
Abstract
Background:
Health care is a demanding field, with a high level of responsibility and exposure to emotional and physical danger. High levels of stress may result in depression, anxiety, burnout syndrome, and in extreme cases, post-traumatic stress disorder. The aim of this study was to determine which personal, professional, and organizational variables are associated with greater perceived stress among critical care nurses for purposes of developing integrative solutions to decrease stress in the future.
Methods:
We conducted a correlation research survey using a cross-sectional design and an in-person survey method. The questionnaire consisted of 2 parts: (1) socioeconomic, professional, and institutional variables and (2) work stressors. Surveys were conducted between January 1, 2011, and December 1, 2015. Multistage cluster random sampling was utilized for data collection. Inclusion criteria were (1) age ≥18 years, (2) registered nurse, (3) works in the intensive care unit (ICU), and (4) willing and able to complete the survey.
Results:
We surveyed 21 767 ICU nurses in Iran and found that male sex, lower levels of peer collaboration, working with a supervisor in the unit, nurse–patient ratios, and working in a surgical ICU were positively associated with greater stress levels. Increasing age and married status were negatively associated with stress. Intensive care unit type (semi-closed vs open), ICU bed number, shift time, working on holidays, education level, and demographic factors including body mass index, and number of children were not significantly associated with stress levels.
Conclusion:
As the largest study of its kind, these findings support those found in various European, North, and South American studies. Efforts to decrease workplace stress of ICU nurses by focusing on facilitating peer collaboration, improving resource availability, and staffing ratios are likely to show the greatest impact on stress levels.
Background
The nursing profession is among the largest workforce in most industrialized countries. 1 Globally, we are experiencing a worsening nursing shortage. Based on 2014 census data, Iran (population 75 million) requires a nursing labor force of approximately 240 000; however, currently it has only 100 000 nurses. 2 As more nurses exit the profession, the individual workload of remaining nurse’s increases, patient safety is jeopardized, job satisfaction decreases, and employer costs increase to replace those nurses. 2
Not all drivers of the global shortage can be mitigated. As in most industrialized nations, the elderly population is among Iran’s fastest growing populations. 2,3 Communicable and chronic diseases are an increasing burden. 3 Other factors include underinvestment in human resources (HRs), inadequate HR planning and management, migration, and high attrition. Attrition occurs due to poor work environments, low satisfaction, inadequate salary, and high stress. 1,2 Stress has a negative impact on nurses and patient outcomes; however, those practicing in critical care settings experience high levels of burnout. 4,5
The aim of this study was to determine which personal sociodemographic, professional, and organizational variables are associated with greater perceived stress among critical care nurses in Iran for the purposes of developing integrative solutions to decrease stress in the future.
Methods
Study Design
We conducted a correlation research survey using a cross-sectional design and an in-person survey method. The study was approved by the investigative review board at Baqiyatallah University of Medical Sciences (Tehran, Iran). Since the research presented no more than minimal risk of harm to participants and involved no procedures for which written consent is normally required outside the research context, the principle of implied consent was employed. Namely, that by completion of the survey instrument, the participant demonstrated their willful consent to participate. In accordance with institutional review board (IRB) requirements, the investigator provided participants with a written informed consent statement regarding the research. Although Iranian medical ethics laws (http://mehr.tums.ac.ir/Codes.aspx) do not specifically address this topic, it is in accordance with other international ethics codes and laws including the US Federal Code of Regulations (45 CFR 46.117c). All parts of the study were reviewed according to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 6 Surveys were conducted between January 1, 2011, and December 1, 2015. Multistage cluster random sampling was utilized for data collection. In the first step, 31 cities in Iran were selected. From each city, 10 hospitals were selected through cluster random sampling with replacement to decrease selection bias, once in the first and second steps, respectively. In the second step, 5 hospitals with more than 100 working nurses in critical care units (CCUs) were selected through cluster random sampling. In 5 cities, all hospitals had fewer than 100 critical care nurses, in which case all 10 hospitals were selected. Participant inclusion criteria were (1) age ≥18 years, (2) registered nurse, (3) works in the intensive care unit (ICU), and (4) willing and able to complete the survey.
Following the baseline stress measurement, a stress intervention was performed during which a 90-minute educational presentation on stress management was administered, followed by posting of educational stress management flyers in the clinical area (main ingress/egress ICU doors, nursing station, clinical work tables, library room door, call room door, rest room door). The poster remained up for 1 month. Repeat stress measurements were then performed at 15 days, 3 months, and 6 months postintervention.
Sample Size
The sample size was calculated based upon the results of the pilot study. 7 In the pilot study, an odds ratio (OR) of 0.90 was observed for the association between years of experience and stress levels. 7 By considering this OR, with proportion of stress of 0.50, 95% confidence level, and 90% power, sample size was calculated as 21 767 nurses. Sample size calculation was performed using G-Power 3.1.2 software (available at http://www.gpower.hhu.de/). 8 Considering a 20% dropout rate, the final sample size reached a total of 17 414 nurses.
Data Collection
Investigators hand-delivered sealed envelopes containing a project summary letter and the questionnaire to certified critical care nurses in the clinical environment. If the nurse consented to participate, the charge nurse arranged for coverage of clinical duties while the survey was completed (usually 10-15 minutes). Upon completion, the form was returned to the researcher in a sealed envelope provided in the initial packet. Each de-identified questionnaire was then evaluated by a panel of 3 investigators to determine suitability for inclusion based upon data completeness and nurse certification status. The survey was administered at 3 time points: (1) baseline preintervention, (2) 15 days postintervention (3) 3 months postintervention, and (4) 6 months postintervention. All questionnaires were de-identified, labeled with a unique patient identifier, and confidentiality maintained. Participants were provided a unique identifier by a person not involved in survey administration or statistical analysis. The key containing patient names and identifiers was kept in a secure location separate from surveys or data files.
Research Instrument
The questionnaire consisted of 2 parts: (1) socioeconomic, professional, and institutional variables and (2) work stressors. The utilized questionnaire was previously derived and validated using a 3 classic round Delphi technique. 7 The surveyed variables are socioeconomic (age, gender, marital status, number of children, body mass index [BMI]), professional (education level and years of critical care nursing experience), and institutional (shift schedule, frequency of working holidays, city, hospital, ICU bed number, nurse–patient ratio, degree of nursing collaboration type of CCU, ICU system, and having a supportive supervisor). Collaboration was measured using a 5-domain Likert-type scale (very low, low, moderate, high, and very high). The presence of a supportive supervisor was measured using a yes/no scale. Part 2 of the questionnaire consisted of a 22-item inventory of work stressors (Table 1) as previously reported. 7 The questionnaire items fell into 3 categories: interactive and communicative (questions 1, 2, 4, 11, 20, and 21), managerial and administrative (questions 3, 9, 10, 12, 14, 15, 16, 19, and 22), and exclusive and situational (questions 5, 6, 7, 8, 13, 17, and 18). The respondents were asked to rate the work stressors on a 5-point Likert-type scale ranging from “causes me no stress” to “causes me extreme stress.” The minimum and maximum scores of the instrument were 22 and 110, respectively. Based upon the results of the pilot study, the threshold for significant stress was set at 67, with values higher than this being indicative of significant stress. 7 This cutoff was derived using both quantitative and qualitative assessments. The quantitative portion was achieved by receiver operating characteristic curve analysis. The qualitative portion was accomplished by the expert panel consisting of psychiatric nurses (n = 5), psychologist (n = 1), psychiatrist (n = 1), ICU nurses (n = 5), CCU nurses (n = 5), dialysis unit nurses (n = 5), intensivists (n = 3), cardiologists (n = 3), nephrologists (n = 3), and ICU administrators (n = 5). After the 2 sessions, the κ agreement coefficient test was .89.
Stressful Situations Instrument With 22 Items.
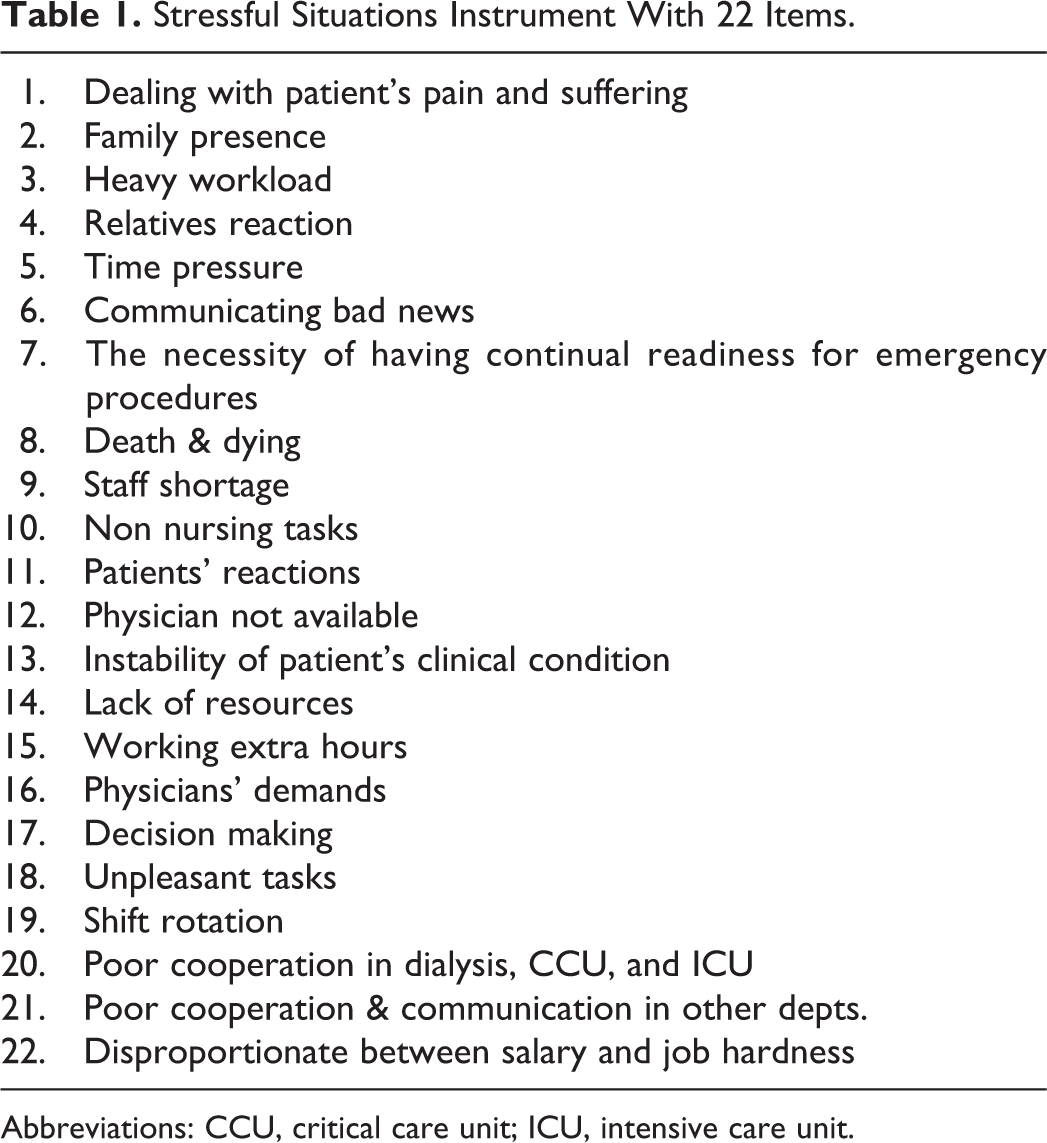
Abbreviations: CCU, critical care unit; ICU, intensive care unit.
Intervention
Following the baseline stress measurement, a stress intervention was performed during which a 90-minute educational presentation on stress management was administered, followed by 1 month of posting educational stress management flyers in the clinical area (main ingress/egress ICU doors, nursing station, clinical work tables, library room door, call room door, rest room door). Repeat stress measurements were then performed at 15 days, 3 months, and 6 months postintervention. Presentation and flyer content were developed using the 3 classic round Delphi technique as previously described, with the previously described questionnaire items serving as the primary content. The presentation was 25 slides including an introduction (slide 1), a discussion of the questionnaire items (slides 2-23), an invitation for open discussion of other stressors (slide 24), and conclusion (slide 25). The poster was 100 × 100 cm and contained the same content as the power point presentation.
Statistical Analysis
Hierarchical logistic regression modeling was used to identify those factors exerting a statistically significant effect on the nurse’s perceived stress levels. All statistical analyses were performed using MLwiN software version 2.31. A 3-level model including nurse, hospital, and city data was constructed to reduce the total variation within the model. Forward selection was used to select the significant variables in the final model.
Results
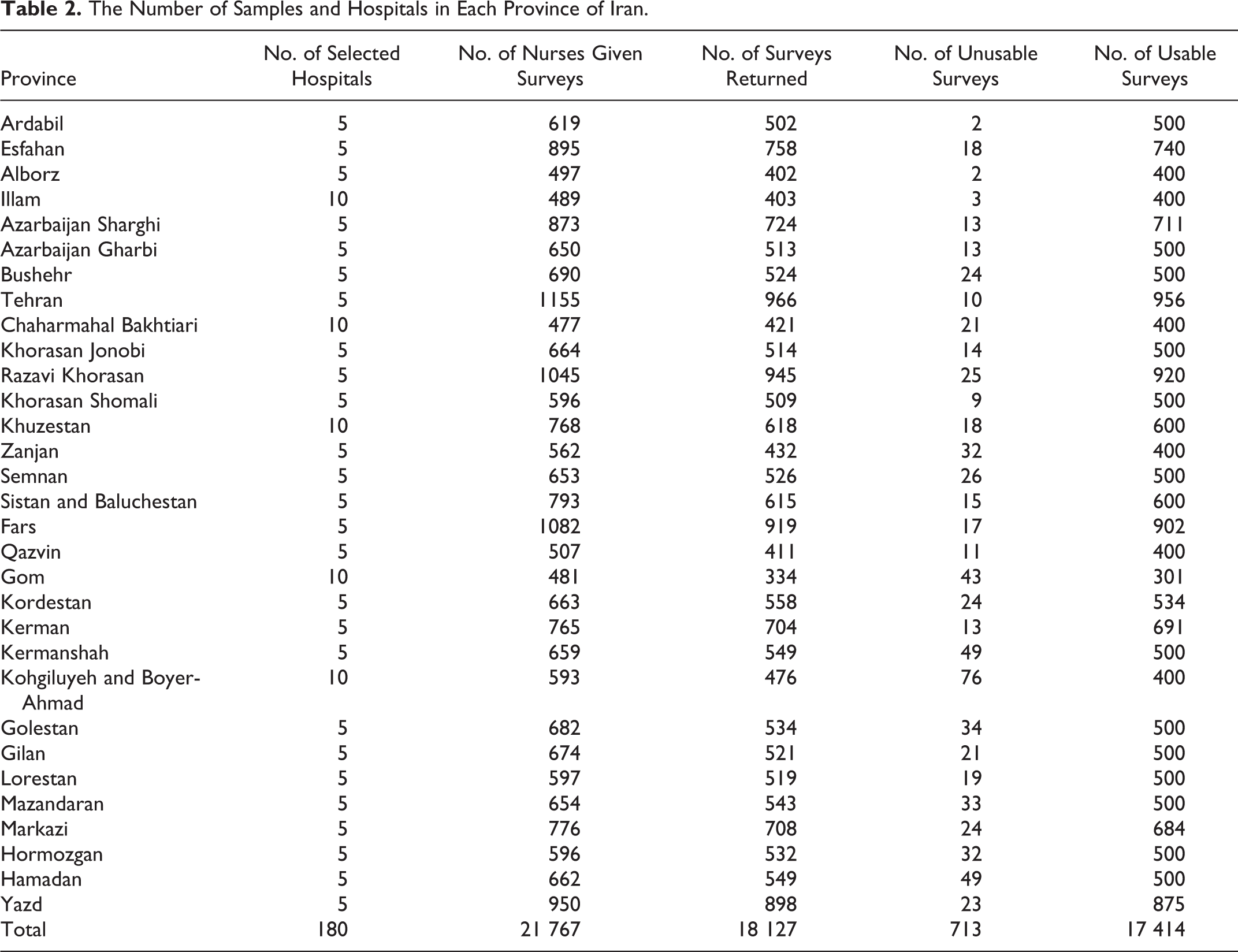
Altogether 790 CCUs at 180 educational and private hospitals were involved, including ICUs (n = 370), coronary care units (n = 240), and dialysis units (n = 180; Table 2). A total of 21 767 participants were administered the survey, and 18 127 returned the survey, with 17 414 returning usable surveys. The response rate of useful questionnaires was 80%. Sociodemographic and clinical features are summarized in Table 3. The mean age was 29 years with a female predominance (69%) and a baccalaureate degree (74%) level of education. Most were married (89%) with children (79%). The average BMI was 28.5. The average nurse-to-patient ratio was 2.78, and the mean years of clinical experience was 20. The mean ICU bed number was 10.69. Sixty percent reported low or moderate levels of collaboration, and most were working in rotation shift (39%) or evening shift (21%). The total stress score, mean (standard deviation [SD]) measured was 69 (3). Using the threshold value of 67 determined in the pilot study, 7 the incidence of stress in Iranian nurses was 71%.
The Number of Samples and Hospitals in Each Province of Iran.
Demographic Factors of Iranian Working Nurses in Critical Care Units.

Abbreviations: BMI, body mass index; ICU, intensive care unit.
aMean.
bGenerally speaking, the Iranian health-care system does not have closed ICUs.
The association of stress and sociodemographic and clinical features was analyzed using a hierarchical logistic regression model (Table 4), with a univariate model as the crude OR and a backward selection model as the adjusted OR. In this hierarchical logistic regression model, the estimated variance for level of cities was 0.13 with standard error (SE) = 0.014 (P < .001) and the estimated variance for hospital type or level was 0.007 with SE = 0.003 (P = .019). Male gender was positively associated with increased stress in both crude (OR: 1.22; P < .001) and adjusted models (OR: 1.19; P < .001). Increasing age had a weak negative association with stress in the multivariate model (OR: 0.95; P < .001), as did years of clinical ICU experience (OR = 1.04, P < .001). Marriage also displayed a negative association with stress on both crude (OR = 0.87, P = .029) and adjusted analysis (OR = 0.72, P = .017). Lower levels of collaboration (multivariate OR: 1.36, P < .001), working with a supervisor on the unit (crude OR: 1.18; P < .001), and nurse–patient ratios (multivariate OR: 1.17; P = .05) were all positively associated with greater stress levels. Working in a surgical ICU was associated with greater stress in the univariate but not multivariate model. The ICU type (semi-closed vs open) was not associated with stress in both models. No closed ICUs were surveyed. Intensive care unit bed number, shift time, working on holidays, education level, and demographic factors including BMI, and number of children were not significantly associated with stress in univariate or multivariate models.
Factors Associated With Stress in Critical Care Nurses in Iran.
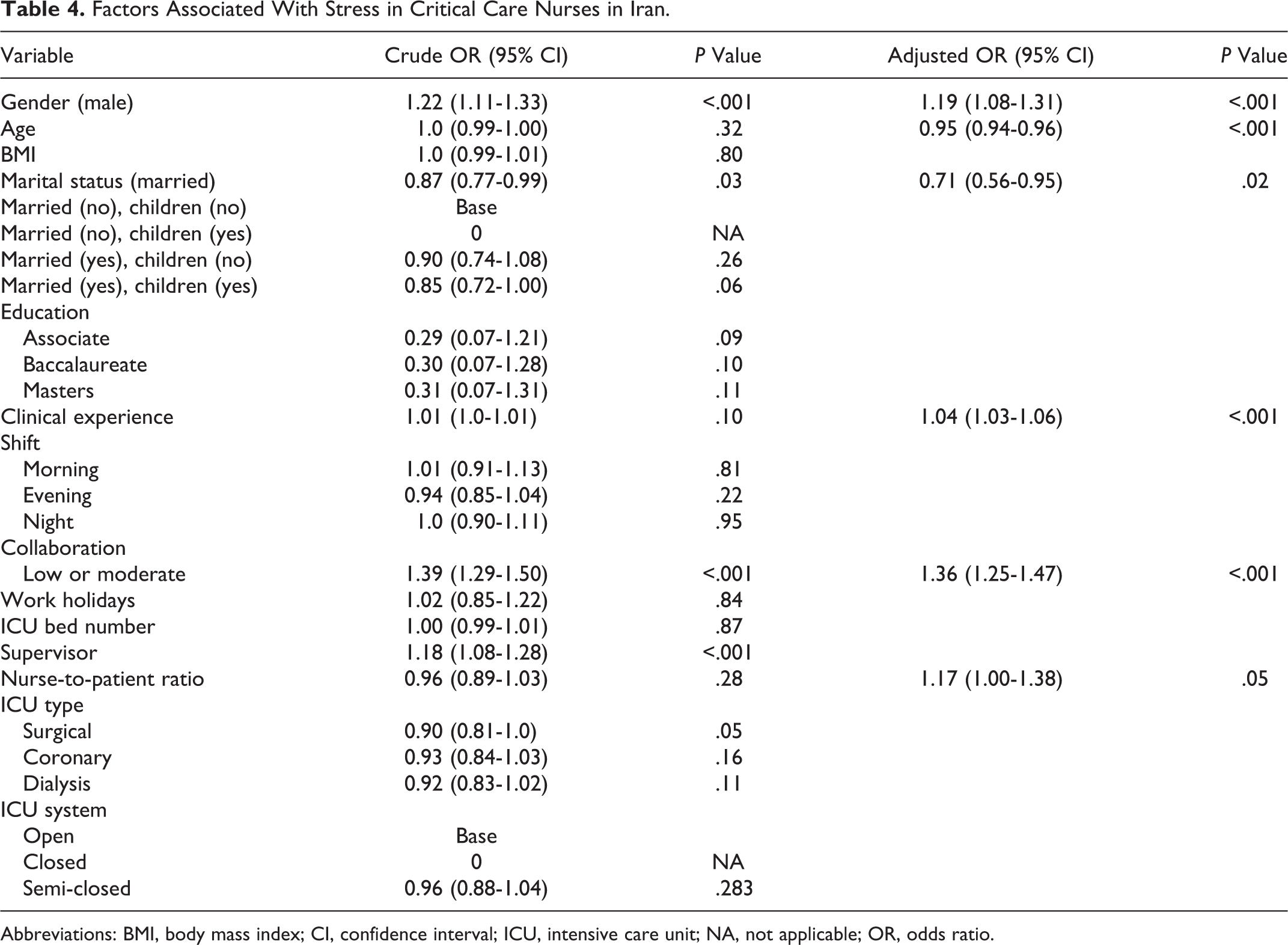
Abbreviations: BMI, body mass index; CI, confidence interval; ICU, intensive care unit; NA, not applicable; OR, odds ratio.
Baseline scores on the stress questionnaire were 94.7 (6.7). Following the stress education intervention, mean scores were 71.7 (4.8) at 15 days postintervention, 64.9 (4.9) at 3 months postintervention, and 57.1 ± 5.4 at 6 months postintervention. Stress scores decreased during the study overall, as well as within both the lower (score ≤67) and higher (score >67) stress subgroups (Table 5). Differences between subgroups were not significant at baseline or measurements 2 or 3, reaching significance only at measurement 4. Improvements were seen in each of the 3 categories: interactive and communicative, managerial and administrative, and exclusive and situational. The observed attrition rate for completed and returned questionnaires from baseline to measurement 2 was 1828, from measurement 2 to 3 was 1611, and from measurement 3 to measurement 4 was 914.
Trends in Stress Scores.
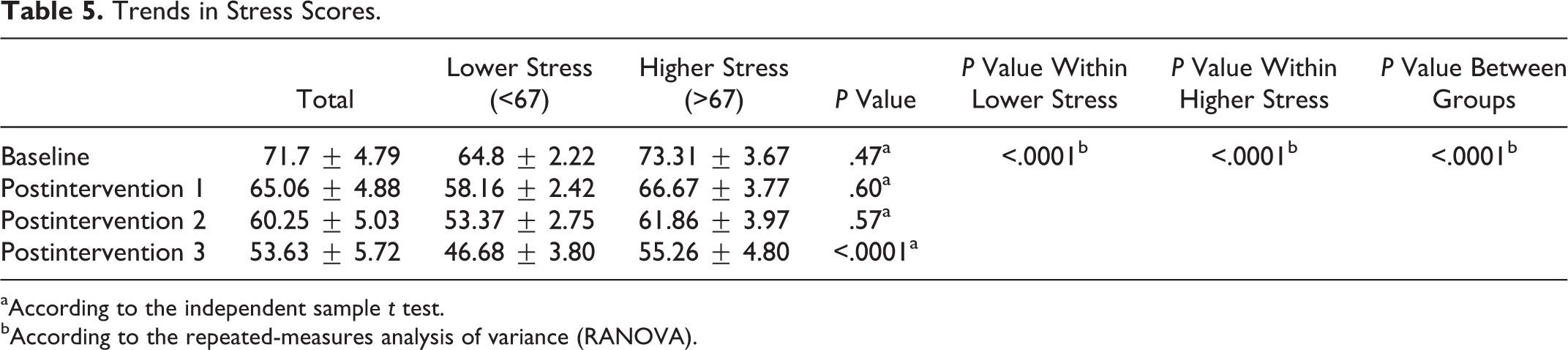
aAccording to the independent sample t test.
bAccording to the repeated-measures analysis of variance (RANOVA).
Discussion
In the 1930s and 1940s, Hans Selye approached the conceptualization of stress from the response end, viewing stress as a dependent variable, “a response to disturbing or threatening stimuli.” 9 Conversely, stimulus-based definitions consider stress to be an independent variable (generally environmental) that causes an individual to respond. Modern definitions take both into account. In the occupational stress literature, a stressor is regarded as any work-related characteristic, situation, or event that might initiate stress, while strain refers to the worker’s psychological or physiological reaction to stress. 10
Stressors may be categorized into 6 broad domains: (1) intrinsic job characteristics, (2) organizational roles, (3) work relationships, (4) career growth issues, (5) organizational factors including climate, structure, and culture, and (6) the home–work interface. 9 Social support may mediate the relationship between stressors and strain and may serve as a buffer between occupational stressors and adverse effects on health. 11 A stress response is triggered when ones perceived demands exceed the resources available to manage the stressor. 12,13
Stress is experienced on a continuum from eustress to burnout syndrome (BOS). Eustress is a term that is associated with the positive benefits of stress. In eustress, psychologic symptoms are excitement, increased mental acuity, and arousal. Individuals function effectively while managing resources to meet demands. 12 This response is intended to be immediate but limited. Frequent, chronic, or excessive stress exposure, however, may result in maladaptive psychological and physical effects. 14 Distress occurs when the stress response becomes maladaptive or negative effects are experienced. 12
The concept of BOS, as first described by Freudenberger in 1974, refers to a protracted course of distress in which one is unable to cope with stressors over an extended period of time, leading to depletion of the body’s defenses and ultimately physical and emotional exhaustion. 15 –18 In 1996, this concept was further refined and BOS was defined as a syndrome of emotional exhaustion, depersonalization, and reduced personal achievement. 19
In extreme cases, providers may develop signs and symptoms of posttraumatic stress disorder (PTSD). Posttraumatic stress disorder is caused by exposure to real or threatened death, serious injury, or sexual violence through direct experience or observation. Individuals may experience repeated invasive distressing memories, dreams, or dissociative events related to the traumatic event, psychological distress when exposed to similar experiences, or pronounced psychological reactions to internal or external cues resembling the event. In PTSD, individuals attempt to avoid distressing memories, thoughts, emotions, and external reminders of the incident. Patients may demonstrate amnesia, negative attitudes toward self or others, self-blame, decreased participation in previously enjoyed activities, or persistent negative emotions. Arousal and reactivity are affected and can present as irritability, aggression, self-destructive behaviors, hypervigilance, concentration difficulties, and sleep disturbances. 20 Posttraumatic stress disorder can be acute or chronic in nature and negatively affect work and home life. Nurses working in acute care environments (emergency department or ICU) are at particular risk for developing compassion fatigue, secondary traumatic stress, and PTSD. 21 This increased risk is due in part to cumulative exposure to direct and indirect traumatic events at work. 22 Moreover, workplace bullying has been identified as a significant predictor of PTSD among both experienced and novice nurses. 22
Coping With Stress
Coping refers to any cognitive or behavioral strategies used to interpret and change environmental conditions (problem-focused or instrumental coping) or manage the negative emotions associated with a stressor (emotion-focused coping). Problem-focused coping is used when the individual views the stressor to be within their control to change, whereas emotion-focused coping is implemented when the stressor is viewed as something to be endured (Table 6). 23 The evaluation of coping outcomes is largely subjective and difficult to measure. 24
Stress-Coping Strategies.
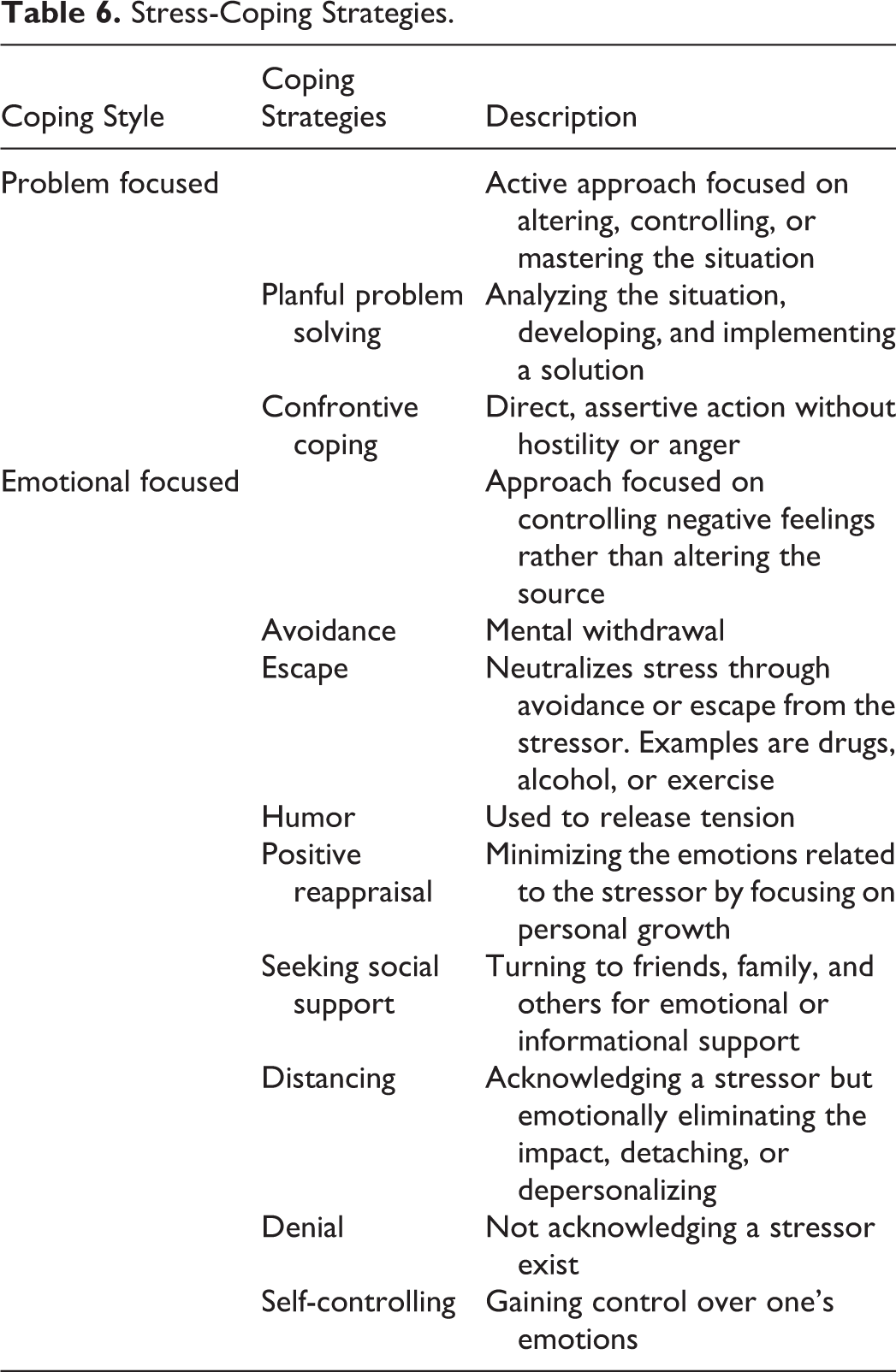
Nurses coping mechanisms may vary based upon the situation, age, and geography. 25 –28 Escape avoidance, denial, and distancing may be used to cope with emotional situations. Practically speaking, they may seek to avoid work, patients’ families, or patient assignments that cause distress or conflict. 29 –31 Moreover, they may not express their feelings due to fears of being judged or creating conflict or a bad work atmosphere. 32 Regarding generational differences, baby boomers tend to use self-controlling behaviors, while escape avoidance behaviors are used more often by Generation Y. 26
Geographical differences in utilized coping strategies highlight the influences of culture and variations in health systems. In a survey of 1554 hospital-based nurses, the most utilized coping strategies were problem focused for those from the United States, whereas emotion-focused strategies were most common for nurses from Asian countries: self-control (Japan, Thailand) and positive reappraisal (South Korea). 27 A smaller subsequent US-based survey of 135 ICU nurses reported the most frequently used coping strategies to be a mixture of problem-focused (confrontive coping, 60%; planful problem solving, 59.2%) and emotion-focused coping strategies (escape avoidance, 62.2%; seeking social support, 49.5%). 33 This variation highlights the difficulty in studying such problems and why stress reduction interventions must be designed and targeted for individual populations.
Individual personality traits also impact coping ability and associated work efficacy. High levels of conscientiousness are associated with active coping and planning with increased ability to address stressors, improved stress management, and decreased stress related to perceived competence, confidence, and time demands. 34,35 The use of problem-focused coping strategies and lowered levels of stress are also associated with the traits of openness, extroversion, and agreeableness. 35 Individuals with these traits report less stress related to dealing with difficult patients and less reduction in professional efficacy. In contrast, individuals with high levels of neuroticism utilize more emotion-focused coping strategies, such as venting, and reported increased role conflict and work overload. 35 Neuroticism, role conflict, and work overload have been reported to predict reduced professional efficacy, emotional exhaustion, and depersonalization in all dimensions of BOS. 36
Resilience, a trait that allows an individual to succeed while enduring hardship, can be learned. A decrease in symptoms of stress, PTSD, BOS, anxiety, and depression is associated with resilience. Hardiness, a trait defined as the incorporation of the elements of commitment, control, and challenge that prepare an individual to handle problematic life events, has been reported to result in increased optimism and flexibility when addressing problems. When addressing stressful situations, hardy individuals use rational-oriented, rather than emotional-oriented, coping styles. Increased hardiness is negatively associated with perceived stress and positively associated with an approaching style of coping. 37
Conditions that contribute to the achievement of emotional well-being in the ICU are achieving best care for the patient’s family, autonomy, achieving goals, and teamwork. In ICU nurses, emotional well-being leading to happiness and personal satisfaction is closely associated with providing the highest quality of care to both the patient and the family and is tied to a continued career working in the ICU. 38 Perceived failure results in distress and reduced emotional well-being. Nurses value the ability to practice autonomously within the ICU, including patient assessments, care plan development, and inclusion in the physicians’ decision-making processes. When teamwork is lacking, anxiety and unhappiness are reported. 38
Stress in Nursing
Health care is a demanding field, and nurses are at a high risk of occupational stress-related problems. 39,40 In this series, 71% of nurses reported being stressed. Moreover, nursing is one profession in which a link between employee well-being and organizational performance has been consistently demonstrated. Organizational stressors include inadequate pay 41,42 and lack of appreciation. 30 In Iran (2008), 48.8% of nurses reported income below the poverty line of 3 million rials (US$300) per month. 42 Frequent interruptions 41 and equipment in need of repair cause moderate to high stress. 43 Inadequate staffing is one of the most commonly cited stressors and likely has a compounding effect on perceived excessive workload. 5,12,21,29,33,41,42,44 –47 Similar to prior studies, we found that nurse–patient ratios were positively associated with increased stress levels in a multivariate analysis (OR: 1.17; P = .05). Nurses feel distressed when staffing ratios are perceived as unsafe 46,48 and when nursing assistant competency, support personnel, and nonlicensed personnel were inadequate for the patients’ demands. 46 Nurses may feel incompetent and that patient safety is jeopardized. 49 Floating to other units may also be a significant stressor. 16 Although we found no association between shift (morning, evening, night) and stress levels, shift rotation has been reported to positively associate with increased stress levels. 5,30 Furthermore, this may be exacerbated by acquired sleep deficits. 33 Distressed nurses may be more sensitive to noise, and auditory stimulation may contribute to concentration difficulties and increased irritability, stress, and fatigue. 43,47,50,51 The mean ICU noise level (71.9 decibels) surpasses the World Health Organization recommended level of 30 decibels, with peaks no greater than 40. 52
The quality of work relationships with patients, patients’ family members, physicians, and charge nurses are significant stressors. 12,18,33,44,47 As previously mentioned, social support may mediate the relationship between stressors and strain and may serve as a buffer between occupational stressors and adverse effects on health. 11 Thus, social support is a key aspect of a nurse’s life and ability to continue in a job. 53 The absence of social support significantly influences job turnover; conversely, nurses who have social support are more likely to stay in their job. 53 As reported in prior studies, our study confirmed that lower levels of supervisor collaboration and support and worse communication with supervisors positively correlated with increased stress. 42,43 Nurses tend to seek emotional support from nursing colleagues before taking problems home, 30,31 although our study did find that married status correlated with lower stress levels. Support is sought from physician colleagues last. 30,31
Stress may arise from the physician–nurse relationship when the physician is not available in an emergency, 33,43,47 uncertainty regarding treatments or transparency of physician disclosure, 12,31,33,44 treatments violating the patient’s wishes (eg, cardiopulmonary resuscitation or prolonged mechanical ventilation), 31,54 when asked by physicians not to disclose information to the patient, 53,54 or if they believe the physician to be incompetent. 31,48 Additionally, they report significant stress when they feel that unnecessarily painful procedures are performed on patients for medical student’s education 31,55 or when asked to assist with a procedure without first acquiring informed consent. 55
Due to the complex nature of working in critical care, nurses in the ICU encounter more ethical dilemmas than general ward nurses. 41 Nurses form bonds with patients and family members and develop a sense of being responsible for patients’ outcomes. 41,45 A consistently reported stressor is dealing with death and dying. 18,30,41,43,44,45,47 This may be worse when the nurse relates the distress from a patient’s situation with one in his/her own personal life, 38 when moral distress results from perceived inappropriate treatment, futile care, 31,48,55 patient suffering from prolongation of the dying process,31,55 or when they feel ignored or not engaged in the decision-making processes. 31 Nurses who participate in end-of-life family conferences report less distress. 48
Dealing with difficult patients is a frequently cited cause of stress for nurses. 18,41,44 Receiving threats from patients or family members does not necessarily result in job turnover but does correlate with avoidance in the form of increased job absenteeism. 53 Emotional abuse correlates with increased intent of turnover. 56 An increase in emotional abuse is associated with unexpected changes in patient acuity and results in increased time to perform tasks. 57 Violence has been correlated with an increase in the supply–demand ratio for nursing care, the number of incomplete nursing tasks at the end of each shift, increased admissions, unexpected changes in patient acuity, falls in medication errors, and delayed medication administration. 57 The perception of physical violence decreased with an increased proportion of bachelor’s degree nurses and more complete skill mix, a finding not assessed in the current study. 57 Positive nurse–physician relationships seem to offer a protective factor, as 1 study found this is inversely correlated with a threat of violence. 57
Although most threats, violence, and emotional abuse are perpetrated by patients and families, studies report coworkers are also responsible for a portion.56–58 Nursing has a hierarchical power structure with a deep-rooted history of victimizing the young and less experienced in the profession.59–61 During the process of becoming a nurse, the experience of being bullied is commonplace and psychologically damaging. 59 In a survey of 156 Israeli ICU nurses, 29% report experiencing bullying and 4% report at least 5 incidents over a week’s time. 58 The most frequently reported method of bullying was “exposed to unmanageable workload.” 58 Lateral violence (also known as horizontal violence) is another source of stress that is similar to bullying and classified as workplace violence. 62,63,70 Examples of lateral violence are gossiping, isolating, scapegoating, verbal aggression, angry outbursts, sabotaging, humiliating, and inequalities in work assignments. This problem is wide spread, with bullying rates reported as: Australia (15%-22%), Brazil (40%), Canada (19%), Italy (22%-30%), Turkey (21%), and United Kingdom (44%), United States (23%-27%). 63,70 Lateral hostility is negatively associated with peer relationships and job satisfaction, and the consequences include symptoms similar to other workplace stressors. 64 Nurses who are victims of lateral hostilities frequently request transfers, and many consider leaving the profession. 62,65 –67
Each of the aforementioned may promote increased absenteeism, turnover, health claims, and injuries, resulting in increased hospital expenditures. 42 A negative correlation exists between subjective stress and job performance. 68,69 Work absenteeism may be associated with physical work demand, autonomy, and physical and psychological aggression from patients and patient’s family members. 53 In a quantitative, cross-sectional study of 461 ICU nurses in the Netherlands, 30% intended to leave their job, with significant associations with night shift (P < .001), age (P < .001), perceived lack of professional development (P < .001), and lack of social support (P < .001). 53 The financial implications of replacing an ICU nurse is US$145 000. 70
Consequences of Stress on Acute Care Providers
The impact of stress can manifest as a variety of physical and psychiatric disorders, with 59% of nurses experiencing a psychiatric disorder. 71 Social dysfunction is the most prevalent psychiatric disorder (71%). 71 Depression and anxiety are common 71 ; however, BOS and PTSD are of particular concern for nurses in the emergency department and the ICU.
Those experiencing burnout have drained their physical and emotional resources in attempting to cope with the stressors present in the work environment. 72 Burnout syndrome is the inability to cope with stressors over an extended period of time 18 where the body’s defense system is depleted leading to exhaustion.17,73 Burnout syndrome has 3 key characteristics including emotional exhaustion, depersonalization, and feelings of failure. Burnout syndrome symptoms may fall into the following categories: affective (eg, depression, emotional instability), cognitive (eg, reduced attention and concentration), physical (eg, fatigue, sleep disturbance, eating problems, headaches), behavioral (eg, reduced job performance), motivational (eg, diminished idealism), interpersonal (eg, irritability, relationship rigidity, indifference), and organizational (eg, job turnover). 18 Studies have reported a burnout incidence of 28% to 33% among ICU nurses 18,32 and is associated with younger age, 18,41 organizational factors such as quality of relationships and perceived conflicts, and receiving requested vacation days. 18 Moreover, burnout is positively associated with higher fast-food consumption, infrequent exercise, higher alcohol consumption, and more frequent painkiller use. 74
Somatic and sleep complaints are highly prevalent (60.7%). 71 Sleep disturbance is common, often associated with work-related concerns (14.8%), affects quality and quantity, occurs on 25.9% of days (regardless of shift status), and plays a role in the development of physical and mental exhaustion. 5,75,76 Physical and mental exhaustion have been reported during 42% and 39% of shifts, respectively, with exhaustion, stress, and hypersomnia occurring in one-third of shifts. 76 Post-shift accidents and near accidents have been positively associated with exhaustion, struggling to stay awake, and the number of consecutive shifts worked. 76 Moreover, it has been reported that stress is related to increased musculoskeletal, gastrointestinal, and cardiovascular symptoms. 75 Muscle cramps and spasms, arthralgia, and back and neck pain are associated with job demands, social support, job strain, overcommitment, and higher stress.75,77
Posttraumatic stress disorder is reportedly experienced at a higher rates in ICU nurses. Manifestations of PTSD are sleep disturbances, irritability, agitation, annoyance, anger, and muscle tension. In a survey of US-based nurses comparing 140 ICU nurses to 121 medical–surgical nurses, 29% of ICU nurses experienced PTSD as compared to 14% of medical–surgical nurses. In a qualitative study of 744 ICU nurses using the Posttraumatic Diagnostic Scale, 21% had a diagnosis of PTSD originating from a workplace traumatic event. 21 Of those nurses experiencing PTSD, 70% reported experiencing symptoms for at least 3 months. 21 The inciting events leading to PTSD were reported as inability to rescue a patient (50%), experiencing verbal abuse by patient family members (39%), performing futile care (36%), and observing a patient expire (29%). 21
Provider Stress and Patient Outcomes
Job stress indicators were found to correlate with increased patient safety incidents. 4 Burnout has been associated with medical errors and inadequate patient safety. 74,78 Medical errors, cognitive errors, and decreased safety compliance are associated with increased stress, long work hours, high patient demand, and fatigue with struggling to stay awake.4,76,79,80 Nurses experiencing lack of autonomy, job instability, and relationship conflict also reported increases in patient safety incidents. 4 In addition to long work hours, 79 working overtime, nights, and rotating shifts have been reported to associate with increased fatigue and risk of medical errors or near errors. 76,79 To illustrate the impact of patient demand on patient safety, an increase of 1 patient in the nurses’ workload results in a 7% increase in patient mortality. 81
Interventions
A number of stress reduction interventions have been purposed and studied in ICU nurses. Given the previously discussed variation in coping mechanisms used by region and culture, 27,33 on-site professional resources offered through an institutional employee assistance program or other entity may be beneficial. This may include employee wellness programs; employee health screenings; adequate staffing; interdisciplinary debriefing following difficult cases; and role model, preceptor, or mentor programs. 82
Educational programs may also plan an important role in promoting staff wellness. These may include education about nursing care of the dying (ie, ELNEC courses) or other experiences aimed at fostering skill development in coping, adaptation, and emotional self-care. Due to the scope of the project and number of study sites, our study employed a combination of an educational lecture followed by visual stimuli posted in the workplace to remind the nurse of lecture material. Lastly, the serial questionnaire assessments also likely reminded participants of content they may have forgotten or not focused on previously. Some have advocated for instructed mindfulness-based stress reduction to decrease stress and burnout. 83 –86 Lastly, specialized retreats may play a role as well.
Limitations
There are some aspects of the Iranian health-care system that limit the generalizability of the findings. For example, most academic and tertiary care ICUs in the United States are closed ICUs; however, ICUs in Iran are generally semi-closed or open. We did not collect data on individual nurse’s psychiatric symptoms or diagnoses. We also did not collect data on workplace violence or lateral hostilities.
Conclusion
Health care is a demanding field, with a high level of responsibility and exposure to emotional and physical danger. In this national survey of 21 767 ICU nurses in Iran, we found that male gender, lower levels of peer collaboration, working with a supervisor on the unit, nurse–patient ratios, and working in a surgical ICU were positively associated with greater stress levels. Increasing age and married status were negatively associated with stress. Intensive care unit type (semi-closed vs open), ICU bed number, shift time, working on holidays, education level, and demographic factors including BMI, and number of children were not significantly associated with stress levels. As the largest study of its kind, these findings support those found in various European, North, and South American studies. Efforts to decrease workplace stress of ICU nurses by focusing on facilitating peer collaboration, improving resource availability, and staffing ratios are likely to show the greatest impact on stress levels.
Footnotes
Authors’ Note
Substantial contributions to conception and design, or acquisition, or analysis of data are credited to Amir Vahedian-Azimi, Mohammadreza Hajiesmaeili, Mari Kangasniemi, Joana Fornés-Vives, Farshid Rahimibashar, Mohammad A. Pourhoseingholi, Leily Farrokhvar, and Andrew C. Miller. Manuscript drafting and revision was performed by Andrew C. Miller, Rita L. Hunsucker, and Amir Vahedian-Azimi. Ethical Approval and Consent to Participate: The investigative review board Baqiyatallah University of Medical Sciences (Tehran, Iran) approved the study. Study participation was optional for respondents. Since the research presented no more than minimal risk of harm to participants and involved no procedures for which written consent is normally required outside the research context, the principle of implied consent was employed. Namely, that by completion of the survey instrument, the participant demonstrated their willful consent to participate. In accordance with IRB requirements, the investigator provided participants with a written informed consent statement regarding the research. Whereas Iranian medical ethics laws (![]() ) do not specifically address this topic, it is in accordance with other international ethics codes and laws including the US Federal Code of Regulations (45 CFR 46.117c). Consent for Publication: Based on the informed consent statement, implied consent allowed for both study participation and publication of de-identified aggregate results. There is no data contained within the manuscript from which individual patients or participants may be identified. Availability of Supporting Data: The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
) do not specifically address this topic, it is in accordance with other international ethics codes and laws including the US Federal Code of Regulations (45 CFR 46.117c). Consent for Publication: Based on the informed consent statement, implied consent allowed for both study participation and publication of de-identified aggregate results. There is no data contained within the manuscript from which individual patients or participants may be identified. Availability of Supporting Data: The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank the Loghman Clinical Research Development Center, Loghman Hakim Hospital, and Shahid Beheshti University of Medical Sciences (Tehran, Iran) for methodological, logistical, and financial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Logistical and limited financial support was provided by the Loghman Clinical Research Development Center, Loghman Hakim Hospital, and Shahid Beheshti University of Medical Sciences in Tehran, Iran. These entities had no role in the collection, analysis, or interpretation of data and in writing of the manuscript.