
Abstract
Background:
Acupuncture treatment has been employed in China for over 2500 years and it is used worldwide as analgesia in acute and chronic pain. Acupuncture is also used in general anesthesia (GA). The aim of this systematic review and meta-analysis was to assess the efficacy of electroacupuncture (EA) in addition to GA in patients undergoing cardiac surgery.
Methods:
We searched 3 databases (Pubmed, Cochrane Library, and Web of Science—from 1965 until January 31, 2017) for randomized controlled trials (RCTs) including patients undergoing cardiac surgery and receiving GA alone or GA + EA. As primary outcomes, we investigated the association between GA + EA approach and the dosage of intraoperative anesthetic drugs administered, the duration of mechanical ventilation (MV), the postoperative dose of vasoactive drugs, the length of intensive care unit (ICU) and hospital stay, and the levels of troponin I and cytokines.
Results:
The initial search yielded 477 citations, but only 7 prospective RCTs enrolling a total of 321 patients were included. The use of GA + EA reduced the dosage of intraoperative anesthetic drugs (P < .05), leading to shorter MV time (P < .01) and ICU stay (P < .05) as well as reduced postoperative dose of vasoactive drugs (P < .001). In addition, significantly lower levels of troponin I (P < .01) and tumor necrosis factor α (P < .01) were observed.
Conclusion:
The complementary use of EA for open-heart surgery reduces the duration of MV and ICU stay, blunts the inflammatory response, and might have protective effects on the heart. Our findings stimulate future RCT to provide definitive recommendations.
Keywords
Introduction
Acupuncture consists of stimulation of specific points on or below the skin and it has been part of traditional Chinese medicine (TCM) for about 2500 years. 1 First knowledge of acupuncture was brought to Europe over 400 years ago. 2 The interest in these techniques has gradually increased in the last 3 centuries but relevant clinical research started as late as the 1980s. Ever since the effectiveness of acupuncture has been controversially discussed in the medical field. Several studies showed that acupuncture is an effective analgesic method on an array of origins of pain, for example, migraine 3 or lower back pain. 4,5 Acupuncture is also successfully used to ease postoperative pain 6 and postoperative nausea and vomiting (PONV). 6 –8 The stimulation of auricular acupuncture points was effective in decreasing anesthetic requirements in volunteers. 9 Furthermore, Han showed the effectiveness of acupuncture in addition to the standard anesthetic techniques. 10
As recently discussed, the reported therapeutic efficacy of acupuncture leads inevitably to the search for a physiological explanation. 8 Pioneer investigations of the physiology of (electro)acupuncture (EA) and the responses of biological mediators and transmitters were conducted in the late 1970s and early 1980s. 11 In particular, mediators of the opioid group like β-endorphins, enkephalins, and dynorphins are involved. 12 –15 Different frequencies used during transdermal electrical acupoint stimulation (EA) result in different physiologic reactions. Low-frequency (2 Hz) stimulation increases the release of β-endorphins, methionine, and enkephalin in both the brain and spinal cord, resulting in the induction of analgesia by binding to µ, ∂ and/or κ receptors, whereas EA with a high-frequency stimulation (100 Hz) augments the release of dynorphins solely in the spinal cord, and analgesia is mediated via κ opioid receptors. 12 –15
In addition to the opioid peptides, diverse signal molecules contribute to mediating acupuncture analgesia.
16
Important messengers are glutamate (N-methyl-
The perception of pain is mainly an interpretation and further processing of signaling in the brain. Identifying the influence of acupuncture stimulation—or any other kind of analgesic method—on the functional level of brain is of relevance in patients undergoing general anesthesia (GA).
Animal studies have shown that acupuncture could mimic ischemic preconditioning and reduce ischemic–reperfusion injury following cardiac surgery. 18,19 Significant improvement in cardiac function and myocardial remodeling of chronic heart failure was also shown. 20
We conducted a systematic review and meta-analysis to evaluate the efficacy of EA in addition to GA in patients undergoing cardiac surgery. We hypothesized that addition of EA during heart surgery showed beneficial effects reducing the intraoperative need for anesthetic drugs, speeding up postoperative recovery, and positively influencing inflammatory and cardiac markers at 24 hours postoperatively.
Materials and Methods
We conducted a systematic Web-based literature search using Medline (PubMed), Web of Science, and Cochrane Library. The “PRISMA 2009 checklist” for systematic reviews and meta-analysis was used (www.prisma-statement.org), which was based on the work of Moher and colleagues. 21 Our search algorithms were (1) acupuncture AND heart surgery and (2) acupuncture AND cardiac surgery. The full query translations are provided as online supplement. There was no language restriction criteria for study inclusion.
Literature was graded and discussed by all authors, taking into account the available evidence published between 1965 and January 31, 2017. Studies were included in the meta-analysis if open-heart surgery was involved, and the outcomes in patients anesthetized with GA only versus those anesthetized with a combination of GA and EA (Figure 1) were compared. Exclusion criteria were no acupuncture during surgery, no GA during surgery, only postoperative data available, animal studies, case reports, and case series.
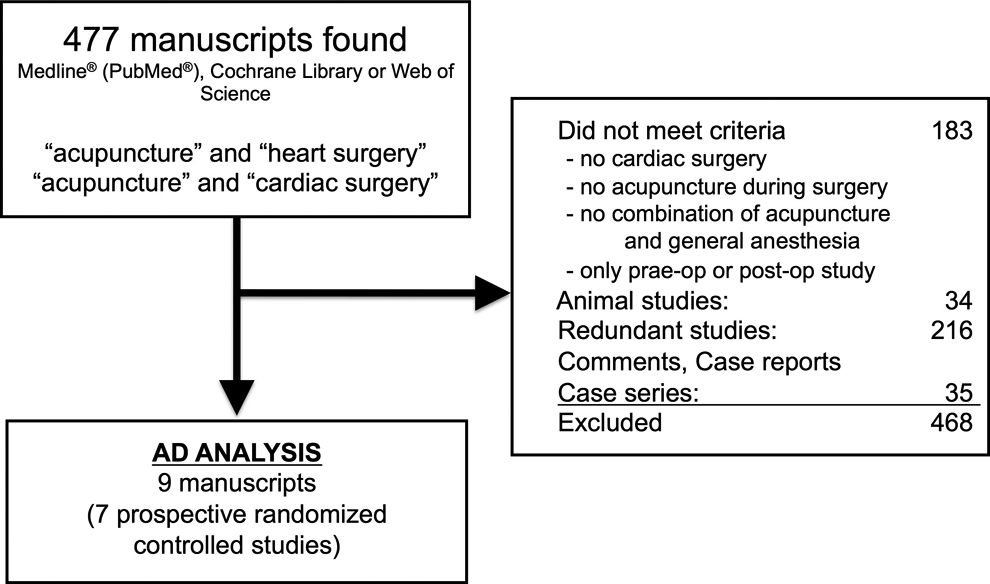
Flowchart of inclusion of studies.
For grading and assessment of the methodological quality of the studies, the 2011 recommendations of the Oxford Centre for Evidence Based Medicine were used. 22
Odds ratio or standardized mean difference was calculated from raw results, group means, standard errors, or values that were extracted from presented figures. We used for analysis the exact p values (eg, p = 0.027) when available in the articles, otherwise the presented standard deviation and n. The analysis was performed with the statistics program CMA for Windows (Biostat Inc, Englewood, New Jersey, USA). The results represent event rates, odds ratios, or the standardized difference of means (SDM)/Hedges g between GA and GA + EA. For all meta-analysis calculations, the random effect model was used. A P value <.05 was considered statistically significant.
Where different postoperative time points were presented, we used the time point 24 hours post surgery for our analysis (eg, troponin, inflammatory mediators).
The risk of bias for this meta-analysis was assessed according to the guidelines of The Cochrane Collaboration’s tool. 23
Results
The literature search with the 2 above-mentioned algorithms reflected a total of 477 publications, of which 468 were excluded.
The most common exclusion criteria were redundancy (n = 216), another 183 studies did not meet the target criteria, while 34 were excluded because they were animal studies. Thirty-five studies were case reports, comments, or case series that were rated as Level 5 evidence and therefore excluded from the meta-analysis.
The remaining 9 articles 24 –32 that met the search criteria were published between 2001 and 2016. Results of 3 articles 29 –31 had identical n as well as demographics, and hence the 3 articles were therefore considered as a single randomized controlled trial (RCT) for this meta-analysis. All 7 studies included were prospective RCTs, with a total of 321 patients, which were graded as Level 2 evidence, as shown in Table 1.
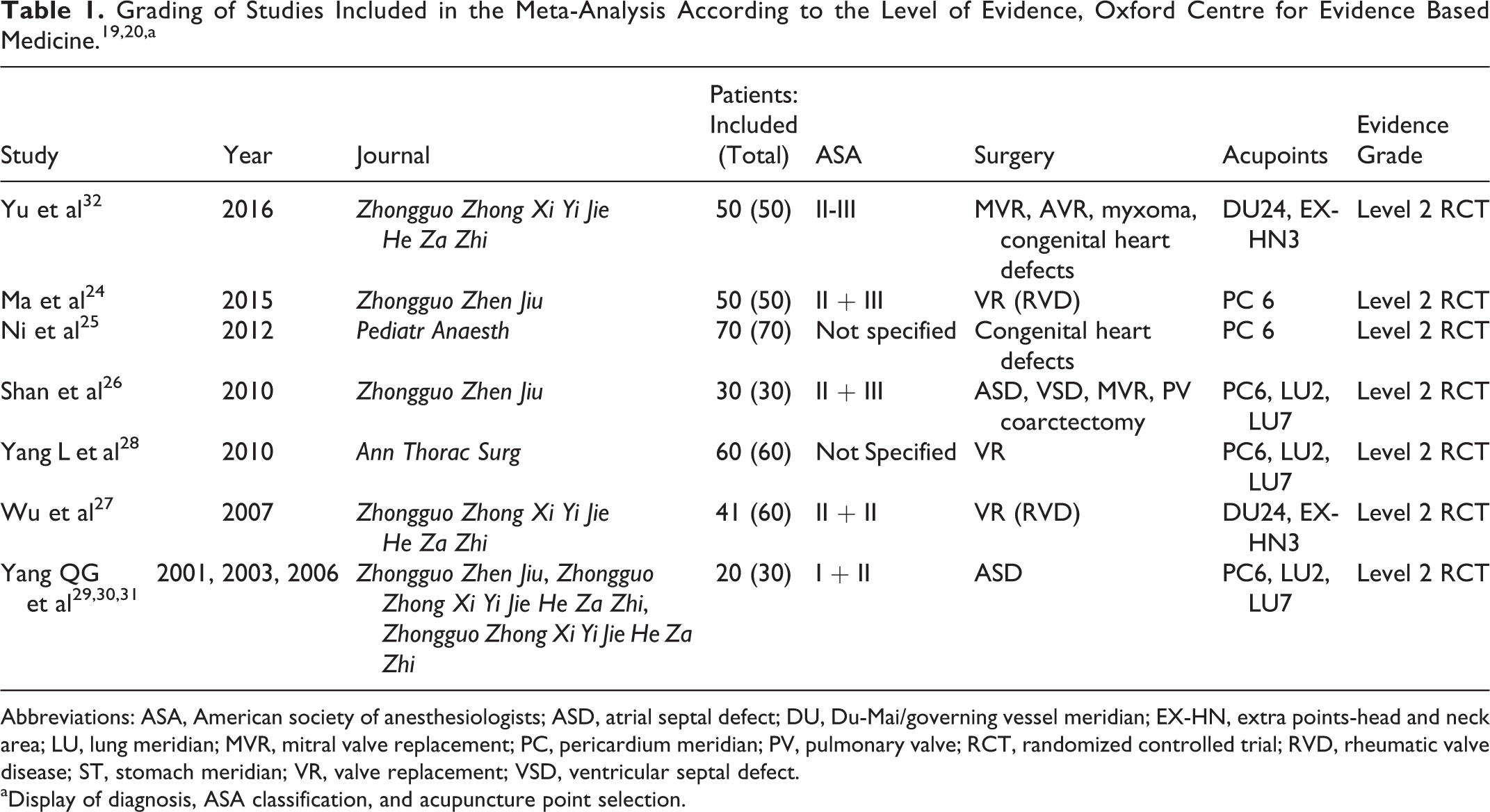
Abbreviations: ASA, American society of anesthesiologists; ASD, atrial septal defect; DU, Du-Mai/governing vessel meridian; EX-HN, extra points-head and neck area; LU, lung meridian; MVR, mitral valve replacement; PC, pericardium meridian; PV, pulmonary valve; RCT, randomized controlled trial; RVD, rheumatic valve disease; ST, stomach meridian; VR, valve replacement; VSD, ventricular septal defect.
aDisplay of diagnosis, ASA classification, and acupuncture point selection.
Several clinical questions were studied. Five RCTs investigated the duration of mechanical ventilation (MV), 25 –28,32 4 presented data according to the intraoperative use of anesthetic drugs. 25,27,28,32 In 3 studies, 25,28,32 the length of stay in the intensive care unit (ICU), and in 2 studies, 25,28 the length of stay in the hospital, were investigated. Three RCTs 24,25,28 presented data for troponin I levels and the use of vasoactive and inotropic drugs. Measurements were taken at different postoperative time points. The dosage of vasoactive drugs were presented using different types of data and was therefore difficult to analyze. Ma et al presented the actual levels of dopamine, 24 whereas Ni et al 25 presented the data on the number of patients who needed any kind of inotropic or vasopressor support. A completely new approach was presented by Yang et al, 28 by introducing an inotrope score (IS) to achieve a weighted evaluation of the vasoactive drug usage (IS in [µg/(kg min)] = dopamine *1 + dobutamine *1 + amrinone *1 + milrinone *15 + epinephrine *100 + norepinephrine *100 + isoprenaline *100). 28
In addition to postoperative troponin I, the postoperative values of proinflammatory (interleukin 2 [IL-2], IL-6, and tumor necrosis factor α [TNF-α]) and anti-inflammatory (IL-10) cytokines were presented at different time points after surgery, which are based on the RCTs. 25,26,29 –31
Six of the 7 studies included in our meta-analysis compared 2 groups: a control group using GA only and a group with additional EA (GA + EA). 24 –28,32 The trial, which presented results in three articles compared 3 groups, GA. The group receiving solely EA was therefore excluded. Another RCT compared 3 groups, GA group, GA + EA group, and GA combined with acupuncture without electrical stimulation (GA + A). This GA + A group was excluded from meta-analysis due to missing electrical stimulation.
In these published studies, acupuncture points were selected according to the system of meridians in TCM. All studies used a minimum of 1 to a maximum of 3 acupuncture points (Table 1), and the acupuncture points were accessed bilaterally where applicable. Needles were placed at the acupoint location and were connected to a HANS EA stimulator 26,27 (model LH202H; Huawei Industrial Development Company, Beijing, China), an Hwato electrical acupoint stimulator (models SDZ-II 28 SDZ-IV 32 or SDZ-V 25 ; Suzhou Medical Instruments Co Ltd, Suzhou, China), or G6805 electrical acupoint stimulator 29 –31 (Shanghai Medical Devices, Shanghai, China). In 1 study, transcutaneous pre-gelled silver–silver chloride electrodes 25 (diameter 1.5 cm) were used instead of needles. Yang et al 28 positioned needles in control group at the same acupoints as in GA + EA but lacking any kind of stimulation.
The electric stimulation was initiated prior to GA induction on the awake patients and was maintained for 20 minutes, 29 –31 30 minutes, 24 –28 or was continued twice daily for 30 minutes in the ICU until discharge to regular ward. 32 The points received either alternating electrical stimulation of 2 Hz/100 Hz, 24,26,27 5 Hz/30 Hz, 28 2 Hz, 25 or 5 Hz 32 disperse/dense wave or 3 to 4 Hz biphasic waves. 29 –31 Stimulus intensity was set according to patient tolerance levels (eg, 8-12 mA 24 and 10-15 mA 29 –31 ).
Following the preparations for acupuncture, patients received standard intravenous GA induction 24,26 followed by either total intravenous anesthesia 24,27 or balanced GA with sevoflurane. 25
The other RCT had no specifications with regard to either GA induction or GA maintenance. One study 24 included only pediatric patients, whereas the other 6 RCTs 26 –32 focused on adult patients.
The analysis of anesthetic drugs revealed a significantly decreased need for sedatives (propofol, midazolam, or dexmedetomidine; SDM 0.730, CI 95%, 0.113-1.347, P = .020; Figure 2), whereas the dosage of opioids (fentanyl or morphine) showed a lower dosage trend with no significance (P = .074).
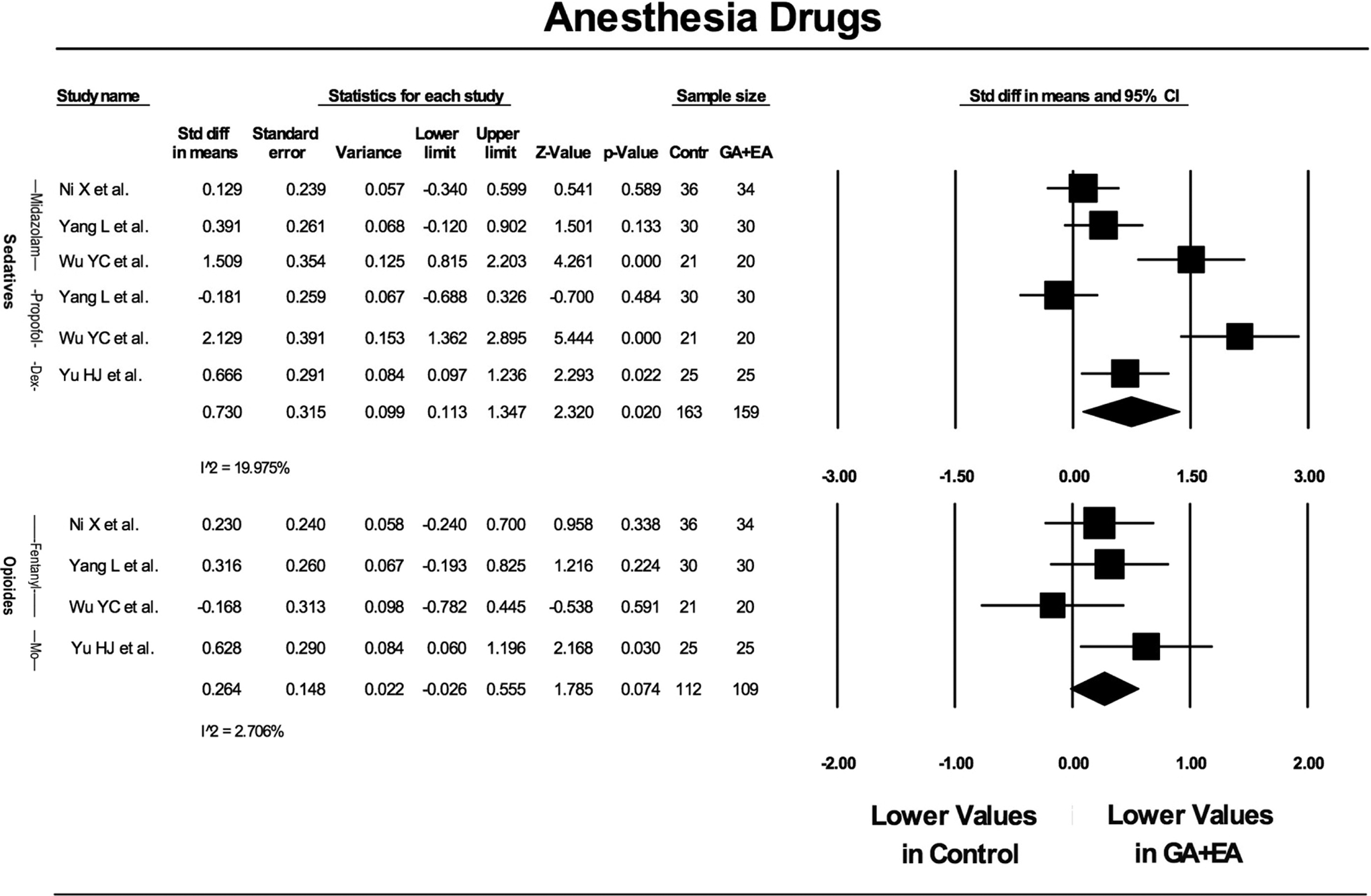
Meta-analysis of anesthesia drugs.
The duration of MV was significantly shorter (hours, minutes) in the GA + EA group compared to GA alone (SDM 0.381, CI 95%, 0. 130-0.631, P = 0.003; Figure 3).
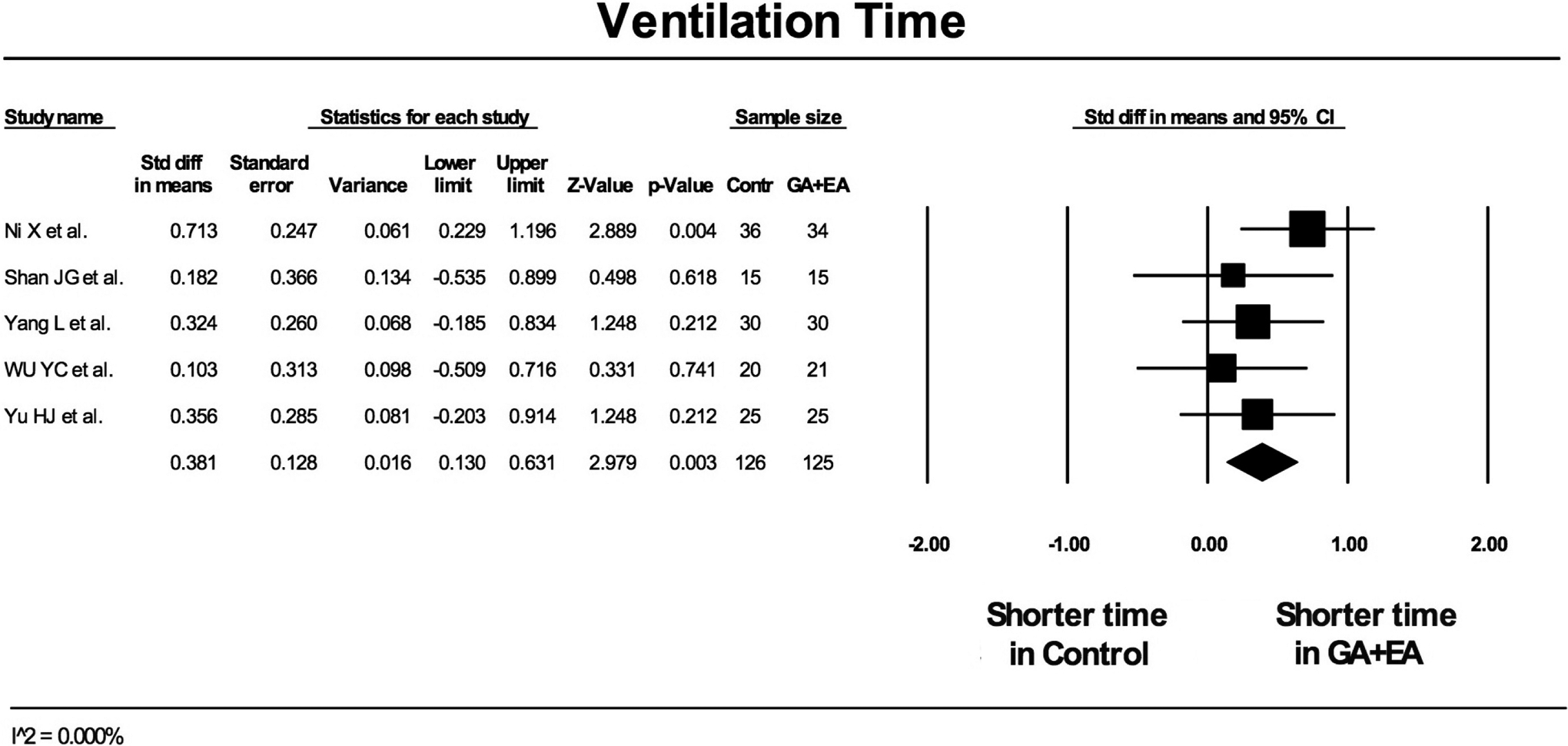
Meta-analysis of ventilation time in cardiac surgery.
During ICU stay, the required dosage of inotropic and vasoactive drugs was significantly lower in the GA + EA group than in the GA-alone group (SDM 0.952, CI 95%, 0.426-1.477, P < .001; Figure 4). The levels of troponin I were significantly lower at 24 hours postoperatively in GA + EA as compared to GA alone (SDM 0.761, CI 95%, 0.259-1.262, P = .003; Figure 5).
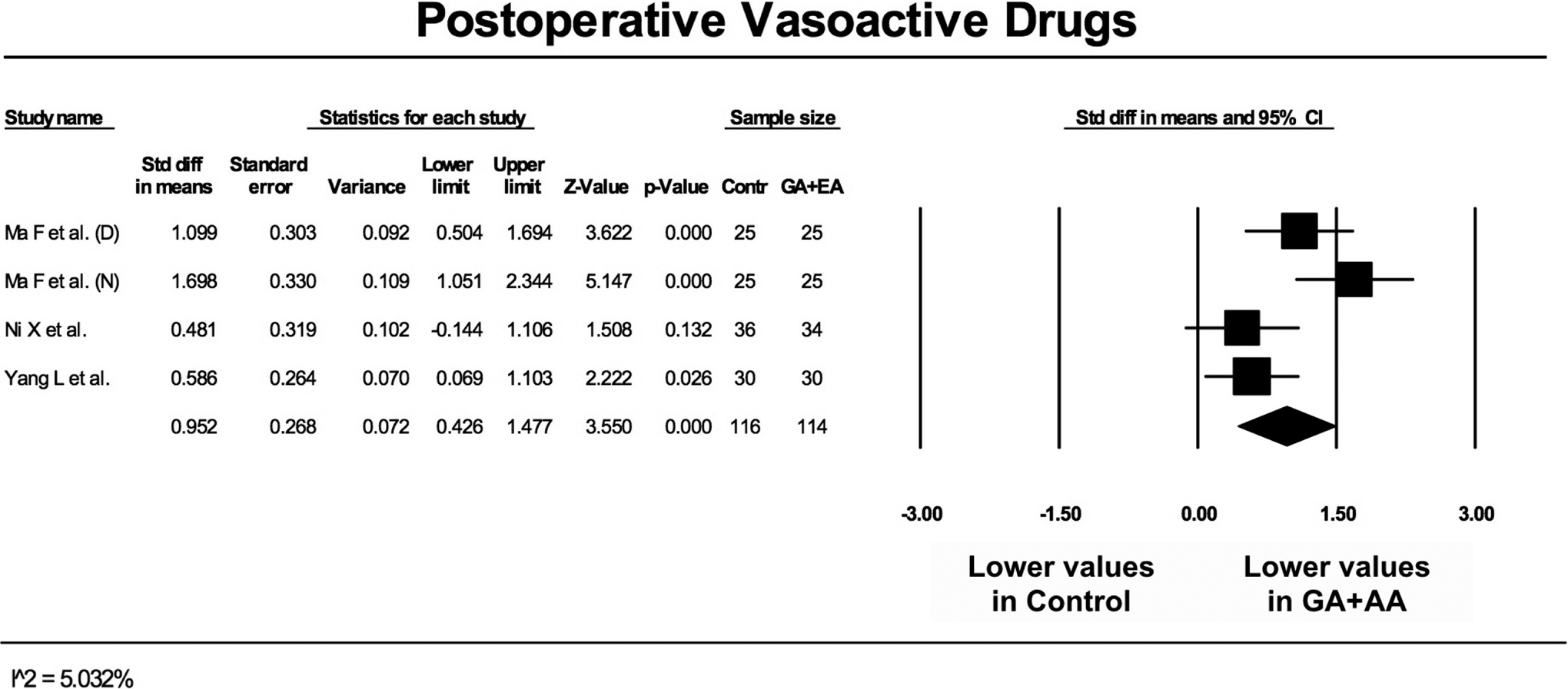
Meta-analysis of postoperative vasoactive drugs (D = Dopamine, N = Norepinephrine).
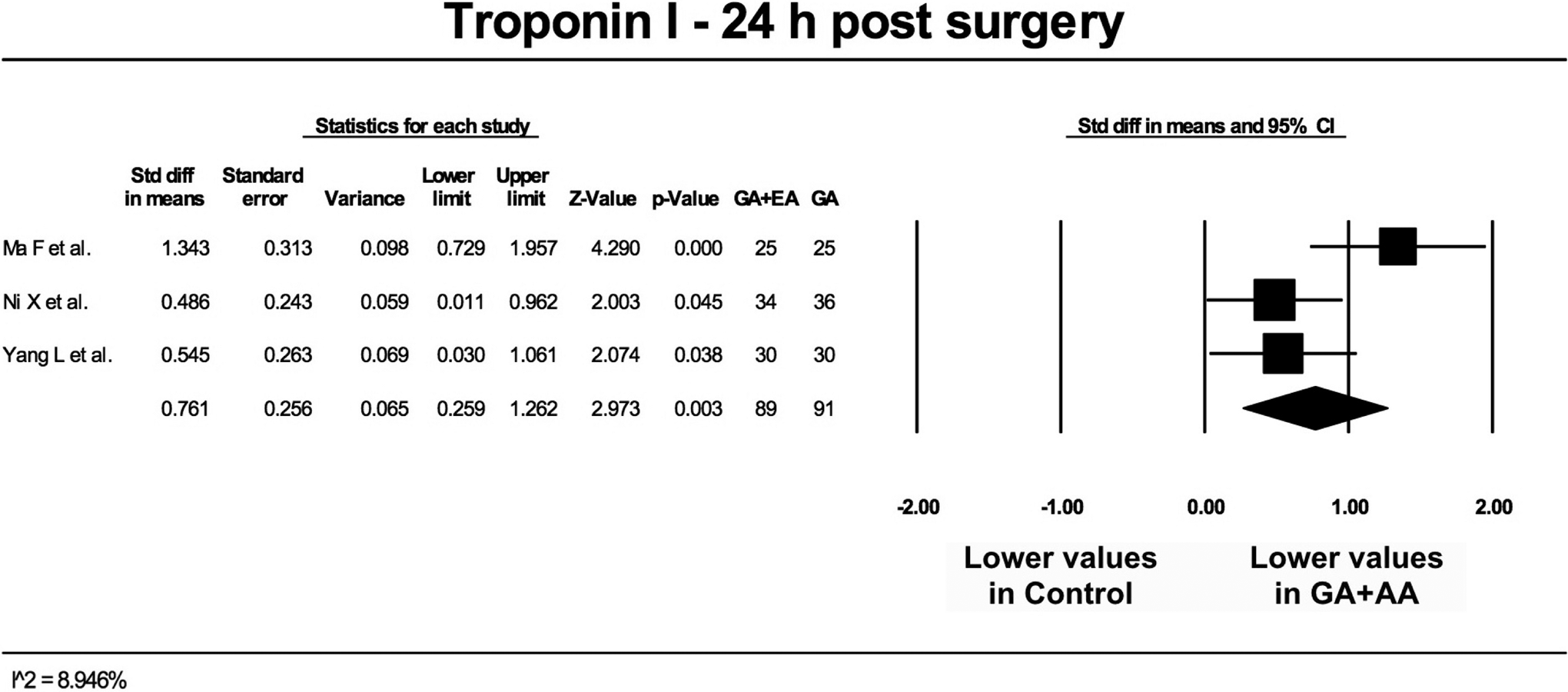
Meta-analysis of cardiac troponin I 24 hours poststernotomy.
The use of EA in addition to GA led to an earlier discharge to the ward from the ICU (SDM 0.384, CI 95%, 0.084-0.685, P = .012; Figure 6), whereas no difference was noted in the duration of hospital stay (P = .176).
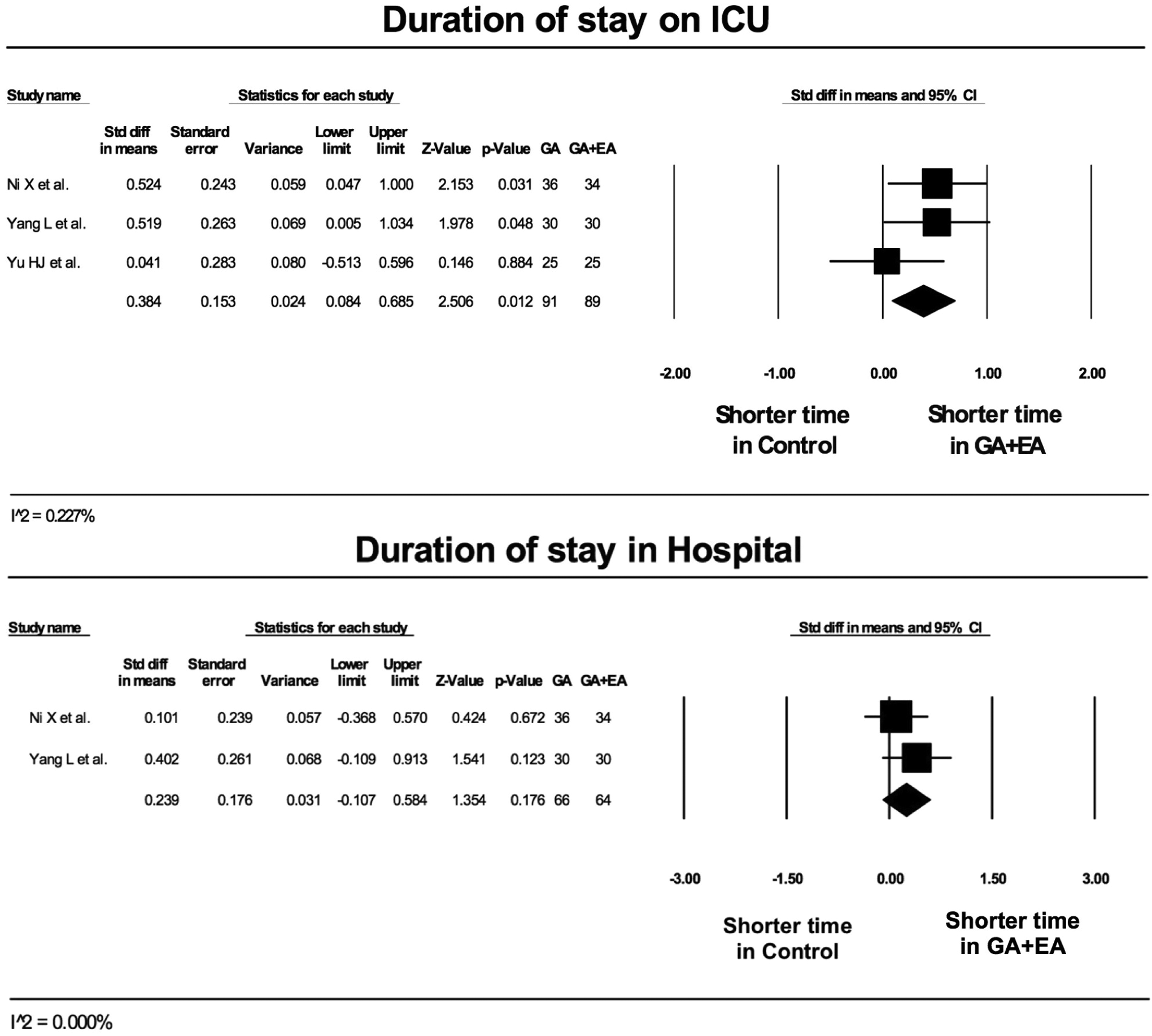
Meta-analysis of duration of stay on intensive care unit and in hospital.
The proinflammatory cytokines IL-6 (P = .440) and TNF-α were lower in GA + EA than in GA, but only TNF-α reached significant levels (SDM 0.753, CI 95%, 0.197-1.309, P = .003). On the other side, IL-2 (SDM −1.674, CI 95%, −2.321 to −1.027, P < .001) and the anti-inflammatory IL-10 (SDM 0.442, CI 95%, −1.760 to −0.026, P = .044) were significantly lower in the GA group than in GA + EA (Figure 7).
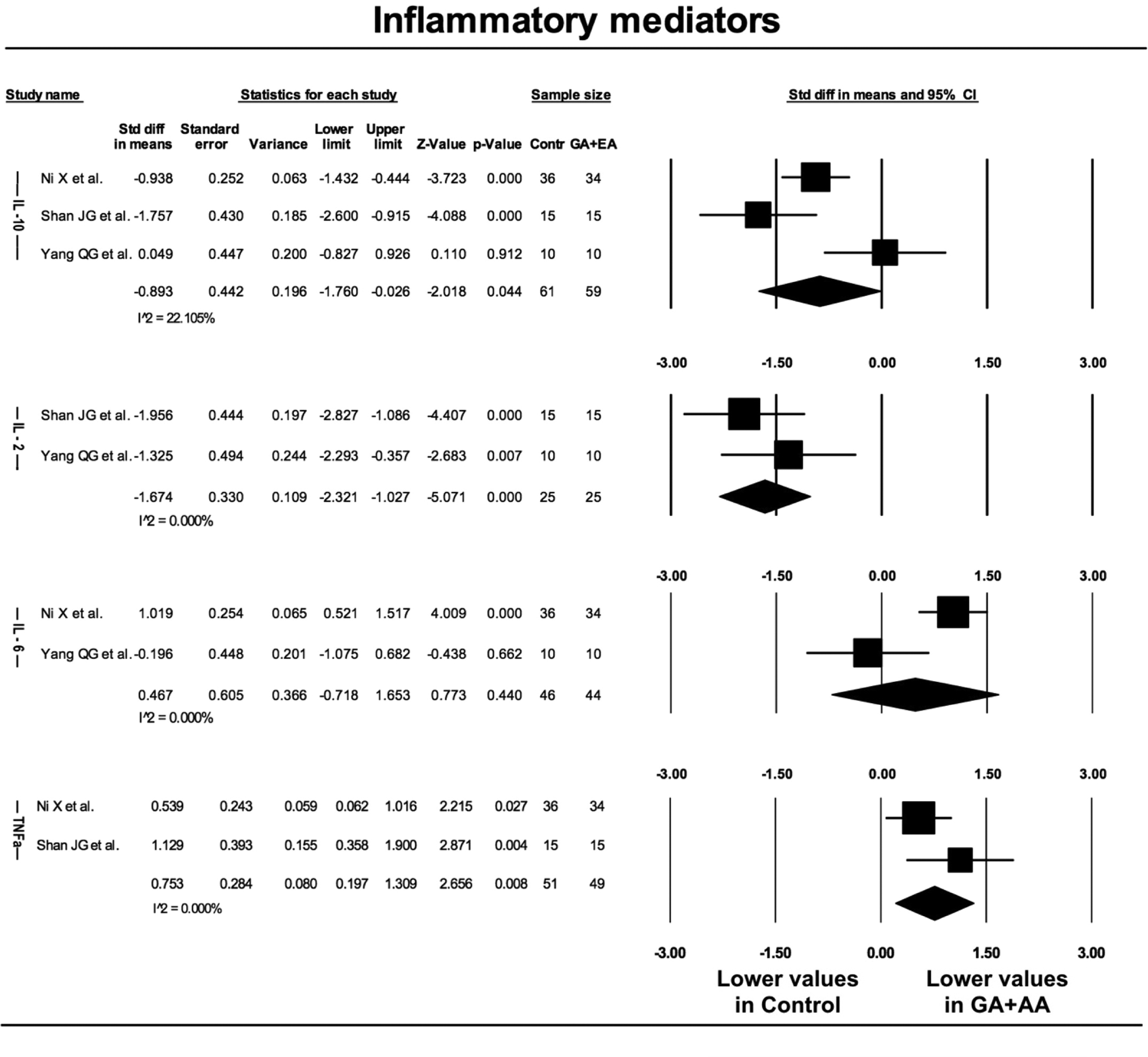
Meta-analysis of the inflammatory mediators IL-10, IL-2, IL-6, TNFa. (IL = Interleukine, TNFa = Tumor necrosis factor alpha).
The depth effects on anesthesia were presented as bispectral index (BIS). The studies stated either the maintenance of a certain BIS (40-60) at all times during GA or that no complications occurred. 28 No significant differences between groups were observed.
Assessment (Figure 8) showed low risk for selection bias (randomization) and attrition bias. Reporting bias was found for the three oldest included articles 29 –31 as they present the same data. In a few studies, the risk for allocation concealment may be a problem. The risk for performance and detection bias is unclear due to insufficient information on the study protocol.
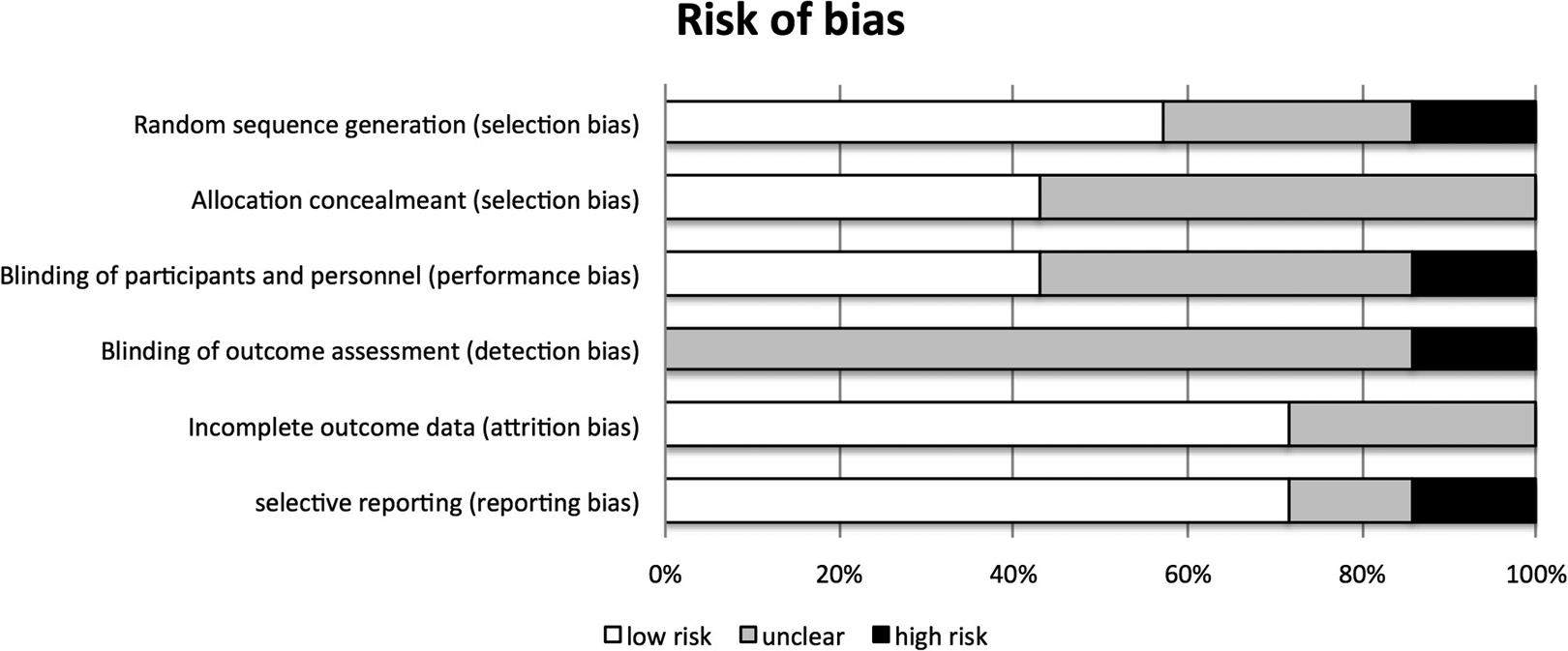
Risk of bias assessment.
Discussion
This study is the first systematic review of the literature and subsequent meta-analysis inspecting the additive effects of EA when combined with GA in patients undergoing open-heart surgery. Seven prospective RCTs with Level 2 evidence were included, with a total of 321 patients.
The main findings of our study confirm the initial hypothesis of multiple beneficial effects of EA when associated with GA in patients undergoing open-heart surgery. In particular, the GA + EA approach was associated with reduced intraoperative need for anesthetic drugs, which led to significantly shorter MV time and stay in ICU as well as lower levels of proinflammatory mediators. Furthermore, patients administered with GA + EA needed significantly less vasoactive drugs postoperatively, and the intraoperative myocardial cell damage was significantly reduced as compared to GA only, as indicated by lower cardiac troponin I blood levels 24 hours after surgery. In this meta-analysis, we point out potential beneficial effects of assisted EA complementary to GA. The results are consistent with publications of lower levels of evidence such as case reports, case series, and animal studies in the field of cardiac surgery. 20,33 The results of animal studies should be interpreted with caution, especially as a different response of opioid receptors following EA has been demonstrated in healthy animals versus animals receiving a painful stimuli. 15 To elucidate the general influence of acupuncture, Ren et al 34 examined the brain of 12 healthy volunteers in a functional magnetic resonance imaging during acupuncture application. The volunteers received EA stimulation on classical acupuncture points according to TCM (verum points) versus stimulation of nonacupuncture points (sham points). The results show higher brain region activation from classical acupuncture point stimulation compared to the shams.
The important result of a reduced intraoperative amount of anesthetic drugs in patients undergoing heart surgery is supported by similar results in other types of surgery. Patients undergoing short-time surgeries (30-120 minutes) were investigated by Gemma and colleagues. 35 Assisted acupuncture (AA) + GA group showed significantly deeper anesthetic levels measured using BIS, with the same dosage of sedative and analgesic drugs as in GA and SA + GA groups. According to RCTs by An et al 36 –38 and Wang et al, 39 in neurosurgical patients required a lower dosage of volatile anesthetic to maintain the same depth of anesthesia (BIS < 50) in AA + GA versus GA.
These observations for reduced need for additional analgesics concur with orthopedic and neurosurgery patients, and surgeries under AA and analgosedation, but not receiving GA.
In the postoperative phase, patients in the EA + GA group required significantly lower dosage of vasoactive drugs, and this probably contributed to a shorter ICU stay, although the overall stay in hospital was not different. The EA + GA approach was associated with reduced damage of perioperative myocardial tissue as shown by significantly lower troponin I levels, which may have contributed to the lower dosage of vasoactive drugs and shorter ICU stay. Several animal models confirmed a cardioprotective effect of EA after myocardial infarction and reperfusion injury. 40 –42 Even an improvement in remodeling and cardiac function through EA has been shown in a rat model with chronic heart failure. 20 By analyzing the dialysate of rats after EA, Redington et al 41 demonstrated that EA stimulation releases cardioprotective factors into the bloodstream. The retransfusion of such dialysate had protective effect toward reperfusion injury in rats with limb ischemia which is achieved by significantly reducing the infarct size and improving the functional recovery. The specific mechanisms are not yet completely understood, and the types of cardioprotective factors described by Redington and colleagues are also unknown. Nevertheless, it was discovered that in myocardial protection significant roles are played by beta-adrenoceptors and the cardiac sympathetic nervous system, and opioid pathways and protein kinase C (PKC)-dependent pathways are also involved. The blockade of the opioid and PKC pathways with naloxone and the nonselective PKC inhibitor chelerythrine led to a complete loss of the cardioprotective effect following the drug administration. 42 Abolishment of the cardioprotective effect of EA pretreatment prior to myocardial injury could be shown by application of propranolol. 40
The data analysis of the inflammatory reaction showed inhomogeneous results. Only the proinflammatory mediator IL-2 was inconsistent with results of significant higher values in EA + GA compared to that of other mediators as TNF-α and IL-10. The significantly higher values in anti-inflammatory mediator IL-10 concur with lower proinflammatory mediator TNF-α in EA + GA group versus GA group and can be interpreted as a beneficial effect of EA on the immune system and could be another explanation for the quicker recovery in the EA + GA group. Further animal studies by Zhang et al 43 showed that EA suppressed the inflammatory response by activation of the hypothalamus–pituitary–adrenal axis. None of the studies in this analysis used the acupuncture point ST-36, but as inflammatory response seems to play a key role among others in cardiac injury, it should be noted that Song et al 44 recently proved that EA at ST-36 attenuated proinflammatory cytokine release and it might be worth to consider this as an additional point in future studies.
Part of the beneficial effect of acupuncture for post-cardiac surgery patient and beneficial effect on their recovery is also the reduction of PONV. Cooke et al 45 showed in 712 patients that even PC-6 acupressure—a stimulation of meridian points without needles—is effective in preventing the onset of PONV following cardiac surgery. These results are consistent with the findings of investigations in craniotomy patients 46 and especially in laparoscopic surgeries, 47,48 which obviously have a high prevalence of PONV. It was also determined that preoperative acupuncture increased the efficacy of acupuncture compared to only postoperative treatment. 47
Besides less complications and a quicker recovery of patients in EA + GAgroup, these results might even implicate an economical value for the health-care system. Cost efficacy is evidenced by reduced drug requirements; and most significantly, although the total time of hospitalization remained the same, preoperative acupuncture seems to reduce the ICU length of stay, which is a major contributor to cost reduction during the hospitalization.
Limitations of this meta-analysis include the relatively low number of trials and the fact that only single center investigations were considered. However, all studies yielded a high level of evidence. Further limitation is provided by our risk of bias assessment and the possibility of a lack of blinding, despite of a lack of any positive information provided. Although we noticed the possibility of publication bias, as results of a similar study were published in 3 articles, the 3 articles were weighted as a single study to prevent bias on our side.
Conclusions
We summarize that the currently available literature is based on studies with a high level of evidence, although the number of studies and included patients is relatively small. This meta-analysis showed that additional electrostimulated acupuncture with needle placement through trained acupuncturists in patients undergoing GA for open-heart surgery may be beneficial due to reduced anesthetic consumption, increased cardiocirculatory stability, attenuation of inflammatory response and cardiac injury, as well as faster recovery with earlier discharge from ICU, which also implicates an economic potential for the hospital.
Supplementary Material
Supplemental Material, 20170227-JICM-Supplemental_material - Meta-Analysis of Electroacupuncture in Cardiac Anesthesia and Intensive Care
Supplemental Material, 20170227-JICM-Supplemental_material for Meta-Analysis of Electroacupuncture in Cardiac Anesthesia and Intensive Care by Sven Asmussen, Rene Przkora, Dirk M. Maybauer, John F. Fraser, Filippo Sanfilippo, Kristofer Jennings, Michael Adamzik and Marc O. Maybauer in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JFF confirmed receipt of grant support from Queensland Health OHMR and NHMRC 1010939.
Supplementary Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.