
Abstract
Objectives:
To evaluate the relationship between rates of discharge directly to home (DDH) from the intensive care unit (ICU) and bed availability (ward and ICU). Also to identify patient characteristics that make them candidates for safe DDH and describe transfer delay impact on length of stay (LOS).
Methods:
Retrospective cohort study of all adult patients who survived their stay in our medical–surgical–trauma ICU between April 2003 and March 2015.
Results:
Median age was 49 years (interquartile range [IQR]: 33.5-60.4), and the majority of the patients were males (54.8%). Median number of preexisting comorbidities was 5 (IQR: 2-7) diagnoses. Discharge directly to home increased from 28 (3.1% of all survivors) patients in 2003 to 120 (12.5%) patients in 2014. The mean annual rate of DDH was between 11% and 12% over the last 6 years. Approximately 62% (n = 397) of patients waited longer than 4 hours for a ward bed, with a median delay of 2.0 days (IQR: 0.5-4.7) before being DDH. There was an inverse correlation between ICU occupancy and DDH rates (rP = −.55, P < .0001, 95% confidence interval [CI] = −0.36 to −0.69, R2 = .29). There was no correlation with ward occupancy and DDH rates (rs = −.055, P = .64, 95% CI = −0.25 to 0.21).
Conclusions:
The DDH rates have been increasing over time at our institution and were inversely correlated with ICU bed occupancy but were not associated with ward occupancy. The DDH patients are young, have few comorbidities on admission, and few discharge diagnoses, which are usually reversible single system problems with low disease burden. Transfers to the ward are delayed in a majority of cases, leading to increased ICU LOS and likely increased overall hospital LOS as well.
Introduction
There is an increasing proportion of discharges directly to home (DDHs) from intensive care units (ICUs), bypassing the traditional transfer to ward protocols prior to hospital discharge. 1 –3 Clinicians seem to have accepted the emerging practice of DDH as necessary because decreasing bed availability is a new reality; so, adapting to this new environment is of significant importance. Currently, there is sparse literature evaluating the practice of DDH, 2 –6 despite its increasing frequency. There are 4 palliative care (oncological ICU, surgical ICU, or patients diagnosed with cancer) publications of ICU patients who were discharged to homes or hospices. 2 –5 One manuscript in the cardiology literature described DDH from an acute care setting as feasible. 6 Potential reasons for the increasing DDH trend include decreasing ward and ICU bed availability, improved community support, and increasing intensivist comfort with the practice. Rather than continuing this new practice of DDH blindly, we propose studying it. It is important for health-care practitioners to better understand why more patients are being sent home directly from the ICU and who may be sent home safely. Safe DDH can improve health-care resource utilization, reduce iatrogenic hospital-acquired morbidity, improve patient satisfaction, and reduce health-care-associated costs. This study will influence the health-care system and direct patient care by informing our ICU discharge protocols (avoiding the traditional transfer to ward). Hence, we initiated the Direct from ICU Sent to Home (DISH) Study to investigate this further.
The primary objective of this retrospective study is to evaluate the association between rates of DDH and bed availability (both in the ICU and in the ward), as an association has not previously been demonstrated in the literature. Our secondary objectives include describing the demographics and clinical characteristics of patients DDH from ICU over a recent 6-year period. Another objective is to describe the overall length of stay (LOS) and the length and types of transfer delays to the ward and to hospital discharge.
Our hypothesis is that an association exists between DDH rates and bed occupancy. We expect to identify a positive correlation between DDH rates and both ICU and ward occupancy. We predict that young age, few comorbidities, and discharge diagnoses (simple, single-system disease processes) will be associated with safe DDH.
Materials and Methods
This study was reviewed by local institutional review boards (Western University Research Ethics Board and Lawson Health Research Institute) and received delegated health sciences approval.
Study Design and Setting
A retrospective cohort design was utilized to identify and describe patients who were DDH from our 26-bed Canadian medical–surgical–trauma ICU at London Health Sciences Centre (LHSC). The LHSC is a 507-bed academic, tertiary care referral center in London, Ontario, Canada. The Critical Care Trauma Centre (CCTC) cares for patients with multiple trauma, surgical procedures (vascular, thoracic, obstetric/gynecological, head and neck, urological, orthopedic, general), and oncological and complex medical disorders.
Data Collection
Data from ICU discharges between April 2003 and March 2015 were extracted using our own critical care database (Critbase). Data from Critical Care Information Service (CCIS—a provincial database) and LHSC corporate metrics data were not fully available until January 2009. Thus, the more comprehensive retrospective cohort analyses of DDH from CCTC were conducted between January 2009 and December 2014 (n = 642 patients).
Data collected included age, gender, preexisting comorbidities, Multiple Organ Dysfunction Score (MODS), 7 Nine Equivalents of Nursing Manpower Score (NEMS), 8 discharge diagnoses, home discharge destination (within or outside London, Ontario), total ICU LOS, and length of transfer delay (time lag between when a patient was ready to leave the ICU and the actual time of transfer/discharge). The total number of preexisting comorbidities was tallied using International Statistical Classification of Diseases Revision (ICD-10) from the patient’s chart and medical history. Likewise, discharge diagnoses were determined using the same ICD-10 criteria and tallied using the main discharge diagnosis plus any other additional contributing diagnoses (new or old) during the ICU admission.
Bed occupancy data were collected from LHSC corporate metrics data sources with regard to occupancy in the ICU and ward occupancy.
Statistical Analysis
Descriptive statistics were generated for demographic, clinical, and outcome parameters. Continuous data (age, MODS, NEMS, transfer delays, LOS, DDH rates) were presented as mean ± standard deviation or median and interquartile range where violations in normality occurred. Categorical data (gender, discharge location, discharge diagnoses) were summarized as total number and percentage of the entire cohort. These statistical analyses were performed with Microsoft Excel, version 14.0.6.
To investigate whether associations exist between ICU occupancy and DDH rates or between ward bed occupancy and DDH rates, coefficients of correlation and the corresponding significance values were calculated. Pearson product–moment correlation coefficients 9 or Spearman rank-order correlation coefficients 10 are reported depending on the distribution of data included. These statistical analyses were performed using Statistical Analysis Software (SAS), version 9.4.
Results
Baseline Demographics and Clinical Characteristics
We identified 642 patients who were DDH from the ICU between January 2009 and December 2014.
For the overall study group (Direct from ICU Sent Home patients—Table 1), the median age was 49 years (interquartile range [IQR]: 33.5-60.4). Males comprised 54.9% of all DDH patients. The median number of preexisting comorbidities was 5 (IQR: 2-7) medical diagnoses contributing to their admission. Patients were discharged home within London 63.7% of the time. The median total ICU LOS was 3 days (IQR: 1.6-5.7). The median total number of discharge diagnoses was 1 (IQR: 1-2).
Baseline Demographics and Clinical Characteristics of All Direct Discharge to Home From Intensive Care Unit Patients (January 2009-December 2014).
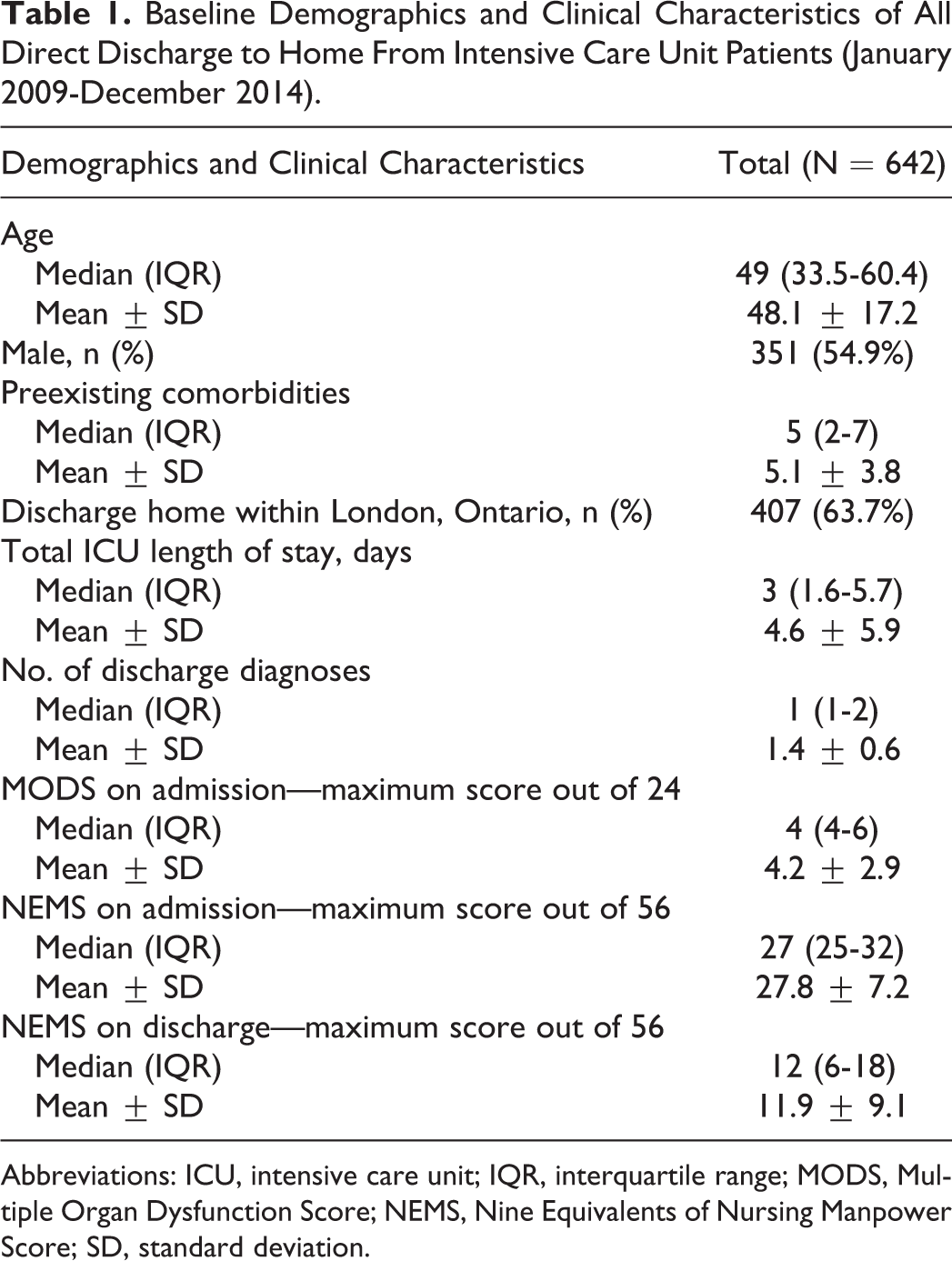
Abbreviations: ICU, intensive care unit; IQR, interquartile range; MODS, Multiple Organ Dysfunction Score; NEMS, Nine Equivalents of Nursing Manpower Score; SD, standard deviation.
To quantify illness severity and burden of disease in the ICU for our DDH patients, we examined MODS and NEMS available from CCIS. For DDH patients, median MODS on admission was 4 (IQR: 4-6). Median NEMS on admission was 27 (IQR: 25-32). Median NEMS at discharge was 12 (IQR: 6-18).
Increasing DDH Rates Over Time
All the direct discharge patients (n = 1109) who were discharged from ICU to home between the fiscal years 2003 and 2015 are shown in Figure 1. As illustrated, there has been an increase in DDH rates over time both in absolute number and also as in a proportion of all survivors who were discharged from the ICU. In 2003 to 2004, there were 28 DDH patients (3.1% of all ICU survivors). This has increased to 120 DDH patients (12.5% of all survivors) over the past year. In the past 6 years, approximately 11% to 12% of all ICU survivors (109-122 patients per year) from the ICU are being directly discharged home.
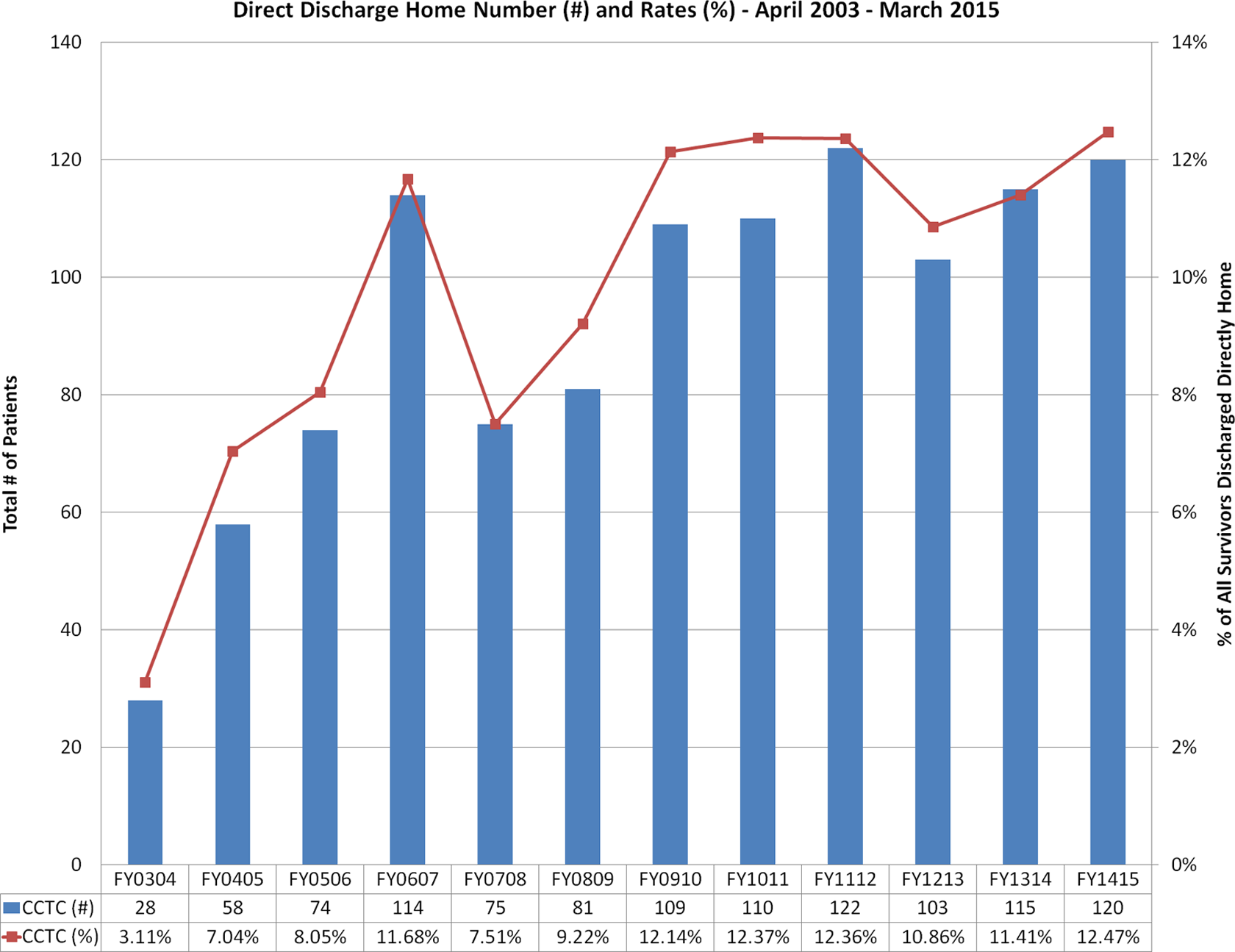
Direct discharge home from ICU (April 2003-March 2015). Absolute number of DDH patients represented by blue bars, percentage of total survivors represented by the red line. DDH indicates discharge directly to home; ICU, intensive care unit.
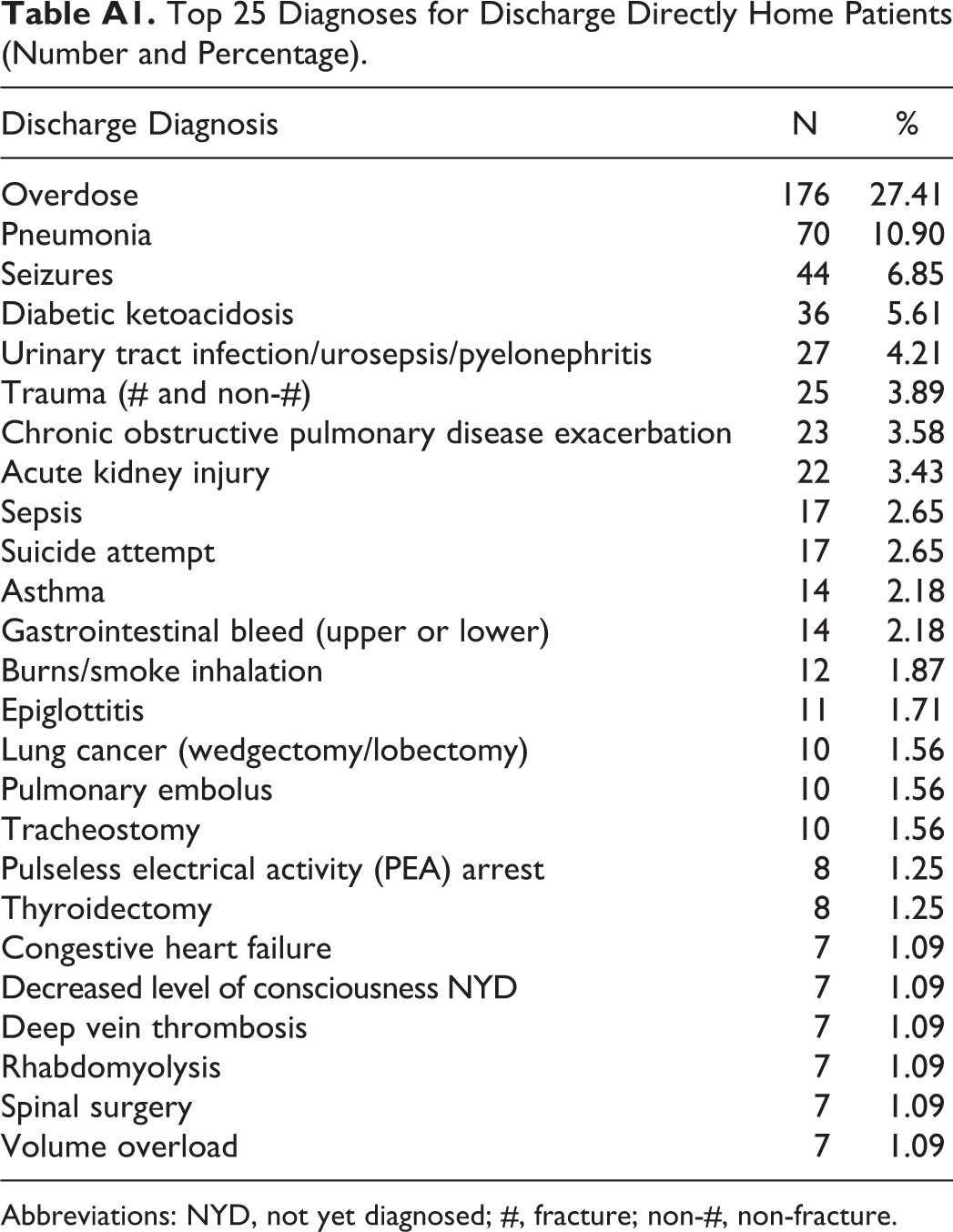
Discharge Diagnoses
The top 25 discharge diagnoses for our DDH patient cohort can be found in Appendix A. The 5 most common discharge diagnoses for patients who are DDH are overdose (176 patients, 27.4%), pneumonia (70 patients, 10.9%), seizures (44 patients, 6.9%), diabetic ketoacidosis from type I diabetes mellitus (36 patients, 5.6%), and urinary tract infection/urosepsis/pyelonephritis (27 patients, 4.2%). The remainder of the top 25 diagnoses were primarily single-system, reversible diagnoses.
Transfer to Ward Delays
The median time window between the request for a ward bed and patient transfer is approximately 4 hours, when a bed is immediately available. We defined 4 hours as a discriminatory cutoff for a “delay” in transfer from the ICU.
In Table 2, there were 167 (26.0%) patients in the DDH patient cohort who were never listed for the ward, as the first initial disposition plan for those patients was to be DDH. The remaining patients were categorized as having had transfer delays to the ward of either less than 4 hours or greater than 4 hours. Many patients who had transfer delays <4 hours (78 patients, 12.1%) were initially listed for the ward, but were DDH shortly thereafter, within 4 hours.
Occurrence of, and Reasons for, Ward Transfer Delay.
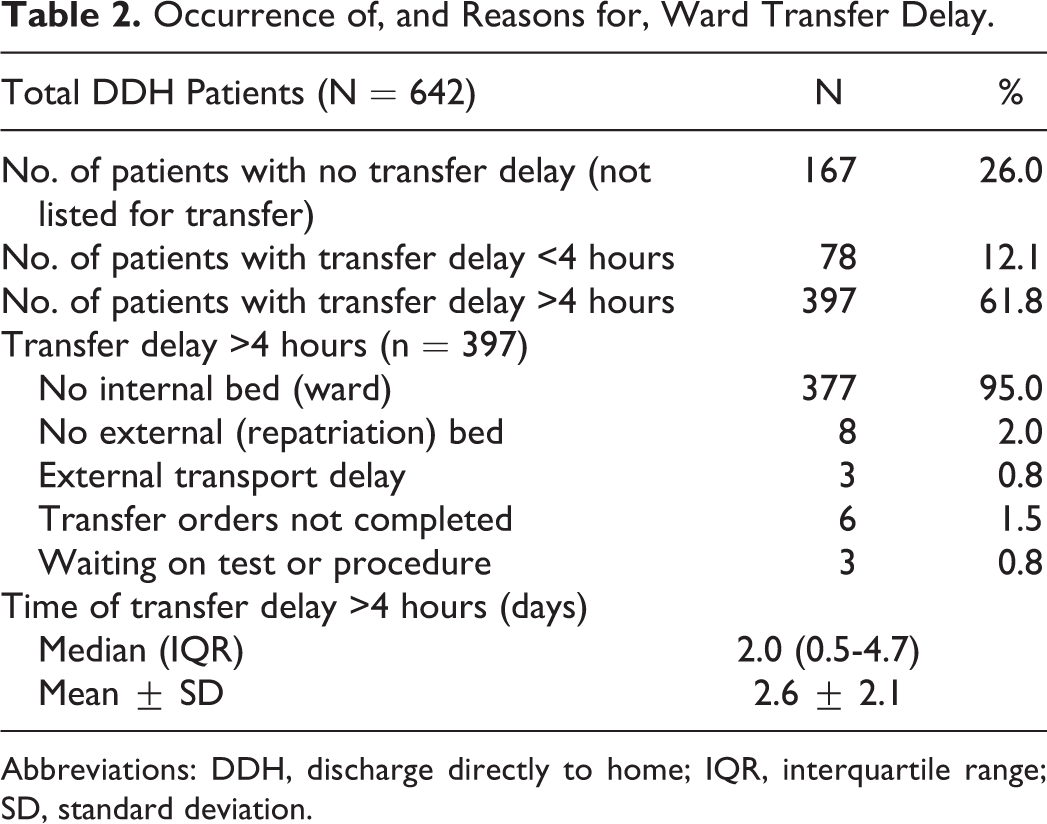
Abbreviations: DDH, discharge directly to home; IQR, interquartile range; SD, standard deviation.
The patients who sustained transfer delays to the ward >4 hours (394 patients, 61.8%) were listed for an extended period of time before finally being DDH. The reasons for the delay were the following: no internal ward bed (377 patients, 95%), no repatriation (external) bed (8 patients, 2%), delay in external transport (3 patients, 0.8%), transfer orders not complete (6 patients, 1.5%), and waiting on a test or procedure (3 patients, 0.8%) made up the minority of the remaining transfer delays. Moreover, when there was a transfer delay of >4 hours, the median delay was 2 days (IQR: 0.5-4.7), with a mean of 2.6 ± 2.1 days.
Intensive Care Unit and Ward Occupancy
Figure 2 shows the overall ICU occupancy and combined ward (medical/surgical) occupancy at Victoria Hospital (VH) as a census average for each month. The red line in each of the graphs represents 100% occupancy for both the ICU and the ward, above which indicates being over-census.
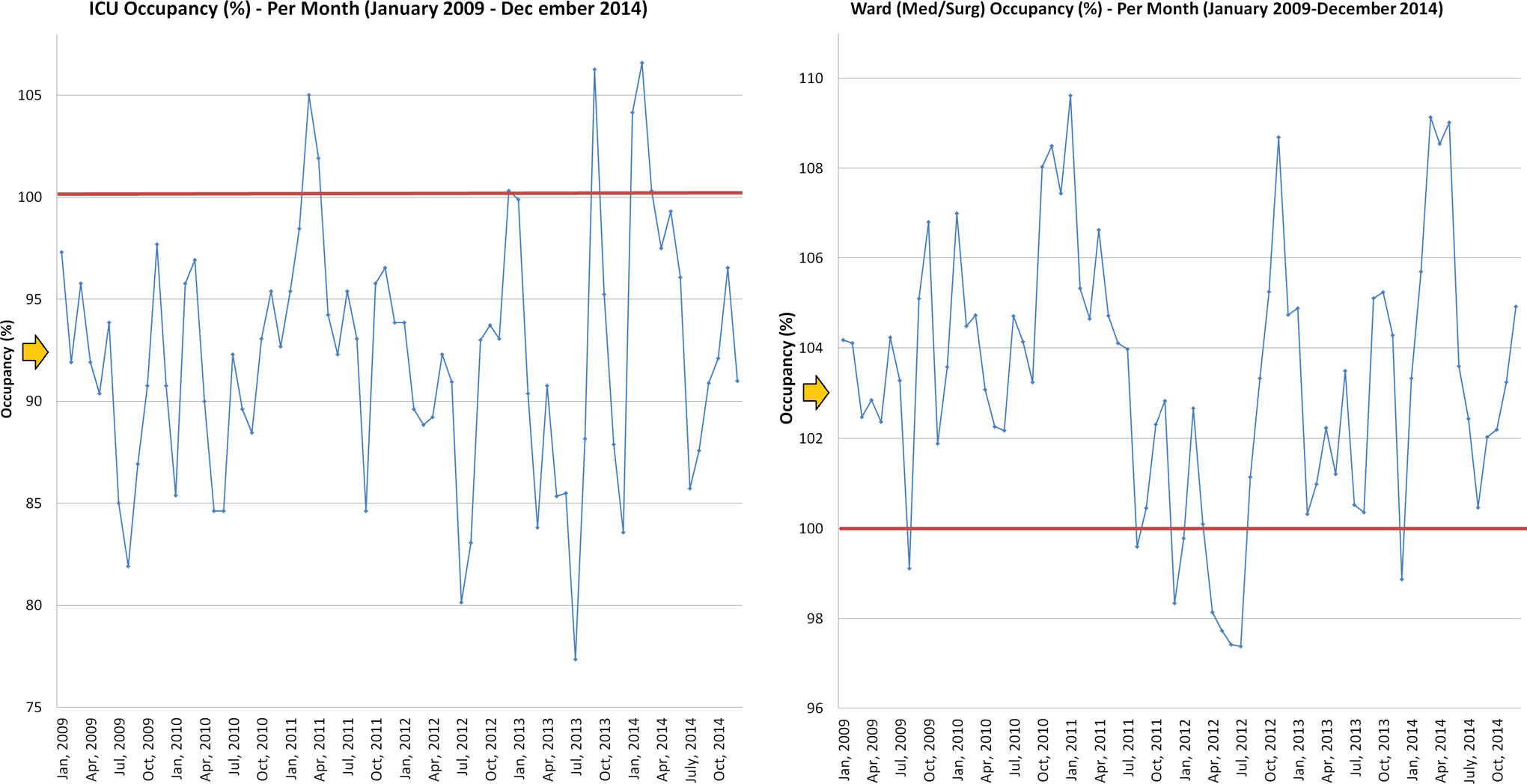
Overall ICU occupancy and ward (medical/surgical) occupancy at Victoria Hospital. Solid red line represents 100% occupancy. Orange arrows represent median occupancy. ICU indicates intensive care unit.
The ICU median occupancy was 92.3% (IQR: 88.4%-95.8%). The ICU occupancy was over-census in 7 (9.9%) of 72 months during the study period. However, the VH ward median occupancy was 103.3% (IQR: 101.7%-104.9%). Furthermore, the VH ward occupancy was over-census in 62 (87.3%) of 72 months during the study period.
Occupancy and Correlation With DDH
Figure 3 shows the correlation between ICU occupancy and the rate of DDH from ICU, as well as ward occupancy and the rate of DDH from ICU. Linear regression demonstrated a negative correlation between ICU occupancy and DDH rate. The scatter plot is normally distributed, hence, we are able to calculate Pearson product–moment correlation coefficient to be −0.55 (P < .0001, 95% confidence interval [CI] = −0.36 to −0.69, R2 = .29).
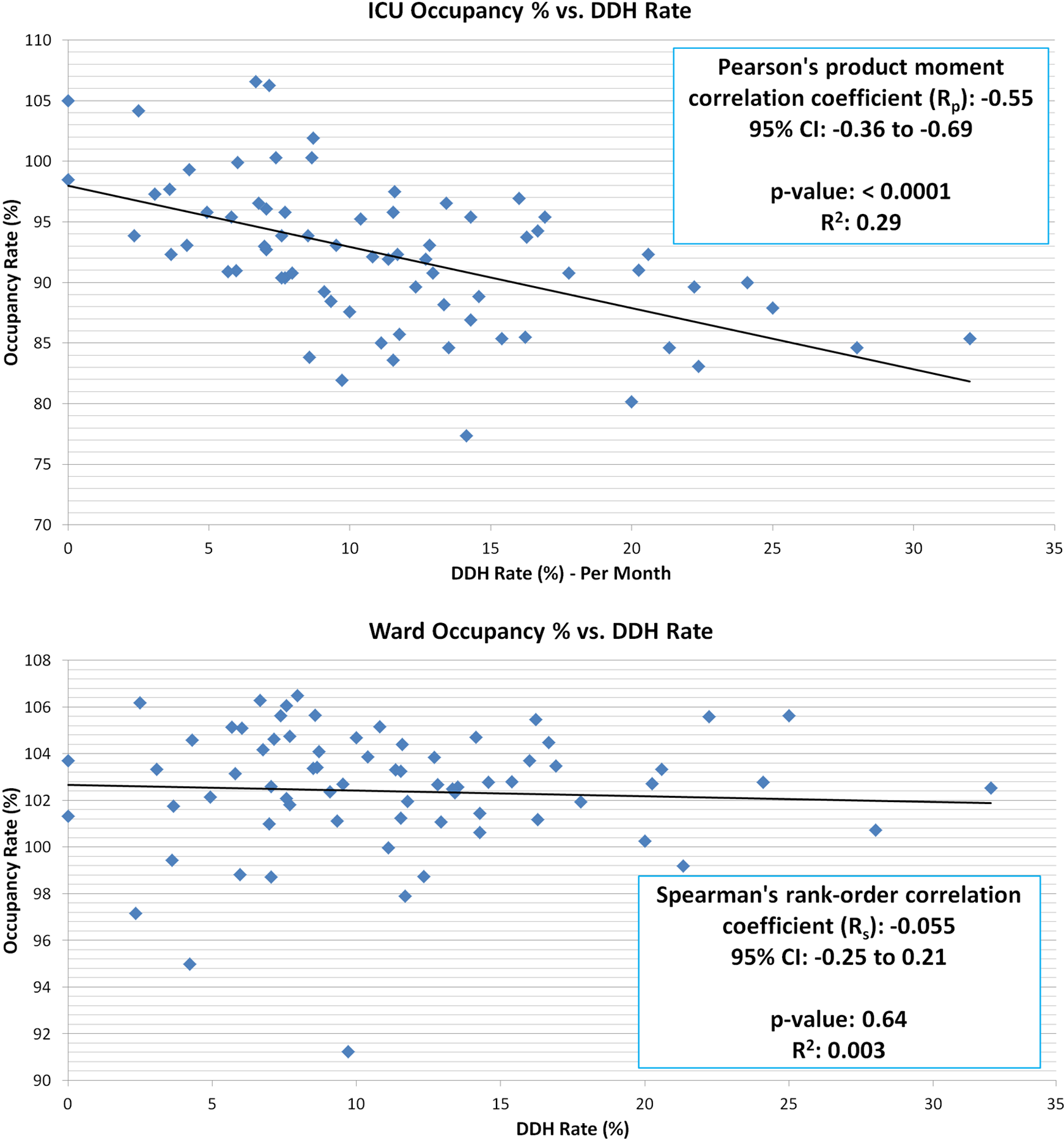
Correlation between ICU and ward occupancy and discharge directly to home rates (2009-2014). ICU indicates intensive care unit.
However, the ward (medical/surgical) occupancy did not demonstrate any correlation with DDH. The data were not normally distributed, hence, the Spearman rank-order correlation coefficient is −0.055 (P = .64, 95% CI: −0.25 to 0.21, R2 = .0030).
Discussion
We report an increasing rate (from 3% to 12%) and number (28 patients to 120 patients per year) of DDHs from ICU between 2003 and 2015, bypassing ward transfer protocols. This is greater than the 4% average rate per year of DDH from the Acute Physiology and Chronic Health Evaluation IV data set. 2,11
An inverse correlation (Pearson correlation coefficient = −0.55, P < .0001, 95% CI = −0.36 to −0.69) was identified between ICU bed occupancy and DDH rates. When ICU occupancy was low, rates of DDH increased. This is contrary to our original hypothesis that high rates of ICU occupancy would lead to higher rates of DDH. Also, it was surprising to find no significant correlation (Spearman correlation coefficient = −0.055, P = .64) with ward bed occupancy and rates of DDH. We anticipated a positive correlation; more patients DDH from ICU when wards are over census.
We can hypothesize a few reasons for our findings. The average ICU occupancy census is 92.2% ± 6.1%, with occupancy over-census occurring in only 7 (9.9%) of 72 months. However, the average ward occupancy was 103.3% ± 2.9%, with occupancy over-census occurring in 62 of 72 months (87.3%). Because ward occupancy is chronically high, it would be difficult to show a positive correlation with DDH rates. Furthermore, the inverse correlation between ICU census and DDH rates likely has to do with ICU bed pressure to the receiving wards. When ICU census is high, there is an increased pressure on the wards to accept ICU transfers (even when ward census is high). However, during times of low ICU census, there is less pressure to transfer patients to the ward, and therefore, patients seem to complete their rehabilitation in ICU rather than the ward and are subsequently DDH from ICU.
Unpublished data from our postcardiac surgery ICU bed flow demonstrates that postoperative cardiac surgery patients whose ward transfers are delayed due to lack of ward beds have increased hospital lengths of stay. Even though the patients are rehabilitating from their surgery in the Cardiac Surgery Recovery Unit (CSRU), and make it to the ward a few days later, their discharge time on the floor doesn’t take into account their overall LOS in the hospital and LOS in the CSRU. The wards tend to keep their patients the requisite 1 to 3 days despite their added day(s) in the cardiac ICU, thereby increasing their total hospital LOS. We suspect that if our DDH patients from ICU had been transferred to the wards, it would have prolonged total hospital LOS in much the same way as it does in the cardiac cohort. We’ve already demonstrated an unnecessary median 2 days (IQR: 0.5-4.7) of increased ICU LOS associated with transfer delays to ward >4 hours. Alleviating bed flow issues in the ICU could potentiate for cost savings. 12
Staff consultants are already bypassing ward transfers and discharging patients directly home in 26% of cases. Still, a proportion of patients had transfer delays <4 hours (78 patients, 12.1%) and were listed for the ward, but when a ward bed was not available, the disposition was changed to DDH to avoid an unnecessary rehabilitation in the ICU. This means the patients were likely ready for home all along. Hence, there was likely a decision between the patient, their attending, and the attending team to not wait for a bed on the ward but to simply discharge the patient home.
A significant proportion of patients (36.3%) were discharged to homes outside London, evidence of physician comfort with DDH to homes outside our catchment area (approximately 21 639 km2 total, 83 km radius).
The inverse correlation between ICU occupancy and DDH, and the lack of correlation between ward occupancy and DDH rates, is a novel finding. Ours is the first study to demonstrate the feasibility of discharging a general ICU population directly home. Discharging these patients home sooner may reduce iatrogenic complications and improve patient comfort.
The use of clinical decision tools is increasing rapidly in medicine. Rigorously derived and validated prediction models improve clinical judgment. 13 –18 The use of a clinical prediction tool to guide DDH could improve the safety of the practice, decrease both ICU and hospital lengths of stay, and improve physician comfort. 19 –21 The identification of the safe DDH demographics (age) and clinical characteristics (preexisting comorbidities, discharge diagnoses, MODS, NEMS, etc) and a validated safety prediction model are needed.
Strengths and Limitations
Our study had several strengths. Its period of study, which was over a decade (2003-2015), is substantial to show the trend toward increased DDH rates over time. The retrospective cohort was also sizable for the time period, and the findings of inverse correlation of DDH and ICU occupancy were novel.
However, our study also has several limitations. Its retrospective nature and lack of outcome data (mortality, morbidity, emergency department bounce backs, readmissions to ICU, and ward) create bias and limit our ability to draw meaningful conclusions about DDH safety. The single-center nature of our data limits its generalizability. Also, our findings are derived from the Canadian Universal Health Care System. As the Canadian population develops more elderly patients, there is a diminishing inpatient bed capacity, promoting direct discharges home from ICU. Lesser developed countries and/or those with different ward to ICU bed ratios may have very different ICU discharge practices. Validating our prediction tool in diverse health-care environments will be important for generalizability.
Conclusion
The practice of DDH from ICU may be increasing (as demonstrated by our single-centered study). Discharge directly to home has an inverse association with ICU occupancy but no association with ward occupancy. Discharge directly to home patients are young and healthy, have few comorbidities, and have few discharge diagnoses. Their diagnoses are usually reversible single-system problems with low disease burden. Many ward transfers are delayed due to ward congestion, leading to overall increased hospital LOS. Future studies should validate our predictors of safe DDH and evaluate the effect of home supports, patient and family satisfaction, and the health economic sequelae of DDH.
Footnotes
Appendix A
Top 25 Diagnoses for Discharge Directly Home Patients (Number and Percentage).
| Discharge Diagnosis | N | % |
|---|---|---|
| Overdose | 176 | 27.41 |
| Pneumonia | 70 | 10.90 |
| Seizures | 44 | 6.85 |
| Diabetic ketoacidosis | 36 | 5.61 |
| Urinary tract infection/urosepsis/pyelonephritis | 27 | 4.21 |
| Trauma (# and non-#) | 25 | 3.89 |
| Chronic obstructive pulmonary disease exacerbation | 23 | 3.58 |
| Acute kidney injury | 22 | 3.43 |
| Sepsis | 17 | 2.65 |
| Suicide attempt | 17 | 2.65 |
| Asthma | 14 | 2.18 |
| Gastrointestinal bleed (upper or lower) | 14 | 2.18 |
| Burns/smoke inhalation | 12 | 1.87 |
| Epiglottitis | 11 | 1.71 |
| Lung cancer (wedgectomy/lobectomy) | 10 | 1.56 |
| Pulmonary embolus | 10 | 1.56 |
| Tracheostomy | 10 | 1.56 |
| Pulseless electrical activity (PEA) arrest | 8 | 1.25 |
| Thyroidectomy | 8 | 1.25 |
| Congestive heart failure | 7 | 1.09 |
| Decreased level of consciousness NYD | 7 | 1.09 |
| Deep vein thrombosis | 7 | 1.09 |
| Rhabdomyolysis | 7 | 1.09 |
| Spinal surgery | 7 | 1.09 |
| Volume overload | 7 | 1.09 |
Abbreviations: NYD, not yet diagnosed; #, fracture; non-#, non-fracture.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.