
Abstract
Background:
Although the quick Sequential Organ Failure Assessment (qSOFA) has been recommended for identifying patients at higher risk of hospital death, it has only a 60% sensitivity for in-hospital mortality. On the other hand, hypothermia associates with increased mortality and organ failure in patients with sepsis. This study aimed to assess the predictive validity of qSOFA for identifying patients with sepsis at higher risk of multiple organ dysfunction or death and the complementary effect of hypothermia.
Methods:
Patients with severe sepsis admitted to intensive care units (ICUs) were retrospectively analyzed. The predictive validities of qSOFA (≥2, positive) and the complementary effect of hypothermia (body temperature ≤36.5°C) for the identification of death or multiorgan dysfunction were evaluated.
Results:
Of the 624 patients, 230 (36.9%) developed multiorgan dysfunction and 144 (23.1%) died within 28 days; 527 (84.5%) had a positive qSOFA. The 28-day mortality rates of patients with positive and negative qSOFA were 25.4% and 10.3%, respectively (P = .001). The rate of positive qSOFA was higher in patients with multiorgan dysfunction (sensitivity, 0.896; specificity, 0.185) and among patients who died within 28 days (sensitivity, 0.931; specificity, 0.181); 10 (6.9%) of 144 deaths were not identified. In cases of positive qSOFA without hypothermia, positive qSOFA + hypothermia, or negative qSOFA with hypothermia, the predictive value for 28-day mortality improved (sensitivity, 0.979). Among the 144 patients who died, only 3 were not identified.
Conclusion:
A qSOFA score ≥2 may identify >90% of 28-day deaths among patients with severe sepsis; hypothermia may complement the predictive ability of qSOFA.
Introduction
The definitions of sepsis and septic shock were recently modified in the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). 1 In these definitions, a novel screening tool, the quick Sequential Organ Failure Assessment (qSOFA), was recommended for evaluating sepsis in accordance with its new definition. 1 The qSOFA criteria for sepsis consist of altered mental status, systolic blood pressure ≤100 mm Hg, and a respiratory rate ≥22 breaths/min. 2 A score of ≥2 showed a sensitivity for in-hospital mortality of >60% in a validation cohort including both intensive care unit (ICU) and non-ICU patients. This scoring system was found to perform better than the SOFA score in predicting in-hospital mortality in settings other than the ICU. 2 Simple recognition and close accordance to other complex systems are some of the advantages of screening using qSOFA. 3 The qSOFA was first introduced as a tool for identifying patients at risk of sepsis with a higher risk of hospital death or prolonged ICU stay both inside and outside the ICU. 4 However, a score of ≥2 showed a sensitivity of only approximately 60% for in-hospital mortality in a previous study, and a third of patients with sepsis at high risk of mortality may not be identified.
Body temperature is a routinely measured vital sign in all patients in the emergency department and wards, and body temperature abnormalities are among the most commonly noted symptoms in critically ill patients. Moreover, these abnormalities frequently trigger changes in the patient management. 5,6 We previously demonstrated that hypothermia was associated with increased mortality and organ failure in patients with sepsis, irrespective of the presence of septic shock. 7
Regardless of that background, the relationship between qSOFA and the presence of hypothermia and their combined effect on identifying infected patients with high risk of mortality have not yet been evaluated in unrestricted situations, that is, both inside and outside the ICU.
The objective of this study was to assess the predictive validity of qSOFA for identifying patients with sepsis at a higher risk of multiple organ dysfunction or death and to assess the complementary effect of hypothermia evaluation on the prediction.
Methods
Study Design and Data Source
This was a retrospective analysis conducted as a part of a multicenter prospective evaluation of severe sepsis in Japan, undertaken by the Japanese Association for Acute Medicine Sepsis Registry Study Group. 7 –9 Both the Japanese Association for Acute Medicine and the Ethics Committees of the participating hospitals approved the study protocol. Data collection was performed as part of the routine clinical examinations and did not require additional medical intervention. Data management and statistical analyses were processed anonymously. For these reasons, the need for written informed consent was waived by both the Japanese Association for Acute Medicine and the Ethics Committees of the participating hospitals.
Patients
Between June 1, 2010, and May 31, 2011, we enrolled 624 patients in this study. All patients were diagnosed as having severe sepsis and were admitted to 1 of 15 ICUs of critical care centers in tertiary care hospitals in Japan. There were no exclusion criteria.
Definitions
Severe sepsis, septic shock, and systemic inflammatory response syndrome (SIRS) were defined according to the American College of Chest Physicians/Society of Critical Care Medicine consensus conference and its revised version from 2003. 10,11 The severity of illness was evaluated according to the Acute Physiology and Chronic Health Evaluation (APACHE) II score at the time of enrollment. 12 Organ dysfunction was assessed according to the SOFA score. 13 Multiple organ dysfunction syndrome (MODS) was defined as a SOFA score ≥12 as described previously. 7 –9,14,15 For the definition of acute increase of SOFA ≥2, baseline SOFA score of 0 was assumed in patients without chronic diagnosis defined per APACHEII. If present, baseline SOFA score of 2 was assigned, as similar to methods used in a previous study. 16 A diagnosis of disseminated intravascular coagulation was made based on the scoring system of the International Society on Thrombosis and Hemostasis. 17 Changes in the fibrin/fibrinogen degradation product were used as a fibrin-related marker, according to the International Society on Thrombosis and Hemostasis criteria. Fibrin/fibrinogen degradation product values of <10, ≥10 but <25, and ≥25 mg/L were defined as no, moderate, and strong increases, respectively. The outcome measures were the 28-day mortality and development of MODS.
Quick SOFA
The “quick SOFA” (qSOFA) score consisted of altered mental status, systolic blood pressure ≤100 mm Hg, and respiratory rate ≥22 breaths/min. 1 In this study, we defined “altered mental status” as a Glasgow coma scale <15. 1,2 The qSOFA was defined as positive for ≥2 and negative for <2.
Body Temperature
Body temperature (Tb) was recorded as the measured value using the method recommended by the American College of Critical Care Medicine and the Infectious Diseases Society of America. 6 Although many previous studies considered 35.5°C as the threshold for hypothermia, 18 –22 we opted to use 36.5°C as the threshold in the present study, because significant differences in the mortality of patients with Tb ≤36.5°C versus >36.5°C were observed in a previous analysis. 7
Statistical Analysis
Data are expressed as the median and interquartile range or number (percentage). Comparisons between 2 groups were performed using the Mann-Whitney U test, and categorical variables were summarized using proportions and compared between the groups using the Pearson chi-square test. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic odds ratios (ORs) were reported along with the 95% confidence intervals (CIs). Receiver–operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic accuracy of each variable. Survival curves were created using the Kaplan-Meier method and compared using the Log-rank test. The independent association of qSOFA and Tb ≤36.5°C with mortality was assessed using logistic regression analysis (forced entry method), using a qSOFA score of ≥2, Tb ≤36.5°C, age, and site of infection as the explanatory variables and 28-day mortality as the categorical outcome. Before multivariate analysis, the variance inflation factor for each explanatory variable was calculated. For all explanatory variables, the variance inflation factor was <5. To assess the complementary effect of hypothermia, predictive ability of qSOFA with Tb ≤36.5°C in addition to Tb ≤36.5°C without qSOFA ≥2 was evaluated. The area under the ROC curve (AUROC) for each score, including qSOFA, qSOFA and Tb ≤36.5°C, SIRS, SOFA for MODS, and 28-day mortality, was also evaluated. All statistical analyses were performed using SPSS 23.0 for Windows (SPSS, Chicago, Illinois). For all analyses, differences with a P value of <.05 were considered statistically significant.
Results
Baseline Characteristics and Outcomes of the Enrolled Patients
During the 1-year study period, a total of 14 417 patients were admitted to the 15 participating critical care centers; of these, 624 (4.3%) patients were diagnosed with severe sepsis and enrolled in this study. The characteristics at enrollment and outcomes of the patients are shown in Table 1. The median age was 72 years, and the median initial APACHE II and SOFA scores were 23 and 8, respectively. The major sites of infection were pulmonary, intra-abdominal, urinary, and skin/soft tissue. More than half of the patients had dysfunction of 3 or more organ systems. The 28-day and overall hospital mortality rates were 23.1% and 29.5%, respectively. The sepsis-related hospital mortality rate was 25.6% (160/624).
Baseline Characteristics and Outcomes of the Enrolled Patients.a
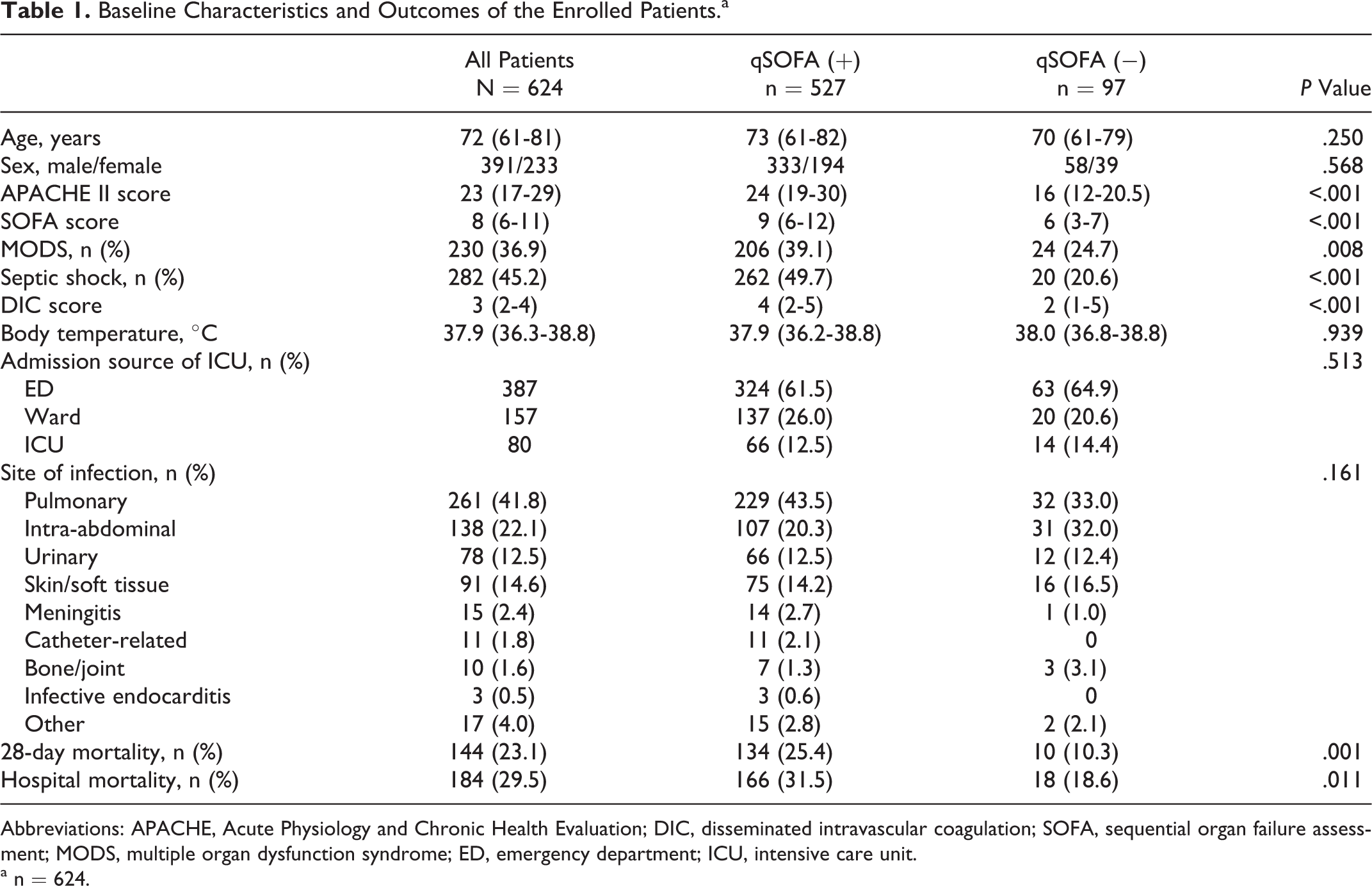
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; DIC, disseminated intravascular coagulation; SOFA, sequential organ failure assessment; MODS, multiple organ dysfunction syndrome; ED, emergency department; ICU, intensive care unit.
a n = 624.
Of the total 624 patients with severe sepsis, 527 (84.5%) had a qSOFA score ≥2, defined as “positive qSOFA.” Although the median age and proportion of men were not different between patients with positive and negative qSOFAs, the APACHE II, and disseminated intravascular coagulation scores, the rates of multiple organ dysfunction and septic shock were significantly higher among patients with positive qSOFA. The 28-day mortality rates of patients with positive and negative qSOFAs were 25.4% and 10.3% (P = .001), respectively, and the overall hospital mortality rates were 31.5% and 18.6%, respectively (P = .011).
Predictive Value of qSOFA for Patients With Severe Sepsis at High Risk of Multiple Organ Dysfunction and 28-Day Mortality
We evaluated the predictive validities of qSOFA for the development of MODS on day 1 and/or day 4 of enrollment and the 28-day mortality (Table 2).
Performance of qSOFA in Predicting the Development of MODS and 28-day Mortality.
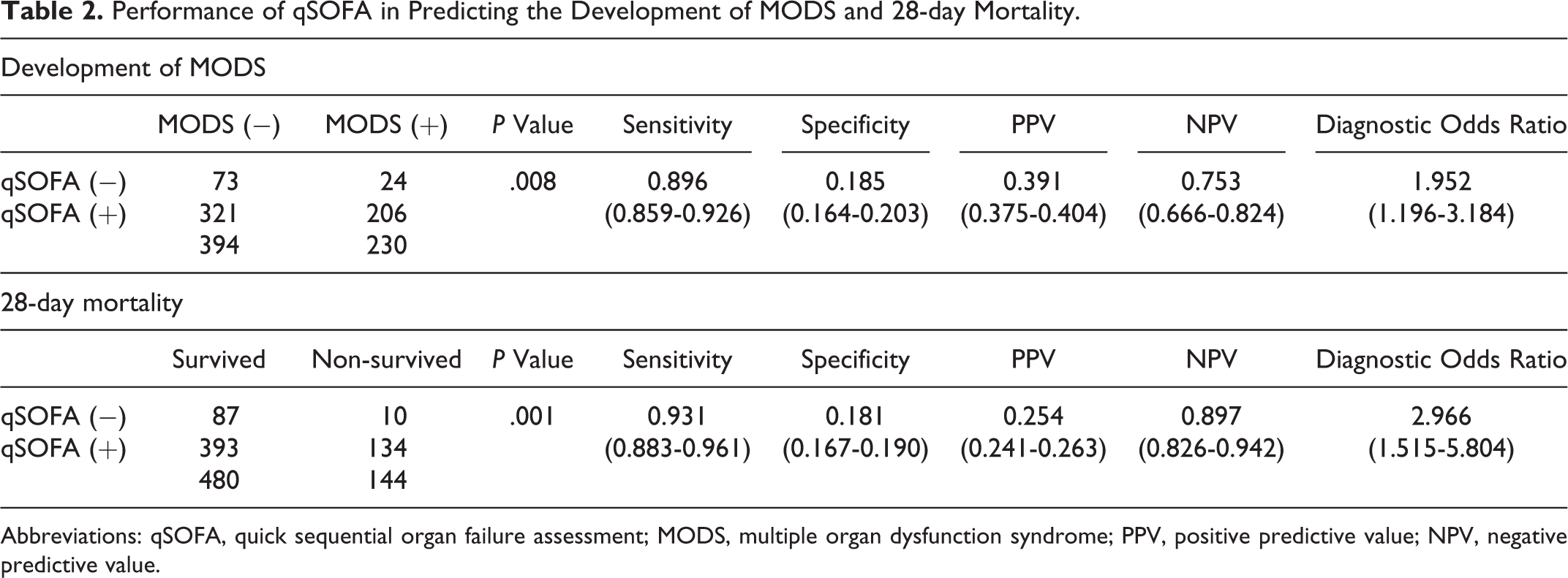
Abbreviations: qSOFA, quick sequential organ failure assessment; MODS, multiple organ dysfunction syndrome; PPV, positive predictive value; NPV, negative predictive value.
The rate of patients with a qSOFA score ≥2 was significantly higher in patients with MODS (P = .008), with a sensitivity, specificity, PPV, and NPV of 0.896 (95% CI, 0.859-0.926), 0.185 (0.164-0.203), 0.391 (0.375-0.404), and 0.753 (0.666-0.824), respectively. However, 24 (10.4%) of 230 patients with development of MODS were not identified by qSOFA. The AUROC of qSOFA for the prediction of MODS was 0.615 (95% CI, 0.570-0.660).
The rate of patients with a qSOFA score ≥2 was significantly higher in patients who died within 28 days (P = .001), with a sensitivity, specificity, PPV, and NPV of 0.931 (95% CI, 0.883-0.961), 0.181 (0.167-0.190), 0.254 (0.241-0.263), and 0.897 (0.826-0.942), respectively. However, 10 (6.9%) of 144 patients who died within 28 days were not identified with qSOFA. The AUROC of qSOFA for the prediction of 28-day mortality was 0.622 (95% CI, 0.571-0.674).
Complementary Effect of Hypothermia (Tb ≤36.5°C) on qSOFA, SIRS, and Increase in SOFA ≥2 to Predict Patients With Severe Sepsis at High Risk of Multiple Organ Dysfunction or Mortality
We evaluated the supplementary predictive values of Tb ≤36.5°C on qSOFA for the development of MODS on day 1 and/or day 4, in addition to 28-day mortality. We also assessed the predictive ability of SIRS and increase in SOFA ≥2.
The rate of patients with Tb ≤36.5°C was significantly higher in patients with MODS (P < .001), with a sensitivity, specificity, PPV, and NPV of 0.361 (95% CI, 0.315-0.406), 0.805 (0.778-0.831), 0.519 (0.453-0.583), and 0.681 (0.661-0.705), respectively. However, 147 (63.9%) of 230 patients with the development of MODS were not identified by the criterion of Tb ≤36.5°C.
The rate of patients with Tb ≤36.5°C was also significantly higher in patients with 28-day mortality (P < .001), with a sensitivity, specificity, PPV, and NPV of 0.424 (95% CI, 0.357-0.490), 0.794 (0.774-0.814), 0.381 (0.322-0.441), and 0.821 (0.801-0.842), respectively. However, 83 (57.6%) of 144 patients with 28-day mortality were not identified by Tb ≤36.5°C (Table 3).
Performance of Tb ≤36.5°C in Predicting the Development of MODS and 28-Day Mortality.
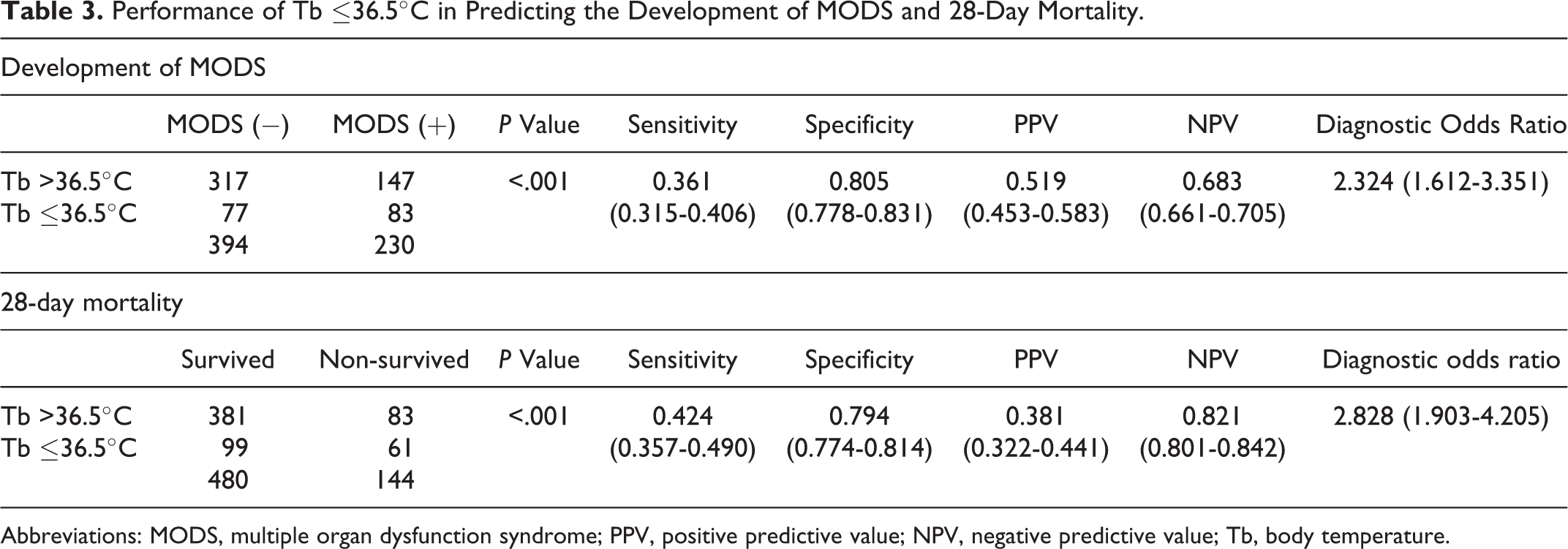
Abbreviations: MODS, multiple organ dysfunction syndrome; PPV, positive predictive value; NPV, negative predictive value; Tb, body temperature.
While no change was observed in predicting the development of MODS (Table 4), if qSOFA and/or Tb ≤36.5°C was present, the predictive value for 28-day mortality improved as determined by an increased sensitivity, NPV, and diagnostic OR. Among the 144 patients who died within 28 days, only 3 patients were not identified as being at high risk of 28-day death by qSOFA and/or Tb ≤36.5°C, with a sensitivity of 0.979 and NPV of 0.961 (Table 5).
Performance of qSOFA and/or Tb ≤36.5°C, SIRS ≥2, and Increase of SOFA ≥2 in Predicting MODS in Patients With Severe Sepsis.
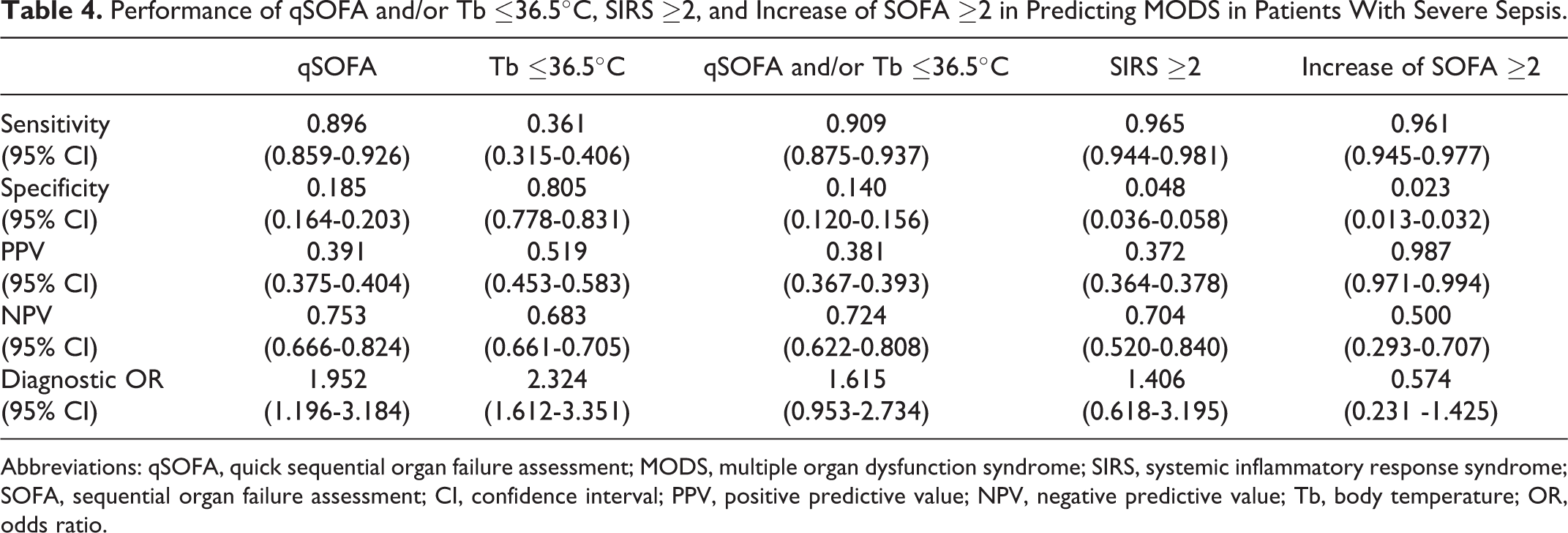
Abbreviations: qSOFA, quick sequential organ failure assessment; MODS, multiple organ dysfunction syndrome; SIRS, systemic inflammatory response syndrome; SOFA, sequential organ failure assessment; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; Tb, body temperature; OR, odds ratio.
Performance of qSOFA and/or Tb ≤36.5°C, SIRS≥2, and Increase of SOFA≥2 in Predicting 28-day Mortality in Patients With Severe Sepsis.
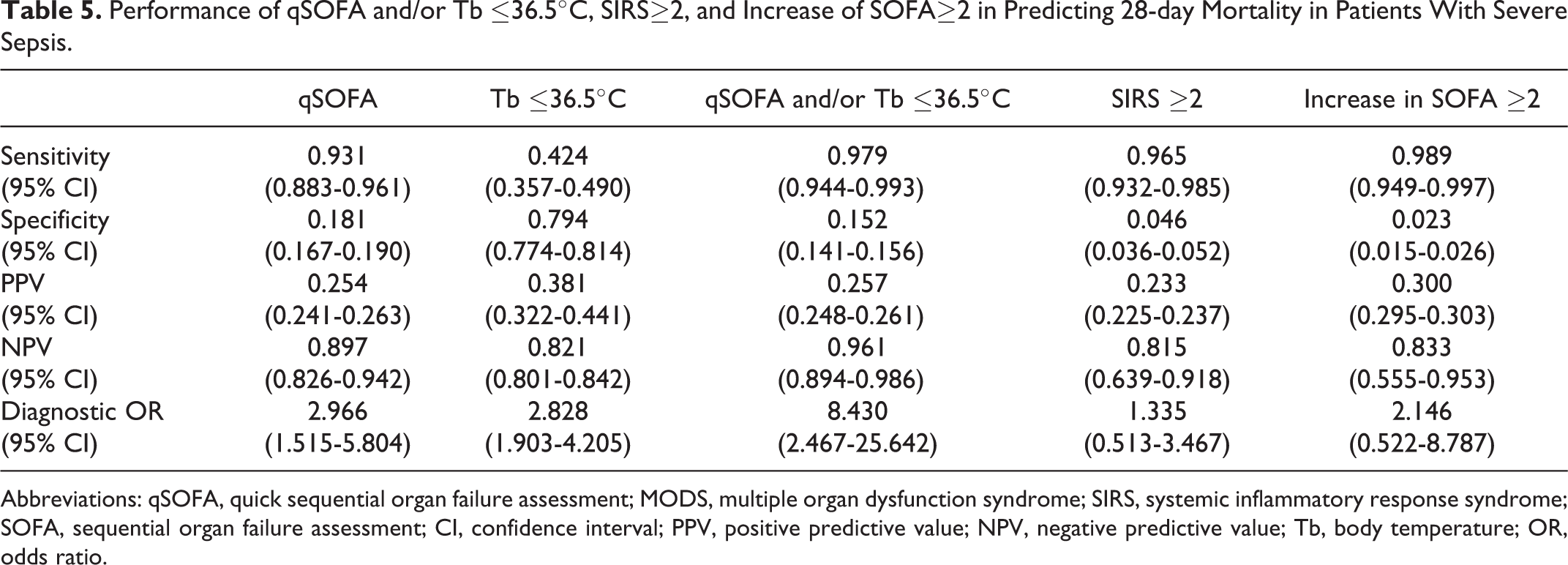
Abbreviations: qSOFA, quick sequential organ failure assessment; MODS, multiple organ dysfunction syndrome; SIRS, systemic inflammatory response syndrome; SOFA, sequential organ failure assessment; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; Tb, body temperature; OR, odds ratio.
Although SIRS ≥2 and an increase in SOFA ≥2 showed sensitivity >0.9 for the development of MODS, they had specificity of <0.1 and less than 2 of diagnostic OR (Table 4). SIRS ≥2 and an SOFA increase ≥2 also showed sensitivity more than 0.9, with specificity <0.1 and PPV of <0.3 for the prediction of 28-day mortality (Table 5).
Predictive ability of qSOFA, qSOFA with hypothermia, SIRS, and SOFA scores for the prediction of patients with severe sepsis at high risk of multiple organ dysfunction or mortality were also evaluated using AUROC for each score individually (Figure 1). Although the superior predictive performance of SOFA over other variables for MODS or 28-day mortality was observed, the AUROCs of qSOFA with Tb ≤36.5°C for both MODS and 28-day mortality were higher than those of qSOFA alone (0.645 [95% CI, 0.600-0.691] vs 0.604 [0.558-0.649]; 0.662 [0.613-0.711] vs 0.611 [0.560-0.662], respectively).
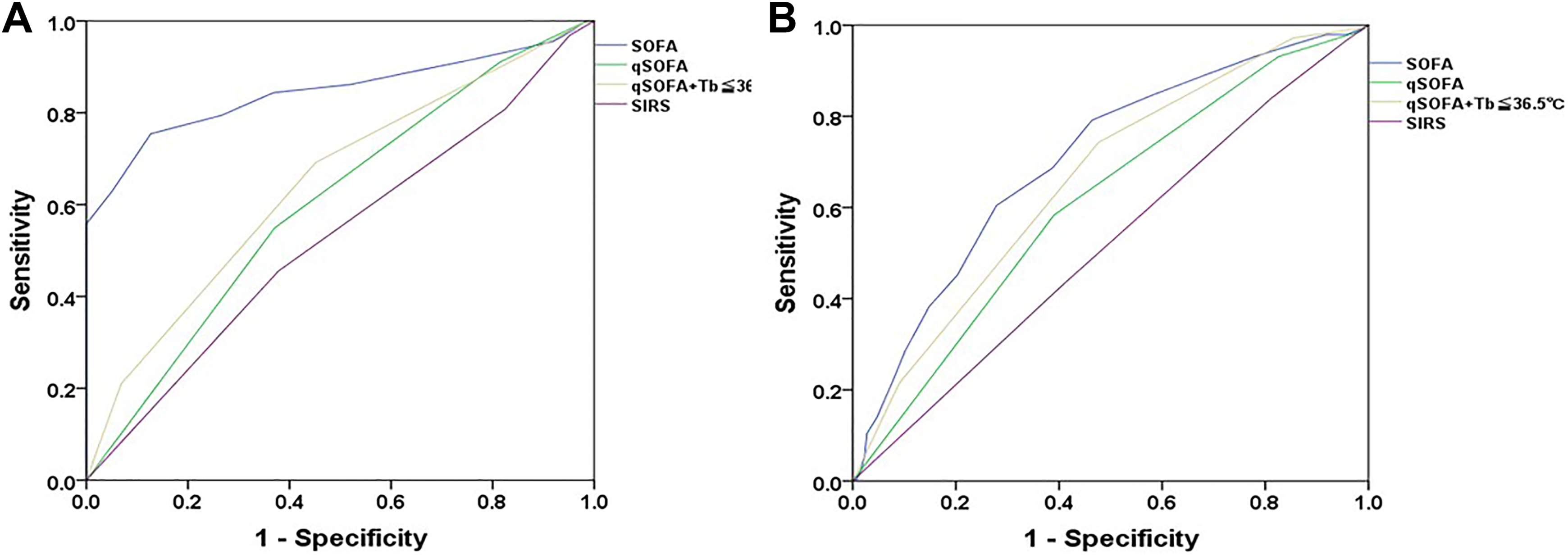
Area under the receiver–operating characteristic curves (AUROCs) of predictive ability for multiple organ dysfunction syndrome or 28-day mortality using qSOFA, qSOFA with Tb ≤36.5°C, SIRS criteria, and SOFA score on ICU admission. ICU indicates intensive care unit; qSOFA, quick sequential organ function assessment; Tb, body temperature; SIRS, systemic inflammatory response syndrome; SOFA, sequential organ function assessment. A, AUROCs for multiple organ dysfunction syndrome qSOFA, 0.604 (95% confidence interval [CI], 0.558-0.649); qSOFA with Tb ≤36.5°C, 0.645 (95% CI, 0.600-0.691); SIRS, 0.528 (95% CI, 0.481-0.576); SOFA, 0.845 (95% CI, 0.807-0.883). B, AUROCs for 28-day mortality qSOFA, 0.611 (95% CI, 0.560-0.662); qSOFA with Tb ≤36.5°C, 0.662 (95% CI, 0.613-0.711); SIRS, 0.518 (95% CI, 0.465-0.571); SOFA, 0.705 (95% CI, 0.658-0.753).
Association of qSOFA and/or Tb ≤36.5°C With Mortality in Patients With Sepsis
In the survival analysis, extended survival was observed in patients with a qSOFA score <2 versus ≥2 (Log-rank test, P = .021; Figure 2A). Patients with sepsis with a positive qSOFA and/or Tb ≤36.5°C had significantly worse survival compared to those with negative qSOFA and/or Tb ≤36.5°C (P = .001; Figure 2B).
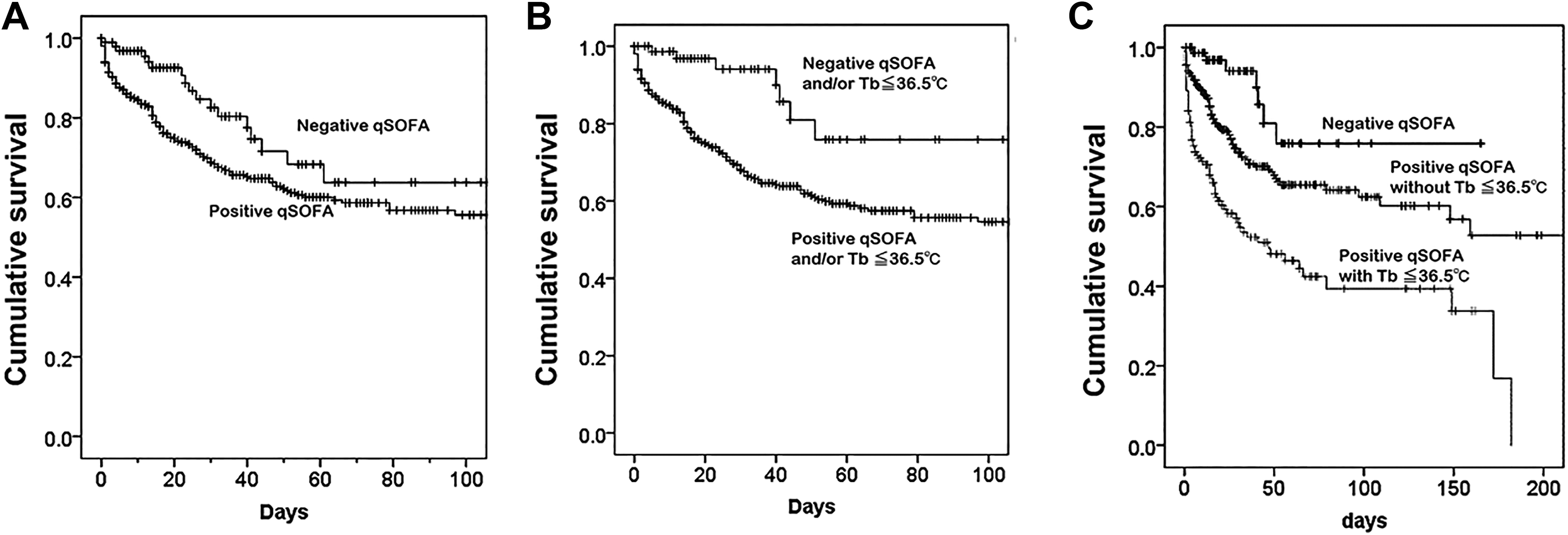
Kaplan-Meier curves for patient survival. A, Kaplan-Meier survival curves for patients with negative (<2) versus positive qSOFA (≥2). Log-rank (Mantel-Cox) P = .021. B, Kaplan-Meier survival curves for patients with positive qSOFA and/or Tb ≤36.5°C versus patients with negative qSOFA and/or Tb ≤36.5°C. Log-rank (Mantel-Cox) P = .001. C, Kaplan-Meier survival curves for patients with (a) negative qSOFA versus (b) positive qSOFA without Tb ≤36.5°C versus (c) positive qSOFA with Tb ≤36.5°C. Log-rank (Mantel-Cox): a versus b, P = .008; c versus a, b, P < .001. qSOFA indicates quick sequential organ failure assessment; Tb, body temperature.
In the comparison between patients with a qSOFA score <2 versus ≥2 and without Tb ≤36.5°C or a score ≥2 with Tb ≤36.5°C, patients with both a qSOFA score ≥2 and Tb ≤36.5°C had significantly worse survival (P < .001 for all; Figure 2C).
A logistic regression analysis was performed using a qSOFA score ≥2, Tb ≤36.5°C, age, source of sepsis, and site of infection as explanatory variables and 28-day mortality as the categorical outcome. The results revealed that qSOFA and Tb ≤36.5°C were independently associated with the 28-day mortality (Table 6).
Logistic Regression Analysis of the Factors Associated With 28-Day Mortality.
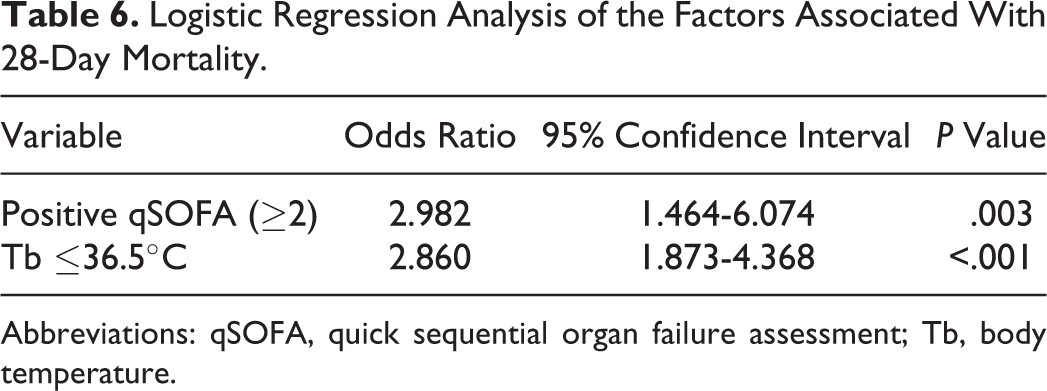
Abbreviations: qSOFA, quick sequential organ failure assessment; Tb, body temperature.
Discussion
In this study, we demonstrated that more than 80% of patients with sepsis having organ dysfunction had a qSOFA score ≥2 (“positive qSOFA”) and that qSOFA could identify 28-day mortality in more than 90% of cases among these patients with sepsis. Moreover, our findings indicate that the predictive validity for mortality of qSOFA may be complemented by adding Tb ≤36.5°C, resulting in a sensitivity of more than 95%.
It has been demonstrated that patients with a qSOFA score ≥2 are at a significantly greater risk of having a prolonged ICU stay or in-hospital mortality. 2 For these patients, clinicians are required to perform additional assessments for organ dysfunction, initiate or escalate therapy as appropriate, and consider referrals to critical care specialists or increasing the frequency of monitoring. 23 In one previous study, as a means to evaluate the validity of clinical criteria for identifying patients with suspected infection at risk of sepsis, patients with suspected infection from a large, multicenter database were analyzed. 2 The authors reported that patients with a positive qSOFA accounted for 24% of cases with infection and 70% of deaths or ICU stays of ≥3 days in the derivation cohort. The analysis further demonstrated that 70% of decedents had a qSOFA score ≥2, while 78% of survivors had a score <2. 2 Further, an infographic regarding qSOFA by the Society of Critical Care Medicine reported that 1 in 4 infected patients have a qSOFA score ≥2 and that such cases account for 3 of 4 deaths. 24
Although the superiority of qSOFA has been demonstrated outside the ICU, qSOFA is independent of laboratory test results and can be evaluated within a minute at any patient’s bedside. The simplicity and repeatability as a tool for the identification of patients could be useful both inside and outside the ICU. 4 Therefore, we evaluated its predictive ability for the development of MODS and 28-day mortality among patients admitted to the ICU, as Raith et al reported. 16
Although fever may not always be associated with an increased risk of mortality in patients with sepsis, hypothermia may be associated with an increased risk of mortality in patients with sepsis, 25 –28 as evidenced by previous large trials. 18,19,21,22,29 A recent retrospective study with data from Australia, New Zealand, and the United Kingdom reported that an elevated peak body temperature in the first 24 hours after ICU admission was associated with decreased in-hospital mortality in patients with infection. 25 The lowest mortality risk was found among patients with a temperature between 39°C and 39.4°C. Similarly, the Fever and Antipyretic in Critically Ill Patients Evaluation Study observed a trend of decreased 28-day mortality in patients with sepsis having temperatures ≥39.5°C. 30 In addition, the incidences of hypothermia (defined as <35.5°C) were 9% in the Methylprednisolone Severe Sepsis Study, 10% in the Veterans Administration Systemic Sepsis Cooperative Study of Glucocorticoid Therapy, and 9.6% in the Ibuprofen Sepsis Study; all of these studies only included patients with severe sepsis. The incidences of 28- or 30-day mortality in patients with hypothermia compared to those without hypothermia in these studies were 62% versus 26%, 57% versus 28%, and 70% versus 35%, respectively. The incidence of hypothermia in the NORASEPT II study, in which only patients with septic shock were included, was 21%; the mortality rates in patients with and without hypothermia were 59% and 34%, respectively. 18,19,22,29 The findings of a recent study are also consistent with these results. We found that hypothermia, defined as Tb ≤36.5°C, accompanied sepsis in approximately 10% of patients and was significantly associated with a 2-fold increased risk of mortality compared to patients without hypothermia. 7
While we opted to use 36.5°C as the threshold temperature for hypothermia based on the findings of our previous analysis in this study, Tb <36.0°C is a widely recognized value for hypothermia as SIRS criteria. If Tb <36.0°C was applied in this analysis, the number of patients with hypothermia decreased to 135 (Tb ≤36.5°C: n = 160), with slight decrease in sensitivity and increase in specificity to both MODS and 28-day mortality by hypothermia. However, the performance of qSOFA and/or Tb <36.0°C in predicting the development of MODS and 28-day mortality were quite similar with those of qSOFA and/or Tb ≤36.5°C; sensitivity, specificity, PPV, and NPV for MODS were 0.909 (95% CI, 0.875-0.937), 0.145 (0.125-0.161), 0.383 (0.368-0.395), and 0.731 (0.631-0.814), respectively and for 28-day mortality were 0.979 (95% CI, 0.944-0.993), 0.156 (0.146-0.161), 0.258 (0.249-0.262), and 0.962 (0.896-0.987), respectively. Among the 144 patients who died within 28 days, only 3 patients were not identified as being at high risk of 28-day death similar to qSOFA and/or Tb ≤36.5°C.
Although we recorded the measured value of Tb using the method recommended by the American College of Critical Care Medicine and the Infectious Diseases Society of America, appropriate Tb for evaluating the prognosis in patients with sepsis has not been determined. Further study is required to evaluate the method, timing, and changes in Tb.
The present study examined the predictive ability of qSOFA for the development of MODS and 28-day mortality in patients with severe sepsis admitted to the ICU; however, it did not evaluate the characteristics including long-term evaluable simplicity or rapidity. Therefore, these recommended features of qSOFA could not be adequately assessed. Despite the proposed utility of qSOFA for identifying high-risk infected patients outside the ICU, the sensitivity of the qSOFA criteria to identify such patients may not be sufficient. However, the present study demonstrated that the qSOFA criteria identified more than 90% of 28-day deaths among patients with sepsis having organ dysfunction. Hence, qSOFA may be more useful for identifying patients with severe sepsis at high risk of death than reported in the previous validation analyses. Moreover, our findings indicate that the predictive validity of qSOFA may be complemented with Tb ≤36.5°C, resulting in a sensitivity of >95% in patients with sepsis having organ dysfunction.
Limitations
There are some limitations to our study. First, this was a retrospective study based on short-term data from a limited population of patients with severe sepsis based on previous definitions. 10,11 Also, approximately two-third of patients was consisted with pulmonary and intra-abdominal infections that may affect the results of the present study. Therefore, proposed role of qSOFA as a screening criteria for sepsis may not be evaluated appropriately. Second, Tb was recorded within 24 hours of a diagnosis of severe sepsis as the highest Tb value used for the APACHE II score, without a standardized method. Third, all patients included in this study were diagnosed with severe sepsis. Core criteria for enrollment was a diagnosis of SIRS (SIRS score of ≥2: 597 patients, 95.7%), and the majority of patients had some organ dysfunction (increase in SOFA score of ≥2: 595 patients, 95.4%). Therefore, the comparison between SIRS and increased SOFA scores may have limited value.
Conclusion
The findings of the present study support the use of qSOFA as a tool for identifying patients with sepsis at a higher risk of hospital death or prolonged ICU stay, both inside and outside critical care units. A qSOFA score of ≥2 may identify more than 90% of 28-day deaths among patients with sepsis, and the addition of Tb ≤36.5°C may complement the predictive validity of qSOFA. A subsequent prospective evaluation will help clarify the validity of qSOFA and may help establish clinically useful parameters.
Footnotes
Authors’ Note
This study was approved by the Japanese Association for Acute Medicine and by the Institutional Review Board of Hokkaido University Hospital for Clinical Research; Ethics Committee of Nagoya University of Graduate School of Medicine; Ethics Committee of Keio University School of Medicine; Fujita Health University ethical review board for epidemiological and clinical studies; Teikyo University Review Board; Ethics Committee of Nippon Medical School Hospital; Ethics Committee of Nippon Medical School Hospital; Center for Clinical Research, Yamaguchi University Hospital; Ethics Review Board of Hyogo College of Medicine; Ethics Committee of Osaka University Hospital; Ethics Committee of Kyorin University; Ethics Committee of Tohoku University Hospital; Ethics Committee of Kawasaki Municipal Hospital; Ethical Committee of Kurume University; and Research Ethics Committee of Kawasaki Medical School and Hospital. Data collection was performed as part of the routine clinical examinations and did not require additional medical intervention. Data management and statistical analyses were processed anonymously. For these reasons, the need for written informed consent was waived by both the Japanese Association for Acute Medicine and the Ethics Committees of the participating hospitals. The data cannot be deposited in publicly repositories since the agreement of the Ethic committee did not cover this aspect. However, we fully agree to discuss and share key data with interest individuals. Shigeki Kushimoto. participated in the study design and data collection and interpretation, performed the statistical analysis, and drafted the manuscript. Satoshi Gando, Hiroshi Ogura, Yutaka Umemura, Daizoh Saitoh, Toshihiko Mayumi, Seitaro Fujishima, Toshikazu Abe, Atsushi Shiraishi, Hiroto Ikeda, Joji Kotani, Yasuo Miki, Shin-ichiro Shiraishi, Koichiro Suzuki, Yasushi Suzuki, Naoshi Takeyama, Kiyotsugu Takuma, Ryosuke Tsuruta, Yoshihiro Yamaguchi, Norio Yamashita, and Naoki Aikawa participated in the study design and data collection and interpretation, performed the statistical analysis, and helped to draft the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded and supported by the Japanese Association for Acute Medicine.
{kind=link}