
Abstract
Purpose:
Gastrointestinal dysfunction and failure (GID and GIF) in critically ill patients are a common, relevant, and underestimated complications in ICU patients. The aims of this study were (1) to determine plasmatic levels of citrulline, glutamine, and arginine as markers of GID/GIF in critically ill patients with or without GID/GIF with or without multiple organ failure (MOF) and (2) to assess the role of intra-abdominal hypertension in these patient groups.
Materials and Methods:
This is a 1-year, monocentric (Italian hospital), prospective observational study. Inclusion criteria were adult patients with GID/GIF, with or without MOF. The GIF score was daily evaluated in 39 critically ill patients. Amino acids were measured at the time of GID or GIF.
Results:
We enrolled 39 patients. Nine patients developed GID and 7 GIF; 6 of patients with GID/GIF developed MOF. Citrulline was lower (P < .001) in patients with GID/GIF (11.3 [4.4] µmol/L), compared to patients without GID/GIF (22.4 [6.8] µmol/L); likewise, glutamine was lower in patients with GID/GIF, whereas arginine was nonstatistically different between the 2 groups. Intra-abdominal pressure was higher in patients affected by MOF (13.0 [2.2] mm Hg) than in patients with GIF/GID without MOF (9.6 [2.6] mm Hg) and compared to patients without GID/GIF (7.2 [2.1] mm Hg).
Conclusions:
Both GID and GIF in critically ill patients are associated with low levels of citrulline and glutamine, which could be considered as markers of small bowel dysfunction. The higher the GIF score, the lower the citrulline levels. Patients affected by MOF had higher levels of intra-abdominal pressure.
Keywords
Introduction
Gastrointestinal dysfunction and failure (GID and GIF) occur frequently in patients admitted to the intensive care unit (ICU) and are associated with increased mortality. 1 –4 Both GID and GIF may promote sepsis and multiple organ failure (MOF) through various mechanisms: alteration in the gut barrier permeability with bacterial translocation into the bloodstream, abnormal activation of the gut-associated lymphoid tissue, and modification of endogenous bacterial microflora. 5,6 Although GIF could be the cause of sepsis, new insight into the comprehension of its pathophysiology suggested that the gastrointestinal (GI) system could be one of the target of septic shock, joining other organs in the MOF. Reintam and colleagues 4 proposed a GIF score and demonstrated its correlation with mortality; the ESICM Working Group on Abdominal Problems 7 defined a list of 4 severity grades for acute GID/GIF and edited recommendations for its management. Unfortunately, GID/GIF may be occult in ICU, and biomarkers that help to detect this syndrome lack strong evidence. 8 Citrulline is one of the most studied biomarkers; the levels refer to the balance between gut synthesis and kidney degradation. 9 Low levels have been associated with sepsis; only one study reported the association between GI symptoms and low plasmatic levels of citrulline. 10 Nevertheless, citrulline has never been related to an acute GID/GIF as defined by the GIF score. 4 Interestingly, glutamine, a precursor of citrulline, has been found to be an independent risk factor for mortality in critical illness. 11
The aims were to investigate (1) the association between plasma citrulline (along with glutamine and arginine) and the clinical diagnosis of GID or GIF as defined by GIF score and (2) the role of intra-abdominal hypertension (IAH) in GID/GIF and in MOF.
Materials and Methods
Design and Setting
This was a monocentric, prospective, observational study and was registered at clinicaltrials.gov NCT02520440. The study was conducted in accordance with the Declaration of Helsinki, and local ethical approval was obtained (registration number 1796/2014).
Study Population
We prospectively enrolled critically ill adult patients with expectance of ICU stay of at least 48 hours. Exclusion criteria were admission to ICU for abdominal trauma or abdominal surgery in the last 6 weeks, presence of inflammatory bowel disease, and a body mass index ≥35.
Intervention and Outcome
Patients were followed daily for the development of GIF and MOF. Gastrointestinal dysfunction was defined as a GIF score = 2 (feeding intolerance or IAH), and GIF if the score was = 3 (feeding intolerance and IAH), as proposed by Reintam and colleagues. 4 Multiple organ failure was defined according to the Sequential Organ Failure Assessment (SOFA) score and was considered present when at least 2 organs reached a SOFA score ≥3. 12
A local protocol for nutrition was applied, which included the initiation of enteral nutrition immediately within the first 24 hours from admission. Parenteral nutrition was added after 7 days, through a single central venous line, only if the enteral nutrition was not sufficient enough to reach the preset calories. Amino acid supplementation was not performed in the enrolled patients.
The following GI symptoms were evaluated daily 7 : (1) gastric residual volumes >200 mL once or 1000 mL/24 h2; (2) absence of bowel sounds; (3) vomiting or regurgitation (any amount); (4) diarrhea (loss of liquid stool ≥3 times/day); (5) bowel distension, radiologically confirmed colonic diameter above 6 cm (9 cm for caecum), or small bowel diameter above 3 cm; (6) appearance of blood in vomit, nasogastric aspirate, or stool; and (7) feeding intolerance (enteral feeding ≤20 kcal/kg/d after 72 hours). Intra-abdominal pressure (IAP) was measured using transvesical Kron’s method; IAH was defined if IAP was ≥12 mm Hg, confirmed in 2 occasions (within 6 hours). It is noteworthy that, in this series, IAH was always associated with feeding intolerance.
Citrulline, arginine, and glutamine were measured at the diagnosis of GID/GIF, median 6 (interquartile range [IQR]: 3-9.25) days after admission, or before the discharge in patients without GID/GIF, median 5 days (IQR: 4-9), by the plasma ion chromatography analyzer Biochrom 30+ (Biochrom Ltd, Cambridge, United Kingdom). The normal values provided by the manufacturer were as follows: citrulline, 12 to 55 μmol/L; arginine, 15 to 128 μmol/L; and glutamine, 205 to 756 μmol/L. Our reference values for citrulline are different from those reported in the literature in patients with normal function of the intestinal mucosa and normal renal function, which are 40 μmol/L (20-60 μmol/L). 13,14
The outcomes were the correlation of citrulline, glutamine, and arginine levels with the clinical diagnosis of GID or GIF as indicated by the GIF score 4 and the role of IAH in GID/GIF and in MOF.
Statistical Analysis
We expressed continuous variables as mean and standard deviation (SD) and discrete variables as counts and percentage. Student t test, Mann-Whitney U test, or χ2 test were used as appropriate. The analysis of variance (ANOVA; and Tukey post hoc test to locate differences) was applied for IAP among patients without GID/GIF, patients with GID/GIF without MOF, and patients with GID/GIF with MOF. The ANOVA was also used to compare citrulline levels and the different GIF score grades (0-3). Two-sided significance tests were used, and P value <.05 was considered as significant. Data were analyzed using STATA 13.0 (StataCorp, College Station, Texas).
Results
Thirty-nine patients were enrolled. Demographic characteristics, admission diagnosis, and outcomes are presented in Table 1. Two patients died in ICU, one presenting GIF and the other with GIF and MOF. Thirteen (81.2%) patients in the GID/GIF group and 14 (60.9%) patients in the other group (P > .05) were mechanically ventilated or received noninvasive ventilation.
Characteristics of the Study Patients.a
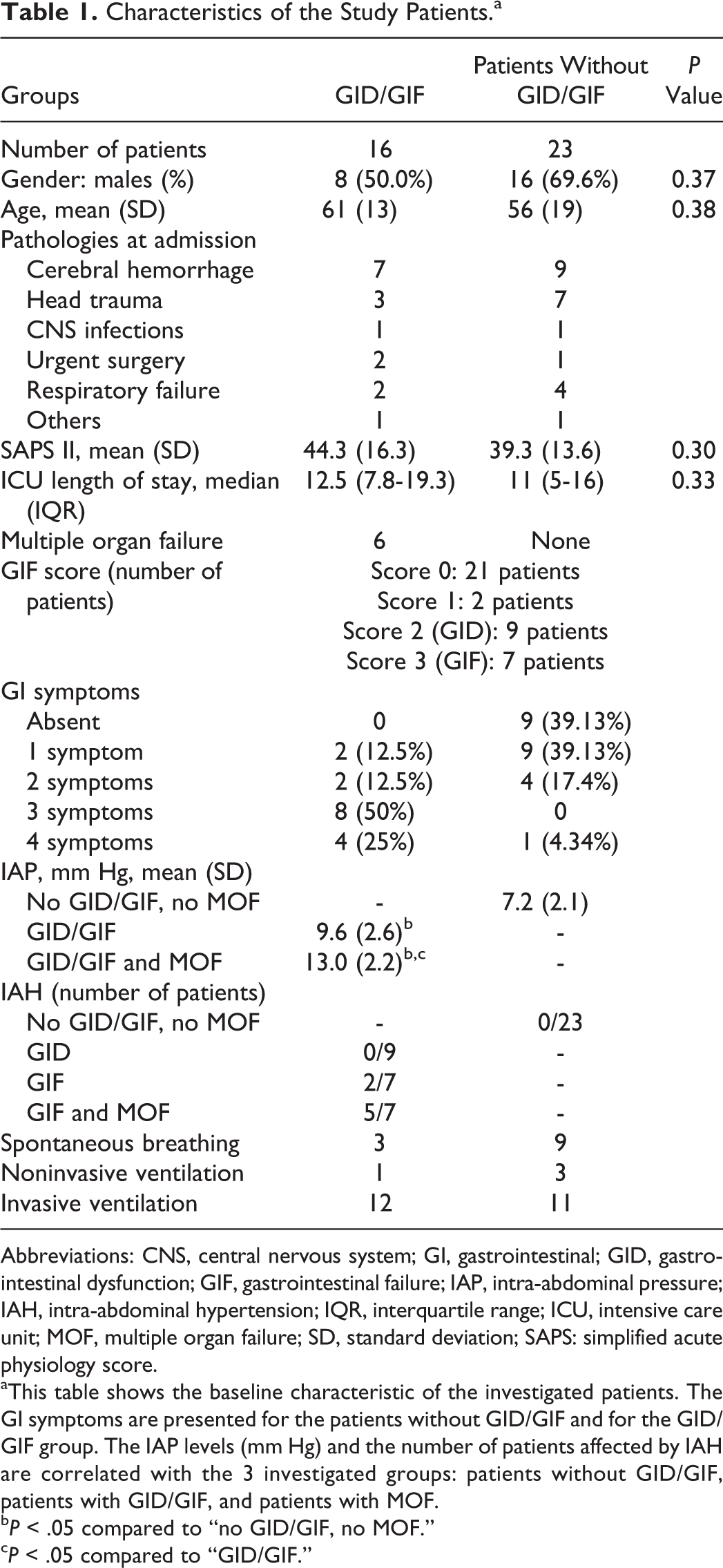
Abbreviations: CNS, central nervous system; GI, gastrointestinal; GID, gastrointestinal dysfunction; GIF, gastrointestinal failure; IAP, intra-abdominal pressure; IAH, intra-abdominal hypertension; IQR, interquartile range; ICU, intensive care unit; MOF, multiple organ failure; SD, standard deviation; SAPS: simplified acute physiology score.
aThis table shows the baseline characteristic of the investigated patients. The GI symptoms are presented for the patients without GID/GIF and for the GID/GIF group. The IAP levels (mm Hg) and the number of patients affected by IAH are correlated with the 3 investigated groups: patients without GID/GIF, patients with GID/GIF, and patients with MOF.
bP < .05 compared to “no GID/GIF, no MOF.”
cP < .05 compared to “GID/GIF.”
Nine patients developed GID and 7 GIF. Six patients with GID/GIF presented MOF: 5 of them in the GIF group and 1 in the GID group. Patients without GID/GIF did not develop MOF (P = .006 compared to GID/GIF group, 2-tailed χ2 test with the Yates correction).
Concerning the GI symptoms, 12 patients with GID/GIF presented 3 or more GI symptoms, whereas only 1 patient had 3 GI symptoms in the group of patients without GID/GIF. Seven patients developed IAH, 5 of them in the MOF group and 2 in the GIF group without MOF. Intra-abdominal pressure was higher in MOF than in patients with GIF/GID without MOF and compared to patients without GID/GIF.
Figure 1 shows plasmatic amino acid levels. In the GID/GIF group, citrulline was below the normal range and lower (P < .001) than patients without GID/GIF (mean [SD]: 11.3 [4.4] vs 22.4 [6.8] µmol/L). Citrulline values in patients with GID/GIF are abnormal, considering both our local laboratory reference values (12-55 μmol/L) and international reference values (40 μmol/L, range: 20-60 μmol/L). 13,14 Likewise, values in patients without GID/GIF are within the normal range, considering both local and international reference values.
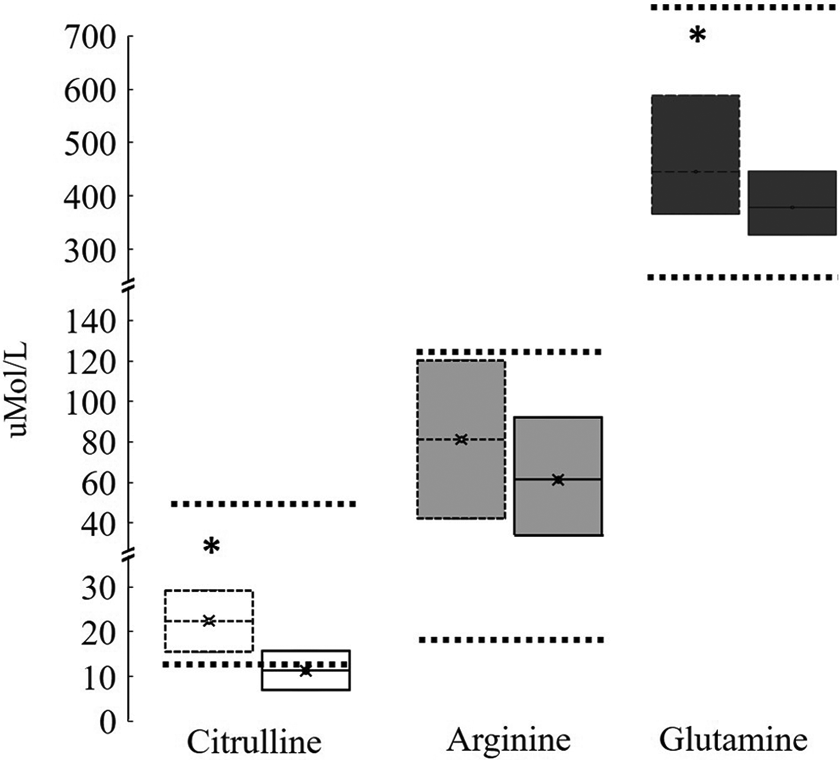
Plasmatic levels of the investigated amino acids. The graph shows the plasmatic levels of citrulline (white box), glutamine (dark gray box), and arginine (light gray box). Boxes on the left (dashed line) refer to patients without gastrointestinal dysfunction/failure (GID/GIF). Boxes on the right (continuous line) refer to patients affected by GID/GIF. Each box reports the mean value and the 95% confidence interval (95% CI). Dot lines: Reference values for each amino acid provided by the local laboratory (see text for absolute reference laboratory values). *P < .05 compared to patients with GID/GIF.
In patients with normal intestinal mucosa function and normal renal function, the plasma citrulline concentration is 40 μmol/L (20-60 μmol/L). 13,14 Despite this range is different compared to the reference value provided in the Methods session, citrulline was below both ranges in patients with GID/GIF (11.3 μmol/L), and within both ranges for patients without GID/GIF (22.4 μmol/L). In Figure 1, the reported dot lines represent the concentration range of amino acids provided by the laboratory which performed the analysis.
Glutamine was lower (P < .05) in patients with GID/GIF compared to the other group (median [IQR]: 395 [350-454] μmol/L vs 453 [384-577] μmol/L), whereas arginine was not different between groups (mean [SD]: 64 [28] μmol/L vs 82 [36] μmol/L; P = .098). Furthermore, the level of citrulline decreased with the higher GIF score levels (0 = 22.2, 1 = 24.5, 2 = 12.6, 3 = 9.6 μmol/L; P < .001; Figure 2).
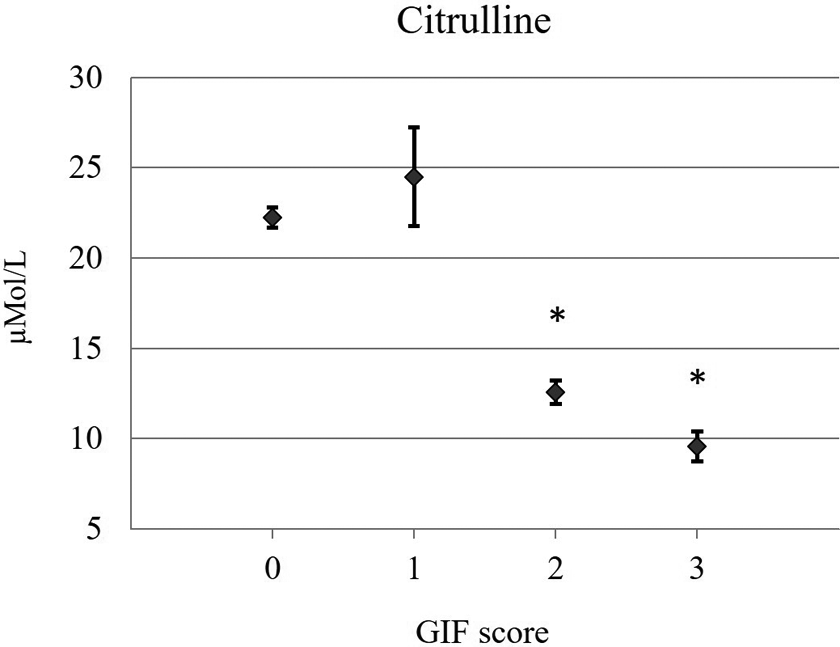
Plasmatic levels of citrulline. Plasmatic citrulline concentration according to the gastrointestinal failure (GIF) score. Diamonds: mean values; bars: standard errors. Data are presented in the text. *P < .05 compared to GIF score 0 and GIF score 1.
Discussion
The results demonstrate that (1) citrulline is lower in patients with GIF/GID compared to patients without GID/GIF; (2) the higher the GIF score, the lower the level of citrulline; (3) glutamine is lower in the GIF/GID group compared to the other (although within the normal reference values); (4) MOF is prevalent in patients with a GIF score = 3; and (5) IAH develops predominantly in patients with MOF.
This is the first study investigating the relationship between the GIF score as proposed by Reintam and colleagues in 2008 and the plasmatic levels of citrulline, glutamine, and arginine. 4 Noordally and colleagues 10 found lower levels of citrulline in critically ill patients with an intestinal dysfunction, diagnosed with the presence of at least 1 GI symptom (feeding intolerance, ileus, diarrhea, GI bleeding, or intestinal ischemia), compared to patients without intestinal dysfunction (mean: 16.3 and 23.9 µmol/L, respectively); other authors reported the role of citrulline as a marker of GID/GIF, although few of them refer to ICU patients. 3,10
This study confirms the 2 alternative explanations regarding the low level of citrulline in GID/GIF: (1) low levels of glutamine found in patients with GID/GIF and low levels of citrulline in patients with GID/GIF could be explained by a reduction in citrulline synthesis from glutamine by the impaired mitochondrial of small bowel enterocytes, as previously demonstrated, and (2) even if not significant (possibly due to the low number of patients in our study), we also found a trend in reduction of arginine in patients with GID or GIF. In fact, citrulline is considered to be a masked form of arginine, because it is not taken up by the liver but rather transformed by the kidney into arginine. 9
Moreover, plasmatic levels of citrulline could reflect the severity of GID/GIF along with the presence of an increased IAP; patients with MOF had a higher GIF score, and all the patients with MOF except 2 had IAH (Table 1). This results in a higher risk of developing IAH for patients with MOF compared to patients without MOF. Since the IAH is one of the parameter to diagnose GIF, GIF might be responsible for a complex inflammatory status that leads to MOF (“gut hypothesis”). 5,6 The diagnoses of GID were always based on the presence of feeding intolerance and not on the presence of IAH, and hence, all patients with IAH also had feeding intolerance. The association between IAH and poor tolerance to enteral feeds is already reported in the literature, 15 and although the possibility to feed patients with IAH exists, the level of nutrition in those patients does not achieve the full nutritional request. 16 In larger series, few patients with IAH did not develop GI symptoms and had a better outcome. 17
Soler Morejón and Tamargo Barbeito 18 found that the increment in IAP was higher in mechanically ventilated patients compared to patients in spontaneous breathing (IAH in 6/50 patients mechanically ventilated and none in the group not ventilated). In our series, a higher percentage of patients were mechanically ventilated in the GID/GIF group compared to the patients without GID/GIF, although not statistically significant, and the absolute number of patients ventilated was similar in the 2 groups.
A recent multicenter study failed to demonstrate that a GI score adds significant additional information to predict 28-day mortality compared to the SOFA score. 19 Nevertheless, we speculate that both citrulline and IAP, already part of GI score, may represent 2 parameters that might be considered to assess the intestinal derangement during MOF and to ameliorate the predictability of the SOFA score.
Conclusions
Low plasmatic levels of citrulline are related to GID/GIF, the higher the level of GIF score, the lower the level of citrulline. Intra-abdominal pressure is an easy to assess parameter, increased in patients with MOF. Larger studies are required in order to develop a GI score capable of improving the SOFA score based on laboratory biomarkers such as citrulline.
Footnotes
Authors’ Note
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. Nazzareno Fagoni, Simone Piva, and Nicola Latronico wrote manuscript, performed analysis on data, and acted as corresponding author. Nazzareno Fagoni, Nicola Latronico, Simone Piva, Frank Rasulo, and Rosella Marino concepted and designed the study, supervised development of work, and helped in data interpretation and manuscript evaluation. Giovanni Chiarini, Daniela Ferrari, Eleonora Grespi, Rita Bertuetti, and Silvia Barbieri helped in acquisition of data and performed analysis on data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.