
Abstract
Objectives:
Our primary aim was to determine the factors leading to prophylactic endotracheal intubation in intensive care unit (ICU) patients undergoing gastrointestinal endoscopy. Secondary aims were to determine the rate of unplanned endotracheal intubations during endoscopy and to determine the rate of aspiration following endoscopy for patients admitted to the ICU.
Methods:
Critically ill adult (≥18 years) patients who underwent upper and lower endoscopic procedures from January 2012 to July 2016 in a medical/surgical ICU were included. Determinants of prophylactic endotracheal intubation prior to endoscopy as well as other postprocedure outcomes were electronically captured by a validated data mart system. Given our focus on aspiration in those who were not endotracheally intubated prior to endoscopy, we used a validated definition a priori.
Results:
A total of 320 patients were included in the final analysis: 76(24%) were intubated prior to endoscopy and 244 (76%) were not. The endotracheally intubated group had a significantly higher Acute Physiologic and Chronic Health Evaluation III (44.5 [16.2] vs 39.5 [15.5]; P = .02) and Sequential Organ Failure Assessment (6.9 [4.4] vs 3.8 [3]; P ≤ .01) scores, higher rate of hematemesis within 24 hours of endoscopy (28 [37%] vs 45 [18%]; P ≤ .01), and higher rate of upper endoscopy (72 [96%] vs 181 [74%]; P ≤ .01). We composed a composite outcome for multivariable analyses, which demonstrated the rate of any complication was significantly higher among those who were intubated prior to the procedure versus those who were not intubated previously (odds ratio: 2.80, 95% confidence interval (CI): 1.16-6.72, P = .02).
Conclusion:
Endoscopy performed in the ICU without endotracheal intubation is safe. However, patient selection for prophylactic intubation prior to endoscopy is of critical importance as illustrated in this study with higher illness severity, planned upper endoscopy, and hematemesis 24 hours prior being key factors on deciding to perform endotracheal intubation. Prophylactic intubation for endoscopy and preexisting cardiac disease were associated with a higher rate of adverse outcomes.
Keywords
Introduction
Gastrointestinal hemorrhage is a common condition requiring intensive care unit (ICU) admission and urgent endoscopy. The ICU physicians are typically responsible for conscious sedation and/or airway management during the procedure. Currently, there are no consensus statements to guide this aspect of care. Prophylactic intubation for all endoscopies is not the standard of care. However, excessive sedation, desaturation, airway obstruction, or aspiration during the procedure may necessitate emergent endotracheal intubation. Emergent endotracheal intubations have been associated with a 30% incidence of complications. 1 A related study performed at Mayo Clinic evaluated the rate of cardiopulmonary complications and the differences between patients who were prophylactically intubated and those who were not and demonstrated that complications after endoscopy were unaffected by the practice of prophylactic intubation. 2 However, there are no published data describing the incidence of emergent endotracheal intubation during endoscopy for critically ill patients and relatively limited data exploring determinants for prophylactic intubation prior to endoscopy.
The proposed study aims to determine the potential factors leading to the decision to perform endotracheal intubation prior to endoscopy. Moreover, we aim to evaluate the incidence of emergent endotracheal intubations with a specific focus on the incidence of aspiration pneumonia in critically ill ICU patients. The results of this study may be used to guide consensus statements regarding conscious sedation for critically ill patients undergoing gastrointestinal endoscopy in the ICU.
Methods
The present study was deemed exempt by Mayo Clinic Rochester institutional review board. All patients gave prior research authorization to use their medical records for research.
Patient Population
All adult (≥18 years) patients admitted to a medical/surgical ICU who underwent gastrointestinal endoscopy (upper and lower) under sedation were included. Patients of <18 years of age, patients who were pregnant at the time of the endoscopy, and patients who refused research authorization were excluded.
Study Design
The present study was conducted as a historical cohort study of all adult patients undergoing gastrointestinal endoscopy in an ICU under conscious sedation from January 2012 to July 2016. Gastrointestinal endoscopic procedures included upper and lower endoscopies. All procedure notes entitled “endoscopy” were searched in the electronic medical record and cross-referenced to the patient’s ICU admission. Date(s) and time(s) of initiation and conclusion of endoscopy were collected, in addition to the date and time of endotracheal intubation, if done during the endoscopy. This information was available from the sedation record in Mayo Information Clinical Systems Chart+ Viewer and Remote View. The remainder of the data was collected using an electronic data mart system. The ICU data mart has been validated previously. 3 We then stratified the cohort into those intubated prior to endoscopy and those who were not intubated previously.
Aspiration
We defined aspiration as follows: (1) a note in the electronic medical record of presence of bilious secretions or particulate matter in the tracheobronchial tree by direct visualization (ie, bronchoscopy); (2) for patients who did not have their tracheobronchial airways directly examined after regurgitation, postoperative chest imaging with infiltrates not identified by preoperative chest imaging, or findings consistent with infiltrates on physical examination; or (3) note in the electronic medical record stating definite aspiration of gastric material (intraprocedure emesis). 4 Aspiration was then grouped into definite, possible, or no aspiration. The information was abstracted manually by study personnel (M.O.S., M.K.). All manually collected data were entered into a standardized case report form. Study personnel were trained in its use prior to implementation. To verify accurate data capture, we manually examined 60 charts at random (N.J.S., D.A.D.).
Statistical Analysis
Unless specified otherwise, data are summarized as mean (standard deviation) for continuous variables and frequency counts and percentages for categorical variables. Characteristics were compared between those who were intubated prior to the procedure and those who were not intubated previously using the 2-sample t test for continuous variables and the χ2 test or Fisher exact test for categorical variables. Complication rates are summarized using point estimates and corresponding 95% confidence intervals (CIs). Given the low number of patients who experienced specific types of complications, a composite end point was created to indicate patients who experienced any complication (with the exception of unplanned intubation). Multivariate logistic regression analyses were then performed with this composite end point as the dependent variable, intubation prior to the procedure as the primary explanatory variable of interest, and all characteristics with some evidence (P < .10) indicating that they differed between those who were intubated prior to the procedure versus those who were not intubated previously included as covariates. Since the type of procedure and the indication for the procedure are highly correlated, separate analyses were performed with one of these variables included in each model. The findings from these analyses are summarized by reporting the odds ratio (OR) and corresponding 95% CIs. In all cases, 2-tailed tests were performed, with P < .05 used to denote statistical significance. All analyses were done by D.R.S.
Sample Size
This study includes all critically ill patients who underwent endoscopy at Mayo Clinic Rochester, Minnesota during a 4-year time period. A formal sample size/power analysis was not performed. Results are presented using point estimates along with corresponding 95% CIs.
Results
The final cohort included 320 critically ill patients who underwent gastrointestinal endoscopy in a medical/surgical ICU (Figure 1). Overall, 76 (24%) patients were endotracheally intubated prior to endoscopy. Patients who were prophylactically endotracheally intubated prior to endoscopy had higher Acute Physiologic and Chronic Health Evaluation (APACHE) III (44.5 [16.2] vs 39.5 [15.5]; P = .016) and Sequential Organ Failure Assessment (6.9 [4.4] vs 3.8 [3]; P ≤ .001) scores compared to those who were not. The same group also had a higher rate of hematemesis prior to endoscopy (28 [37%] vs 45 [18%]; P ≤ .001] as well as having upper endoscopy performed more frequently (72 [96%] vs 181 [74%]; P ≤ .001) than those who were not endotracheally intubated. Of note, neither body mass index nor the patients’ comorbidities influenced the rate of endotracheal intubation for endoscopy, although there was a trend for patients with cirrhosis being intubated more frequently (18 [24%] vs 36 [15%]; P = .070; Table 1).
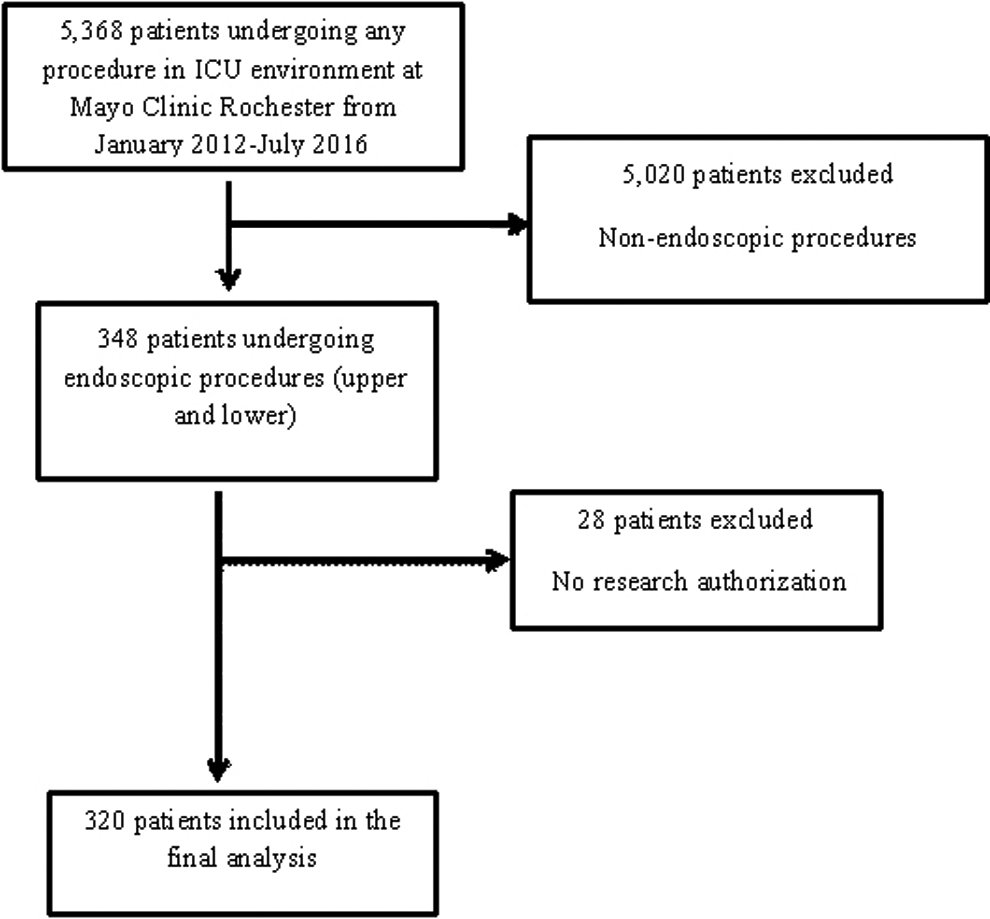
Patient flow diagram.
Patient Characteristics.
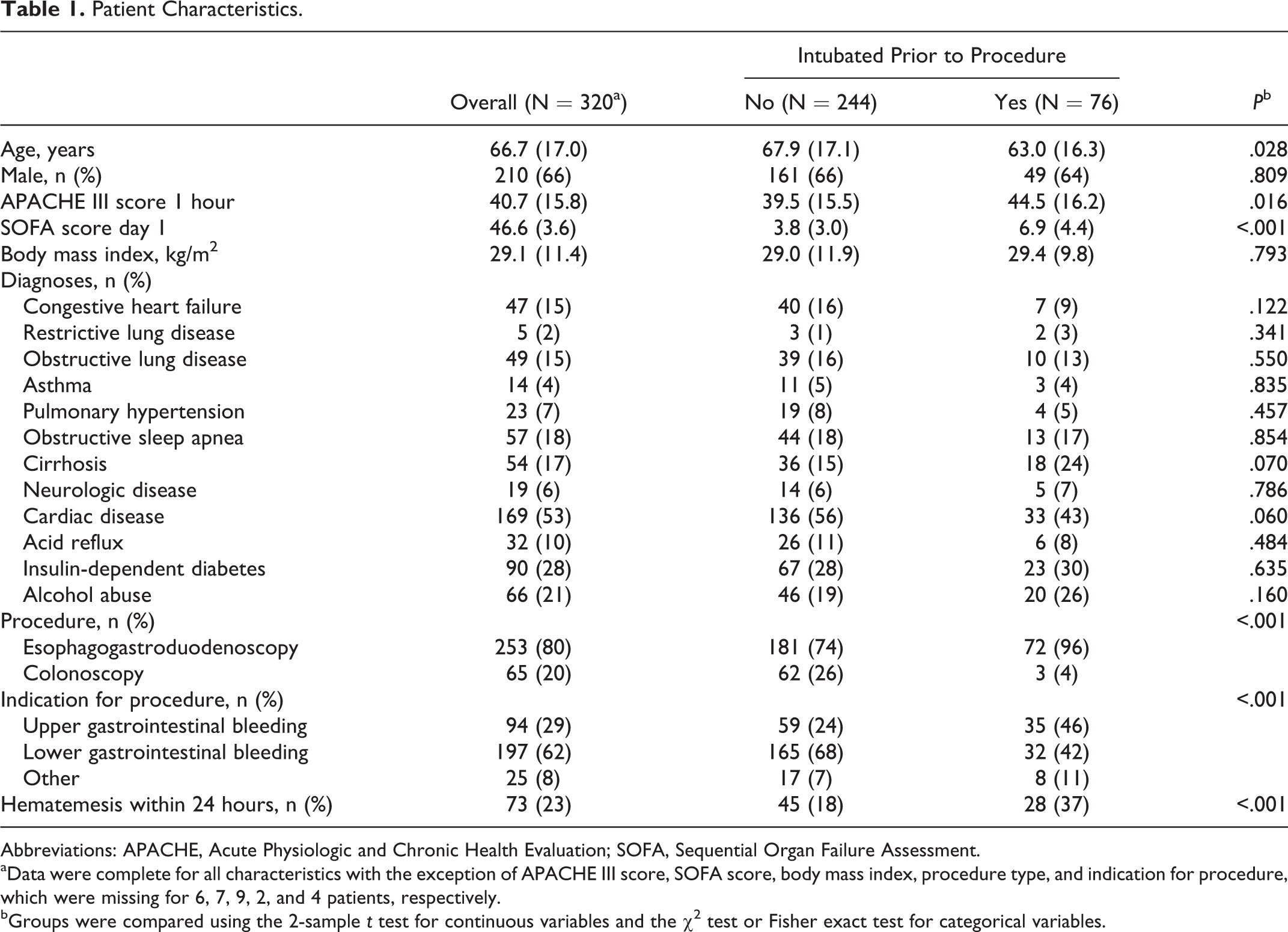
Abbreviations: APACHE, Acute Physiologic and Chronic Health Evaluation; SOFA, Sequential Organ Failure Assessment.
aData were complete for all characteristics with the exception of APACHE III score, SOFA score, body mass index, procedure type, and indication for procedure, which were missing for 6, 7, 9, 2, and 4 patients, respectively.
bGroups were compared using the 2-sample t test for continuous variables and the χ2 test or Fisher exact test for categorical variables.
Overall, the group experienced a low rate of complications with pneumonia, aspiration, and acute respiratory distress syndrome (ARDS) occurring in 13 (4%), 8 (3%), and 6 (2%) patients, respectively. There was no significant difference in the rates of pneumonia (10 [4%; 95% CI, 2%-7%] vs 3 [4%; 95% CI, 1%-11%]; P = 1.00) or aspiration (4 [2%; 95% CI, 1%-4%] vs 4 [5%; 95% CI, 2%-13%]; P = .09) between groups. However, the prophylactic endotracheal intubation group had a significantly higher rate of ARDS (4 [5%; 95% CI, 2%-13%] vs 2 [1%; 95% CI, 0%-3%]; P = .03). The rate of unplanned endotracheal intubations occurred in 9 patients with a frequency of approximately 4% (95% CI, 2%-7%; Table 2).
Postprocedural Complications.
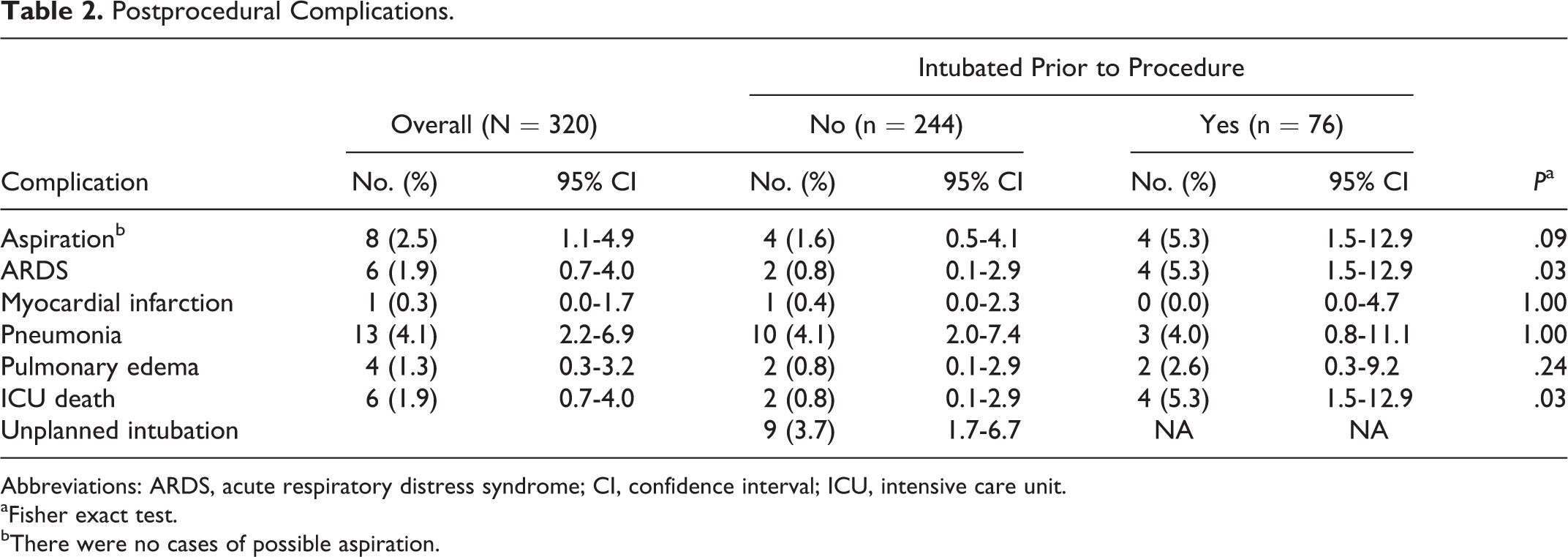
Abbreviations: ARDS, acute respiratory distress syndrome; CI, confidence interval; ICU, intensive care unit.
aFisher exact test.
bThere were no cases of possible aspiration.
While in the ICU, we observed a significantly higher rate of death in those who were endotracheally intubated prior to endoscopy as compared to those who were not (4 [5%; 95% CI, 2%-13%] vs 2 [1%; 95% CI, 0% to 3%]; P = .03; Table 2).
In order to perform multivariable analyses, a composite end point was created to indicate patients who experienced aspiration, ARDS, myocardial infarction, pneumonia, pulmonary edema, or ICU death. There were 34 (11%) of 320 patients who experienced one or more of these events, including 15 (20%) of 76 patients who were intubated prior to the procedure and 19 (8%) of 244 patients who were not. From multivariable analyses, the rate of any complication was significantly higher among those who were intubated prior to the procedure versus those who were not intubated previously (OR: 2.80, 95% CI: 1.16-6.72, P = .02) and those with preexisting cardiac disease (OR: 2.71, 95% CI: 1.12-6.60, P = .03; Table 3).
Multivariable analyses.a
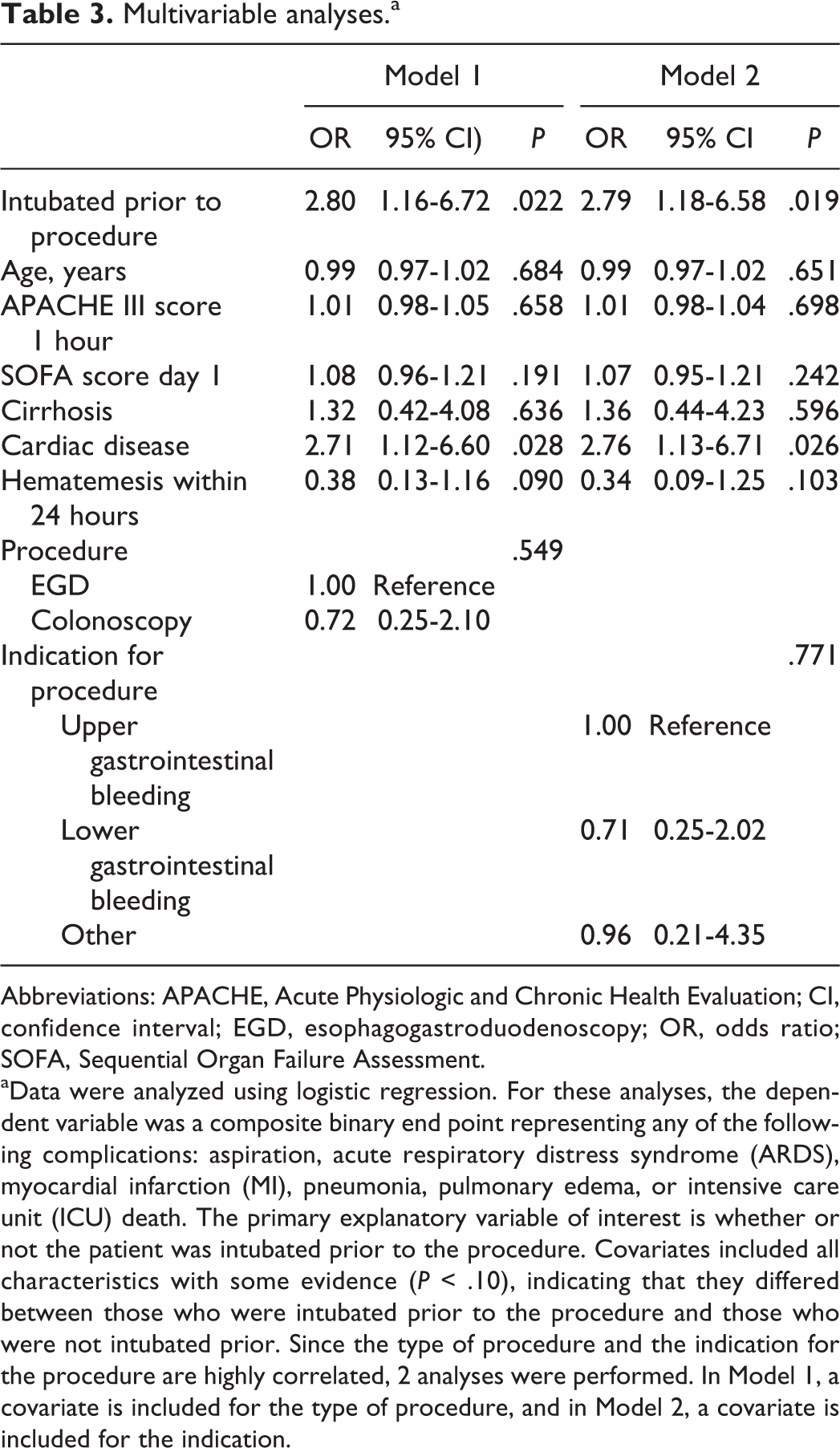
Abbreviations: APACHE, Acute Physiologic and Chronic Health Evaluation; CI, confidence interval; EGD, esophagogastroduodenoscopy; OR, odds ratio; SOFA, Sequential Organ Failure Assessment.
aData were analyzed using logistic regression. For these analyses, the dependent variable was a composite binary end point representing any of the following complications: aspiration, acute respiratory distress syndrome (ARDS), myocardial infarction (MI), pneumonia, pulmonary edema, or intensive care unit (ICU) death. The primary explanatory variable of interest is whether or not the patient was intubated prior to the procedure. Covariates included all characteristics with some evidence (P < .10), indicating that they differed between those who were intubated prior to the procedure and those who were not intubated prior. Since the type of procedure and the indication for the procedure are highly correlated, 2 analyses were performed. In Model 1, a covariate is included for the type of procedure, and in Model 2, a covariate is included for the indication.
Discussion
Our aim was to ascertain the determinants of prophylactic endotracheal intubation in critically ill patients undergoing upper and lower endoscopy. Our results demonstrate that although the practice of endoscopy, both upper and lower, is safe in the critically ill patients, prophylactic endotracheal intubation occurred more frequently in those with higher illness severity scores and having had a history of hematemesis prior to the procedure. Upper endoscopy was associated with a larger number of prophylactic intubations as compared to lower endoscopy.
Our results are consistent with those from a prior study by Rehman and colleagues. 2 They determined that the probability of endotracheal intubation was dependent on APACHE III score, age, the presence of hematemesis, previous lung disease, and the number of transfusions. In our study, we found that age was lower in those endotracheally intubated prior to endoscopy, which was congruent with other studies. 5,6 Although the study by Rehman and colleagues and our study were both performed at the same center, we included surgical ICU patients and lower endoscopies into our analysis. This likely contributed to the differences. Thus, in a mixed ICU population having both upper and lower endoscopy performed, higher illness severity, planned upper endoscopy, and the presence of hematemesis within 24 hours of the endoscopy event are associated with prophylactic endotracheal intubation.
The complication rates noted in the current study are significantly lower than reported in prior studies. 7,8 For example, Rudolph and colleagues demonstrated an aspiration rate of 12% to 15% with an even higher rate (48%) occurring in those endotracheally intubated specifically for airway protection. Their definition for aspiration focused on hospital records and new pulmonary infiltrates on chest imaging. 7 Our definition was expanded to include the evaluation of the tracheobronchial tree. Despite a more sensitive definition, we found a considerably lower rate in our study. This likely relates to temporal shifts in care as the prior study took place between 1988 and 1992 as well as smaller sample size.
The most frequent complication noted was pneumonia, which occurred in 13 patients, with the majority of patients not endotracheally intubated prior to endoscopy (10 [4%] vs 3 [4%]). This is in contrast to the study of Tang and Wang. 8 They noted a higher rate of pneumonia in the prophylactic endotracheal intubation group. However, their cohort was relatively small, with around 100 patients included in the final analysis. In addition, their cohort did not include surgical ICU patients or lower endoscopies and was conducted from 2008 to 2013. Again, temporal shift in care may also explain the discrepancy. Of note, a meta-analysis conducted in 2015 demonstrated a higher rate of pneumonia in patients receiving prophylactic endotracheal intubation prior to upper endoscopy; however, this was heavily weighted by the study of Rehman and colleagues. 9 This was confirmed in a subsequent study in 2016. 6 The above studies used a more concrete definition than ours, which add to the discrepancy and may explain the contrasting results.
We noted that the only significant finding in postprocedure outcomes related to the development of ARDS in the prophylactic endotracheal intubation group. This is consistent with the prior study done by Rehman and colleagues and likely relates to the fact that this patient population had a higher rate of illness severity as well as had a higher rate of hematemesis, which is a risk factor for the development of ARDS. 2,10
We noted a higher ICU mortality in those endotracheally intubated prior to endoscopy. The observed increased mortality in this group likely relates to the characteristics of patient selection, as this group had a higher illness of severity compared to the group not endotracheally intubated prior to endoscopy. Previous studies have demonstrated this association as well. 11 –16
In order to delineate the above outcomes more specifically, we created a composite outcome given the limited number of events. We found a significant association between prophylactic intubation and preexisting cardiac disease with the composite outcome. In regard to cardiac disease, the literature demonstrates that cardiopulmonary disease, advanced age, and higher illness severity are patient-related risk factors for cardiopulmonary adverse events associated with upper endoscopy. 17,18 Our composite outcome primarily involves cardiopulmonary adverse events.
Our study has significant limitations. We did not perform any matched analysis between those endotracheally intubated and those not intubated prior to endoscopy. This was a descriptive study only. However, we set out to determine the characteristics leading to endotracheal intubation prior to endoscopy, and thus, our study approach was sufficient for the question at hand. Further limitations include definitions that were used for certain outcomes. For example, our definition of aspiration was not the same as used in other studies. However, we expanded on a definition that has been previously validated in the literature. Pneumonia was established based on clinical documentation in the medical record along with chest imaging demonstrating infiltrate and elevated white blood cell count. Our definition is not an established definition and it is nonspecific. Finally, other limitations include not capturing certain important data variables such as smoking history and anticoagulation (possible confounding) as well as missing data fields and the retrospective design.
Conclusion
Airway management during endoscopy performed in the critically ill patients is not standardized. Our results demonstrate that although the practice of endoscopy, both upper and lower, is safe in the critically ill patients, whether an airway is established or not, prophylactic endotracheal intubation occurred more frequently in those with higher illness severity scores and having had a history of hematemesis prior to the procedure. Upper endoscopy was associated with a larger number of prophylactic intubations as compared to lower endoscopy. Clinicians should be cognizant of the above factors when deciding to perform endotracheal intubation for the critically ill patients prior to endoscopy. Finally, it should be recognized that performing intubation prior to endoscopy may be associated with a higher rate of adverse outcomes, especially in those patients with preexisting cardiac disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Division of Critical Care Medicine with no direct financial support.