
Abstract
Purpose:
We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the effect of high-flow nasal cannula (HFNC) on reintubation in adult patients.
Procedures:
Ovid Medline, Embase, and Cochrane Database of Systematic Reviews were searched up to November 1, 2016, for RCTs comparing HFNC versus conventional oxygen therapy (COT) or noninvasive ventilation (NIV) in adult patients after extubation. The primary outcome was reintubation rate, and the secondary outcomes included complications, tolerance and comfort, time to reintubation, length of stay, and mortality. Dichotomous outcomes were presented as risk ratio (RR) with 95% confidence intervals (CIs) and continuous outcomes as weighted mean difference and 95% CIs. The random effects model was used for data pooling.
Findings:
Seven RCTs involving 2781 patients were included in the analysis. The HFNC had a similar reintubation rate compared to either COT (RR, 0.58; 95% CI, 0.21-1.60; P = .29; 5 RCTs, n = 1347) or NIV (RR, 1.11; 95% CI, 0.88-1.40; P = .37; 2 RCTs, n = 1434). In subgroup of critically ill patients, the HFNC group had a significantly lower reintubation rate compared to the COT group (RR, 0.35; 95% CI, 0.19-0.64; P = .0007; 2 RCTs, n = 632; interaction P = .07 compared to postoperative subgroup). Qualitative analysis suggested that HFNC might be associated with less complications and improved patient’s tolerance and comfort. The HFNC might not delay reintubation. Trial sequential analysis on the primary outcome showed that required information size was not reached.
Conclusion:
The evidence suggests that COT may still be the first-line therapy in postoperative patients without acute respiratory failure. However, in critically ill patients, HFNC may be a potential alternative respiratory support to COT and NIV, with the latter often associating with patient intolerance and requiring a monitored setting. Because required information size was not reached, further high-quality studies are required to confirm these results.
Introduction
In adult patients after weaning and extubation, reintubation rate is approximately 10% to 20% and is associated with poor outcomes. 1 Because hypoxemia is one of the major causes of extubation failure, almost all patients receive oxygen commonly provided via nasal cannula, simple or Venturi face mask, which is referred to as conventional oxygen therapy (COT). 2,3 Nevertheless, COT might be sometimes inadequate, especially in patients with acute respiratory failure (ARF) demanding high inspiratory flow. 4,5 In these cases, noninvasive ventilation (NIV) is often applied. Although studies have shown that, compared to COT, the application of NIV could decrease the reintubation rate in high-risk patients, 6,7 whether routine use of NIV prevents reintubation is still inconclusive. Additionally, minimizing air leaks and gastric distension and patient’s cooperation and tolerance are crucial for the success of NIV. 8 –11 Moreover, a high degree of health-care resources are required for the application of NIV, which is usually carried out in intensive care units (ICUs) or other monitored settings. 8 –11
High-flow nasal cannula (HFNC), which delivers heated and humidified oxygen and air via nasal prongs with a maximum flow of 60 L/min and at a prescribed inspired oxygen concentration, might provide an alternative to COT or NIV. 12,13 The HFNC was first and extensively used in neonatal and pediatric patients and might improve oxygenation, decrease need for intubation, and attenuate complications. 14 –16 More recently, HFNC has attracted great attention as a potential supportive therapy in a variety of adult patients with diverse underlying conditions, including ARF, during bronchoscopy, or during intubation, and so on. 17 –19 Although a number of systematic reviews and meta-analyses examining the use of HFNC in adult patients have been published recently, none of them exclusively focused on the effect of HFNC on reintubation. 20 –25 Consequently, 3 important questions relating to the role of HFNC in postextubation management remain unanswered. First, can HFNC, compared to COT or NIV, avoid reintubation? Second, which specific patient population(s) might benefit from HFNC? Third, from a safety perspective, does HFNC do more than simply delay invariable reintubation with its associated risks? Therefore, we conducted this systematic review and meta-analysis of randomized controlled trials (RCTs) examining the use of HFNC after extubation to focus on these questions.
Materials and Methods
The present work followed the preferred reporting items for systematic reviews and meta-analyses guidelines (PRISMA), 26,27 and the protocol was registered on PROSPERO (http://www.crd.york.ac.uk/PROSPERO/; CRD42016033449).
Study Identification
Two trained investigators (H.W.H. and X.M.S.) independently performed study searching, screening, and identification. Discrepancies were resolved by discussion and consensus. Ovid Medline, Embase, and Cochrane Database of Systematic Reviews were searched for relevant studies published from inception to November 2016. The comprehensive computer search was conducted using the key words of “HFNC” or “HHFNC” or “HHFN” or “high-flow nasal cannula” or “high-flow nasal cannulae” or “high-flow oxygen therapy” or “nasal high-flow oxygen therapy” and “oxygen therapy” or “COT” or “SOT” or “venturi mask” or “NIPPV” or “non-invasive positive pressure ventilation” or “noninvasive positive pressure ventilation” or “non-invasive ventilation” or “noninvasive ventilation” and “post-extubation” or “after extubation” or “following extubation” or “extubated patients.” In addition, we searched the bibliographies of all selected articles and reviews for other relevant studies.
Studies complying with the following criteria were included: (1) design: RCT; (2) population: adult (≥18 years) patients after extubation; (3) intervention: the use of HFNC compared to a control group receiving COT or NIV. The COT included low-flow (nasal prong, simple, or nonrebreather mask) or high-flow devices (Venturi or high-flow face mask). The NIV included bilevel positive airway pressure (BiPAP) or continuous positive airway pressure (CPAP); and (4) outcomes: reintubation rate reported as either primary or secondary outcome. Studies published in abstract form were excluded.
Outcome Variables and Definitions
The primary outcome was reintubation. The overall rate of reintubation and need for NIV was also collected in trials comparing HFNC with COT. The secondary outcomes included complications, tolerance and comfort, time to reintubation, length of stay (LOS), and mortality.
Reintubation rate was separately compared in HFNC versus COT only or HFNC versus NIV only. Post hoc analysis was performed in the subgroup of postoperative and critically ill patients.
Data Extraction and Risk of Bias Assessment
Two investigators (H.W.H. and X.M.S.) independently extracted data using a standardized form, with no blinding of trials (eg, authors, institutions, or the publication source). We assessed the methodological quality of the study using the risk of bias assessment tool from the Cochrane handbook for RCTs. 27 Since blinding caregivers was not possible with this intervention, we only assessed whether outcome assessors were blinded. Disagreements were resolved through group discussion and consensus. For each outcome, we independently rated the quality of evidence across trials using the grading of recommendation assessment, development and evaluation (GRADE) approach. 28
Data Synthesis and Analysis
Data were analyzed using RevMan Review Manager (version 5.3; Nordic Cochrane Review Centre, Copenhagen, Denmark). Dichotomous outcomes were presented as risk ratio (RR) with 95% confidence intervals (CIs). Continuous outcomes were presented as weighted mean difference (MD) and 95% CIs. Statistical heterogeneity across trials was evaluated by χ2 and I 2 tests. The random effects model was used for data pooling which incorporates heterogeneity and gives wider CIs when heterogeneity is present. 29 Interaction P values were calculated to test for differences between the subgroups. A P value <.05 was considered statistically significant. Funnel plot was performed to determine publication bias. Trial sequential analysis (TSA) was used to assess the possibility of random error due to paucity of available data and was conducted using TSA Program version 0.9 (Copenhagen Trial Unit, Denmark). If the cumulative Z curve enters the futility area or crosses the trial sequential monitoring boundary, the anticipated effect may reach a sufficient level of evidence, and further trials are not needed. If this does not occur, evidence is insufficient for drawing a conclusion.
Results
Trial Identification and Characteristics
The study selection process is shown in Figure 1. The initial database search yielded 857 records. Of 44 potentially eligible studies, we excluded 26 non-postextubation studies, 17 –19,30 –52 9 non-RCT studies, 53 –61 1 abstract, 62 and 1 study not involving reintubation rate. 63 Finally, 7 RCTs with 2781 patients were included. 64 –70 In particular, RCTs comparing HFNC to COT or NIV to prevent need for intubation (rather than reintubation) in patients with ARF either in emergency department 30,38,39 or in hospital 41 or ICU 40 were excluded.
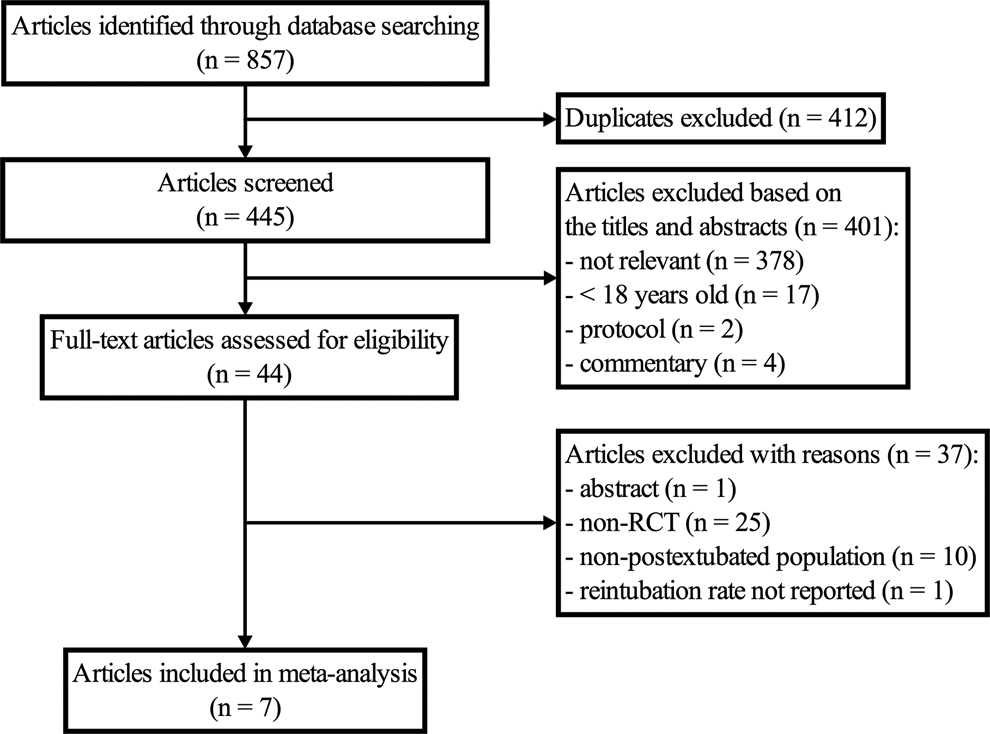
Study inclusion flowchart.
Table 1 describes the characteristics of the included trials. Five trials were multicenter.
64
–67,69
Four trials only enrolled postoperative patients, 3 in cardiothoracic surgery patients
67,68,70
and 1 in major abdominal surgery patients,
64
while the other 3 trials enrolled critically ill patients.
65,66,69
Duration of mechanical ventilation prior to extubation was 6 hours in patients after major abdominal surgery
64
and ranged from 12 to 15 hours in patients after cardiac surgery
67,68
and 1 to 2 to 5 days in critically ill patients
66,69
. The characteristics of the interventions and predefined outcomes are listed in Table 2. As presented, 5 RCTs compared HFNC with COT,
64,66,68
–70
including nasal prongs or simple face mask
Characteristics Data of Studies Included in Meta-Analysis.
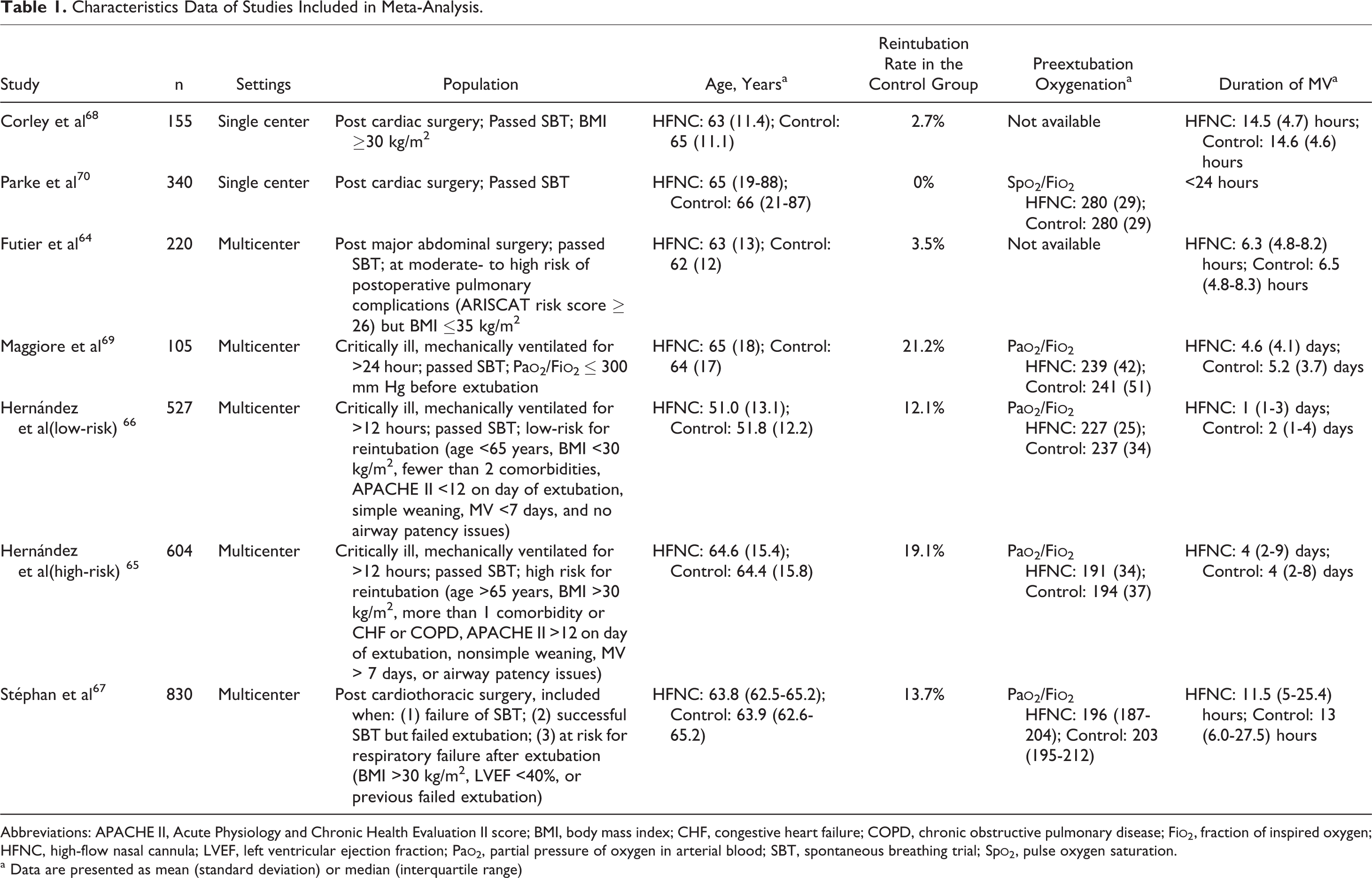
Abbreviations: APACHE II, Acute Physiology and Chronic Health Evaluation II score; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; Fi
a Data are presented as mean (standard deviation) or median (interquartile range)
Characteristics of Interventions and Predefined Outcomes of Studies Included in Meta-Analysis.
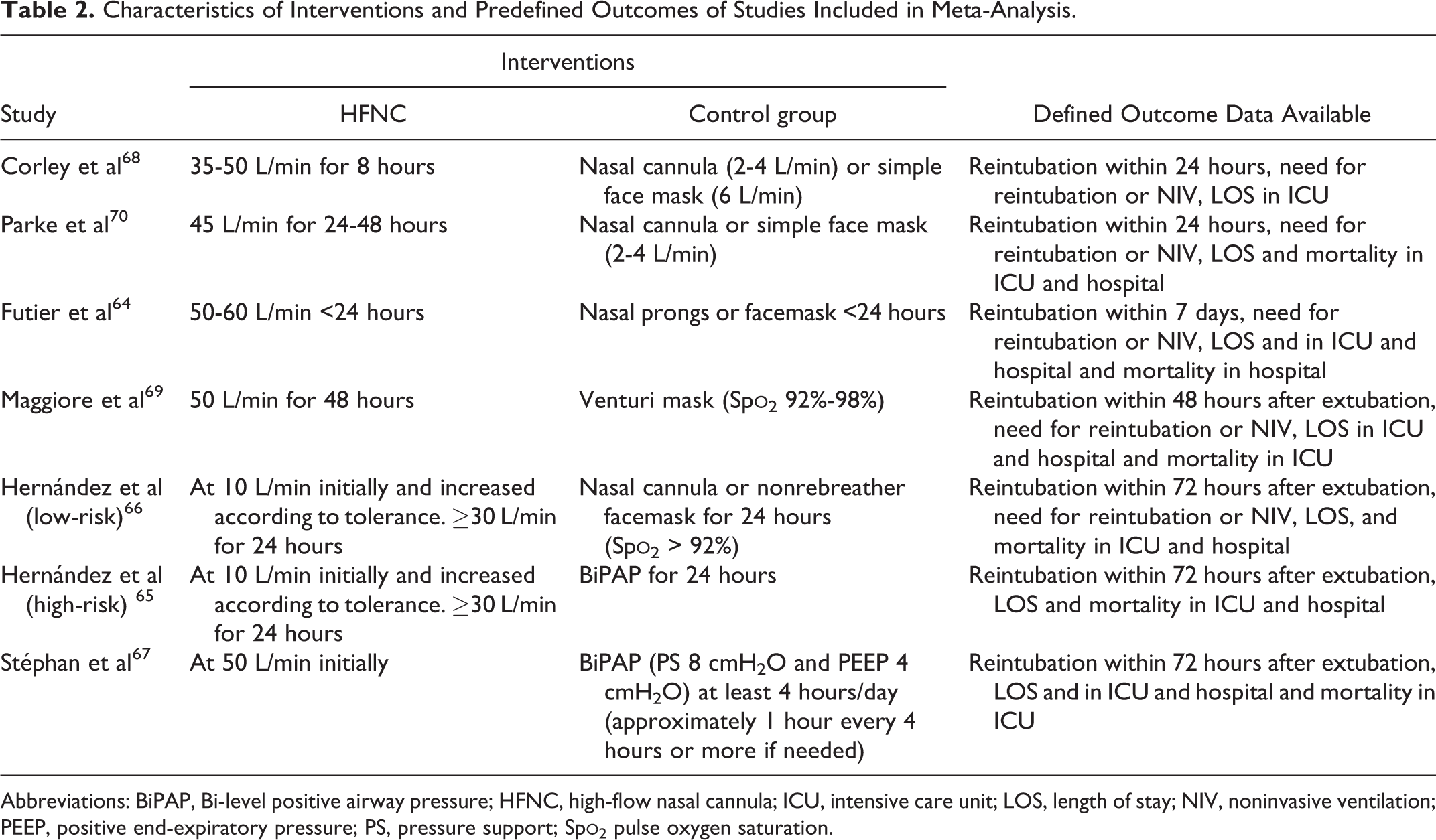
Abbreviations: BiPAP, Bi-level positive airway pressure; HFNC, high-flow nasal cannula; ICU, intensive care unit; LOS, length of stay; NIV, noninvasive ventilation; PEEP, positive end-expiratory pressure; PS, pressure support; Sp
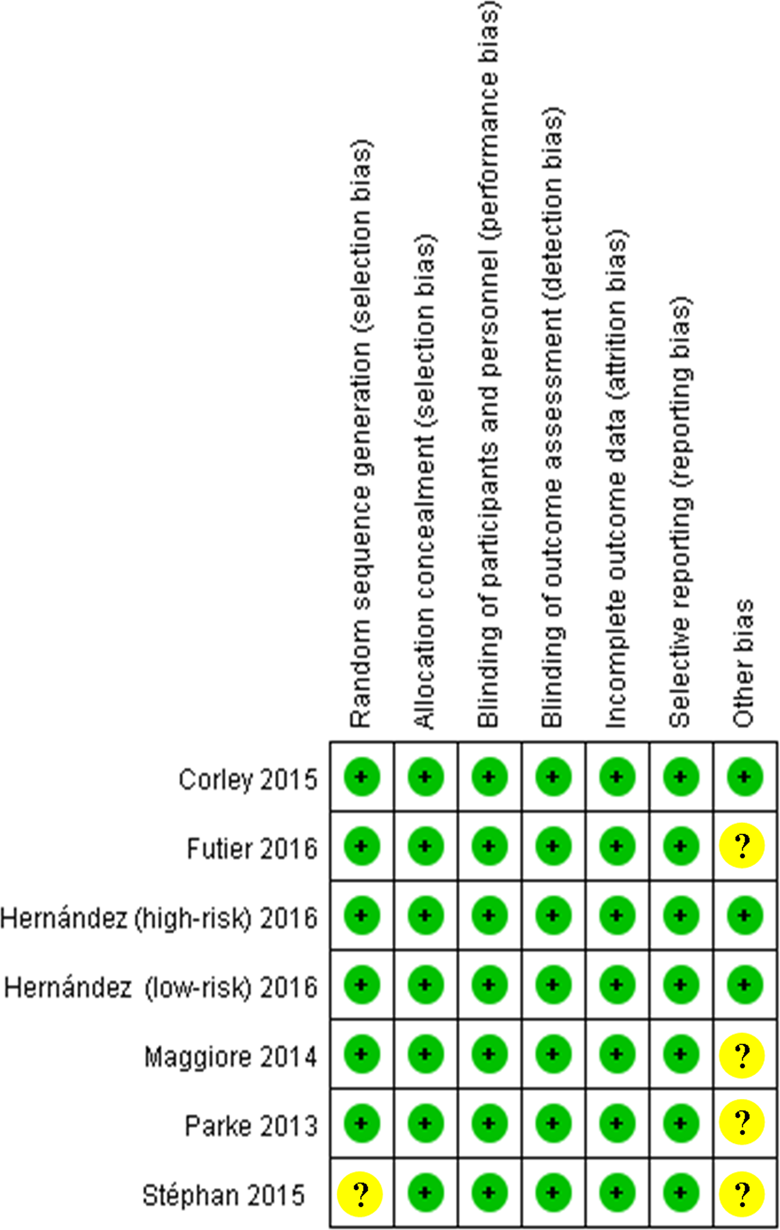
Summary of risk of bias. Green circles indicate low risk of bias and yellow circles indicate unclear risk of bias.
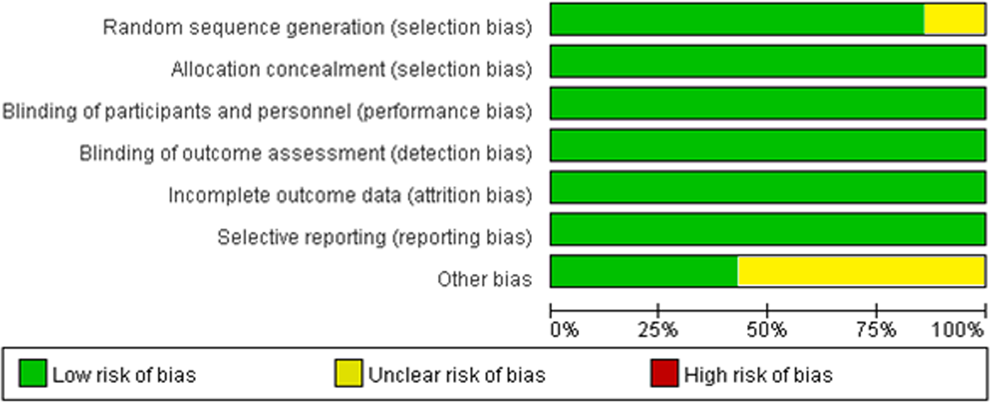
Overall risk of bias using the Cochrane risk of bias tool.
Quality of Evidence of Included Trials Assessed by the Grading of Recommendation Assessment, Development, and Evaluation (GRADE).
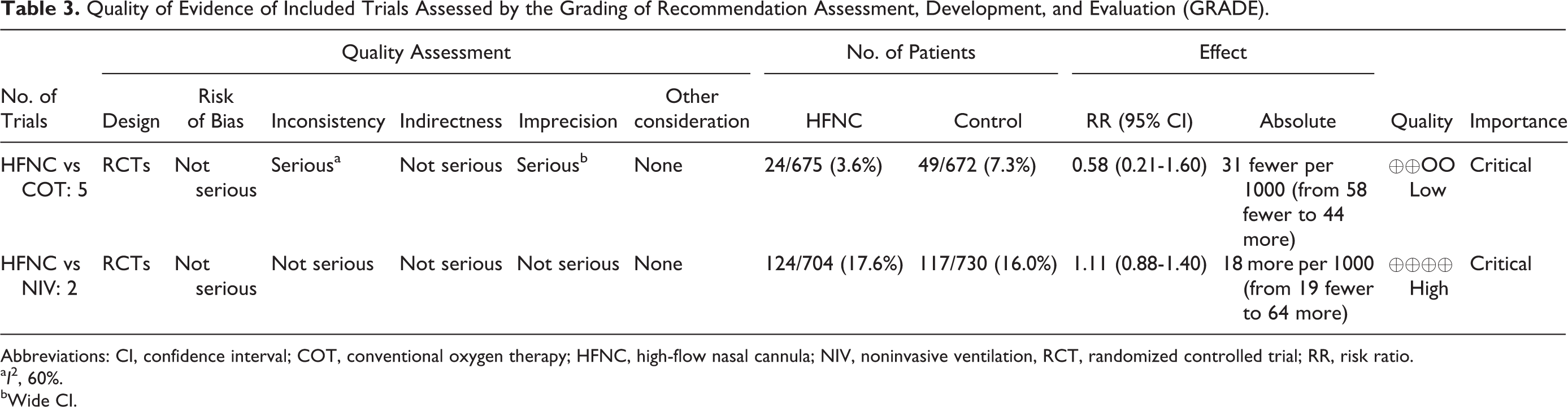
Abbreviations: CI, confidence interval; COT, conventional oxygen therapy; HFNC, high-flow nasal cannula; NIV, noninvasive ventilation, RCT, randomized controlled trial; RR, risk ratio.
a I 2, 60%.
bWide CI.
Reintubation Rate
Reintubation rate was reported as the primary outcome in 3 RCTs 65 –67 and as the secondary outcome in 4 RCTs. 64,68 –70 Five RCTs compared HFNC to COT, 64,66,68 –70 and no significant difference was found in reintubation rate overall (n = 13 47; P = .29; I 2 = 58%; RR, 0.58; 95% CI, 0.21-1.60; Figure 4A). Subgroup analysis in critically ill patients 66,69 found that HFNC significantly decreased reintubation rate compared to COT (n = 632; P = .0007; I 2 = 4%; RR, 0.35; 95% CI, 0.19-0.64), while in the subgroup of postoperative patients, 64,68,70 reintubation rate was similar in the 2 groups (n = 715; P = .61; I 2 = 23%; RR, 1.44; 95% CI, 0.35-5.86; interaction P = .07). Results were similar if the outcome was expanded to include reintubation or need for NIV with lower rates in HFNC-treated patients only in the subgroup of critically ill patients (P = .0001) and not in the postoperative patient subgroup (P = .12) with significant differences between subgroups (interaction P < .001; Figure 5). Two RCTs compared HFNC with NIV, in critically ill 65 and postoperative patients. 67 No significant difference was found in reintubation rate overall (n = 1434; P = .37; I 2 = 0%; RR, 1.11; 95% CI, 0.88-1.40) or between the 2 subgroups (interaction P = .52; Figure 4B). The TSA showed that the cumulative Z curves did not cross any of the boundaries and reached the required information size, so evidence was insufficient for drawing a conclusion.
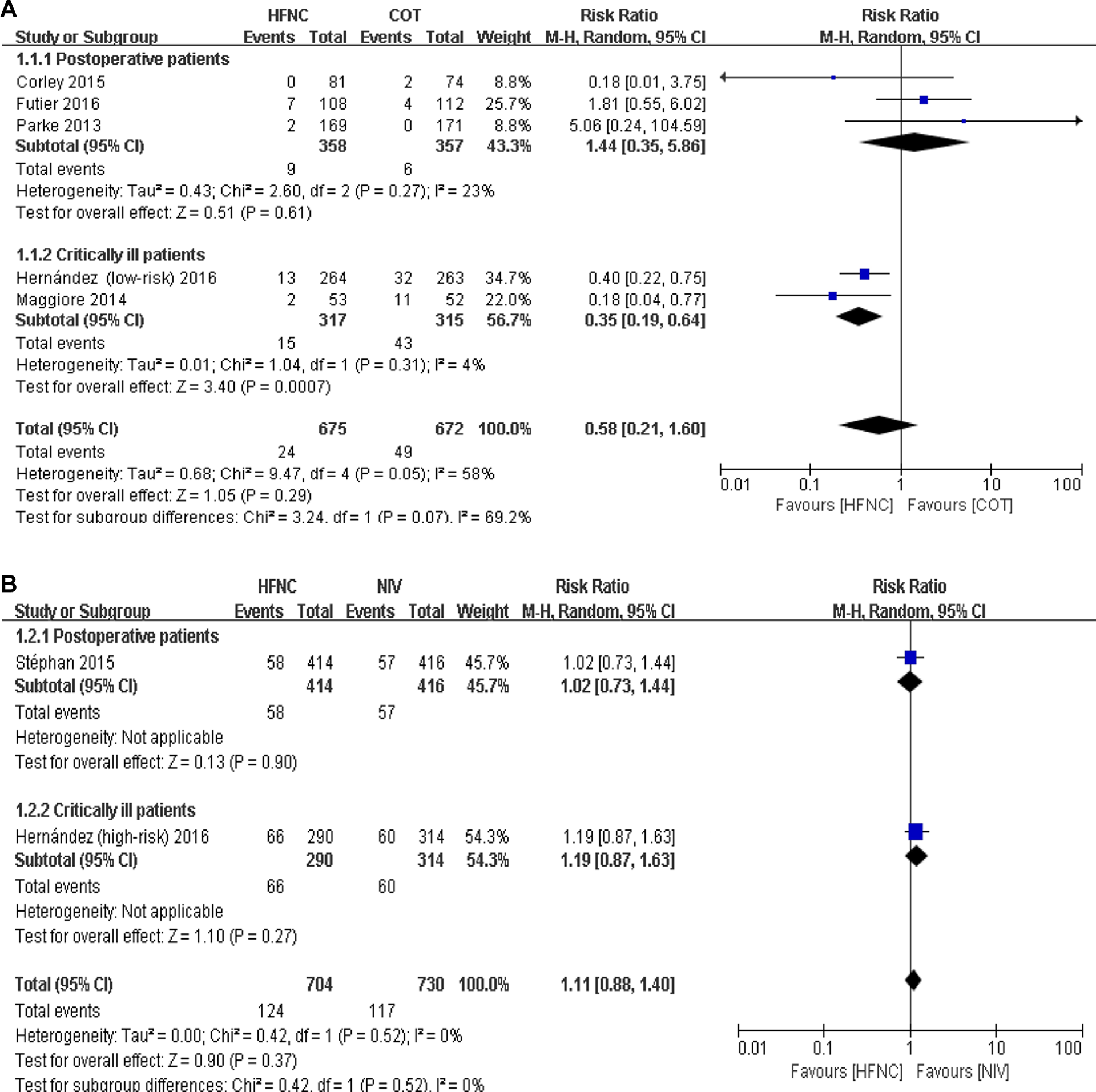
Forest plot comparing reintubation rate after extubation in high-flow nasal cannula (HFNC) versus conventional oxygen therapy (COT;A) and in HFNC versus noninvasive ventilation (NIV; B). Including only the postoperative cardiac surgery trials (Parke et al70 and Corley et al68) change the post-operative pooled RR from 1.44 (95% CI: 0.36-5.81, P = .61; I 2=22%) to 0.96 (95% CI: 0.04-24.84, P = .98; I 2 = 57%) and the postoperative versus critically ill subgroup interaction P value from .07 to .55.
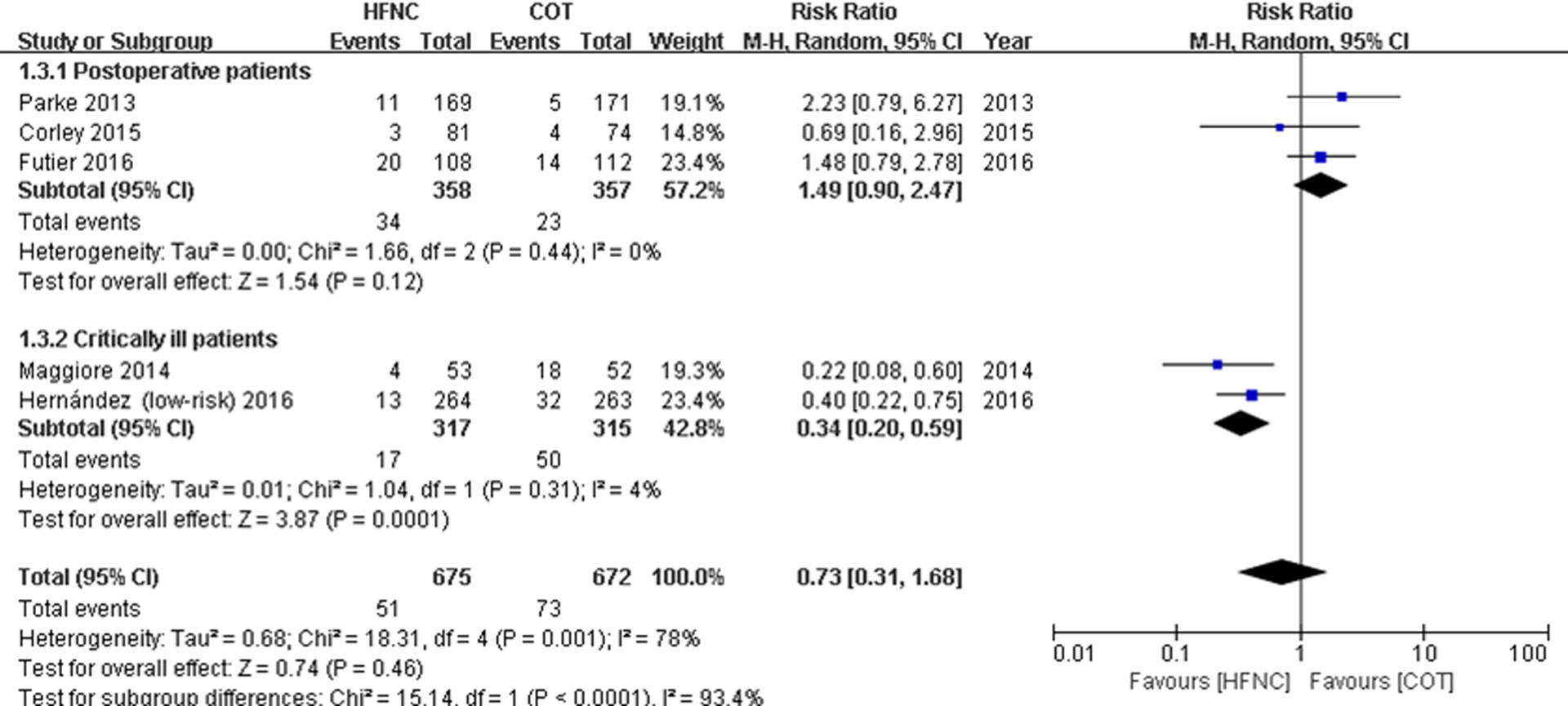
Forest plot comparing the overall rate of reintubation and need for noninvasive ventilation (NIV) after extubation between high-flow nasal cannula (HFNC) and conventional oxygen therapy (COT). Including only the postoperative cardiac surgery trials (Parke et al70 and Corley et al68) change the postoperative pooled risk ratio (RR) from 1.49 (95% confidence interval [CI]: 0.90-2.47, P = .12; I 2 = 0%) to 1.39 (95% CI: 0.45-4.31, P = .57; I 2 = 40%) and the postoperative versus critically ill subgroup interaction P value from <.0001 to .03.
Complications, Tolerance, and Comfort
Complications were reported using different measures in 4 trials, 2 each comparing HFNC with COT 66,69 and NIV. 65,67 Hernandez et al reported that no nasal mucosa or skin trauma was found in the HFNC group in both low-risk (HFNC vs COT) and high-risk (HFNC vs NIV) patients. 65,66 Stéphan et al 67 found that, compared to NIV, HFNC decreased the trend in skin breakdown (7.9% vs 14.2%; P = .05) in cardiothoracic patients with ARF. When compared to Venturi mask, Maggiore et al 69 found a lower rate of interface displacement (32% vs 56%, P = .01) and oxygen desaturation (40% vs 75%, P < .001) in the HFNC group.
Tolerance and comfort were reported in 5 trials, 3 in HFNC versus COT 64,66,69 and 2 in HFNC versus NIV. 65,67 Comparable tolerance and comfort was found in 3 trials. 65,67,69 Hernandez et al 65 found that in high-risk patients, all patients in the HFNC group tolerated HFNC, but 42.9% patients in the NIV group discontinued NIV for 25% or more of the per-protocol time. When compared to Venturi mask, lower interface-related discomfort scores (rated on 0-10 scales; mean [standard deviation]: 2.6 [2.2] vs 5.1 [3.3], P = .006) and airway dryness scores (2.2 [1.8] vs 3.7 [2.4], P = .002) at 24 hours were found to be lower in the HFNC group. 69
Time to Reintubation
Two trials reported time to reintubation, and no significant difference was found in either HFNC versus COT (median [interquartile range]: 19 [12-28] vs 15 [9-31] hours, P = .10) 66 or HFNC versus NIV (26.5 [14-39] vs 21.5 [10-47] hours; absolute difference, +5 hours; 95% CI, −24 to 34 hours). 65
Length of Stay and Mortality
All included trials reported LOS. For ICU LOS, no significant difference was found in either HFNC versus COT 64,66,68 –70 or HFNC versus NIV 65,67 (Figure 6). There was no significant difference in the overall pooled HFNC versus COT results between subgroup analysis in critically ill and postoperative patients (interaction P = .83). The 1 RCT in critically ill patients 65 suggested a 1-day decrease in ICU LOS in HFNC versus NIV (P = .006), but the other RCT in high-risk postoperative patients 67 showed no difference (P > .999) so that a statistical difference was found between subgroups (interaction P = .04).
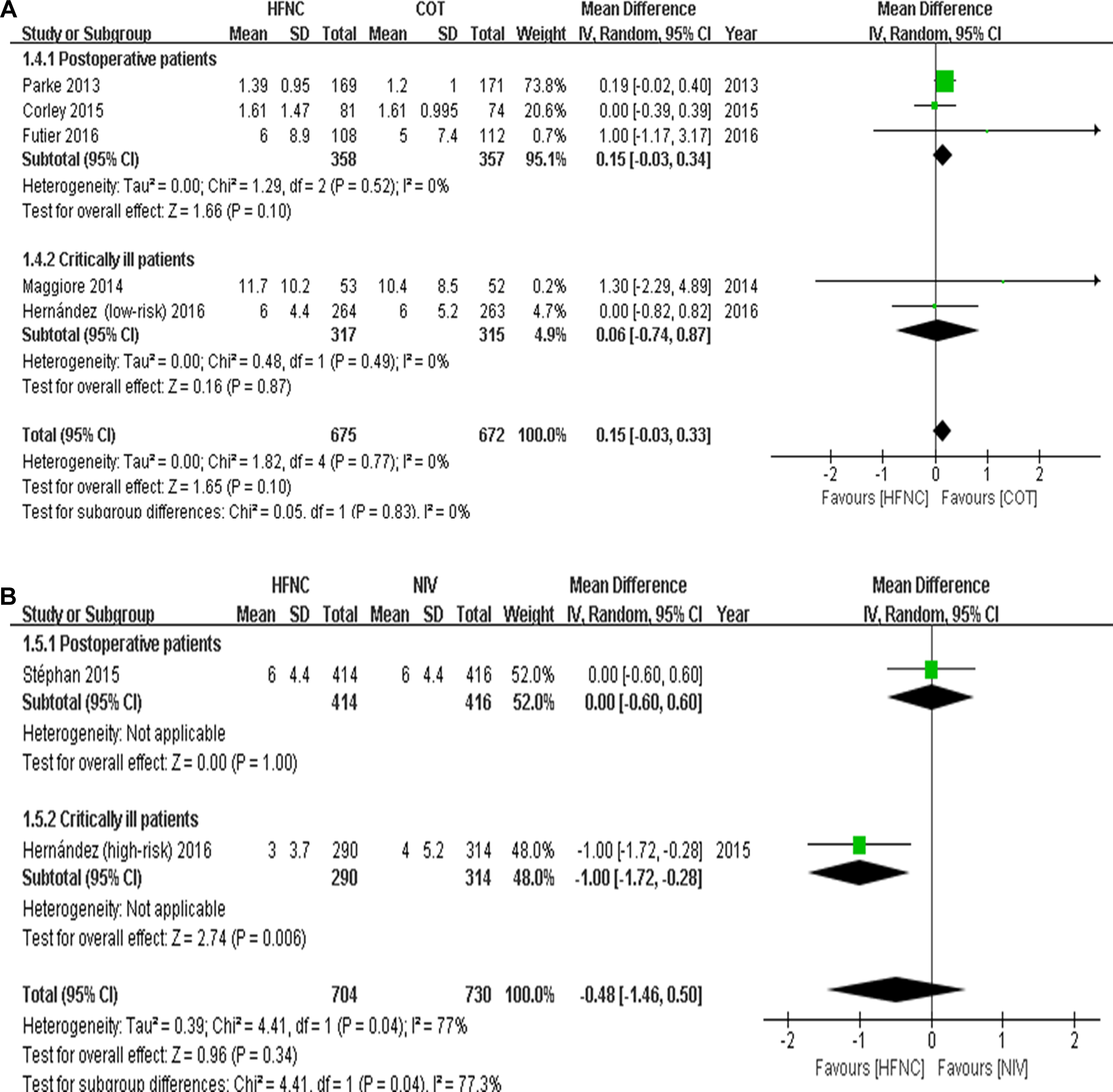
Forest plot comparing the intensive care unit (ICU) length of stay in high-flow nasal cannula (HFNC) versus conventional oxygen therapy (COT; A) and in HFNC versus noninvasive ventilation (NIV; B).
For hospital LOS (Figure 7), there was no significant difference in HFNC versus COT (P = .23), 64,66,70 while a trend to decreased hospital LOS was suggested in HFNC versus NIV (n = 1434; I 2 = 23%; P = .08; MD, −1.42 days; 95% CI, −3.01 to +0.18 days). 65,67 The overall pooled results between subgroups were not statistically different (interaction P = 0.11 [HFNC vs COT] and 0.26 [HFNC vs NIV]). Mortality (ICU and/or hospital) was reported by a limited number of RCTs and was similar regardless of comparison (Figures 8 and 9).
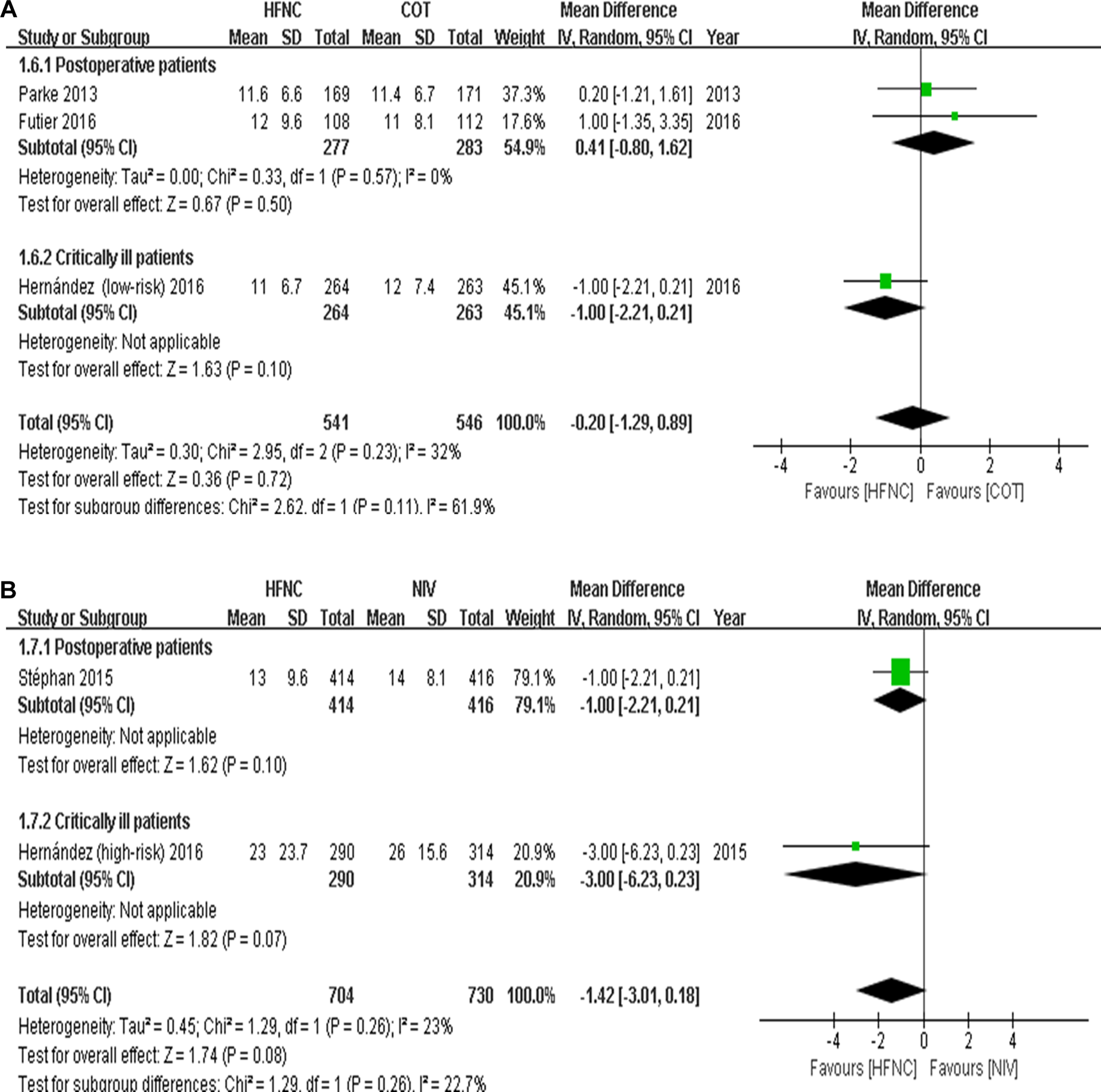
Forest plot comparing the hospital length of stay in high-flow nasal cannula (HFNC) versus conventional oxygen therapy (COT; A) and in HFNC versus noninvasive ventilation (NIV; B).
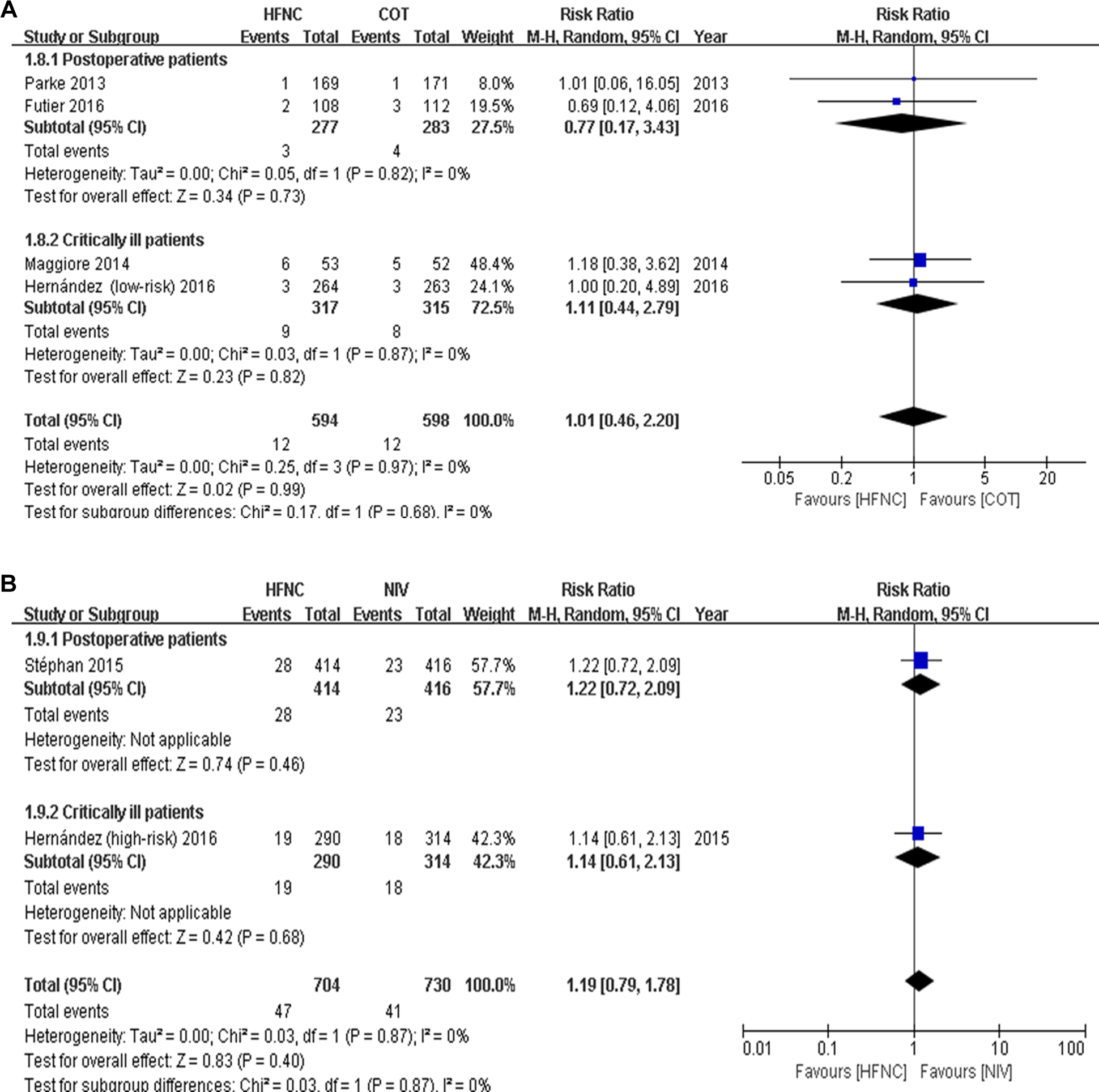
Forest plot comparing the intensive care unit (ICU) mortality in high-flow nasal cannula (HFNC) versus conventional oxygen therapy (COT; A) and in HFNC versus noninvasive ventilation (NIV; B).
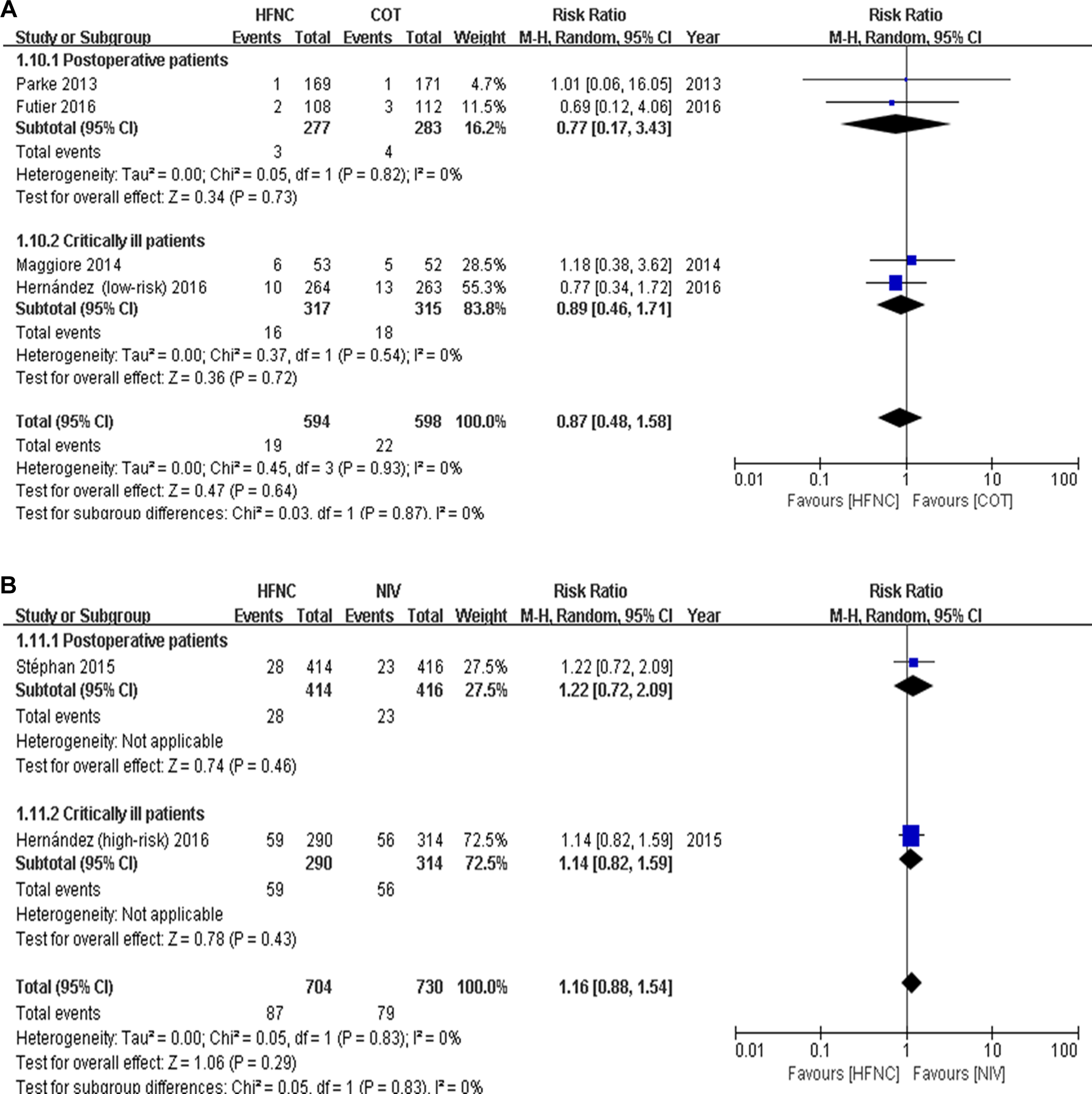
Forest plot comparing the hospital mortality in high-flow nasal cannula (HFNC) versus conventional oxygen therapy (COT; A) and in HFNC versus noninvasive ventilation (NIV; B).
Discussion
The present systematic review and meta-analysis specifically focused on the effect of HFNC on reintubation in adult patients after extubation and yielded 3 major findings. First, compared to COT, HFNC may reduce reintubation (or reintubation plus NIV) rates in critically ill patients but not in postoperative patients. Second, while HFNC demonstrates similar reintubation rate compared to NIV, HFNC results potentially in less complications and better patient tolerance and comfort. Third, limited available RCT data suggest that HFNC does not increase the risk of delayed reintubation.
Theoretically, HFNC may favor successful extubation in several ways, including generation of flow-dependent positive end-expiratory pressure, delivery of a more reliable inspired oxygen concentration, and more efficient humidification and heating. 60,63,71 –77 However, given the additional equipment and staff resources required, one would like to be able to identify which patients are most likely to benefit from this technique after extubation. The 5 RCTs comparing HFNC with COT were stratified as postoperative (either cardiothoracic 68,70 or major abdominal 64 ) and critically ill. 66,69 Patients undergoing intrathoracic or abdominal surgery were pooled because both are at risk of postoperative pulmonary complications. 78 –80 In addition, a meta-analysis by Neto et al suggested that the total incidence of postoperative lung injury was similar for abdominal and thoracic surgery (3.4% versus 4.3%, P = .2). 79 In all postoperative trials, durations of mechanical ventilation were short, and reintubation rates were very low (0%-3.5%; Table 1), suggesting minimal opportunity for further improvement in reintubation. In contrast, the 2 RCTs enrolling critically ill patients had higher control group reintubation rates (12% 66 and 21% 69 ), and the application of HFNC postextubation significantly reduced reintubation when compared to COT. Our analysis suggested that, for postoperative patients without ARF receiving short-term mechanical ventilation, COT might still be the first-line oxygen therapy strategy after extubation, whereas for critically ill patients who were mechanically ventilated due to ARF for a relatively longer time prior to extubation and at higher risk of reintubation, HFNC might be a potential alternative to COT. Future studies should focus more on patient populations, including postoperative patients, at higher risk of reintubation.
Studies have suggested that prophylactic NIV appear ineffective in low-risk patients, 81 whereas other investigations in high-risk patients show that the use of NIV could avoid reintubation and improve outcomes. 6,7,10,82 However, the major obstacle in the application of NIV lies in patient tolerance and staff workload. 8 –11 The HFNC may address some of these issues. In the 2 included trials in the present analysis, HFNC was compared to NIV by the noninferiority design in critically ill 65 or cardiothoracic surgery 67 patients at high-risk of extubation failure. Our pooled results showed that HFNC was similar to NIV for preventing extubation failure, which suggests that HFNC could be used as an alternative respiratory support to NIV in high-risk patients. The potential advantages of HFNC over NIV include fewer complications and better tolerance and comfort. However, complications and tolerance were not reported uniformly in these studies. 65,67 These are also important topics for the future confirmatory studies.
One safety concern relating to the use of HFNC after extubation is the possibility of reintubation delay. One retrospective study suggested that failure of HFNC might result in delayed intubation and worse outcomes in patients with ARF. 33 Similar concerns have arisen in an RCT, where patients were randomized to NIV for respiratory failure after extubation that yielded similar but delayed reintubation rates and higher mortality in the NIV group. 83 Only 2 of our included RCTs (by the same research team) reported reintubation time. 65,66 Although a similar time to reintubation was found in these studies (in either HFNC vs COT or HFNC vs NIV), this outcome variable should continue to be monitored in future investigations. To minimize these potential risks, close monitoring and prespecified strict reintubation criteria may help detect HFNC failure in a timely manner. In a recent study by Roca et al, 84 an easy-to-use ROX index, defined as the ratio of pulse oximetry/fraction of inspired oxygen to respiratory rate, could identify patients at low risk of HFNC failure. In order to avoid delayed reintubation, early predictors of HFNC failure need to be further explored.
This is the first meta-analysis to focus exclusively on the use of HFNC after extubation in adult patient populations. Six meta-analyses examining the use of HFNC in adult patients have been published recently, with inconsistent conclusions. 20 –25 Four meta-analyses suggested no differences in intubation or mortality in patients treated with HFNC compared to those treated with usual care (COT or NIV). 20 –23 In contrast, 2 others showed that compared to COT, HFNC was associated with a lower rate of endotracheal intubation. 24,25 The merging of indications for HFNC (primary ARF and postextubation) and comparators (COT and NIV) might have contributed to these inconsistent results. 20 –25 Five of these meta-analyses included a mixture of RCTs evaluating the use of HFNC in patients with ARF postextubation. 20 –22,24,25 The sixth 23 did focus on postextubation but only in patients after cardiac surgery and only comparing HFNC to COT so that this meta-analysis included only 2 RCTs. 68,70 Our meta-analysis included all relevant RCTs included in these previous meta-analyses as well as 2 or more additional RCTs compared to each of the other meta-analyses. In addition to focusing on the use of HFNC after extubation and including a larger number of RCTs, other strengths of the present analysis are the separate comparison of HFNC with COT only or NIV only, and the subgroup analysis in different patient populations. Although the required information size was not reached in the present meta-analysis to give definitive conclusions, our results allowed us to identify specific comparisons and patient populations where HFNC may be beneficial (namely, compared to COT in critically ill patients who were mechanically ventilated due to ARF for a relatively longer time prior to extubation, with a higher risk of reintubation) and guide further study direction to confirm and further refine these findings.
Our study also has limitations. The main limitation is the small number of included RCTs making it difficult to reach definitive conclusions, particularly when these are based on subgroups each containing very few RCTs. This is aggravated by inevitable variations in the inclusion criteria, interventions, and end point definitions among the included RCTs contributing to heterogeneity. In addition, we were unable to conduct an adequate stratified analysis on the patients with different body mass indexes and between medical and surgical patients, as our planned protocol, because of limited relevant data.
Conclusion
This systematic review and meta-analysis of RCTs in adult patients after extubation suggests that COT may still be the first-line postextubation management in postoperative patients without ARF, but HFNC may provide benefit to avoid reintubation in critically ill patients with ARF under relatively longer duration of mechanical ventilation. The HFNC is not inferior to NIV in patients with risks of extubation failure, but HFNC exhibits fewer complications and is better tolerated. However, required information size was not reached, so further high-quality studies are required to confirm these results. The results of this study suggest that future studies examining reintubation should focus on critically ill patients with higher risks of extubation failure.
Footnotes
Authors’ Note
Hua-Wei Huang and Xiu-Mei Sun contributed equally to this article. H.W.H., X.M.S., and J.X.Z. contributed to study design and study conduct; H.W.H., X.M.S., Z.H.S., and G.Q.C. contributed to data analysis; H.W.H., X.M.S., Z.H.S., G.Q.C., L.C., J.O.F., and J.X.Z. contributed to data interpretation; H.W.H., X.M.S., L.C., J.O.F., and J.X.Z. contributed to writing and revising the paper. All authors read and approve the final manuscript. Jan Friedrich holds a Clinician Scientist Award from the Canadian Institutes of Health Research. The sponsors had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grant from the Beijing Municipal Administration of Hospital (ZYLX201502).