
Abstract
Purpose:
Bloodstream infections (BSIs) caused by Acinetobacter species have been extensively reported, however, which majorly focused on respiratory tract infections. The risk of mortality and the effect of early catheter removal on survival in catheter-related BSIs (CRBSIs) caused by Acinetobacter spp. remain unclear. This study aims to investigate that.
Methods:
This is a retrospective multicentric study conducted in Taiwan from 2012 to 2014. Patients with at least 1 positive blood culture and catheter culture for the same Acinetobacter spp., showing symptoms and signs of CRBSIs, were included (n = 119). Risk factors for 30-day mortality were analyzed using a logistic regression model. The characteristics of patients with early catheter removal (within 48 hours after CRBSIs) were compared to those without removal matching for age, sex, and disease severity.
Results:
There were no differences in 30-day mortality with regard to causative Acinetobacter spp., catheter type, site, and appropriateness of antimicrobial therapy. Patients with higher Acute Physiologic and Chronic Health Evaluation (APACHE) II scores (odds ratio [OR]: 1.12; 95% confidence interval [CI]: 1.02-1.23; P = .014), shock (OR: 6.43; 95% CI: 1.28-32.33; P = .024), and longer hospitalization before CRBSIs (OR: 1.04; 95% CI: 1.00-1.08; P = .027) had a significantly higher 30-day mortality rate. Early removal of catheters after CRBSIs was not associated with better survival benefits.
Conclusion:
Higher disease severity (APACHE II score), shock, and longer hospitalization before bacteremia were independently associated with a higher 30-day mortality in CRBSIs caused by Acinetobacter spp. In previous published guidelines, infected catheters were suggested to be removed in CRBSIs caused by gram-negative bacilli. Even though early removal of catheters did not associate with a better survival outcome in current results, it should be judiciously evaluated according to the clinical conditions and risks individually. For better elucidation of these issues, further well-controlled prospective study may be warranted.
Introduction
Acinetobacter species are emerging nosocomial pathogens. 1 The prevalence of bloodstream infections (BSIs) caused by Acinetobacter spp. is increasing among immunocompromised hosts and intensive care units (ICUs) patients. 2 –4 The most clinically relevant Acinetobacter spp. are A. baumannii, A. nosocomialis, and A. pittii and are together referred to as the A. baumannii (Ab) group.
In addition to primary bacteremia without an obvious source, the most frequent infectious sources of BSIs caused by Acinetobacter spp. are pneumonia and catheter-related infections. 5 –7 Although pneumonia caused by Acinetobacter spp. has been extensively reported, 8 –12 there were limited studies elucidating the risk of mortality for catheter-related BSIs (CRBSIs) caused by Acinetobacter spp. 4 The management of intravascular catheters in patients with BSIs is affected by several factors, including the characteristics of the causative pathogens. For example, catheter removal resulted in more favorable clinical responses and lower risks of complications in CRBSIs caused by Staphylococcus aureus; however, in those caused by coagulase-negative Staphylococcus species, the advantages of catheter removal were not as obvious. 13 –16
In CRBSIs caused by gram-negative bacilli (GNBs), catheter removal was recommended within 48 to 72 hours to prevent BSI relapse. 17 Catheter removal has also been recommended in CRBSIs caused by higher virulence GNBs, such as Pseudomonas aeruginosa. 18 However, in CRBSIs caused by Acinetobacter spp., early catheter removal outcome has not been determined. This study aims to investigate the risk factors of mortality and the impact of catheter retention or early removal in patients with CRBSIs caused by Acinetobacter spp.
Materials and Methods
Study Population
This retrospective study was conducted at 4 medical centers in Taiwan—the Changhua Christian Hospital (CCH, 1676 beds); Mackay Memorial Hospital (MMH, 2055 beds); Taipei Veterans General Hospital (TVGH, 2900 beds); and Tri-Service General Hospital (TSGH, 1712 beds) of National Defense Medical Center, from January 2012 to December 2014.
Patients with at least 1 positive blood culture yielding Acinetobacter spp. and infection-related symptoms and signs were included in the study. In cases where 2 or more positive blood cultures were available, only the first blood culture was included. The CRBSI was defined as the presence of catheter exit site inflammation and a positive catheter segment semiquantitative culture (at least 15 colony-forming units [CFUs]) for the same organism as the blood culture. 19 In patients without removal of catheters, CRBSI was defined as at least 1 positive blood culture obtained from a peripheral vein and one of the following for the same organism—(1) differential time period of catheter versus peripheral blood culture positivity of more than 2 hours or (2) simultaneous quantitative blood culture with >5:1 ratio CFU (catheter to peripheral). 20 No antimicrobial-coated catheters were used during the study period.
Exclusion criteria were BSIs with an identified source other than a catheter; isolation of 1 or more microorganisms, other than the Acinetobacter spp., from the blood during the same BSI episode (polymicrobial BSIs); patients younger than 20 years of age; and patients with incomplete medical records. The protocol was approved by the institutional review boards of each site with a waiver for informed consent. The approval numbers were CCH: 140514; MKH: 14MMHIS125; TSGH: 1-105-5-100; and TVGH: 2015-04-003C.
Species Identification and Antimicrobial Susceptibilities
The phenotypic identification of the Ab group isolates was performed using the Vitek 2 systems (bioMérieux, Marcy l’Etoile, France). A multiplex PCR method was used to identify A. baumannii to the species level. 21 Isolates identified as non-A. baumannii species of Acinetobacter were identified by 16S-23S ribosomal DNA intergenic spacer sequence analysis. 22 Antimicrobial susceptibilities were determined by the agar dilution method and interpreted according to the Clinical Laboratory Standards Institute. 23,24 Multidrug resistance was defined as resistance to 3 or more of the following classes of antimicrobial agents—antipseudomonal cephalosporins, antipseudomonal carbapenems, ampicillin/sulbactam, fluoroquinolones, and aminoglycosides. 1
Data Collection
Clinical information was recorded and included demographic characteristics, underlying diseases, Charlson comorbidity score, 25 the presence of a catheter, type and site of catheter insertion at the time of BSI onset, and duration of ICU and hospital stay. The date of acquisition of BSI was defined as the day of the blood draw that yielded Acinetobacter spp. positive culture. Catheter-related BSIs were considered ICU-acquired if they appeared 48 hours after ICU admission. Previous ICU admission was defined as ICU admission in the 4 weeks prior to CRBSI onset. Chronic pulmonary diseases included chronic obstructive pulmonary disease, asthma, bronchiectasis, pulmonary fibrosis, and chronic pulmonary tuberculosis. Recent surgery was defined as surgical procedures performed in the 4 weeks prior to CRBSI onset. Immunosuppressive therapy was defined as treatments with cytotoxic agents in the 6 weeks; corticosteroids treatments with prednisolone at a dosage of ≥10 mg/d, for more than 5 days, in the 4 weeks; or other immunosuppressive agents in the 2 weeks prior to CRBSI onset. Neutropenia was defined as an absolute neutrophil count <0.5×109 neutrophils/L. Chronic kidney disease was defined as an estimated glomerular filtration rate <60 mL/min/1.73 m2. Shock was defined as hypotension (systolic blood pressure [SBP] <90 mmHg, mean arterial pressure <70 mmHg, or an SBP decrease >40 mmHg), with evidence of end organ dysfunction. 26 The severity of illness was evaluated using the Acute Physiologic and Chronic Health Evaluation (APACHE) II score 27 in the 24 hours prior to BSI onset. Early removal of catheters was defined as removal of the catheters within 48 hours of CRBSI diagnoses. Appropriate antimicrobial therapy was defined as administration of at least 1 antimicrobial agent, to which the causative pathogen was susceptible, for more than 24 hours, with an approved route and dosage for end organ(s) function, within 48 hours of BSI onset. Antimicrobial therapy that did not meet this definition and monotherapy with an aminoglycoside were considered inappropriate.
A matched case-control study was used to compare the effect of catheter removal within 48 hours (case) or catheter retention for more than 48 hours (control) on mortality. The criteria of matched control included age, sex, and APACHE II scores. Sex was 1:1 matched in the 2 groups, and the differences of age and APACHE II score between the matched cases were less than 5 years and 5 points, respectively.
Statistical Analyses
To assess the differences between groups, a χ2 test with Yates’ correction or Fisher’s exact test was used to compare the discrete variables, whereas the Student’s t test or Mann-Whitney rank sum test was used to analyze the continuous variables. Univariate analyses were performed separately for each of the risk factor variables to ascertain the odds ratio (OR) and 95% confidence interval (CI). Logistic regression models were used to explore independent risk factors associated with 30-day mortality. All biologically plausible variables with a P value <.2 in the univariate analysis, exhibited by at least 10% of the patients, were considered for inclusion in the logistic regression model for multivariate analysis. Time to mortality was analyzed using Kaplan-Meier survival analysis and log-rank test. A P value <.05 was considered statistically significant. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) software version 18.0 (SPSS, Chicago, Illinois).
Results
During the study period, we evaluated 874 BSIs caused by Acinetobacter spp. (CCH: 138, MMH: 134, TSGH: 222, and TVGH: 380). Two hundred and twenty-one cases were excluded as the patients had polymicrobial or concomitant infection at the time of presentation. A total of 119 patients with documented CRBSI met the clinical and microbiological criteria to be eligible for the study.
The clinical characteristics of 30-day survivors and nonsurvivors of CRBSIs caused by Acinetobacter spp. are presented in Table 1. Forty-one (34.5%) of 119 patients died within 30 days of Acinetobacter CRBSI onset. The nonsurvivors had a significantly higher proportion of male, ICU-acquired CRBSIs, longer hospitalization before CRBSI onset, chronic liver and kidney diseases, solid malignancies, and ventilator use than the survivors. There were also more cases of shock (43.9% vs. 7.7%; P < .001) and higher APACHE II scores (median: 27 vs. 15; P < .001) among the nonsurvivors. Furthermore, the rate of multidrug resistance among the causative pathogens was higher in the nonsurvivors (73.2% vs. 32.1%; P < .001), whereas more survivors received an appropriate antimicrobial therapy (50.0% vs. 31.7%), although this was not statistically significant (P = .056). The antimicrobial susceptibilities of blood isolates and appropriate antimicrobial therapies from patients with CRBSIs caused by different Acinetobacter spp. are shown in Table 2. There were no statistical differences in mortality among patients receiving appropriate or inappropriate antimicrobial therapies in CRBSIs caused by different Acinetobacter spp. (data not shown).
Demographic and Clinical Characteristics of 30-Day Survivors and Nonsurvivors with Catheter-Related Bloodstream Infections Caused by Acinetobacter Species.
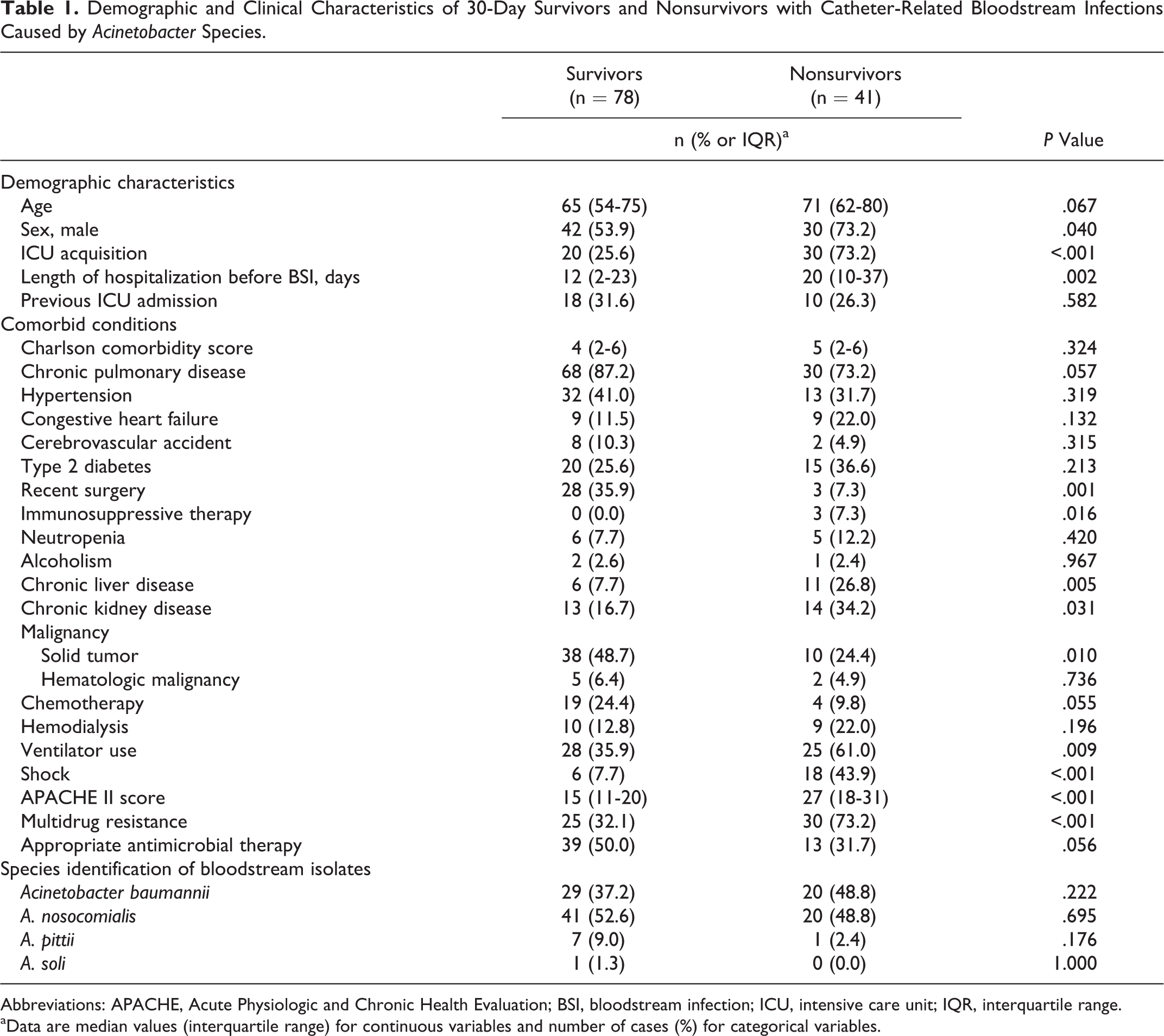
Abbreviations: APACHE, Acute Physiologic and Chronic Health Evaluation; BSI, bloodstream infection; ICU, intensive care unit; IQR, interquartile range.
aData are median values (interquartile range) for continuous variables and number of cases (%) for categorical variables.
Comparison of Antimicrobial Susceptibilities of the Blood Isolates and Appropriate Antimicrobial Therapies from Patients with Catheter-Related Bloodstream Infections Caused by Different Acinetobacter Species.
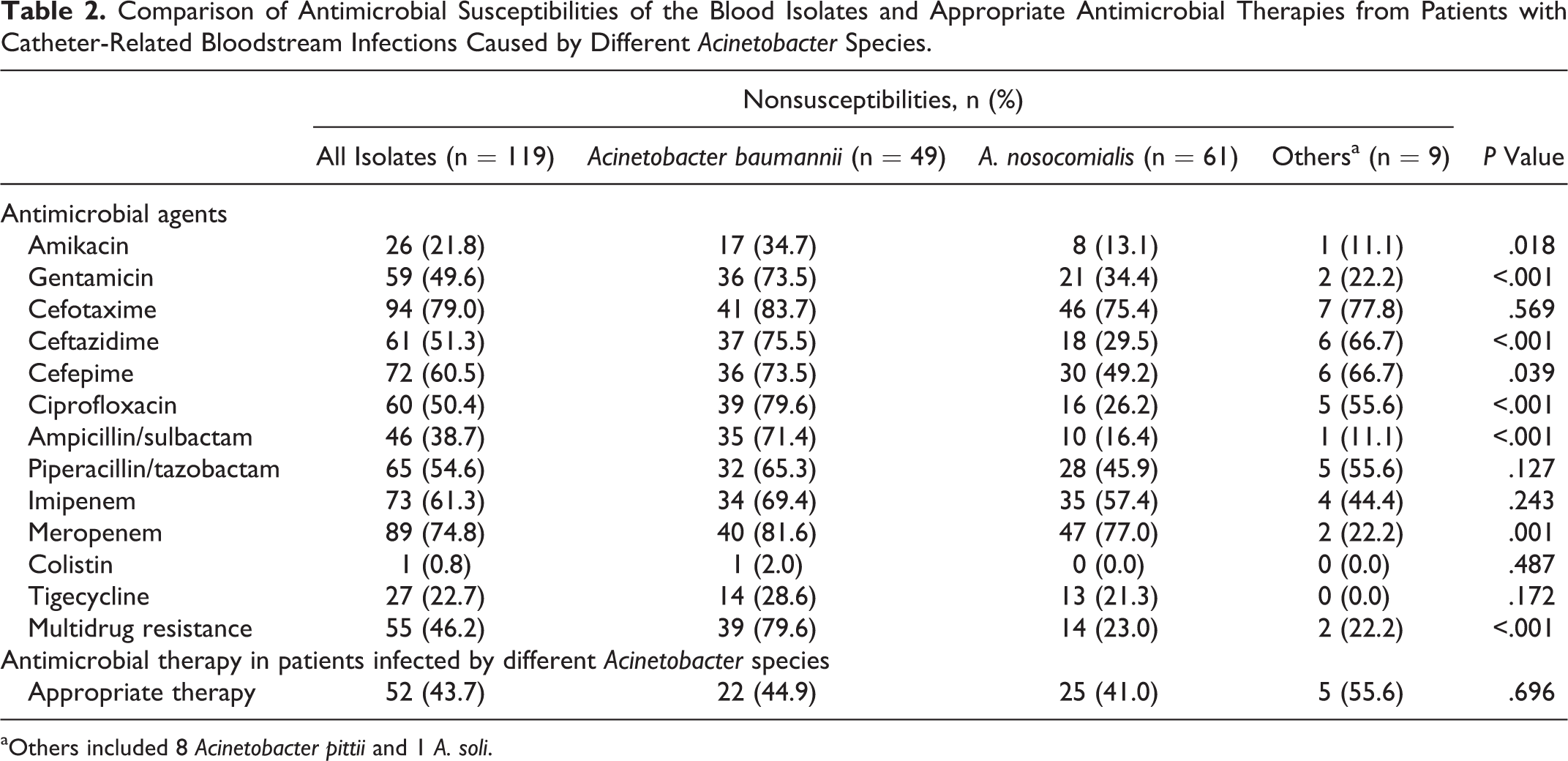
aOthers included 8 Acinetobacter pittii and 1 A. soli.
Table 3 shows the catheter characteristics among 30-day survivors and nonsurvivors. A higher proportion of nonsurvivors had central venous catheters (CVCs), as opposed to port catheters, which were more common in the survivors. Patients with CVCs had a significantly higher 30-day mortality than those with port catheters (45.6% vs. 13.8%; P = .002). All port catheters were subclavicularly inserted, whereas no specific insertion site of CVCs was associated with a higher 30-day mortality. Among patients with either CVCs or port catheters, the rates of catheter removal within 48 hours were similar between the 30-day survivors and nonsurvivors.
Comparison of Catheter Characteristics and Differences between 30-Day Survivors and Nonsurvivors in Catheter-Related Bloodstream Infections Caused by Acinetobacter Species.
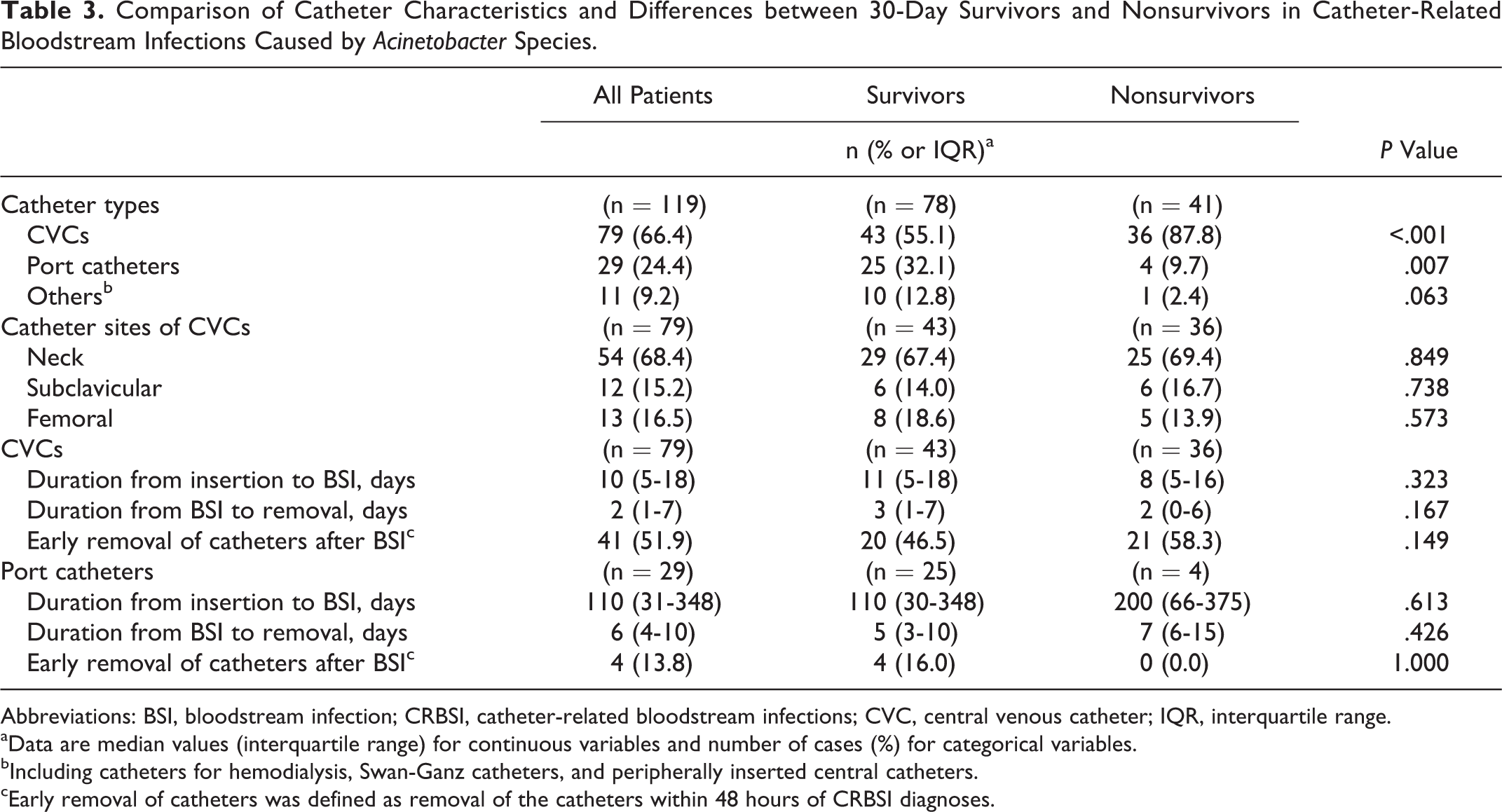
Abbreviations: BSI, bloodstream infection; CRBSI, catheter-related bloodstream infections; CVC, central venous catheter; IQR, interquartile range.
aData are median values (interquartile range) for continuous variables and number of cases (%) for categorical variables.
bIncluding catheters for hemodialysis, Swan-Ganz catheters, and peripherally inserted central catheters.
cEarly removal of catheters was defined as removal of the catheters within 48 hours of CRBSI diagnoses.
A. baumannii was an important factor affecting mortality; even though its P value was .223 in the univariate analysis, it was still incorporated in the multivariate analysis. Multivariate analysis identified shock (OR = 6.43; 95% CI = 1.28-32.33), high APACHE II score (OR = 1.12; 95% CI = 1.02-1.23), and longer hospitalization before BSIs (OR = 1.04; 95% CI = 1.00-1.08) as independent risk factors for 30-day mortality, whereas recent surgery (OR = 0.08; 95% CI = 0.01-0.58) was identified as a protective factor (Table 4). Presence of CVCs, early removal of catheters after BSIs, multidrug resistance, appropriate antimicrobial therapy, and BSIs caused by A. baumannii were not associated with a better or worse outcome.
Factors Associated with 30-Day Mortality in Patients with Catheter-Related Bloodstream Infections Caused by Acinetobacter Species.
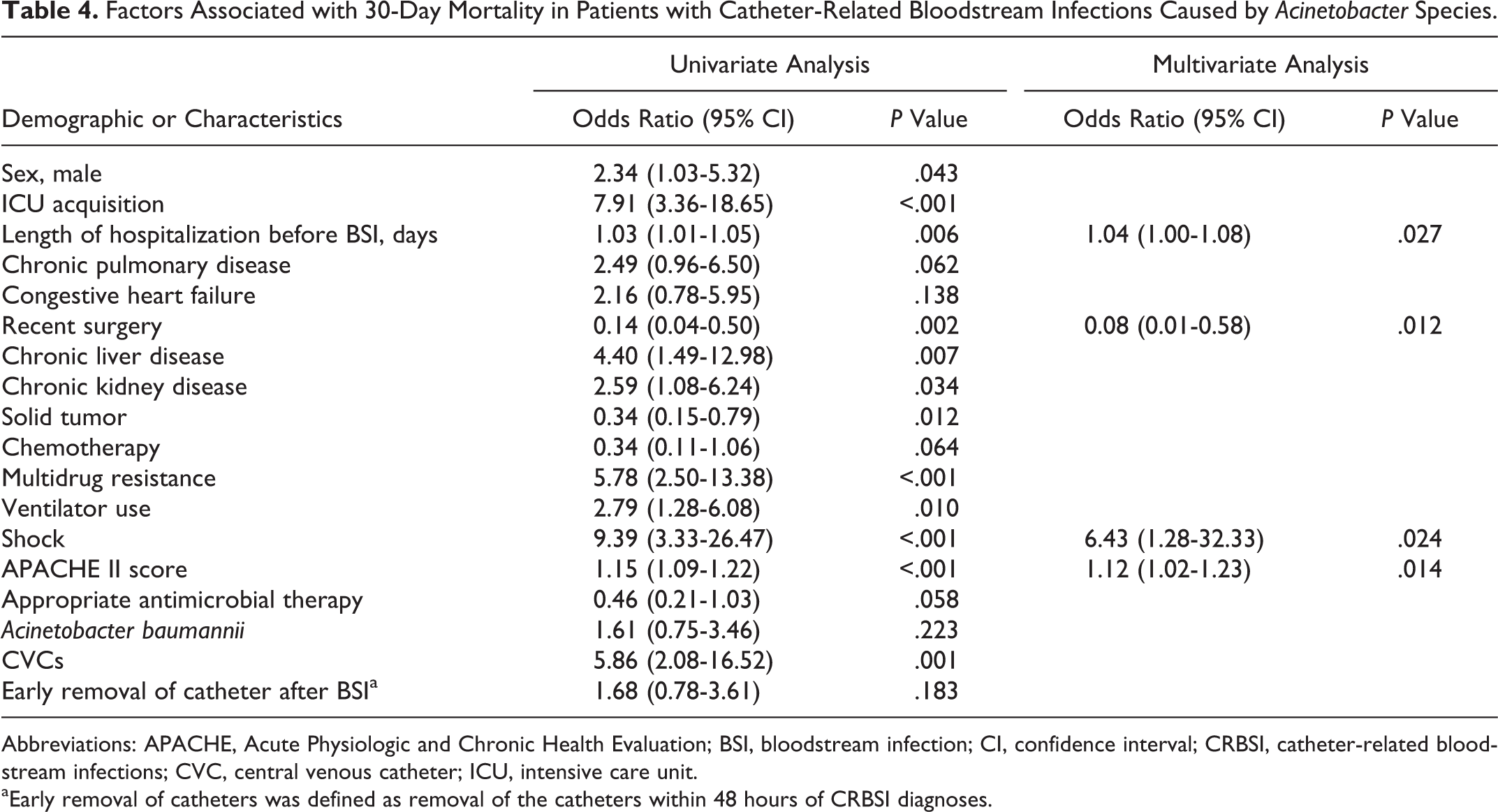
Abbreviations: APACHE, Acute Physiologic and Chronic Health Evaluation; BSI, bloodstream infection; CI, confidence interval; CRBSI, catheter-related bloodstream infections; CVC, central venous catheter; ICU, intensive care unit.
aEarly removal of catheters was defined as removal of the catheters within 48 hours of CRBSI diagnoses.
There was no statistically significant difference in 30-day mortality among patients with early catheter removal or retention. There were also no statistical differences in 30-day mortality among the 2 groups regarding early catheter removal or retention in different Acinetobacter spp., disease severities, and appropriateness of antimicrobial therapy. In patients with CVCs, the 30-day mortality rates in those with early removal and retention of catheters were 51.2% and 39.5%, respectively. In those with port catheters, the 30-day mortality rates with removal and retention of catheters were 0% and 16.0%, respectively. Furthermore, in patients with CVCs, the APACHE II score was significantly higher than port and other catheters (median: 21 vs. 14 vs. 17; P < .001). And the 30-day mortality rate was significantly lower in patients having CRBSIs with CVCs receiving appropriate antimicrobial therapies than those without (31.3% vs. 55.3%; P = .033; Supplemental Table 1), but it was not significant in patients with port and other catheters.
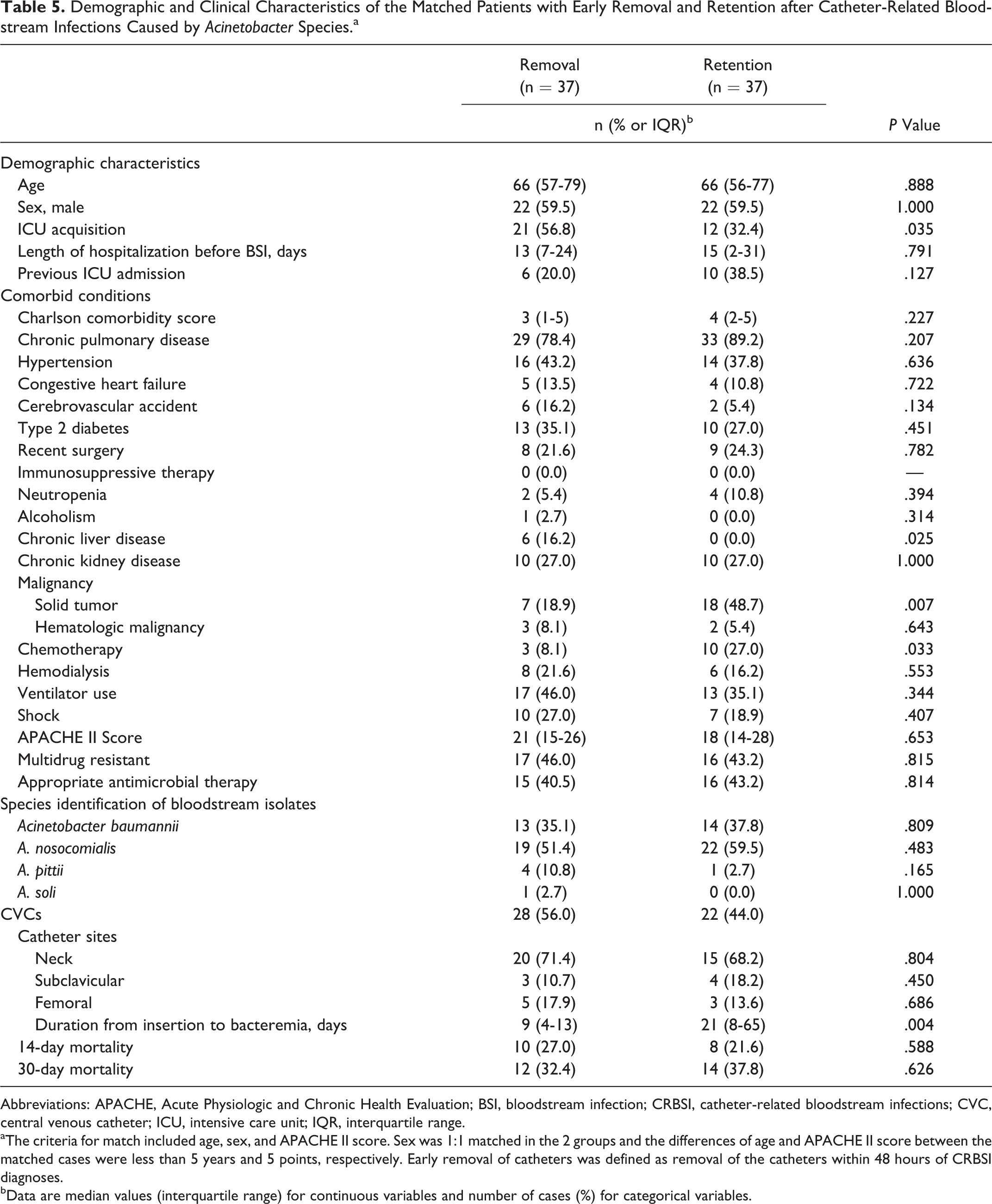
To further elucidate the impact of catheter removal or retention on risk of mortality, we performed a matched case-control analysis by matching patients with removal or retention of catheter for age, sex, and APACHE II score. No significant differences were observed in 14- and 30-day mortality between the patients with retention of catheters and removal of catheters within 48 hours (Table 5).
Demographic and Clinical Characteristics of the Matched Patients with Early Removal and Retention after Catheter-Related Bloodstream Infections Caused by Acinetobacter Species.a
Abbreviations: APACHE, Acute Physiologic and Chronic Health Evaluation; BSI, bloodstream infection; CRBSI, catheter-related bloodstream infections; CVC, central venous catheter; ICU, intensive care unit; IQR, interquartile range.
aThe criteria for match included age, sex, and APACHE II score. Sex was 1:1 matched in the 2 groups and the differences of age and APACHE II score between the matched cases were less than 5 years and 5 points, respectively. Early removal of catheters was defined as removal of the catheters within 48 hours of CRBSI diagnoses.
bData are median values (interquartile range) for continuous variables and number of cases (%) for categorical variables.
Discussion
This is the first multicenter study investigating the risk factors associated with mortality and the influence of early catheter removal or retention on the survival outcome of CRBSIs caused by Acinetobacter spp. Patients with higher disease severity (APACHE II score), shock, and longer hospitalization before BSIs had a significantly higher 30-day mortality rate. In contrast, multidrug resistance, the use of appropriate antimicrobial therapy, and BSIs caused by A. baumannii were not associated with better or worse 30-day mortality. Early removal of catheters after BSIs did not result in additional survival benefits.
Acinetobacter spp. were previously considered opportunistic pathogens and have emerged as a severe nosocomial threat recently. 1 Longer hospitalization before BSIs was an independent risk factor for mortality in the present study. Bloodstream infections caused by Acinetobacter spp. usually take a longer time to develop infections, and reports have shown that nonsurvival was generally accompanied by a longer hospitalization before BSIs. 5,6,28 In addition, patients with prolonged hospitalization usually present with more comorbidities and generally have worse outcomes. Recent surgery was identified as a protective factor; compared to inoperable patients who are generally old and present with comorbidities, those who undergo surgeries are usually not as ill to be able to receive anesthesia and probably have better clinical outcomes. Recent surgery was also a protective factor for mortality in our previous study elucidating BSIs caused by carbapenem-resistant Acinetobacter spp. at a single-center study, where the patients were even older and more severely ill. 29 In addition to the patients’ underlying problems, whether patients in surgical wards or ICUs could be infected with less virulent or less drug-resistant strains of Acinetobacter spp. than other patients has not been determined. Appropriate antimicrobial therapy was not associated with a better outcome in the present study. We have previously reported that the use of appropriate antimicrobial therapy significantly reduced 14-day mortality in patients with severe BSIs (APACHE II score >25) caused by A. baumannii 6 but not A. nosocomialis. 30 Because, in this study, more than half of the CRBSIs were caused by A. nosocomialis, the effect of appropriate antimicrobial therapy might have been obscured. Furthermore, the APACHE II scores of patients infected with A. baumannii were relatively low (median: 17, interquartile range: 11-28), therefore appropriate antimicrobial therapy may not be associated with a significantly decreased mortality. But in CRBSIs caused by CVCs, the APACHE II score was high, and appropriate antimicrobial therapy led to a better survival outcome.
The guidelines of Infectious Diseases Society of America and the review by Raad et al 13 , 15 recommend the removal of CVCs in addition to antimicrobial therapy for patients with CRBSIs caused by GNBs. A removal is also recommended for the cases of long-term venous or port catheters, whereas catheter salvage is only to be considered in cases with uncomplicated infections that respond well to antimicrobial therapy. In patients with Acinetobacter spp.-induced CRBSIs, catheter removal has previously been associated with better clinical responses (eg, defervesce), but not with better or worse survival, in the study by Seifert et al. 4 The factors independently associated with mortality were shock, rapid disease progress, and ventilator use. In this study, early removal of catheters was not associated with a better survival outcome.
The mortality rates of BSIs caused by Acinetobacter spp. range from 28.1% to 46.2%. 5,7,28 In the present study, patient with CVCs had a mortality rate (46.6%) close to previously reported values; however, for patients with port catheters, we recorded a relatively low mortality rate (13.8%). An increasing number of studies have also shown the effectiveness of antibiotic-lock treatments (ALTs) in catheter salvage of catheter-related infections. 15,18,31 –33 Therefore, in Acinetobacter spp. CRBSIs related to port catheters, ALTs may be considered in addition to systemic antibiotic therapy for catheter preservation when the infections are not too serious, since long-term vascular catheters were more difficult to establish, and the mortality rates in such patients were relatively low. Further study is needed to determine which patients will not have grave outcomes from the retention of port catheters in CRBSIs caused by Acinetobacter spp.
There were limitations to this study. The issue of catheter removal is subject to several limitations regularly found in retrospective studies. The causal relationship between disease severity and catheter removal that impacted on mortality cannot be well elucidated, and several confounding factors such as the impact of disease severity, and personal experience of the clinicians on the decision-making of removal or retention of the catheter, cannot be well controlled for in a retrospective study design. Further well-controlled prospective studies will be required to elucidate the influence of catheter removal in CRBSIs caused by Acinetobacter spp.
Conclusion
Higher disease severity (APACHE II score), shock, and longer hospitalization before bacteremia were independently associated with a higher 30-day mortality in CRBSIs caused by Acinetobacter spp. In previous published guidelines, infected catheters were suggested to be removed in CRBSIs caused by GNBs. Even though early removal of catheters did not associate with a better survival outcome in current results, it should be judiciously evaluated according to the clinical conditions and risks individually. For better elucidation of these issues, further well-controlled prospective study may be warranted.
Supplemental Material
Supplemental Material, Supplemental_Table_1 - Risk of Mortality of Catheter-Related Bloodstream Infections Caused by Acinetobacter Species
Supplemental Material, Supplemental_Table_1 for Risk of Mortality of Catheter-Related Bloodstream Infections Caused by Acinetobacter Species by Yi Lee, Yi-Tzu Lee, Yung-Chih Wang, Chung-Ting Chen, Jun-Ren Sun, Chang-Pan Liu, Yuan-Meng Liu, Shu-Chen Kuo, Chun-Hsiang Chiu, Ya-Sung Yang, Jung-Chung Lin, and Te-Li Chen in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Tri-Service General Hospital (TSGH-C100-103, TSGH-C102-113, TSGH-C103-125, TSGH-C104-119, TSGH-105-113, TSGH-C106-096, MAB101-03, DV104-09, and MAB102-13), Taipei Veterans General Hospital (V103B-021, V104B-017, and V105B-005), and the Ministry of Science and Technology (MOST 103-2314-B-016-039, MOST 104-2314-B-016-051, MOST 104-2314-B-075-043-MY3, and MOST 105-2628-B-016-003-MY2).
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.