
Abstract
Purpose:
Sepsis is the leading noncardiac cause of intensive care unit (ICU) death. Pre-ICU admission site may be associated with mortality of ICU patients with sepsis. This study quantifies mortality differences among patients with sepsis admitted to an ICU from a hospital ward, emergency department (ED), or an operating room (OR).
Methods:
We conducted a retrospective cohort study of 1762 adults with sepsis using ICU record data obtained from a clinical database of an academic medical center. Survival analysis provided crude and adjusted hazard rate ratio (HRR) estimates comparing hospital mortality among patients from hospital wards, EDs, and ORs, adjusted for age, sex, and severity of illness.
Results:
Mortality of patients with sepsis differed based on the pre-ICU admission site. Compared to patients admitted from an ED, patients admitted from hospital wards had higher mortality (HRR: 1.35; 95% confidence interval [CI]: 1.09-1.68) and those admitted from an OR had lower mortality (HRR: 0.37; 95% CI: 0.23-0.58).
Conclusion:
Patients with sepsis admitted to an ICU from a hospital ward experienced greater mortality than patients with sepsis admitted to an ICU from an ED. These findings indicate that there may be systematic differences in the selection of patient care locations, recognition, and management of patients with sepsis that warrant further investigation.
Introduction
Sepsis is the 10th leading cause of US mortality, 1 –3 and the leading noncardiac cause of death in intensive care units (ICUs). 4 –6 The importance of early disease recognition has led to educational campaigns 7 and public health prevention programs, 8 whereas clinical trials 9 –12 have identified early recognition of serious infections, prompt treatment with appropriate antimicrobials, source control, and prompt resuscitation as key aspects of treatment associated with sepsis survival.
A few studies have shown that outcomes for critically ill adults with sepsis vary by their location immediately before admission to an ICU, but our understanding of the causes of this variation is incomplete. 13 The observation that patients admitted directly to hospital wards have higher in-hospital sepsis mortality than patients coming from the emergency department (ED) has led to the hypothesis that ED providers may detect and rapidly treat adults with sepsis more expeditiously than hospital ward providers. Studies supporting this observation, however, have primarily involved analysis of administrative data and have not included patients from other pre-ICU care settings such as the operating room (OR). It is difficult to exclude lower patient acuity as a cause of the lower mortality in patients coming from the ED because studies reporting this did not adjust for acuity with a robust acuity measure such as the Acute Physiology and Chronic Health Evaluation IV (APACHE IV) severity of illness measure, which was developed in large populations of critically ill adults. 14
We investigated the hypothesis that patients with sepsis have different mortality outcomes that can be predicted by their pre-ICU admission source. We used clinical data derived from a large health-care system’s medical records, allowing us to adjust for severity of illness and to stratify analyses by length of stay on the hospital wards prior to ICU admission for sepsis.
Methods
Study Design and Setting
We conducted an observational cohort study in 7 ICUs (3 medical, 2 surgical, 1 cardiac, and 1 mixed unit) at a level 1 trauma center in Worcester, Massachusetts (UMass Memorial Medical Center) serving more than 800 000 people residing in Worcester county (85% white, ∼13% ≥ age 65 years). 15 Data were collected from October 2012 to May 2015. UMass Memorial Medical Center is a 687-bed academic medical center that serves 41 454 inpatients annually. 16,17 This research was approved by the institutional review board of the University of Massachusetts; the informed consent requirement was waived.
Eligibility Criteria
Eligible patients had an ICU stay during the study period, were aged ≥18 years at admission, and met consensus definitions for sepsis, severe sepsis, or septic shock during the first 48 hours of ICU admission by documented physician diagnosis, which was then confirmed by a board certified intensivist through record review. 18 This method of identifying sepsis diagnoses has been previously validated in a subset of cases from this database and found to be highly accurate in previous studies. 19
According to the consensus definitions, a diagnosis of sepsis requires the presence of a clinically diagnosed infection in association with clinical criteria for the diagnosis of the systemic inflammatory response syndrome. Patients are considered to have severe sepsis if they met sepsis criteria and also had clinically diagnosed organ dysfunction. A septic shock diagnosis requires the presence of hypotension unresolved after volume resuscitation. 7
We excluded patients transferred from an outside hospital and patients transferred from a medical ICU to another hospital and included only first ICU admissions for each patient. In accord with the definition of “present on admission, 20 ” patients initially diagnosed with sepsis after the first 48 hours of ICU admission were excluded.
Admission Location
The primary characteristic of interest was the location from which the patient was admitted to the ICU, recorded when the admission order was created through the electronic health record (EHR). Admission location was defined as the last place the patient was cared for prior to transfer to an ICU and categorized as ED, hospital ward, OR, and others. Patients admitted to the ICU from a postoperative recovery unit were included in the OR group. All other patients were grouped into the “other” category. Because of the heterogeneous nature of this group, mortality estimates are not reported, although these patients were included in the statistical models. These categories were chosen based on commonly used EHR categories to reflect hospital practice and be of the most utility to those looking at quality improvement efforts.
Outcomes
The primary outcome was time until in-hospital mortality. Follow-up time was calculated as the number of days from sepsis diagnosis until death with censoring at hospital discharge. Time to ICU mortality was predefined as a secondary outcome and calculated as days from sepsis diagnosis to time of death in an ICU with censoring upon ICU discharge.
Potential Confounders
Patient demographics (age, gender), illness severity, neurological function measured by the Glasgow Coma Scale score, day of the week admitted, and body mass index (BMI) were considered potential confounders. 21 –23 Illness severity was defined using APACHE IV and Acute Physiology Score (APS) scores. 14,24 The APACHE IV and APS scores were recorded during the first 24 hours of admission. APACHE IV scores were obtained under a license from Cerner (Kansas City, Missouri). Burden of chronic disease was measured by the Chronic Health Evaluation measure. 25 Age, illness severity, and gender were a priori included in adjusted models. Other potential confounders (BMI, 26 Glasgow Coma Scale score, 27 and day of week admitted) 28 were tested for inclusion in the models using a 10% change of estimate strategy. Hospital level factors including the volume of patients with sepsis, which have been shown to impact treatment delay 29 were not expected to change during the study and were not included in the analyses. 22
Statistical Analyses
We compared patient characteristics including demographics, illness severity, and other characteristics by ICU admission location. Proportions were reported for categorical variables, and data were summarized by means and standard deviations, or medians and interquartile ranges for normally and nonnormally distributed continuous variables, respectively. Kaplan-Meier survival curves were calculated by admission location; the Wilcoxon test was used to detect differences. Cox proportional hazards models estimated associations between ICU admission source and mortality outcomes, adjusted for age, sex, and illness severity, after the proportional hazards assumption was verified. Other covariates were tested for inclusion using a 10% change in the estimate threshold and evaluated for collinearity. Because multicollinearity was observed with the APACHE IV and APS, only the APACHE IV score was included. We reported crude hazard rate ratios (HRRs), adjusted HRRs, and 95% confidence intervals (CIs). Time to event was defined as time from sepsis diagnosis at or after ICU admission to time of death. Patients who were not dead were censored at the time of hospital discharge.
Prespecified Subgroup Analyses
Cox proportional hazards models were used for subgroup analyses. We conducted an analysis to determine whether mortality among patients admitted to the ICU from hospital wards changed based on the length of stay prior to ICU admission. 30 Exposure was divided into categories: wards <2 days, wards 2 to 7 days, wards >7 days, ED, OR, and others. Another subgroup analysis restricted the population to 48 hours of follow-up from the time of ICU admission. We suggest that this restriction implies that sepsis is the most likely immediate cause of death.
Results
Among 24 872 ICU admissions, 2525 were for patients with sepsis, severe sepsis, or septic shock. We excluded 289 cases admitted from ICUs from another hospital, 112 patients discharged from the ICU to another hospital, and 1 underage case. Of the remaining 2123 admissions, 1951 were first admissions of unique patients. Of these, 1762 patients had sepsis diagnoses at the time of ICU admission or within 48 hours of admission, representing the final sample (Figure 1).
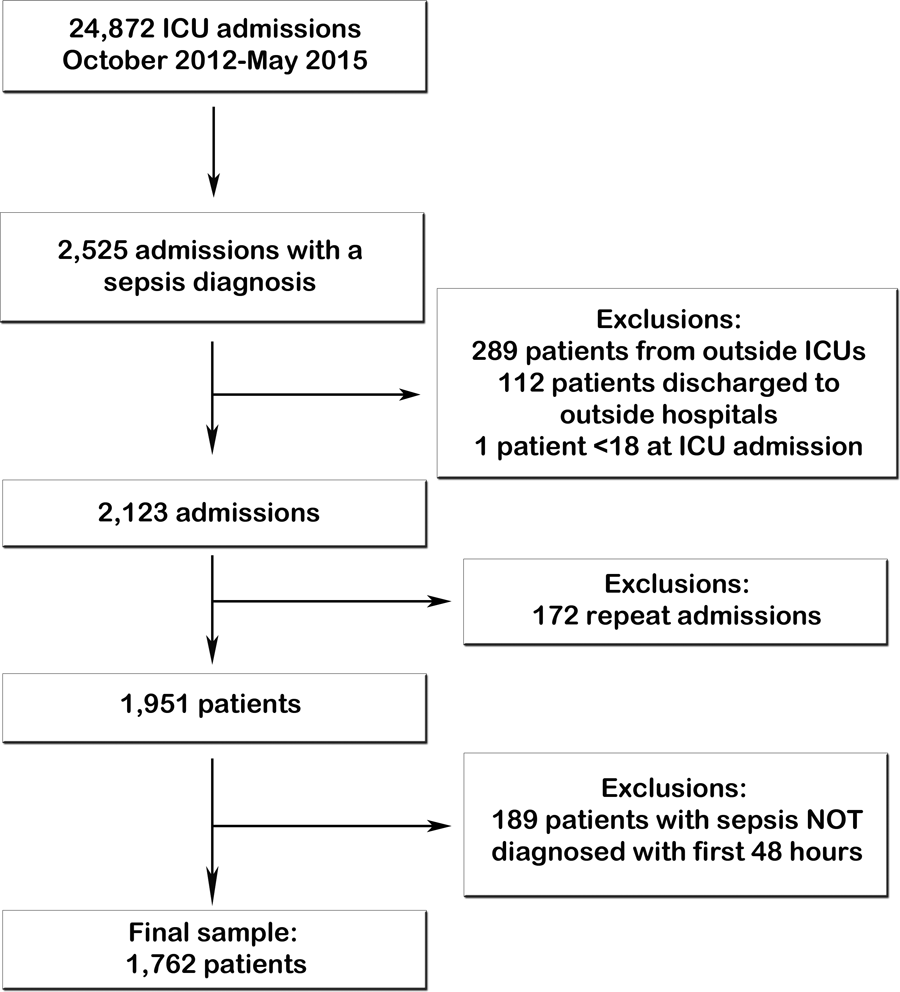
Selection of patients and study exclusions.
Sixty-eight percent of patients were admitted to the ICU from an ED, 19% from a hospital ward, and 11% from an OR. The characteristics of the study patients and their pre-ICU length of stay differed significantly by site with patients admitted to the ICU from the hospital wards having the longest pre-ICU length of stay. Patients admitted to the ICU from the OR had the longest total hospital lengths of stay; however, total ICU lengths of stay were similar among all groups. Patients admitted to an ICU from an OR were generally younger and less likely to have been admitted on a weekend and had a lower burden of chronic disease compared to other groups. Patients admitted to an ICU from a hospital ward were more likely to be underweight and be more severely ill at the time of admission to the ICU. Other demographic factors were relatively evenly distributed among groups (Table 1).
Characteristics of ICU Patients With Sepsis by ICU Admission Location.a,b.
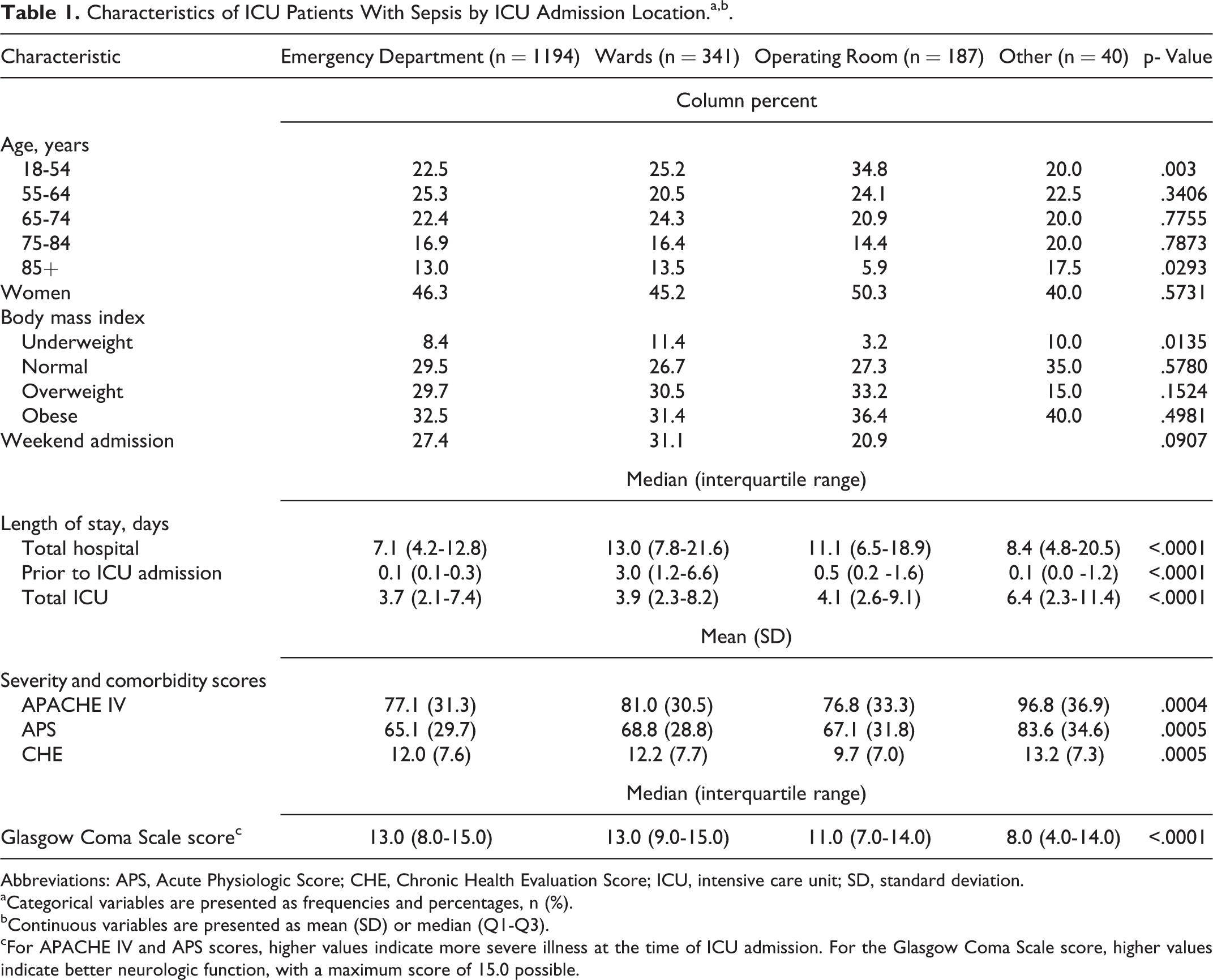
Abbreviations: APS, Acute Physiologic Score; CHE, Chronic Health Evaluation Score; ICU, intensive care unit; SD, standard deviation.
aCategorical variables are presented as frequencies and percentages, n (%).
bContinuous variables are presented as mean (SD) or median (Q1-Q3).
cFor APACHE IV and APS scores, higher values indicate more severe illness at the time of ICU admission. For the Glasgow Coma Scale score, higher values indicate better neurologic function, with a maximum score of 15.0 possible.
Hospital and ICU mortality rates differed by the pre-ICU admission site, with patients admitted to the ICU from the hospital wards having the highest rates of both hospital and ICU mortality compared to patients admitted to the ICU from the ED. Patients admitted to an ICU from an OR had the lowest rates of both hospital and ICU mortality compared to patients admitted to an ICU from an ED or hospital ward. There were 415 in-hospital deaths; 75% occurred in the ICU. Kaplan-Meier curves (Figure 2) show early separation of survival across settings (Wilcoxon test: P < .005). The unadjusted in-hospital death rate among patients admitted to an ICU from an ED was 23.6 per 1000 person-days, versus 30.1 per 1000 person-days among those admitted from the wards, and 7.3 per 1000 person-days among those patients admitted from an OR. The ICU rate of death was 28.1 per 1000 person-days among patients directly admitted to the ICU from the ED, 41.1 deaths per 1000 person-days among patients initially admitted to a hospital ward, and 9.9 per 1000 person-days among those admitted from an OR (Table 2). Adjusted HRRs were similar to crude HRRs.
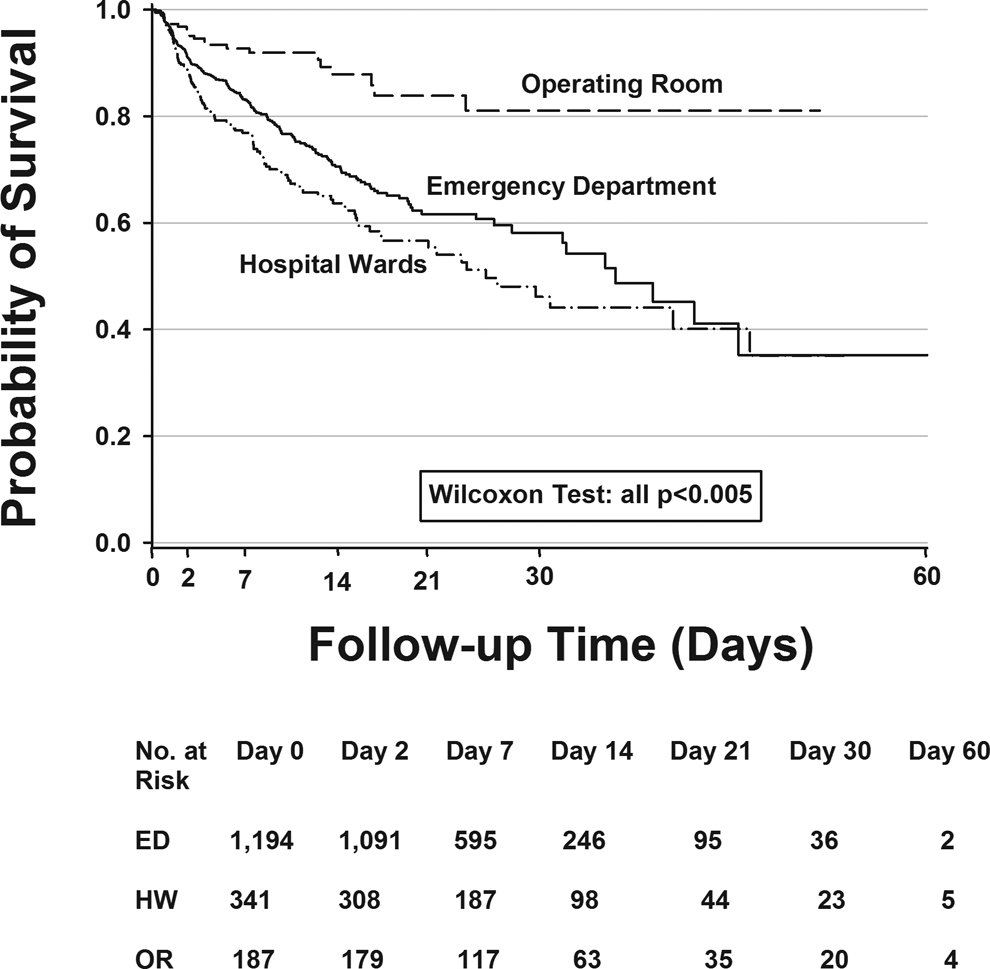
Kaplan-Meier survival curves by admission location.
Association Between ICU Admission Source and Mortality From Sepsis in ICU Patients.a
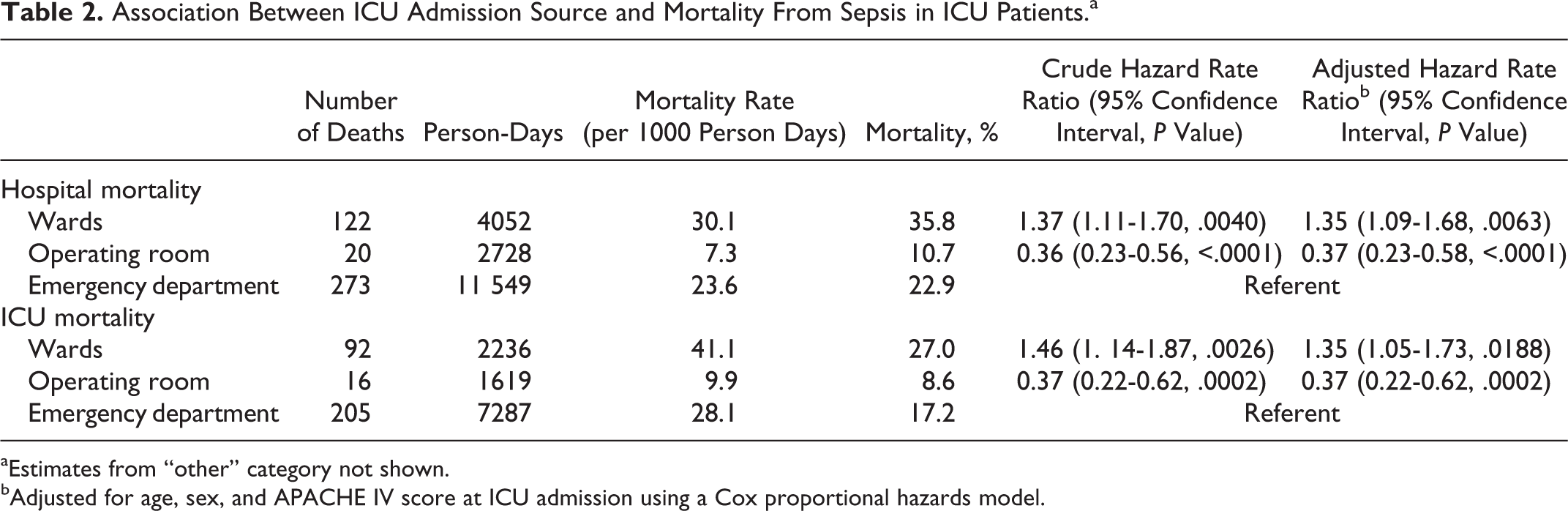
aEstimates from “other” category not shown.
bAdjusted for age, sex, and APACHE IV score at ICU admission using a Cox proportional hazards model.
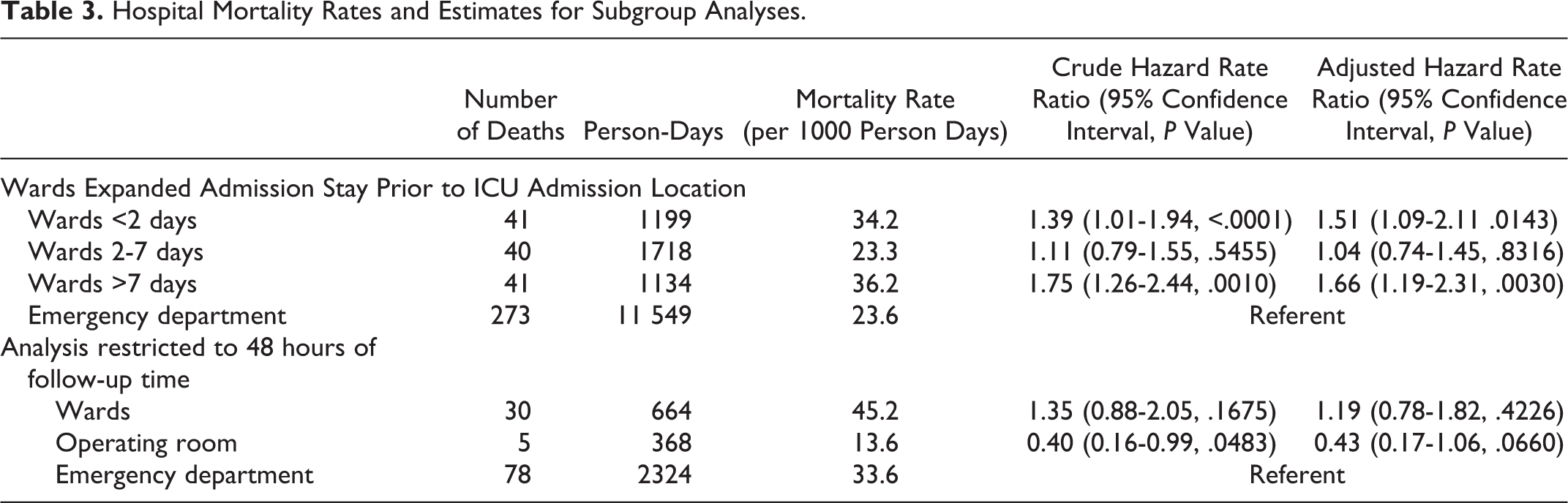
Among patients admitted to the ICU from a hospital ward, those patients with the shortest (<2 days) and those with the longest (>7 days) prior to admission to the ICU had increased rates of mortality. The median time to ICU admission from hospital admission for the group of patients who spent less than 48 hours on the wards was 24 hours (interquartile range: 13.68 hours to 36 hours). Among the group of patients who spent 48 hours or less on the hospital wards prior to ICU admission, there was a median time of 2.64 hours prior to ICU admission for sepsis diagnoses (interquartile range: 13.44 hours prior to admission to 2.4 hours post ICU admission). There was a median time between sepsis diagnosis and hospital admission of 4.08 hours after admission (interquartile range: 3.8 hours prior to hospital admission to 24 hours after admission) for those patients spending less than 48 hours on the hospital wards. When we restricted the population to 48 hours of follow-up, estimates of mortality rates did not appreciably change; however, precision was reduced (Table 3).
Hospital Mortality Rates and Estimates for Subgroup Analyses.
Discussion
We found significant associations among pre-ICU admission source and in-hospital and ICU mortality for patients with sepsis even after accounting for several key patient level factors such as severity of illness and comorbidity burden. Patients with sepsis admitted to the ICU from hospital wards had significantly higher mortality than patients admitted from the ED. Patients with sepsis admitted to the ICU from the OR had the lowest mortality. The direction of these associations are consistent with reports from clinical trials, 9 –11 guidelines for the treatment of sepsis, 31 and national patient safety recommendations. It has long been recognized by practicing clinicians that expeditiously identifying sepsis, more rapidly providing effective antimicrobials, early resuscitation, and effective source control are key determinants of outcomes, 12 but it is challenging to accurately measure the timeliness of delivery of these practices in different settings and additional work is needed to clarify what factors may be driving differences in mortality among patients with sepsis at different pre-ICU locations of care.
Our findings on sepsis-related hospital mortality among hospital ward patients, stratified by length of stay prior to ICU admission, lead us to speculate about possible modifiable determinants of mortality. We found an increased mortality rate among patients with both the shortest and longest lengths of stay on a hospital ward prior to ICU admission compared to a group with a stay of 2 to 7 days. Those with short lengths of stay may have been inappropriately triaged from the ED to the wards rather than the ICU and received less timely and effective initial care than those directly admitted to the ICU from the ED. However, among the patients spending less than 48 hours on the wards prior to ICU admission, the median time spent with sepsis was 1 day, suggesting that diagnosis and management in the ED may have initially improved the patient’s condition but that the improvement may not have been sustainable. We speculate that patients with the longest stays on the wards may have developed infections due to more virulent hospital acquired pathogens, or nutritional deficiencies and other factors that compromise immune function. 32,33,34
Our findings are consistent with and extend the findings of others. The estimates of hospital and ICU mortality from this study are consistent with recent estimates from 2 similar studies that did not use the APACHE IV acuity measure 5,35 and are consistent with a more narrowly focused study of patients directly admitted to wards. 36 Our study found a substantial number of patients with sepsis were admitted to the ICU from the OR, indeed 11% of our cases were identified as being admitted from the OR, a setting not addressed in previous studies. Among these patients, 40% had elective urological, orthopedic, or abdominal surgical procedures for a known or suspected infection and had circulatory compromise that was recognized and managed in the OR. The nature of these surgical procedures is consistent with generally accepted surgical practice emphasizing prompt source control to achieve better outcomes among patients with infections. The strength of our finding that patients admitted to the ICU from the OR had better outcomes compared to patients admitted to the ICU from the ED lends support to the validity of the model.
This study has important limitations. The findings of this single-center study may not be applicable to all centers. The patients included in this study were likely to be more severely ill than many patients with sepsis and to have higher mortality risk. While informative, including patients referred from an OR also introduced selection bias as patients determined to be able to withstand the physiological demands of surgery are likely to be healthier than other patients, and patients with infectious diseases amenable to surgical intervention may have lower mortality rates than patients with other conditions. Adjustment for the organ system involved in the infection giving rise to sepsis could reduce this bias. Age and illness severity were distributed relatively evenly among pre-ICU admission sites and adjusted for in the analyses, limiting bias from these 2 correlates of physiologic stamina. Although we adjusted for age, illness severity, and chronic disease burden, it is possible that the adjustments did not fully control for confounding. Stratification by presenting stage of sepsis (sepsis, severe sepsis, or septic shock) may provide additional information and control for confounding; however, we were unable to stratify our data in this fashion and suggest this sort of stratification as an area of interest in future research in this area. However, given that these patients required management in an intensive care setting, it is likely that a substantial majority of patients would meet criteria for severe sepsis or septic shock. Similarly, while principal procedure codes were available for a portion of the patients, future research with more granularity of surgical procedures and whether those procedures were intended for source control is needed. Additionally, we were not able to use microbiology data to determine virulence of pathogens, or to evaluate the timing of delivery of fluid and antibiotics, nor were we able to evaluate initial choices of antibiotics for appropriateness to the pathogen or the patient’s response to initial resuscitation attempts. Exposure categories were determined based on EHR reports of patient location but do not necessarily directly reflect patient time spent at each location precisely. Nonetheless, pre-ICU admission source categories drawn from the EHR may prove useful for quality improvement efforts and design and targeting of studies to the care locations most likely to derive substantial benefit.
This study found an association between the pre-ICU admission site of care and mortality among patients with sepsis, confirming prior findings of differences of the outcomes of patients based on their pre-ICU care setting within the hospital. This observation is an important building block for looking at the factors that determine differences in selection of patients for location of care and recognition and management of sepsis. These studies would further our understanding of which resources are required to improve sepsis recognition and treatment and allow educational campaigns to better tailor their messages to the site of care potentially reducing the number of lives lost due to sepsis.
Footnotes
Acknowledgments
The authors would like to thank Jacob Hunnicutt and Christina Griecci for their role in reviewing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.