
Abstract
Objective:
To evaluate the impact of telemedicine programs in intensive care unit (Tele-ICU) on ICU or hospital mortality or ICU or hospital length of stay and to summarize available data on implementation cost of Tele-ICU.
Methods:
Controlled trails or observational studies assessing outcomes of interest were identified by searching 7 electronic databases from inception to July 2016 and related journals and conference literatures between 2000 and 2016. Two reviewers independently screened searched records, extracted data, and assessed the quality of included studies. Random-effect models were applied to meta-analyses and sensitivity analysis.
Results:
Nineteen of 1035 records fulfilled the inclusion criteria. The pooled effects demonstrated that Tele-ICU programs were associated with reductions in ICU mortality (15 studies; risk ratio [RR], 0.83; 95% confidence interval [CI], 0.72 to 0.96; P = .01), hospital mortality (13 studies; RR, 0.74; 95% CIs, 0.58 to 0.96; P = .02), and ICU length of stay (9 studies; mean difference [MD], −0.63; 95% CI, −0.28 to 0.17; P = .007). However, there is no significant association between the reduction in hospital length of stay and Tele-ICU programs. Summary data concerning costs suggested approximately US$50 000 to US$100 000 per Tele-ICU bed was required to implement Tele-ICU programs for the first year. Hospital costs of US$2600 reduction to US$5600 increase per patient were estimated using Tele-ICU programs.
Conclusions:
This systematic review and meta-analysis provided limited evidence that Tele-ICU approaches may reduce the ICU and hospital mortality, shorten the ICU length of stay, but have no significant effect in hospital length of stay. Implementation of Tele-ICU programs substantially costs and its long-term cost-effectiveness is still unclear.
Introduction
Intensive care medicine remains one of the most worrisome clinical medicine issues in developing countries. 1 –3 Economic growth and aging population prompted needs for critical care. 2,4 However, shortages of critical care staffs and intensive care unit (ICU) equipment hindered better critical care services, 5 which is predominant in countries with big populations like China. 1,6,7 Trained intensivists have been supposed to decrease mortality and costs of the ICU. 8 –11 However, there is a lack of well-trained intensivists for critically ill patients, especially in rural areas and a few community hospitals. 12 Even in the developed countries such as the United States, the predicted severity of ICU staff shortfall is notable during the next 3 decades. 4,13,14 Thereby, alternative care modes are urgently needed to meet the rapid expansion of demand in critical care.
Telemedicine, defined as “the use of medical information exchanged from one site to another via electronic communications to improve a patient’s clinical health status,” 15 has been put forward as an alternative solution to the issue of intensivists shortage. It is suggested to help severe patients get access to high quality of intensive care medicine. 16 –18 In ICU telemedicine (Tele-ICU) models, off-site critical care experts can access patients’ data such as medical records, laboratory test, and radiographic outcomes; implement remote real-time monitoring of vital signs; and facilitate the communication with bedside clinicians via computerized audiovisual approaches. 19,20
Conclusions regarding the impacts of Tele-ICU programs are inconsistent: Some studies reported that Tele-ICU programs showed more advantages in clinical and economic aspects compared with standard ICU care, 21 –23 whereas others did not. 24,25 The impacts of Tele-ICU in terms of patients’ clinical outcomes have been evaluated previously by 2 meta-analyses. 26,27 These meta-analyses stated that although the Tele-ICU programs might tend to be associated with lower ICU or hospital mortality, the effects were variable among different studies. Moreover, no evidence concerning the costs was examined in these meta-analyses. As a rapid growth of research in this area during the more than 4 years since publication of the latest meta-analysis, 26 there is a need for a new updated meta-analysis to determine the effects of Tele-ICU programs on patients and financial outcomes. It is hypothesized that there might be significant effects of Tele-ICU programs in reducing ICU mortality and length of stay, hospital mortality and length of stay, and the hospital cost for critically ill patients.
Materials and Methods
This meta-analysis followed the guidelines suggested by the Preferred Reporting Items for Systematic Reviews and Meta-analyses. 28 The methodology was based on recommendation by the Meta-analysis of Observational Studies in Epidemiology group. 29
Search Strategy
Seven electronic databases were searched: MEDLINE (Ovid, January 1, 1946, to May 24, 2016), EMBASE (Ovid, January 1, 1974, to May 27, 2016), the Cochrane Central Register of Controlled Trials (the Cochrane Library, Issue 6, June 2016), AMED (Ovid, January 1, 1985, to June 2, 2016), PyschINFO (Ovid, January 1, 1987, to June 4, 2016), CINAHL (Ebsco, January 1, 1982, to June 6, 2016), and Web of Science (January 1, 1970, to June 7, 2016; see details in Appendix 1). We also manually searched conference proceedings from annual meeting of American Telemedicine Association, European Society of Intensive Care Medicine, and American College of Chest Physician and Society of Critical Care Medicine between 2000 and 2016 and 4 major critical care journals, Critical Care, Intensive Care Medicine, Critical Care Medicine, and Chest between 2000 and 2016. Reference lists of all included studies were screened to identify additional publications. All literature searches were conducted with the assistance of a proficient medical information researcher. No language restrictions were applied and studies reported in languages other than English were translated when necessary. The authors of potential inclusion articles were attempted to contact to acquire more information about their studies.
Inclusion Criteria and Study Selection
All retrieved articles eligible for further review were selected by an initial screening of identifying titles and abstracts. Studies for final inclusion had to meet the inclusion criteria based on the PICO frame 30 : (1) participant: patients of all ages admitted to ICU; (2) intervention: adoption of telemedicine programs in ICU; (3) comparison: critical care delivered via telemedicine versus conventional ICU care; (4) outcome: at least one of the following outcomes of interest: primary outcome: ICU mortality; secondary outcome: hospital mortality, ICU or hospital length of stay, and implementation costs; and (5) design: controlled trials or observational trials. Studies that failed to report the details about the data of outcomes of interest were excluded. Two reviewers (J.C. and D.S.) independently screened all retrieved records based on the predefined inclusion criteria. Publication information of the retrieved records, such as authors, affiliations, journal titles, and funds, was hidden from the reviewers to reduce selector bias. When several publications reported the data from the same population, only the study with the most recent and complete data was included.
Data Extraction and Assessment of Study Quality
The following information was extracted independently by 2 reviewers (J.C. and D.S.) from each included study and recorded in a predesigned data recording form to control the within-study biases: authors, year of publication; population, age, gender; severity of illness index; physician ICU staffing models before telemedicine use; types of hospital and ICU where study took place; Tele-ICU care or structure modes; and outcomes. Disagreements were resolved through discussion between the reviewers or by consulting a third review author (W.Y.) when needed.
Two reviewers (J.C. and D.S.) assessed the methodologic quality of included studies using the Newcastle-Ottawa Quality Assessment Scale (NOS) for nonrandomized trials in a systematic review. 31 The score ranges from 0 to 9, with higher scores demonstrating higher quality.
Subgroup Analysis, Sensitivity Analysis, and Meta-Regression
The following subgroup analyses were planned: (1) type of hospitals: community hospitals versus noncommunity hospitals, including tertiary hospitals, urban hospitals, health-care systems, and academic medical centers; (2) type of Tele-ICU care models: continuous care model, scheduled care model, and reactive care model 32 ; (3) type of Tele-ICU structural models: centralized Tele-ICU and decentralized Tele-ICU 33 ; (4) ICU physician staffing patterns preintervention: low intensity (optional intensivist consultation or no intensivist) and high intensity (closed ICUs or mandatory intensivist consultation); and (5) the stratification of study quality: low- (NOS score ≤ 6) or high-quality studies (NOS score > 6). A sensitivity analysis by deleting each study in turn was performed to examine the impact of each study on the overall risk estimate and to test whether the results of the analyses were robust to reach conclusions. A linear meta-regression analysis was performed to explore some of the heterogeneous effect sizes between studies and to evaluate the effects of confounding factors on the influence of Tele-ICU programs. The continuous variables examined by meta-regression were year of publication, sample size, age, and duration of Tele-ICU intervention.
Data Synthesis and Analysis
Interrater agreement for initial screening, final inclusion, and assessment of study quality was reported using Cohen κ statistic. Data were synthesized based on a Mantel-Haenszel random-effects model for a more conservative effect. 34 Pooled data were reported as risk ratios (RRs) with 95% confidence intervals (CIs) for dichotomous outcomes and mean differences (MDs) with 95% CI for continuous outcomes. Statistical heterogeneity among studies was assessed using the χ2 test 35 and Ι2 statistic. 36 Evidence of publication bias was assessed by inspecting for asymmetry in Begg funnel plots and by conducting Egger test. 37 P values <.05 were considered statistically significant. All analyses were performed using Review Manager 5.3 statistic software (The Cochrane Collaboration, Oxford, England) and Stata 12 (StataCorp, College Station, Texas).
Results
Study Inclusion
The search strategies identified a total of 1035 records, 981 from electronic database and 54 from manual searching sources. Details regarding the search, study selection, and reason for exclusion are shown in Figure 1. Nineteen before-and-after design studies with 192 365 ICU patients (156 413 pre-Tele-ICU and 35 952 post-Tele-ICU), 72 hospitals, and 110 ICUs that fulfilled the final selection criteria (κ = .92) were identified and included in this meta-analysis. 21 –25,38 –51 Among these 19 articles, Marcin et al reported their results of patients’ outcomes and costs in 2 publications, 43,44 respectively; therefore, the 2 publications were included as 2 studies. Similar situation was applied to another 2 publications. 24,38 The remaining 47 studies were deemed to be ineligible for a variety of reasons: 17 were not original studies; 12 and 4 failed to compare the outcomes of interest and the intervention of interest, respectively; 4 reported data in a more recent study; and 10 provided insufficient data of outcomes to statistical analysis (see details in Appendix 2).
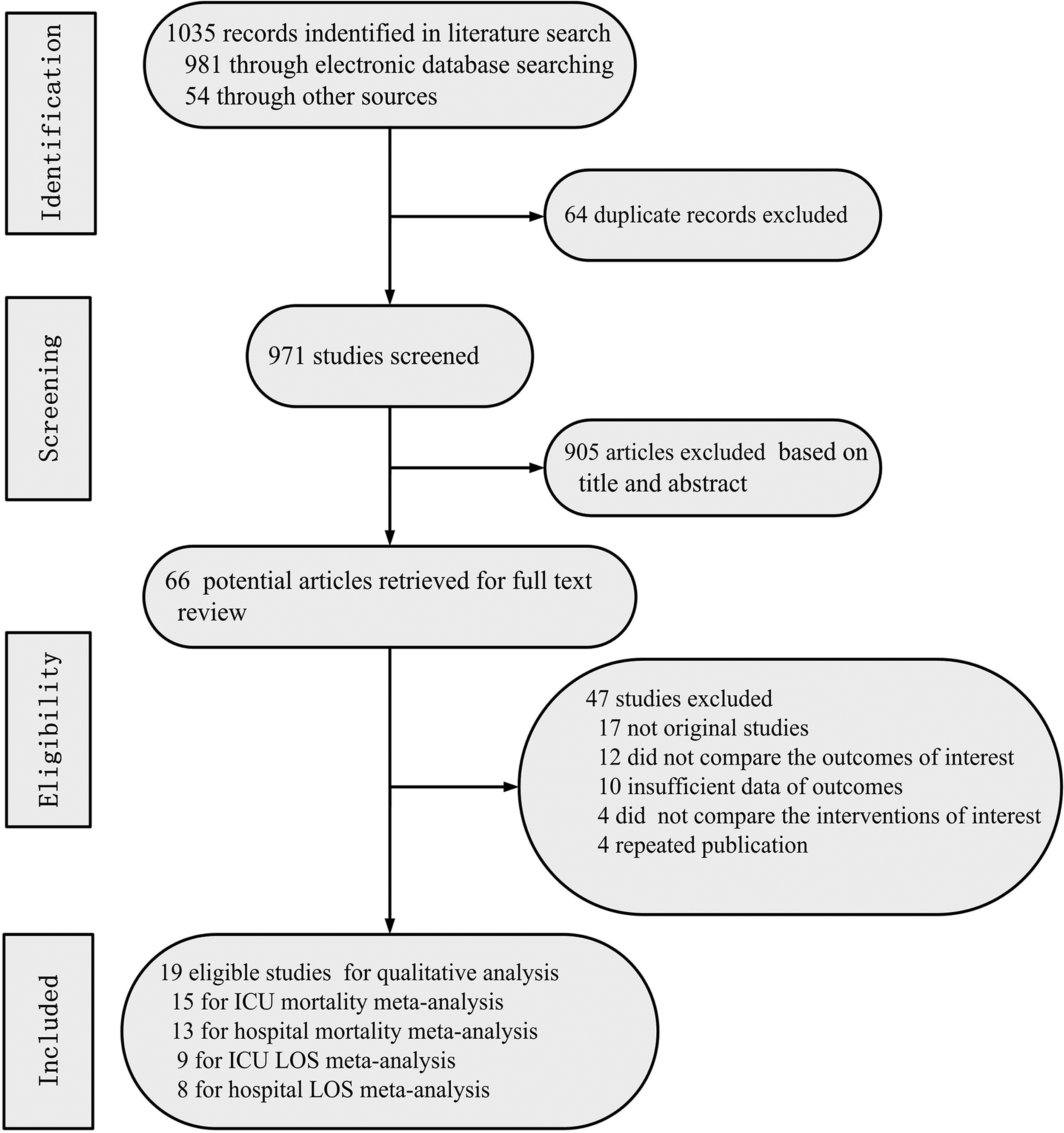
Flowchart showing systematic literature search and study selection process.
Study Characteristics and Quality Assessment
Characteristics of included studies are presented in Table 1. The median number of patients was 2823 (range: 296-118 990). The mean ages of participants enrolled were 63 years (range: 5.5-67 years) in the conventional care group and 65 years (range: 5.3-67 years) in the Tele-ICU care group. The intensity of ICU physician staffing patterns varied among studies before the implementation of Tele-ICU programs: 6 studies had high-intensity ICU staffing, 24,40,41,43 –45 7 studies had low physician ICU staffing, 21 –25,47,49 and the remaining studies reported no obvious demarcation. There were 10, 21,22,24,25,38,40,41,45,49,51 1, 23 and 2 43,44 studies which adopted continuous care, scheduled care, and reactive care models, respectively. Centralized and decentralized structure models were implemented in 11 21,24,25,38 –41,45,46,49,51 and 4 studies, 22,23,43,44 respectively (see details in Appendix 3). Overall study quality assessed by NOS was moderate (median, 6; range, 3-9; κ = .87; see details in Appendix 4).
Characteristics of Study Included.
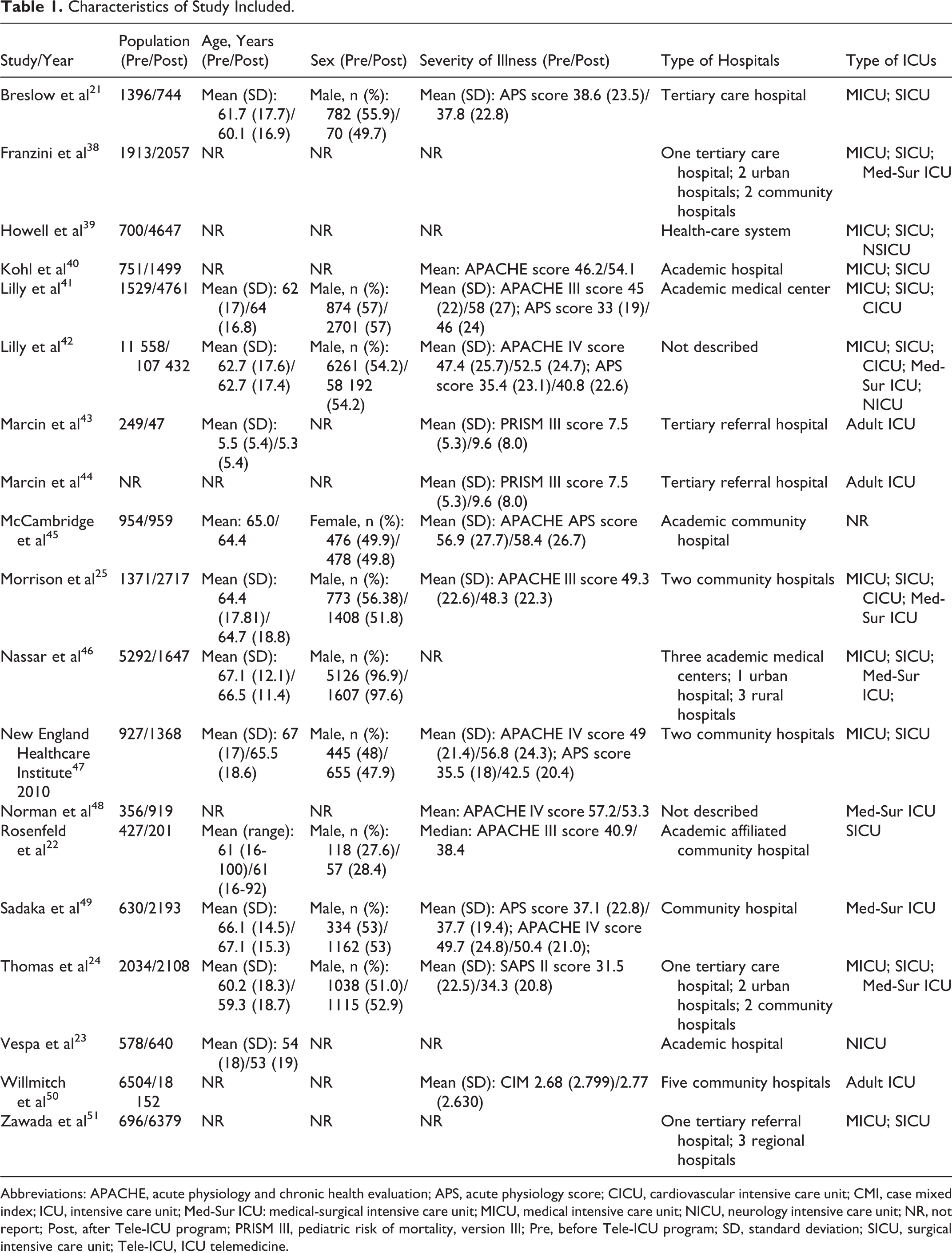
Abbreviations: APACHE, acute physiology and chronic health evaluation; APS, acute physiology score; CICU, cardiovascular intensive care unit; CMI, case mixed index; ICU, intensive care unit; Med-Sur ICU: medical-surgical intensive care unit; MICU, medical intensive care unit; NICU, neurology intensive care unit; NR, not report; Post, after Tele-ICU program; PRISM III, pediatric risk of mortality, version III; Pre, before Tele-ICU program; SD, standard deviation; SICU, surgical intensive care unit; Tele-ICU, ICU telemedicine.
Primary Outcome
ICU mortality
Fifteen studies presented outcomes of ICU mortality among 166 436 patients. 21 –25,39 –43,45 –47,49,51 The relationship between Tele-ICU program application and ICU mortality is illustrated in Figure 2. The overall pooled effect size (RR) for ICU mortality associated with the use of Tele-ICU programs was 0.83 (95% CI, 0.72-0.96; P = .01), with significant heterogeneity between studies (Ι2 = 78%, P < .00001). The Egger test manifested no evidence of publication bias (P = .713; see funnel plots in Appendix 5).
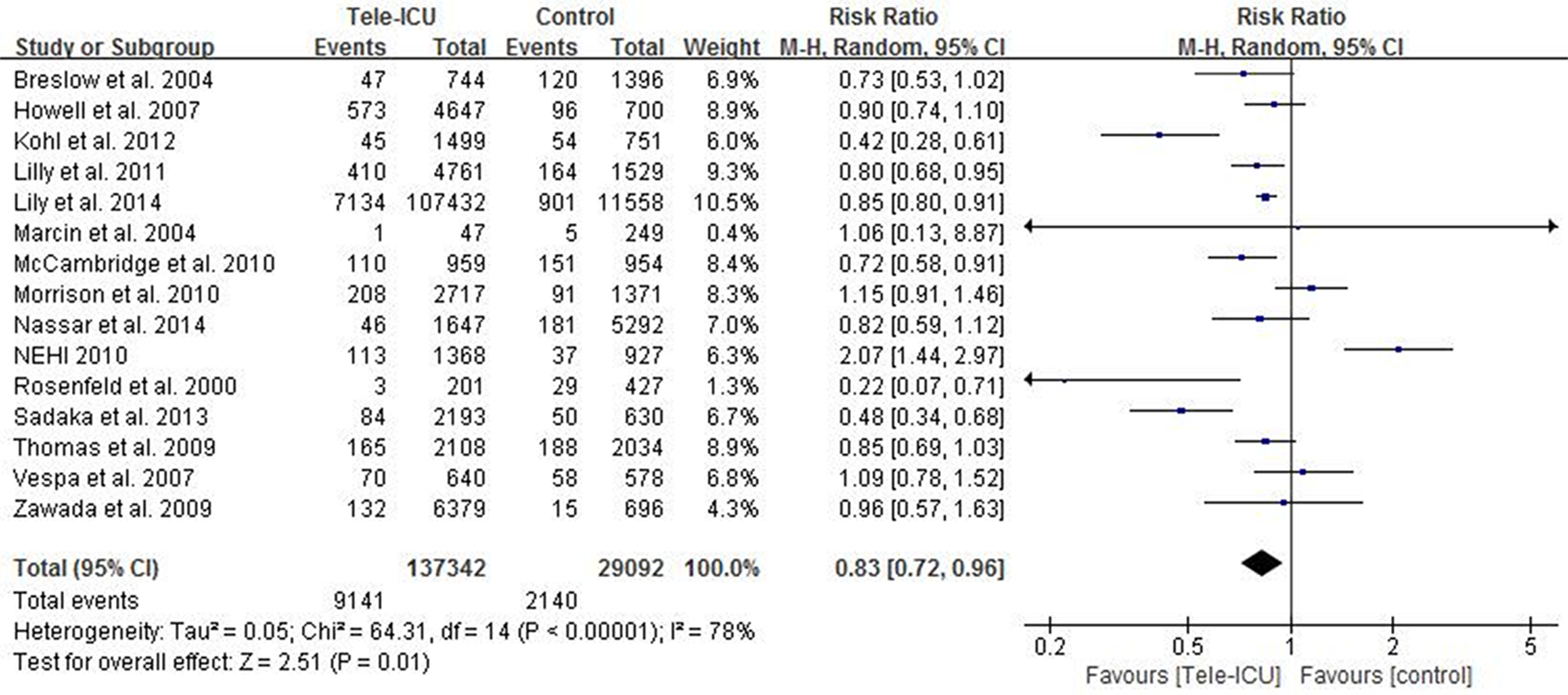
Forest plot of comparisons: intensive care unit telemedicine (Tele-ICU) care versus conventional critical care. Outcome: ICU mortality. Weight is the relative contribution of each study to the overall treatment effect (risk ratio and 95% confidence interval) on a log scale assuming a random-effects model.
Second Outcomes
Hospital mortality
Hospital mortality was reported in 13 studies among 183 209 participants. 21,22,24,25,40 –42,45 –51 In pooled analysis, there was a significant reduction in the hospital mortality associated with Tele-ICU programs (RR, 0.74; 95% CI, 0.58-0.96; P = .02). There was obvious heterogeneity between studies with an Ι2 of 97% (P < .00001; see Figure 3).
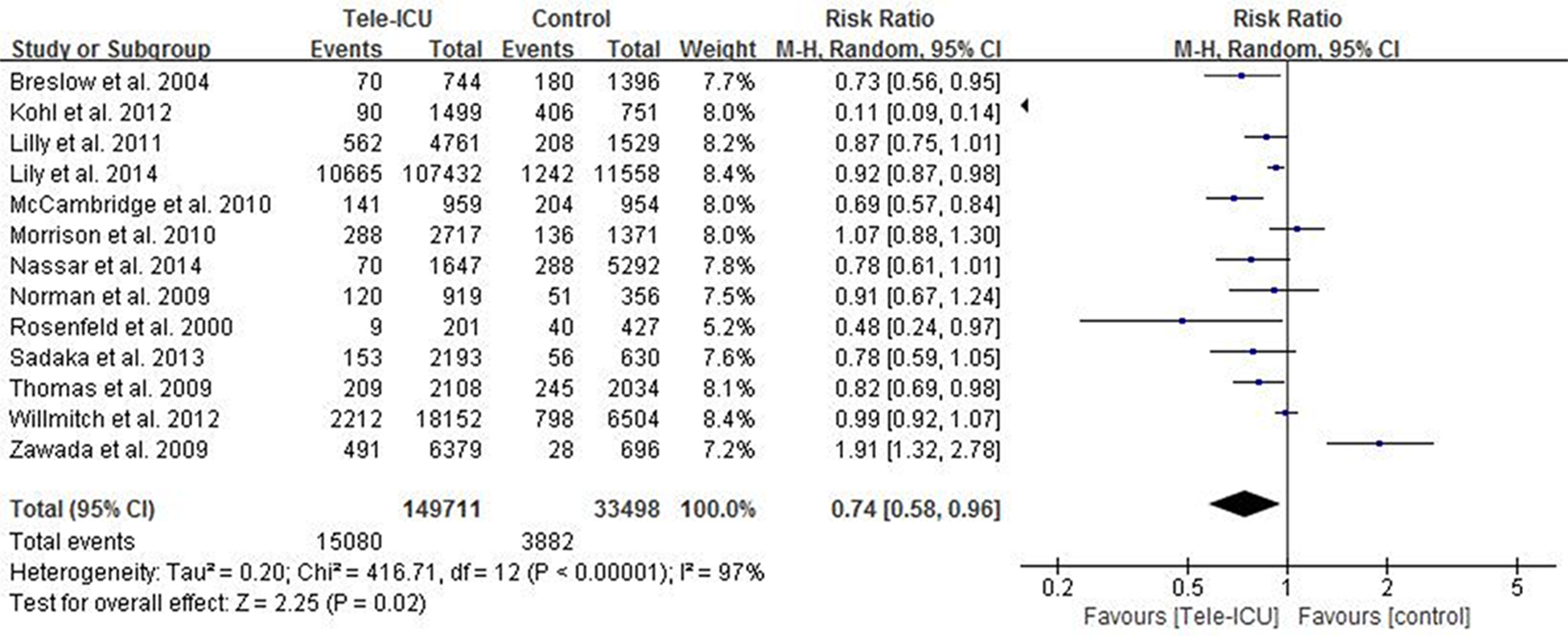
Forest plot of comparisons: intensive care unit telemedicine (Tele-ICU) care versus conventional critical care. Outcome: hospital mortality. Weight is the relative contribution of each study to the overall treatment effect (risk ratio and 95% confidence interval) on a log scale assuming a random-effects model.
Length of stay
The ICU length of stay was examined in 9 studies. 21 –23,25,40,41,46,49,50 The pooled data demonstrated Tele-ICU programs contributed to a remarkable reduction in ICU length of stay (MD, −0.63; 95% CI, −0.72 to 0.17; P = .007), with notable heterogeneity between studies (Ι2 = 93%, P < .00001; see Figure 4). Hospital length of stay was reported in 8 studies. 21,22,25,40,41,46,49,50 No significance difference was detected between Tele-ICU programs care and conventional care groups (MD, −0.27; 95% CI, −1.14 to 0.59; P = .54), with a high degree of heterogeneity (Ι2 = 92%, P < .00001; see Figure 5).
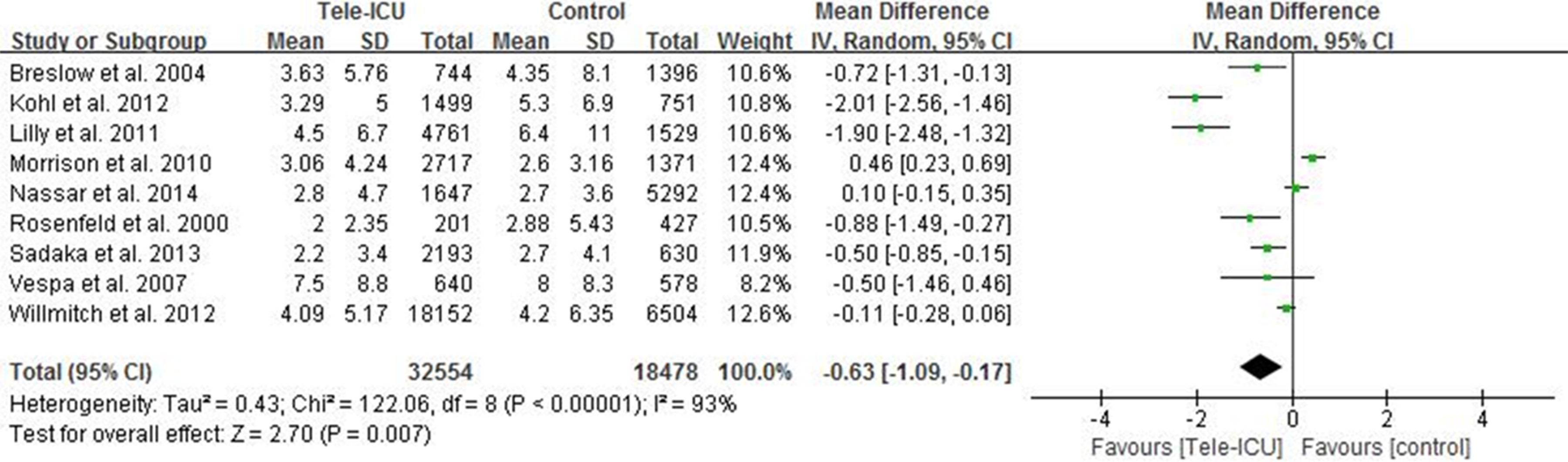
Forest plot of comparisons: intensive care unit telemedicine (Tele-ICU) care versus conventional critical care. Outcome: ICU length of stay. Weight is the relative contribution of each study to the overall treatment effect (mean difference with 95% confidence interval).
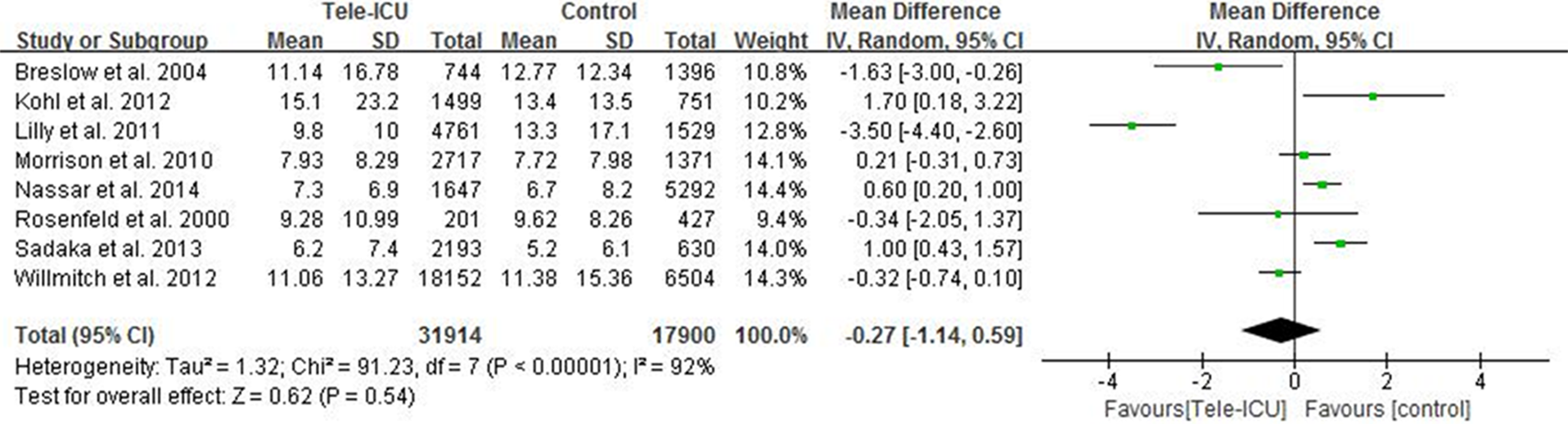
Forest plot of comparisons: intensive care unit telemedicine (Tele-ICU) care versus conventional critical care. Outcome: hospital length of stay. Weight is the relative contribution of each study to the overall treatment effect (mean difference with 95% confidence interval).
Cost and cost-effectiveness
Eight studies estimated the costs before and after Tele-ICU programs. 21,22,25,38,44,47,48,51 Implementation costs of Tele-ICU programs mainly include telemedicine technology and operating fees, staffing fees, and hospital variable fees. Table 2 summaries the costs of Tele-ICU programs according to the reported data. A common vendor (VISICU Inc, Baltimore, Maryland) supplied telemedicine system for 6 studies. 21,25,38,47,48,51 Based on the provided information, the estimated total cost to implement Tele-ICU programs ranged from US$50 000 to US$100 000 per Tele-ICU bed in the first year. The cost per patient for hospital varies from US$2600 reduction to US$5600 increase after using Tele-ICU programs.
Summary of Costs on Tele-ICU Programs.
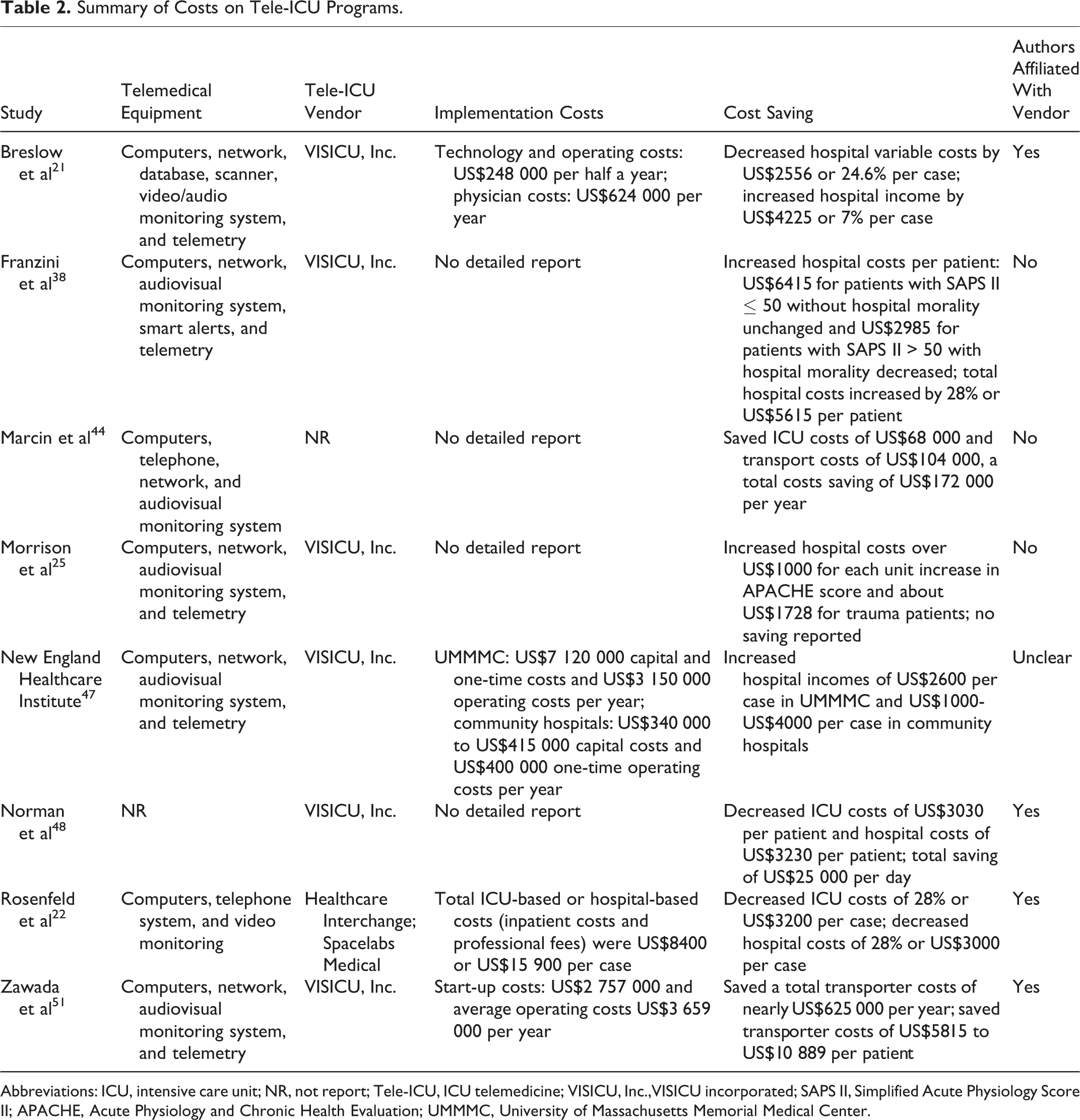
Abbreviations: ICU, intensive care unit; NR, not report; Tele-ICU, ICU telemedicine; VISICU, Inc.,VISICU incorporated; SAPS II, Simplified Acute Physiology Score II; APACHE, Acute Physiology and Chronic Health Evaluation; UMMMC, University of Massachusetts Memorial Medical Center.
Subgroup Analysis, Sensitivity Analysis, and Meta-Regression
The study conducted by Thomas et al presented data at hospital level, 24 which were included and analyzed on both community hospital and noncommunity hospital level (Table 3). The pooled effects that presented notable reductions in ICU mortality were associated with Tele-ICU programs implemented in noncommunity hospital (RR, 0.80; 95% CI, 0.66-0.95; P = .01), Tele-ICU continuous care (RR, 0.72; 95% CI, 0.58-0.88; P = .002), Tele-ICU centralized structure (RR, 0.77; 95% CI, 0.66-0.90; P = .001), and high-intensity ICU staffing pre Tele-ICU use (RR, 0.70; 95% CI, 0.56-0.89; P = .004). However, the stratification analysis of study quality showed no significant difference in ICU mortality between higher quality (RR, 0.85; 95% CI, 0.72-1.00; P = .05) and lower quality (RR, 0.79; 95% CI, 0.54-1.17; P = .24). The result of sensitivity analysis indicated that no single study dominated the overall RR. The 15 study-specific RRs ranged from a high value of 0.87 (95% CI, 0.76-1.00) to a low value of 0.79 (95% CI, 0.70-0.89) via deletion of the study by Kohl et al 40 and the study by New England Healthcare Institute, 47 respectively (see details in Appendix 6). Meta-regression analyses showed that year of publication (P = .879), sample size (P = .897), age (P = .865), and duration of Tele-ICU programs (P = .274) were not associated with the effects of Tele-ICU programs on ICU mortality.
Subgroup Analysis of ICU Mortality.
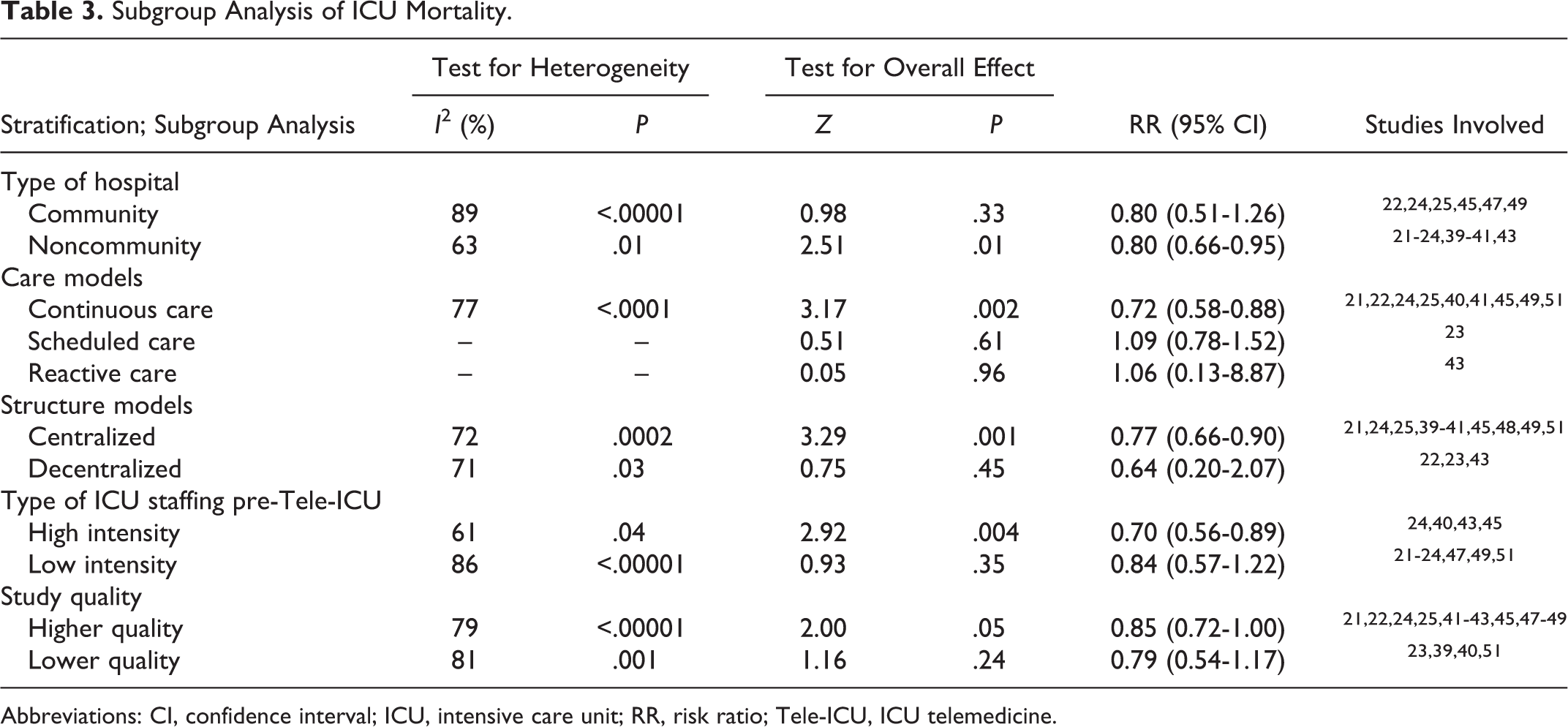
Abbreviations: CI, confidence interval; ICU, intensive care unit; RR, risk ratio; Tele-ICU, ICU telemedicine.
Discussion
The current meta-analysis of Tele-ICU programs was relevant to a significant reduction in ICU mortality, hospital mortality, and ICU length of stay but had no effect on hospital length of stay. An initial implementation cost of Tele-ICU programs was estimated to be US$50 000 to $100 000 per Tele-ICU bed in the first year. The hospital costs vary from US$2600 reduction to US$5600 increase per patient, which were similar to the results of a recent systematic review and meta-analysis. 52 Moreover, it was found that the relationship between application of Tele-ICU programs and ICU mortality varied based on factors such as type of hospitals, Tele-ICU care model, Tele-ICU structure model, and ICU physician staffing model preintervention. However, the subgroup analysis found that a significant reduction in ICU mortality was not associated with the Tele-ICU programs, regardless of high or low study quality. Summarily, the findings of this study suggest the Tele-ICU programs play roles in improving clinical outcomes for critical illness patients, but strength of evidence entails further research in this area.
Results of the present study are in line with those of a recent meta-analysis. 26 Wilcox and Adhikari reported that ICU mortality or length of stay and hospital mortality or length of stay were all reduced after the use of Tele-ICU programs. 26 One explanation for the different results might be more studies with more participants enrolled in this review to extend the evidence. Results of subgroup analysis concerning study quality were consistent with those of 2 previous reviews. 26,27 Several other subtypes analyses were performed to explore the high degree of heterogeneity. A range of discrepancies regarding Tele-ICU models and hospital-level variables, such as location, management pattern, medical equipment configuration, staffing, and teaching resources among studies, may affect the analyzing outcomes. 53 It is crucial to attempt to explore the effects of Tele-ICU based on different situations. After stratification analyses, it is inferred that Tele-ICU programs are inclined to manifest their effects in better resource configured hospitals, such as tertiary hospitals, urban hospitals, and academic medical centers. Hospitals equipped with active Tele-ICU care models or centralized Tele-ICU structure models are also beneficial from Tele-ICU programs. Whereas, it appears that there is no significant difference concerning ICU mortality by using Tele-ICU programs in hospitals with lower intensivists staffing, such as community or rural hospitals. 54
An increasing body of evidence indicates Tele-ICU programs would be an effective approach to improve clinical outcomes and reduce hospital costs by increasing ICU volume, 55 improving adherence to best practice, 47 and decreasing complications and length of stay for patients. 56,57 Nevertheless, quite a few barriers still need to be overcome before Tele-ICU programs are put into clinical use. One of the barriers examined in our study is apparent variations in sample size, characteristic of population, conceptual framework, telemedicine technologies measurement methods, preintervention ICU environment, how Tele-ICU programs monitored, and duration of intervention showed in Tables 1 and 2. These factors may contribute to a high degree of clinical heterogeneity. However, we did not find significant correlation between ICU mortality and probable confounding factors such as year of publication, sample size, age, and duration of Tele-ICU intervention by meta-regression. Additionally, it is assumed that patients’ medical history, professional level of critical care staff, acceptance degree of Tele-ICU programs, and local socioeconomic status may also be confounding factors affecting the outcomes of Tele-ICU programs. However, we failed to evaluate these factors because of limited data. In all, it is arduous to assess the effects of Tele-ICU due to the lack of a standard definition and implementation guidelines for Tele-ICU intervention. 58
This review has several limitations. First, although comprehensive search strategies and strict inclusion criteria were adopted for screening eligible studies, sample bias and selection bias could be inevitable. Moreover, the methodologic limitations of nonrandomized trials included in this review are prone to result in a high risk of bias. Second, it is regrettable not to identify the source of heterogeneity among studies in primary outcome, even if adequate subgroup analyses, sensitivity analysis, and meta-regression analyses were conducted to explore clinical variations and the probable confounding factors. Third, the inconsistent severity of illness among the included studies and unadjusted data used by this meta-analysis may have overestimated the effects and yielded potentially misleading conclusions. 59 Finally, subgroup analyses should be interpreted with caution due to the potential bias inherent in subgroup analyses and the lack of criteria to assess the credibility of subgroup analyses in this review. 60
Conclusions
The present meta-analysis indicates that Tele-ICU programs may reduce ICU mortality, hospital mortality, and lengths of ICU stays. However, Tele-ICU programs are not associated with decreased lengths of hospital stays. Meanwhile, this study implies that an approximate of US$50 000 to US$100 000 per Tele-ICU bed is estimated to implement Tele-ICU programs in the first year. The cost per patient for the hospital varies from US$2600 reduction to US$5600 increase after Tele-ICU programs application. The long-term cost-effectiveness of the programs requires further exploration.
Supplemental Material
Supplemental_materials - Clinical and Economic Outcomes of Telemedicine Programs in the Intensive Care Unit: A Systematic Review and Meta-Analysis
Supplemental_materials for Clinical and Economic Outcomes of Telemedicine Programs in the Intensive Care Unit: A Systematic Review and Meta-Analysis by Jing Chen, Dalong Sun, Weiming Yang, Mingli Liu, Shufan Zhang, Jinhua Peng, and Chuancheng Ren in Journal of Intensive Care Medicine
Footnotes
Authors’ Note
Jing Chen and Dalong Sun contributed equally to this work. Chuancheng Ren had access to all the data in this study and takes full responsibility for the integrity of the work and the accuracy of data analysis. Jing Chen, Dalong Sun, and Chuancheng Ren contributed to the conceptualization of the study, the search for candidate studies, and the interpretation of the data. Jing Chen, Dalong Sun, and Weiming Yang contributed to the title, abstract, and full paper review and data abstraction. Dalong Sun, Weiming Yang, Mingli Liu, and Jing Chen contributed to the quality assessment. Jinhua Peng contributed to guidance regarding the context of the study. Jing Chen, Dalong Sun, and Weiming Yang contributed to the data analysis. Jing Chen contributed to the drafting of the initial manuscript. Dalong Sun, Weiming Yang, Mingli Liu, and Chuancheng Ren contributed to the manuscript revision. The appendixes can be found in the Supplemental Materials section of the online article.
Acknowledgments
The authors thank Tianwu Chen, PhD, for helping with editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.