
Abstract
Lactic acid and base deficit (BD) values are frequently monitored in the intensive care unit and operating room setting to evaluate oxygenation, ventilation, cardiac output, and peripheral perfusion. Although generally obtained from an arterial cannula, such access may not always be available. The current study prospectively investigates the correlation of arterial and peripheral venous values of BD and lactic acid. The study cohort included 48 patients. Arterial BD values ranged from −8 to 4 mEq/L and peripheral venous BD values ranged from −8 to 4 mEq/L. Arterial lactic acid values ranged from 0.36 to 2.45 μmol/L and peripheral venous lactic acid values ranged from 0.38 to 4 μmol/L. The arterial BD (−0.4 ± 2.2 mEq/L) was not significantly different from the peripheral venous BD (−0.6 ± 2.2 mEq/L). The arterial lactic acid (1.0 ± 0.5 μmol/L) was not significantly different from the peripheral venous lactic acid (1.1 ± 0.6 μmol/L). Pearson correlation coefficients demonstrated a very high correlation between arterial and peripheral venous BD (r = .88, P < .001) and between arterial and peripheral venous lactic acid (r = .67, P < .001). Bland-Altman plots of both pairs of measures showed that the majority of observations fell within the 95% limits of agreement. Least-squares regression indicated that a 1-unit increase in arterial BD corresponded to a 0.9-unit increase in peripheral venous BD (95% confidence interval [CI]: 0.7-1.0; P < .001) and a 1-unit increase in arterial lactic acid corresponded to a 0.9-unit increase in peripheral venous lactic acid (95% CI: 0.6-1.2; P < .001). These data demonstrate that there is a clinically useful correlation between arterial and peripheral venous lactic acid and BD values.
Introduction
Arterial and venous blood samples are frequently monitored in the intensive care unit (ICU) and operating room setting to evaluate oxygenation, ventilation, cardiac output, and systemic perfusion. Depending on the site of monitoring, variations in the pH, base deficit (BD), and lactic acid values may be noted. In the adult patient in the ICU or emergency department setting, a clinically acceptable correlation has been noted between pH, BD, and lactic acid when comparing venous and arterial samples. 1 –4 However, there are no studies evaluating intraoperative correlations and limited data in the pediatric population regarding the correlation of peripheral venous and arterial values. The current study evaluated the correlation of arterial and peripheral venous values of lactic acid and BD during intraoperative care in a cohort of pediatric patients.
Methods
This study was approved by the institutional review board of Nationwide Children’s Hospital (IRB #15-00793) and registered at clinicaltrials.gov (NCT #02888431). Given its limited impact on clinical care and low risk, the need for written consent was waived. Verbal consent was obtained from a parent, and when age was appropriate, verbal assent was obtained from the patient. This was a prospective, cross-sectional, intraoperative study comparing pH, BD, and lactic acid values from simultaneously obtained arterial and peripheral venous samples. There was no change in clinical or anesthetic care as a result of this study. Patients undergoing anesthetic care requiring the insertion of an arterial cannula for a surgical procedure (posterior spinal fusion) were considered eligible for inclusion. Patients were excluded from recruitment if there was intracardiac shunting or residual congenital heart disease. As clinically indicated, when an arterial sample was obtained, a simultaneous sample was obtained from a peripheral venous catheter for routine blood gas analysis and lactic acid determination. A tourniquet was not used to obtain the sample from the peripheral venous cannula. The sample was drawn from a large-bore intravenous cannula to ensure free flow of blood. Only 1 sample set (arterial and venous values) was obtained from each patient.
Statistical Analysis
Correlations between arterial and venous values of BD and lactic acid were assessed using Pearson correlation coefficient and Bland-Altman plots. Least-squares regression was used to determine the change in each central value corresponding to a unit change in the arterial value. Differences between mean central and arterial values were assessed using paired t tests. P < .05 was considered statistically significant. Analyses were performed using Stata/IC 13.1 (StataCorp LP, College Station, Texas).
Results
The initial study cohort included 50 patients; however, complete data were available from 48 patients (30 females and 18 males), ranging in age from 1 month to 22 years (12.6 ± 4.8 years). The American Society of Anesthesiologists physical status for all of the patients was either 2 or 3. Arterial BD values ranged from −8 to 4 mEq/L and venous BD values ranged from −8 to 4 mEq/L. Arterial lactic acid values ranged from 0.36 to 2.45 μmol/L and venous lactic acid values ranged from 0.38 to 4 μmol/L (normal values for reference laboratory: 0.5-2.2 μmol/L). The arterial BD (−0.4 ± 2.2 mEq/L) did not differ significantly from the peripheral venous BD (−0.6 ± 2.2 mEq/L). The arterial lactic acid (1.0 ± 0.5 μmol/L) also did not significantly differ from the peripheral venous lactic acid (1.1 ± 0.6 μmol/L). Pearson correlation coefficients demonstrated a high correlation between arterial and peripheral venous BD (r = .88, P < .001) and between arterial and peripheral venous lactic acid (r = .67, P < .001). Bland-Altman plots of both pairs of measures showed that the majority of observations fell within the 95% limits of agreement (Figures 1 and 2). Least-squares regression indicated that a 1-unit increase in arterial BD corresponded to a 0.9-unit increase in peripheral venous BD (95% confidence interval [CI]: 0.7-1.0; P < .001) and a 1-unit increase in arterial lactic acid corresponded to a 0.9-unit increase in peripheral venous lactic acid (95% CI: 0.6-1.2; P < .001).
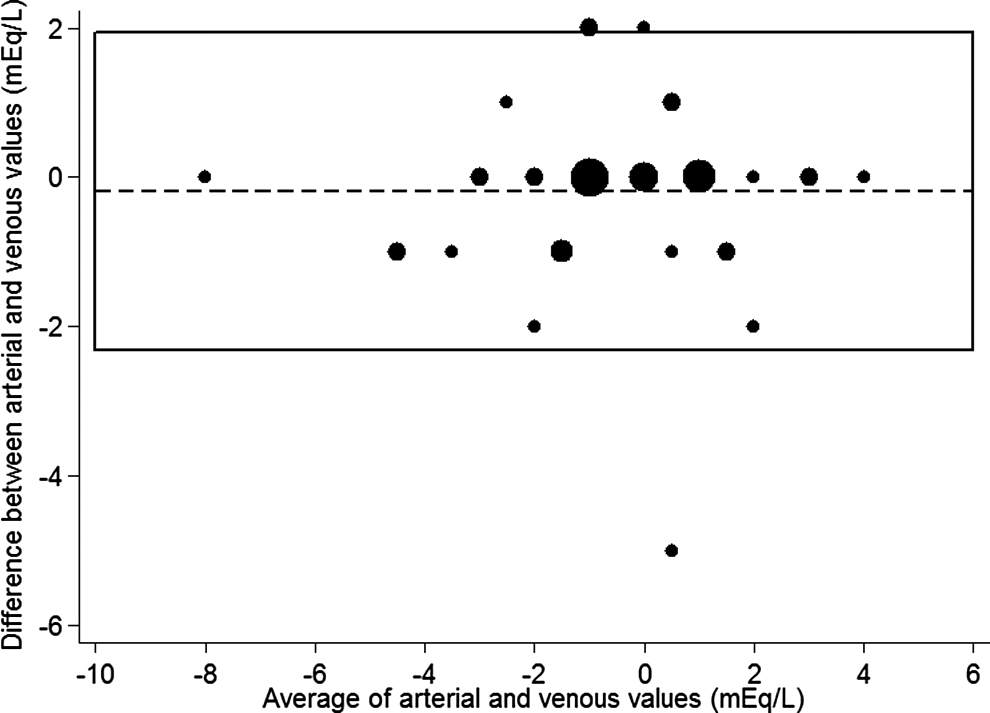
Bland-Altman plot of agreement between arterial and venous measures of base deficit. The box shows the 95% limits of agreement. The marker (icon) sizes are weighted by the number of observations at each value.
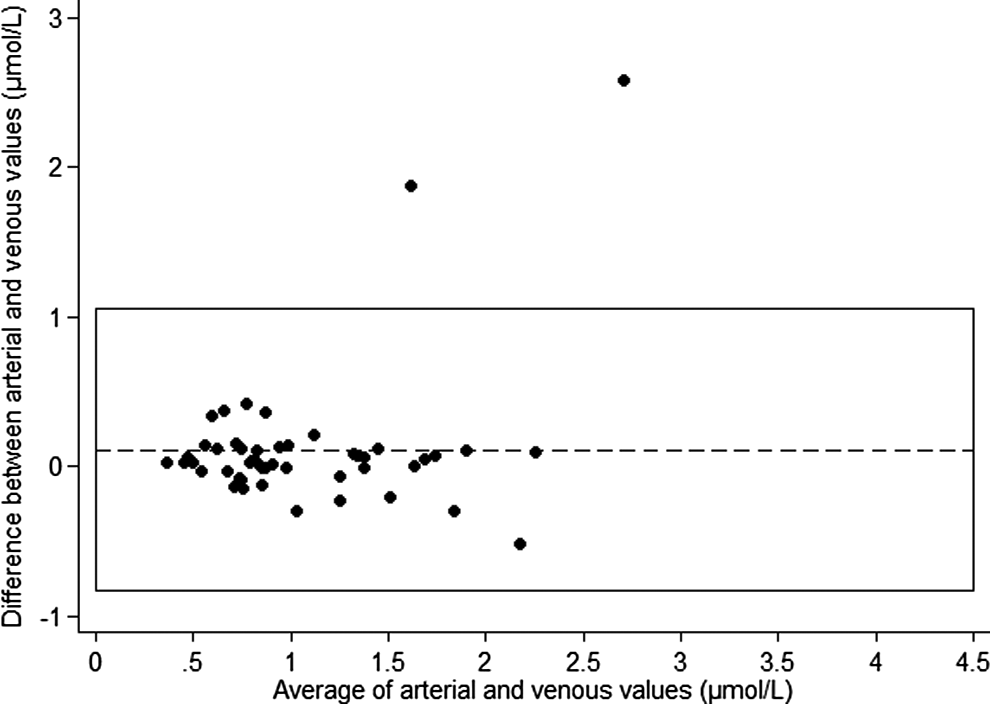
Bland-Altman plot of agreement between arterial and venous measures of lactic acid measured in μmol/L. The box shows the 95% limits of agreement. The marker (icon) sizes are weighted by the number of observations at each value.
Discussion
Lactic acid is produced as an end product of anaerobic metabolism when pyruvate cannot enter the Krebs cycle. Numerous etiologies may be responsible for the development of lactic acidosis in critically ill patients including circulatory failure and hypoxia. Several studies have demonstrated the predictive value of lactic acid and its trends in various clinical scenarios including surgery for congenital heart disease. 5 –9 There is also a growing body of literature showing the benefit of acute medical management with early goal-directed therapy based on lactic acid clearance. 5
Although there may be numerous causes for an increasing BD in the ICU setting, hypoperfusion is the primary etiologic event. There are various clinical scenarios where using a venous value would be more practical and expedient such as in patients who lack arterial access. In such circumstances, it has been demonstrated that there is a strong correlation between central venous and arterial values. 1 –4 However, in the early phases of resuscitation and other specific clinical scenarios, it is feasible that neither arterial nor central venous access may be present.
Previous studies in adults have demonstrated a clinically acceptable correlation between peripheral venous and arterial values.
1,2
In the emergency department setting during the early phases of acute care, peripheral venous lactic acid has been shown to correlate closely with arterial values such that clinically useful equations have been derived equating the 2 values.
1
In the ICU setting, central venous values of pH, bicarbonate, base excess, and lactic acid have also been shown to correlate with arterial values.
2
In a large meta-analysis including 1768 patients from 18 heterogeneous studies, there was no clinically significant difference between peripheral and arterial blood gas measurements of pH, with the arterial pH being 0.03 higher than the venous pH (95% CI: 0.029-0.038).
2
However, the venous and arterial Pa
We are aware of no previous studies comparing arterial and peripheral venous values in children. The current study demonstrates a clinically useful correlation between lactic acid and BD values obtained from an arterial cannula and a peripheral venous site (peripheral intravenous cannula). Therefore, real-time measurements of BD or lactate in either arterial or venous samples intraoperatively and postoperatively may be utilized to guide therapy. This correlation may be affected by use of a tourniquet or inadequate flow from peripheral venous sites. The range of values in the current study was within those that are usually encountered in routine clinical practice. We did not have values in the extremes of those encountered in critically ill patients. With disturbed perfusion, decreased cardiac output, shock, or other conditions, the results may vary. Future studies are needed to further define the correlation of these values in critically ill patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.