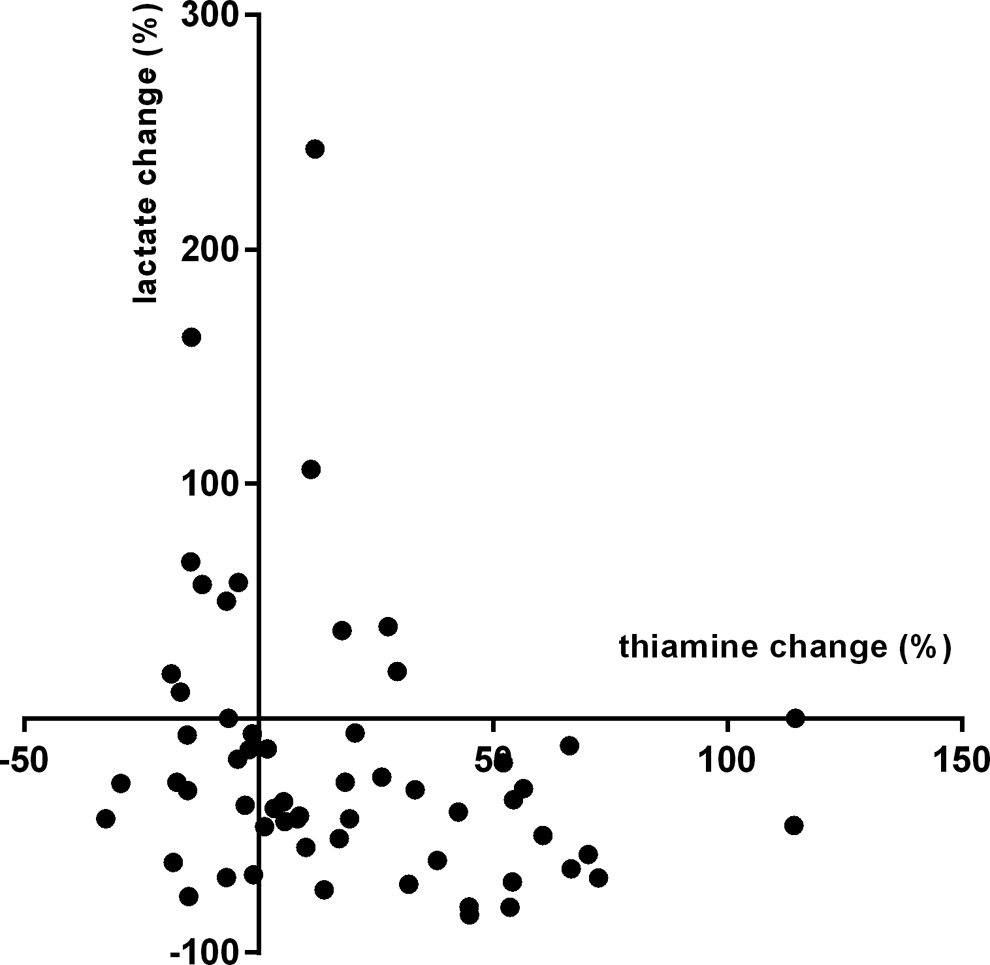
Relation between change in thiamine and lactate levels.
Discussion
This is the first observational prospective study on changes in thiamine levels in ICU patients who are being treated with IIT. We found thiamine deficiency to be present in 39.7% of patients at the time of admission to our ICU. In patients who were being admitted because of gastrointestinal pathology or who had surgery before ICU admission, the prevalence was even higher. Contrary to our hypothesis, we did not see a decrease in whole blood thiamine levels after the initiation of IIT.
Remarkably, little is known about the incidence of thiamine deficiency in critically ill patients. Most of the literature is based on clinical presentation in case reports 2,3,7,12 –17 and few cohort studies. 18 –22 Clinical recognition of thiamine deficiency is difficult because of the vague and nonspecific neuropsychiatric symptoms with which it often presents, such as diffuse weakness, fatigue, and cognitive impairment. 23 –25 Especially in critically ill patients, these symptoms can quickly be overlooked or attributed to the underlying disease, and only very few patients progress to develop classic signs of beriberi.
The prevalence of thiamine deficiency in our population was much higher than the 10% to 20% reported by other authors. 18 –21 Only one recent study on patients with severe sepsis found a comparably high baseline prevalence of thiamine deficiency. 26 This might be explained by the large number of patients in our cohort who were admitted because of gastrointestinal pathology or after recent surgery and therefore had a high risk of preexistent malnutrition and a systemic inflammatory response. Gastrointestinal pathology is a common feature in case reports on symptomatic thiamine deficiency. 3,13 Furthermore, it has been shown that major surgery, as a surrogate for the stress of critical illness, causes additional reduction in thiamine levels. 22,27 We found the prevalence of thiamine deficiency in patients admitted for reasons other than gastrointestinal pathology to be comparable to that reported in most literature. Another possible reason for the higher than normal prevalence might be the high median age of patients in our cohort. Although age was not associated with thiamine deficiency in our study, other authors have found a comparably high prevalence and positive association with age in elderly volunteers, independent of underlying comorbidity. 28,29
We hypothesized that the high glucose and insulin given in the context of IIT might increase the utilization of thiamine and therefore might cause thiamine deficiency with a resulting increase in serum lactate. Despite having a catalytic role, thiamine destruction does occur when it is utilized in a reaction with pyruvate decarboxylase. 30 A decline in thiamine concentration has been found by other authors examining the effect of critical illness or surgery on thiamine concentration in populations not treated with IIT. 18,21,22,27 More in parallel to our hypothesis, thiamine levels declined in a cohort of children after initiation of insulin therapy as treatment for diabetic ketoacidosis. 21 However, contrary to our hypothesis, we found a small but statistically significant increase in whole blood thiamine and decrease in lactate concentration during the first 48 hours of admission in our patients. This increase might be explained by the amount of thiamine present in our enteral feeding formula, which is higher than the recommended daily intake for healthy adults of 1.2 mg/d. 31 Thus, patients who are not receiving any thiamine through enteral feeding or by other means of supplementation might still be at increased risk for development or worsening of thiamine deficiency.
An inverse association of thiamine and lactate levels has also been reported by other authors. 18,27,32 Although thiamine deficiency can cause increased lactate production, there are numerous other and probably more important factors influencing lactate production and clearance not accounted for in our analysis. Whether the higher baseline lactate level in the thiamine-deficient group is a result of the thiamine deficiency itself or merely an indication of more serious underlying illness cannot be answered by our data.
Limitations of our study include the lack of a control group, which raises the possibility of confounding. However, this would have affected our conclusion only if we had found a decrease in thiamine concentration or increase in lactate, which then might have been attributed to other factors or the disease state itself. Because IIT was, at the time of the study, thought to be beneficial, it would furthermore have been unethical to deny this standard of care to the control group. Another issue we faced is the absence of evidence on which to define a clear cutoff value used for determining thiamine deficiency. We used 100 nmol/L as is reported by our laboratory, although other authors have used different cutoff values and different methods for determining thiamine concentrations, making a direct comparison difficult. A notable difference between our IIT protocol and the classic Leuven protocol is the decrease in glucose infusion as enteral feeding was increased, resulting in an unchanged calorie intake and therefore lowering the risk of hyperglycemia. Another difference between the protocol used during data collection and contemporary guidelines is the glucose target range of 80 to 110 mg/dL, which has in most ICUs changed to a less strict target of 80 to 150 mg/dL. However, we believe our results are still applicable in current clinical practice, as these changes in guidelines do not influence baseline prevalence of thiamine deficiency and are unlikely to result in a change of thiamine status during treatment, given the shown absence of thiamine decrease during our more strict glucose regulation.
In conclusion, IIT or strict glucose regulation does not appear to cause or worsen thiamine deficiency. However, based on the high prevalence of deficiency at admission, it might still be warranted to supplement thiamine (eg, 100 mg once daily for up to 2 weeks) in all patients admitted to the ICU, especially when there is underlying gastrointestinal disease or recent surgery. Whether this actually has an effect on clinical outcomes should be the subject of further research.
Footnotes
Authors’ Note
Wouter van Snippenburg was responsible for the interpretation of the results and the writing of the manuscript. Mariet Reijnders and Jose Hofhuis participated in the development of the protocol and the data collection. Rien de Vos participated in the methodological development of the study protocol. Stephan Kamphuis participated in the development of the protocol and the data collection. Peter Spronk participated in the development of the protocol, the data collection and analysis, and drafting of the manuscript. All authors reviewed and approved the final manuscript and agree to be fully accountable for ensuring the integrity and accuracy of the work.
Acknowledgments
The authors would like to thank Albertine Pors-Horssen for her assistance in literature research and Hans Rommes, Aly Hovingh and Tineke Havekes for their assistance in data collection and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.