
Abstract
Background:
Disseminated intravascular coagulation (DIC) has been recognized as an urgent and critical condition in patients with sepsis. Therefore, unfamiliar and time-consuming tests or a complex scoring system are not suitable for diagnosis. Sepsis-induced coagulopathy (SIC), a newly proposed category delineated by a few global coagulation tests, has been established as an early warning sign for DIC. The purpose of this study was to elucidate the characteristics of SIC, especially in relation to the score of the International Society on Thrombosis and Haemostasis (ISTH) for overt DIC.
Method:
A data set for 332 patients with sepsis who were suspected to have DIC, antithrombin activity <70%, and treated with antithrombin substitution was utilized to examine the relationship between SIC and overt DIC. The performance of SIC calculated at baseline (ie, before treatment) as well as on days 2, 4, or 7 was analyzed in terms of its ability to predict 28-day mortality and overt DIC.
Results:
At baseline, 149 (98.7%) of 151 patients with overt DIC according to the ISTH definition were diagnosed as having SIC. Of the 49, 46 (93.9%) patients who developed overt DIC between days 2 and 4 had received a prior diagnosis of SIC. The sensitivity of baseline SIC for the prediction of death was significantly higher than that of overt DIC (86.8% vs 64.5%, P < .001). The sensitivity of SIC on days 2, 4, and 7 was significantly higher than those of overt DIC (96.1%, 92.3%, and 84.4% vs 67.1%, 57.7%, and 50.0%, P < .001, .001, and .001, respectively), although the specificity of SIC was lower at all time points.
Keywords
Introduction
Disseminated intravascular coagulation (DIC) was defined as “an acquired syndrome characterized by the intravascular activation of coagulation with loss of localization arising from different causes” by the Scientific Subcommittee on DIC of the International Society on Thrombosis and Haemostasis (ISTH) in 1991. 1 The ISTH overt DIC diagnostic criteria were released according to this definition and have been used worldwide. Despite the high prevalence of DIC and its prognostic implications, the treatment of this detrimental condition has not been very successful in most countries especially after the withdrawal of recombinant activated protein C. 2,3 In contrast, anticoagulant therapy using antithrombin concentrate and recombinant thrombomodulin has undergone extensive evaluation and is widely used for the treatment of patients with septic DIC in Japan. 4 –7 Thus, the latest Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock recommend the use of antithrombin for sepsis-associated DIC and antithrombin activity less than 70%. 8 Recent studies have revealed that a survival benefit of anticoagulant therapy is evident only in patients with septic DIC and not in non-DIC patients who have sepsis. 9,10 Therefore, the early identification of patients with sepsis with DIC who may benefit from anticoagulant therapy has become a major goal in the emergency and critical care fields. In 2006, the Japanese Association for Acute Medicine (JAAM) released diagnostic criteria for DIC which have been widely used since then. 11 However, since the systemic inflammatory response syndrome category adopted in JAAM-DIC is no longer used for the diagnosis of sepsis, 12 new criteria that fit the new definition would be ideal. 13
Along with the progress in understanding the pathogenesis of DIC in different background conditions, coagulation markers specific for each underlying cause of DIC have been proposed. 14,15 For example, DIC secondary to infections is characterized by the excessive suppression of fibrinolysis arising from the overproduction of plasminogen activator inhibitor 1. 16 We recently found a limited value for these markers and proposed the sepsis-induced coagulopathy (SIC) criteria that use the new definition of sepsis and only 2 laboratory markers, that is, platelet count and prothrombin time (PT). The aim of the present study was to validate the SIC diagnostic criteria and examine the relationship between SIC and ISTH overt DIC. 17,18
Patients and Methods
Data Collection
Data were collected from a multi-institutional postmarketing surveillance performed by Nihon Pharmaceutical Co Ltd (Tokyo, Japan). A total of 332 patients with sepsis and suspected DIC, with antithrombin activity <70%, and treated with antithrombin concentrate were registered between April 2015 and May 2016. Antithrombin concentrate (30-60 IU/kg/d; Nihon Pharmaceutical Co, Ltd) was administered for up to 3 consecutive days from the days of suspected sepsis.
Laboratory Measurements and Diagnostic Criteria
The platelet count, fibrin/fibrinogen degradation products (FDPs) or
SIC and ISTH Overt DIC Scoring Systems.a,b
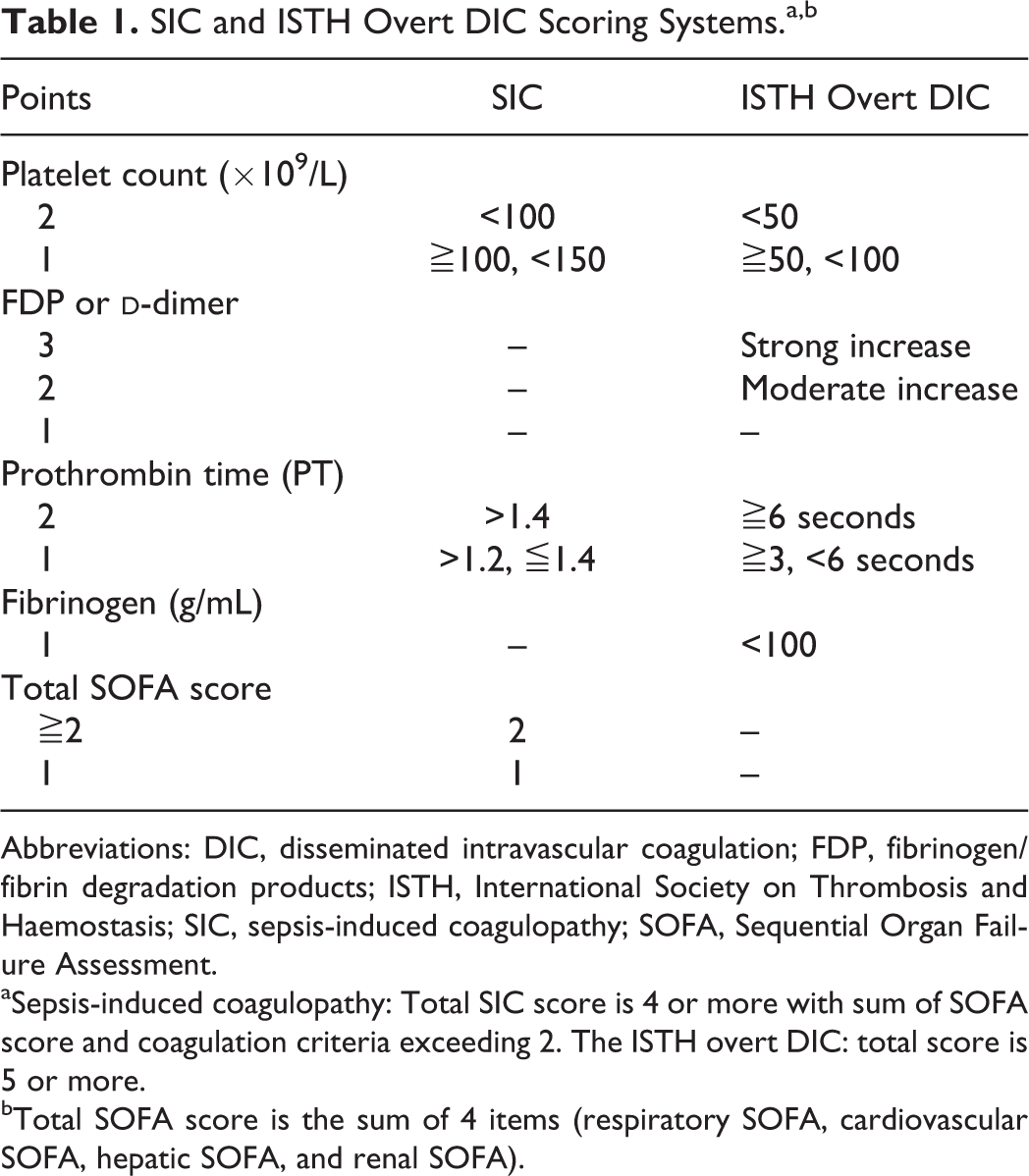
Abbreviations: DIC, disseminated intravascular coagulation; FDP, fibrinogen/fibrin degradation products; ISTH, International Society on Thrombosis and Haemostasis; SIC, sepsis-induced coagulopathy; SOFA, Sequential Organ Failure Assessment.
aSepsis-induced coagulopathy: Total SIC score is 4 or more with sum of SOFA score and coagulation criteria exceeding 2. The ISTH overt DIC: total score is 5 or more.
bTotal SOFA score is the sum of 4 items (respiratory SOFA, cardiovascular SOFA, hepatic SOFA, and renal SOFA).
Ethics Approval, Patient Consent, Study Permissions, and Consent to Publish
The postmarketing surveillance was performed under the supervision of the Japanese Ministry of Labour and Welfare and was conducted in accordance with the Declaration of Helsinki, Good Vigilance Practice, and Good Post-Marketing Study Practice. For the data analysis, since the complete anonymization of personal data was performed upon data collection and the identification of individual patients was not possible, this study did not need ethical approval and the ethics committee of Juntendo University School of Medicine waived the need to obtain informed consent and the patients’ agreement. For the same reason, the institutional committee determined that consent to publish was not required.
Statistical Analysis
The numerical values in the text and tables represent the median and interquartile range. Univariate associations were evaluated using the McNemar test, Fisher exact test, or unpaired Wilcoxon signed rank test. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for 28-day mortality were calculated for SIC at baseline (day 1) and on days 2, 4, and 7. A P value <.05 was considered to denote statistical significance. All the analyses were performed using SPSS 22.0 for Windows (IBM SPSS Inc, Chicago, Illinois).
Results
Baseline Characteristics of the Study Population
Of the 332 patients included in the study, 76 were not alive at 28 days (mortality rate, 22.9%). Table 2 shows the baseline characteristics of the patients. The median age of the survivors was 73.0 (65-80) years, compared with 78.5 (68-86) years for the nonsurvivors (P < .001). No significant difference in gender distribution between the survivors and nonsurvivors was seen. As for the coagulation profile at baseline, the platelet count, FDP,
Baseline Characteristics of the Patients.a
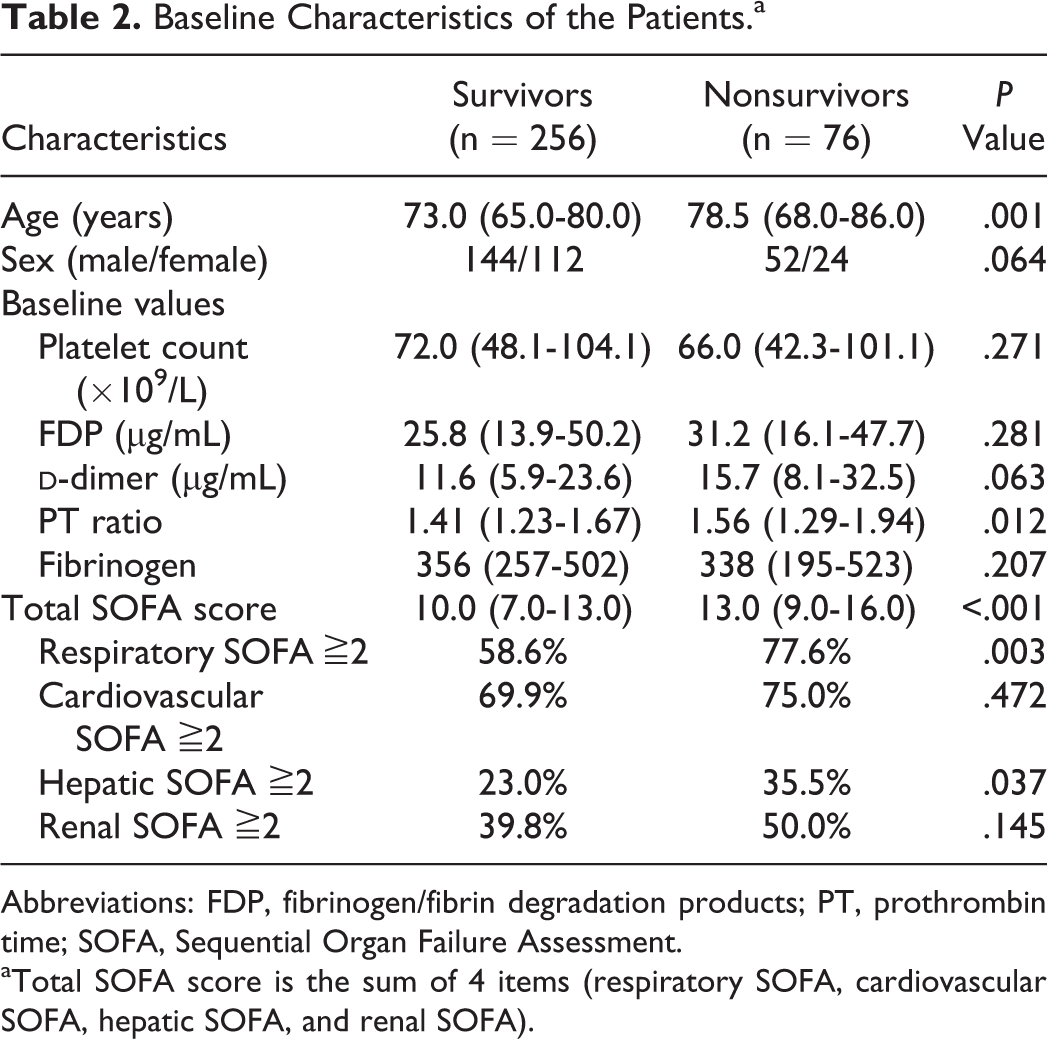
Abbreviations: FDP, fibrinogen/fibrin degradation products; PT, prothrombin time; SOFA, Sequential Organ Failure Assessment.
aTotal SOFA score is the sum of 4 items (respiratory SOFA, cardiovascular SOFA, hepatic SOFA, and renal SOFA).
Twenty-Eight-Day Mortality
The sensitivity, specificity, PPV, and NPV for 28-day mortality of the SIC and ISTH overt DIC are shown in Table 3. The 28-day mortality rate for patients with SIC at baseline was 23.1%, compared to 32.5% in patients diagnosed as having overt DIC at baseline (P = .040). Figure 1A and B shows the relationships between the SIC and overt DIC scores and the mortality rate. The mortality rate was 13.7% for an SIC score of 4 at baseline, and it gradually increased as the score increased reaching a maximum of 28.0% for a score of 6. For the overt DIC, the mortality rate ranged between 25.3% and 50.0% for scores of 5 to 7 points. The mortality rate was below 14.9% when the overt DIC score was 4 or less. The sensitivity of SIC at baseline was 86.8%, which was significantly higher than the sensitivity of overt DIC (64.5%; P < .001). The sensitivity of SIC increased from baseline to day 2, 4, or 7 and remained significantly higher than the sensitivity of overt DIC at all these time points (Table 3). There was no difference in NPV between SIC and ISTH overt DIC. The specificity of SIC was significantly lower at any of the time points considered.
Comparison of SIC and ISTH Overt DIC.
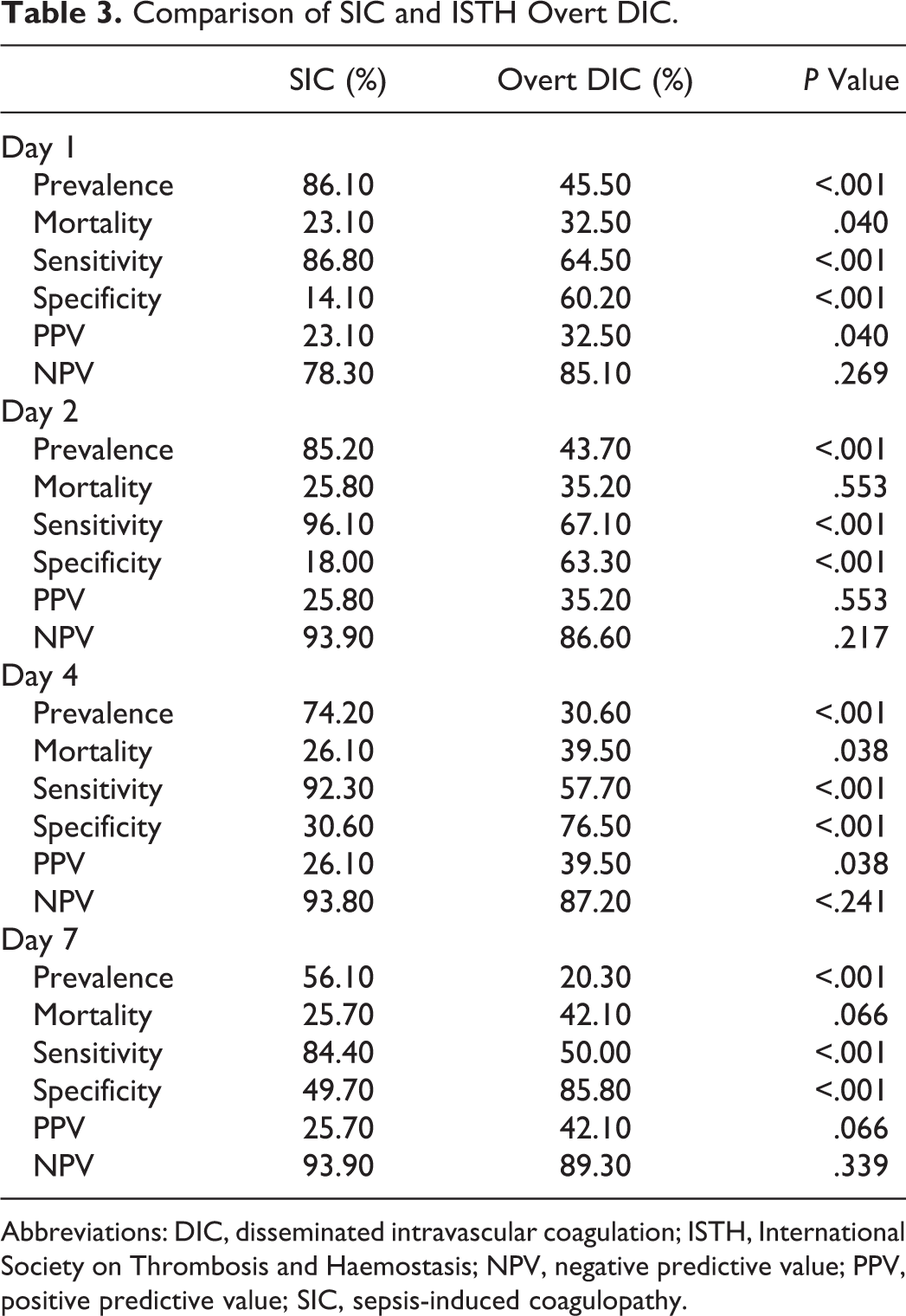
Abbreviations: DIC, disseminated intravascular coagulation; ISTH, International Society on Thrombosis and Haemostasis; NPV, negative predictive value; PPV, positive predictive value; SIC, sepsis-induced coagulopathy.
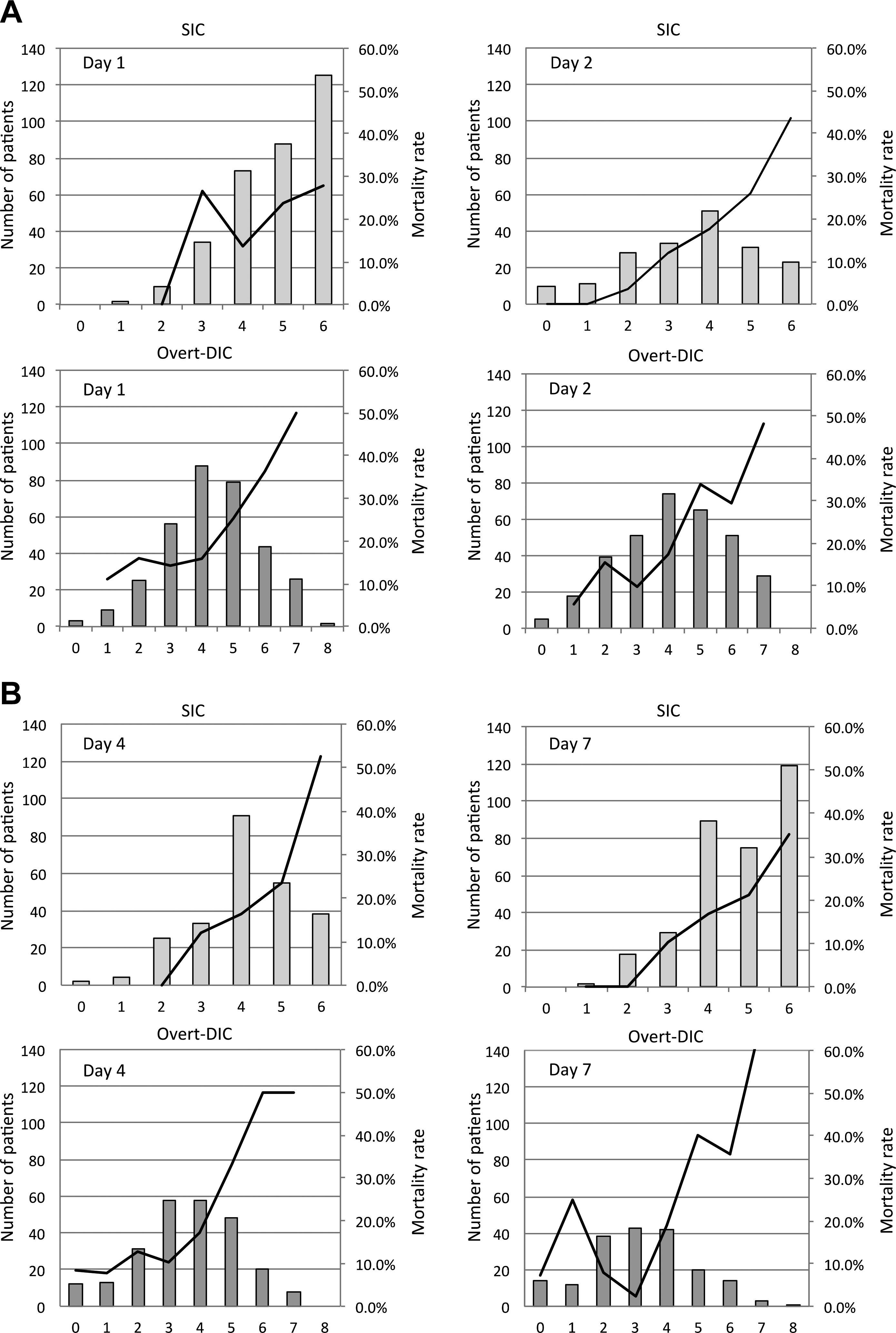
Patient counts and mortality rates according to the SIC and the overt DIC classifications. The patient distributions (bars) and the mortality rates (lines) are plotted according to the SIC scores (above) and the overt DIC scores (below). The x-axis represents the score. The mortality rate increased as SIC score elevated except score 3 on day 1. Similar trend was in overt DIC. DIC indicates disseminated intravascular coagulation; SIC sepsis-induced coagulopathy. A: Day 1 and 2; B: Day 4 and 7.
International Society on Thrombosis and Haemostasis Overt DIC and SIC
The number of patients diagnosed as SIC was about twice or more of than that of overt DIC (Figure 2). On day 2, 145 cases had ISTH overt DIC, and 104 (71.7%) cases had been diagnosed as overt DIC on day 1. The remaining 41 were newly diagnosed as having overt DIC on day 2. Among these 41 newly diagnosed overt DIC cases, 38 (92.7%) cases had SIC on day 1. All 8 cases who were newly diagnosed as having overt DIC on day 4 had been diagnosed as having SIC on day 1 (Figure 3). In total, SIC preceded overt DIC in 46 (93.9%) of 49 patients.
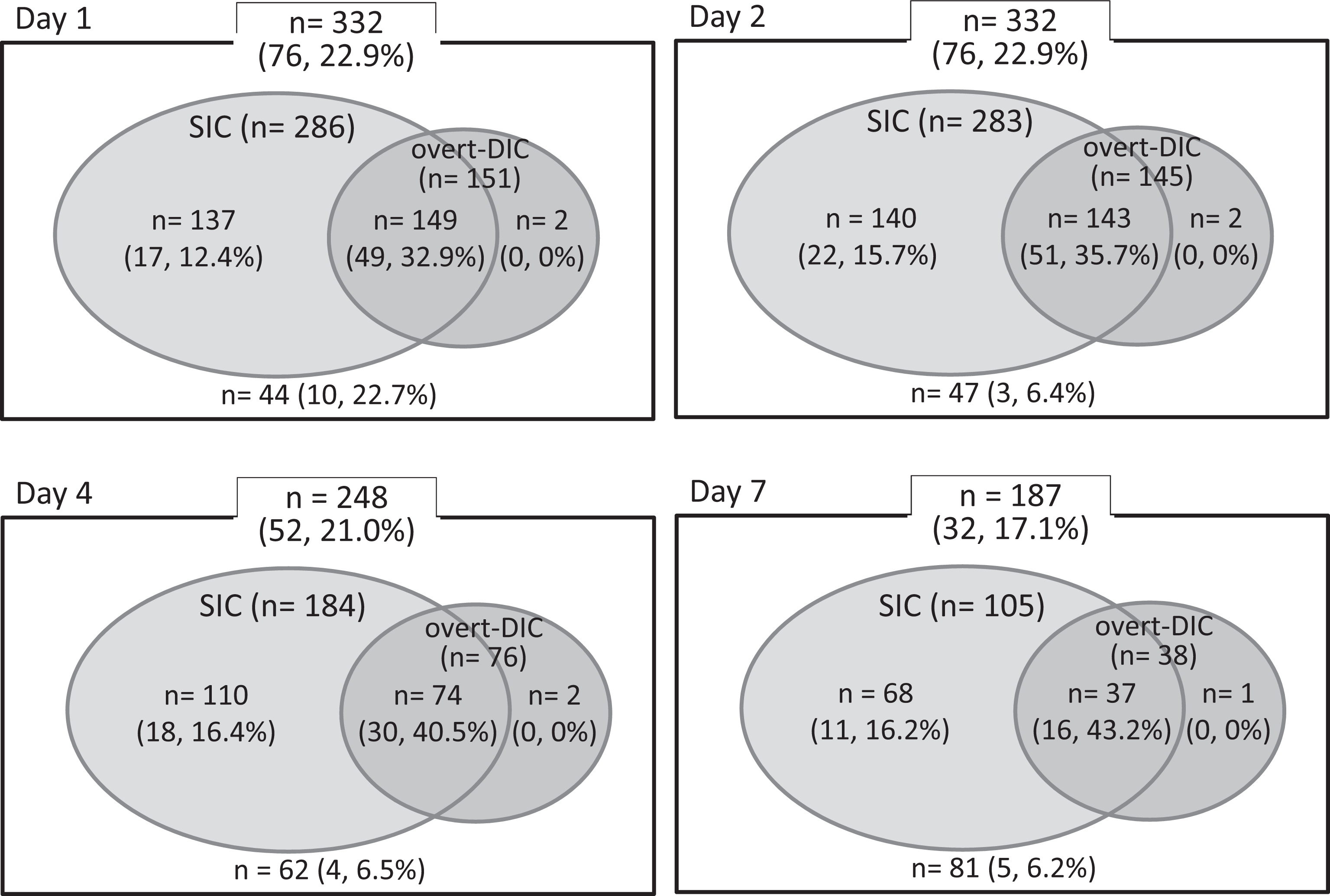
Distribution of patients according to the SIC and ISTH overt DIC diagnostic criteria. Each figure shows the comparison between SIC and ISTH overt DIC. The numbers represent the number of cases in each category and numbers in parentheses are of nonsurvivors and the mortality rate. Most of the overt DIC cases are included in SIC. DIC indicates disseminated intravascular coagulation; ISTH, International Society on Thrombosis and Haemostasis; SIC, sepsis-induced coagulopathy.
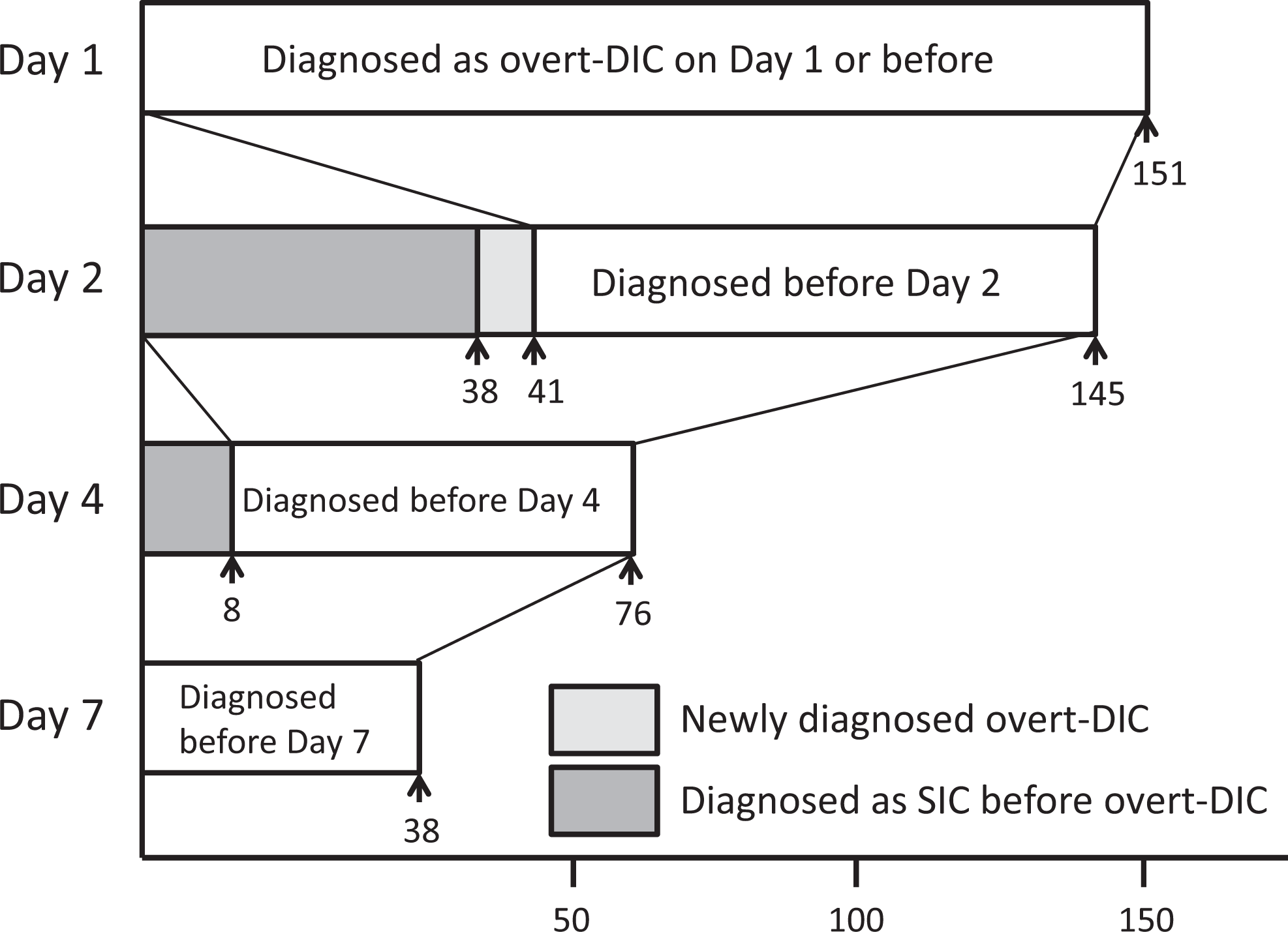
Distribution of patients according to ISTH overt DIC diagnostic criteria. On day 2, 41 cases were newly diagnosed as having overt DIC and 38 (92.7%) cases were diagnosed as SIC on day 1. All 8 cases who were newly diagnosed as having overt DIC on day 4 had been diagnosed as having SIC on day 1. DIC indicates disseminated intravascular coagulation; ISTH, International Society on Thrombosis and Haemostasis; SIC, sepsis-induced coagulopathy
Discussion
Sepsis is almost universally associated with coagulation activation ranging from minor abnormalities in the sensitive tests to fulminant DIC. 19 Coagulation activation is widely accepted to induce microvascular thrombosis leading to multiple organ dysfunction in sepsis, 20 and the severity of coagulopathy is known to be directly correlated with mortality. 21 Furthermore, DIC has been shown to be an independent predictor of multiple organ dysfunction and mortality. 21,22 Hence, confirming the presence of coagulopathy or DIC is important for assessing the severity of sepsis.
Sepsis-induced coagulopathy is a new criterion proposed by the active members of ISTH/DIC subcommittee in 2017 that identifies “sepsis with coagulopathy.” 18 It was established based on the need for a simple and easy-to-use criterion and therefore consists of only 3 parameters, that is, platelet count, PT-INR, and the SOFA score. The definition of sepsis was updated in 2016 from “infection-induced systemic inflammatory response” to “infection with organ failure” with the total SOFA score that had to be at least 2 points. 12 To account for this new definition of sepsis, the SIC requires at least 2 points for the SOFA score. In addition, the sum of the criteria for the platelet count and PT-INR had to be 2 or higher. The SIC score was derived using data from 1498 patients with sepsis treated with recombinant thrombomodulin. In the present study, we reexamined the characteristics of SIC by using the recent data obtained from the patients with sepsis with antithrombin activity <70% and treated by antithrombin.
With respect to the comparisons of diagnostic performance, the superiority or inferiority of diagnostic criteria cannot be determined because DIC is purely a concept. 23,24 The setting of diagnostic criteria could only be changed by balancing the sensitivity and specificity to mortality. In case of the JAAM-DIC, it has been repeatedly shown to have higher sensitivity but lower specificity in comparison with ISTH overt DIC. 21,25 However, this type of comparison may not be appropriate for SIC, since SIC was established to identify patients with a high risk of DIC at an earlier time point using only a few common tests.
The ISTH overt DIC diagnostic criteria were established in 2001, and although it was suggested that they could predict mortality, sensitivity was relatively low. The present study confirmed the low sensitivity, which was 64.5% on day 1 and remained relatively low on day 2, 4, or 7. In an attempt to detect the coagulopathy at earlier stages, a more sensitive score for non-overt-DIC was proposed by ISTH. 1 However, the non-overt-DIC scoring system is more complex and included nonroutine laboratory tests such as protein C, antithrombin, and other molecular markers. Most physicians in Japan use the JAAM-DIC diagnostic criteria because of its higher sensitivity, and the latest Japanese Clinical Practice Guidelines for the Management of Sepsis and Septic Shock recommend the use of JAAM-DIC diagnostic criteria. 8 However, we think that a combination of ISTH overt DIC and SIC is very useful since it can overcome the issue of low sensitivity of overt DIC. On the contrary, overt DIC compensates for the low specificity of SIC. Sepsis-induced coagulopathy is also useful to reduce the medical expense and avoid unnecessary follow-up.
The SIC scoring system includes only 2 of the 4 markers included in the ISTH score, which simplifies calculation and provides an easy tool to identify patients at risk for overt DIC. In addition, the SIC score does not require the measurement of FDP, which is required by the ISTH overt DIC score and thus is expected to increase applicability.
The efficacy of anticoagulant therapy for sepsis is still under debate. 26,27 Recent studies have repeatedly reported significant benefits in the subsets of patients with sepsis diagnosed with DIC but with no effect in those without DIC. 10,14 The use of antithrombin in patients with sepsis has become standard practice in Japan since the landmark observations of Tagami et al 5,28 who reported a reduced mortality rate among patients with sepsis treated with a supplemental dose of antithrombin. In addition to antithrombin, recombinant thrombomodulin has become part of the therapeutic armamentarium in patients with sepsis and is currently under investigation in a phase 3 multinational study which uses very similar criteria to SIC to define the target coagulopathy (NCT01598831). Since anticoagulant therapy is popular in Japan, emergency and critical care physicians will appreciate a diagnostic tool like SIC that makes early diagnosis possible. The international harmonized guidance also stated that although further prospective evidence from randomized controlled trials is required, administration of antithrombin or recombinant thrombomodulin may be considered in certain patients with DIC. In this guidance, the prophylactic doses of unfractionated heparin or low-molecular-weight heparin are recommended in critically ill and nonbleeding patients with DIC for the prevention of venous thromboembolism. 29 However, the authors do recognize that suitability of SIC as an indicator for anticoagulant therapy was out of the scope of the present study.
The present study has some limitations. First, since the data set was obtained from a postmarketing survey for antithrombin, selection bias is likely to exist. Second, all patients had decreased antithrombin activity and were treated with antithrombin, which might have affected the prognosis. We have to remind that all patients examined in this study had decreased antithrombin activity of less than 70%, and therefore, SIC score was SIC and antithrombin activity of less than 70% and ISTH score was ISTH score and antithrombin activity of less than 70%. The diagnostic performance of SIC should also be examined in patients not receiving antithrombin or recombinant thrombomodulin. Third, since the present study was a retrospective analysis, the usefulness of SIC remains to be determined in a future prospective study.
In summary, DIC may be underdiagnosed in emergency and critical care departments. The SIC diagnostic criterion was specifically established to identify SIC using a minimal number of items. The present study revealed that SIC can help to prevent sepsis-associated DIC from being overlooked by aiding early diagnosis. Furthermore, the monitoring of SIC score is useful for evaluating the severity of SIC. The active diagnosis of SIC is expected to support the prediction of sequentially occurring ISTH overt DIC.
Conclusion
Sepsis-induced coagulopathy seems to be valuable for predicting overt DIC. It is simple, easy to use, and suitable for application in emergency care settings. The usefulness of this scoring system should be examined in a future prospective study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Makoto Arakawa is an employee of Nihon Pharma Co. Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the fund from Ministry of Education, Culture, Sports, Science and Technology–Supported Program for the Strategic Research Foundation at Private Universities 2017.