
Abstract
Purpose:
To compare the development of clinically significant hemodynamic event (ie, hypotension or bradycardia) in adults with septic shock receiving either propofol or dexmedetomidine.
Materials and Methods:
A retrospective cohort study of adults with septic shock admitted to an intensive care unit (ICU) at an academic medical center between July 2013 and July 2017.
Results:
Patients in the propofol (n = 35) and dexmedetomidine (n = 37) groups developed a clinically significant hemodynamic event at similar frequencies (31.4 vs 29.7%, P = .99). All patients with an event experienced hypotension, whereas 2 (5.4%) patients in the dexmedetomidine group also experienced bradycardia. Most patients in both groups (70% vs 90%) received an escalating sedative dose, and almost half (42.9%) in the dexmedetomidine group had the sedative dosage increased more frequently than every 30 minutes. Patients in both groups had similar ICU (24.1 vs 24.3 days, P = .98) and hospital (37.9 vs 29.7 days, P = .29) lengths of stay. There was no difference in median time to hemodynamic event between the groups (propofol 1 hour [interquartile range, IQR: 0.5-9.9] vs dexmedetomidine 2 hours [IQR: 1.5-11.1 hours], P = .85).
Conclusion:
Patients with septic shock receiving propofol or dexmedetomidine experienced similar rates of clinically significant hemodynamic events. Most patients did not experience an event and those who did most frequently did so in the first couple of hours of therapy.
Introduction
The most recent guidelines for the management of pain, agitation, and delirium in adults receiving care in an intensive care unit (ICU) endorsed by the Society of Critical Care Medicine recommend a nonbenzodiazepine agent preferentially to benzodiazepines to provide light sedation in patients experiencing or at risk of agitation due to their improved safety and efficacy profiles. 1 Propofol and dexmedetomidine, 2 of the most commonly used nonbenzodiazepines, have side-effect profiles that include bradycardia and hypotension. 2,3 In many patient populations, if these effects occur, they can be mitigated without causing patient harm. However, patients experiencing septic shock may be at increased risk of these adverse effects and their negative sequelae due to the pathophysiology of the syndrome. 4 Additionally, decisions to initiate and titrate these sedatives in patients with septic shock may be more complicated than those in hemodynamically stable patients.
In an a priori subgroup analysis of patients with sepsis and without sepsis from the Maximizing Efficacy of Targeted Sedation and Reducing Neurological Dysfunction trial, there were similar rates of sinus bradycardia (13% vs 6%) and vasoactive medication dosage increase (26% vs 47%) between the patients treated with dexmedetomidine and lorazepam. Additionally, patients in the dexmedetomidine group with sepsis had a similar frequency of bradycardic (13% vs 24%, P = .46) and hypotensive (26% vs 33%, P = .69) events compared to patients without sepsis. 5 In the Dexmedetomidine for Sepsis in Intensive Care Unit Randomized Evaluation trial, there was no difference in bradycardic events between patients with sepsis who received dexmedetomidine compared to those who were sedated with propofol, midazolam, or an analgesic (7% vs 2%, P = .10). Two-thirds of patients in each group experienced shock during their treatment course; however, the etiology of the shock and effect of the sedation strategy on hypotension were not described. 6 In a cohort of patients with sepsis (33%) and severe sepsis (67%), those who received propofol for sedation experienced a >20% decrease in mean arterial pressure (MAP) as frequently as patients who received another sedative strategy (58.6% vs 63.2%, P = .53). The other sedative strategies were more frequently midazolam (41.4%) and fentanyl (41.4%) and less frequently dexmedetomidine (6.9%). 7 The authors were unable to conclude whether patients with sepsis or severe sepsis progressed to septic shock or experienced a sedative-associated adverse effect.
The specific effects of nonbenzodiazepines on development of clinically significant hypotensive and bradycardic events in patients with sepsis and more specifically septic shock remain undetermined due to ambiguous definitions and heterogeneous populations in previous studies. The purpose of this study was to compare the development of clinically significant hypotension and bradycardia in adult patients with septic shock receiving either propofol or dexmedetomidine.
Materials and Methods
Study Design
This was a retrospective, observational, cohort study of adult patients with septic shock admitted to an ICU at Rush University Medical Center between July 1, 2013, and July 31, 2017. Our institution has 684 beds and 5 ICUs (medical, surgical, cardiovascular, cardiac, and neurosciences).
Patients
Patients who were eligible for inclusion were at least 18 years of age, admitted to an ICU for >48 hours, mechanically ventilated, met the sepsis-2 definition of septic shock (confirmed or suspected infection with sepsis-induced hypotension that persists, despite adequate fluid resuscitation and at least 2 of the following: tachycardia [heart rate > 90 beats/min], tachypnea [respiratory rate > 20 breaths/min], fever or hypothermia [temperature >38°C or <36°C], and leukocytosis or leukopenia [white blood cell count >1200/mm3 or <4000/mm3]), 8 and received a continuous infusion of either propofol or dexmedetomidine for at least 2 hours or until an adverse event occurred, whichever came first, after being on a stable dosage of vasopressor medication(s) for at least 2 hours. All patients had an initial target MAP of 65 mm Hg. Patients eligible for inclusion were excluded if they received propofol and dexmedetomidine concurrently. Institutional policies to guide propofol and dexmedetomidine use were in place during the study period. Recommendations were to initiate propofol at 5 to 10 μg/kg/min and titrate by 5 to 10 μg/kg/min every 5 to 10 minutes up to a maximum dosage of 80 μg/kg/min to achieve a target sedation score and to initiate dexmedetomidine at 0.2 μg/kg/h and titrate by 0.1 μg/kg/h every 30 minutes up to a maximum dosage of 1.4 μg/kg/h to achieve a target sedation score. All patients had an initial target Richmond Agitation Sedation Scale score of 0 to −2. Patients receiving these medications had continuous hemodynamic monitoring. Adjunctive sedative and analgesic agents were defined as another agent (ie, benzodiazepines, fentanyl, and ketamine) used as an intermittent bolus or continuous infusion.
Study Outcomes
The primary outcome was the development of a clinically significant hemodynamic event, defined as either clinically significant hypotension (an increase in vasopressor dosage by at least 20%, addition of another vasopressor, and/or decrease from baseline in systolic blood pressure by 30 mm Hg or MAP by 10 mm Hg) or clinically significant bradycardia (a decrease from baseline in heart rate by 30 beats/min or heart rate less than 50 beats/min). 3 Secondary outcomes were the development of clinically significant hypotension and clinically significant bradycardia as well as mortality at 28 days, ICU length of stay, hospital length of stay, mechanical ventilation duration, propofol or dexmedetomidine (sedative) dosage and dosage increases at time of hemodynamic event, loading dose within 30 minutes of sedative initiation, hemodynamic event following loading dose, dexmedetomidine dose titrations more frequently than 30-minute intervals, and occurrence of a hemodynamic event on renal replacement therapy.
Statistical Analysis
Because the rates of hypotension and bradycardia in critically ill patients with septic shock had not previously been investigated, a convenience sample was used to evaluate the primary and secondary outcomes. Baseline characteristics were compared between propofol and dexmedetomidine groups. Primary and secondary outcomes were analyzed via student t test for continuous data and Pearson χ2 or Fisher exact test, as appropriate, for categorical data. All analyses were performed using Spss.v23. Based on the data distribution, the mean and standard deviation (SD) or median and interquartile ranges (IQRs) were used to report the analyses of baseline characteristics and primary and secondary outcomes. A P Value of .05 was utilized when determining statistical significance between treatment groups. A Kaplan-Meier analysis was performed to review the time to hypotension (ie, event) between the propofol and dexmedetomidine treatment groups.
Results
Seventy-two of 447 patients screened were included with 35 patients in the propofol group and 37 patients in the dexmedetomidine group (Figure 1). Baseline and clinical characteristics were similar between the 2 treatment groups. More than 80% of patients in both groups were receiving a continuous infusion of fentanyl (85.7% vs 81.1%) along with propofol or dexmedetomidine. No patient received a continuous infusion of a benzodiazepine. Sequential organ failure assessment (SOFA) scores within 6 hours of ICU admission were similar between propofol and dexmedetomidine groups (13 [IQR: 9-17] vs 12 [IQR 7-17], Table 1).
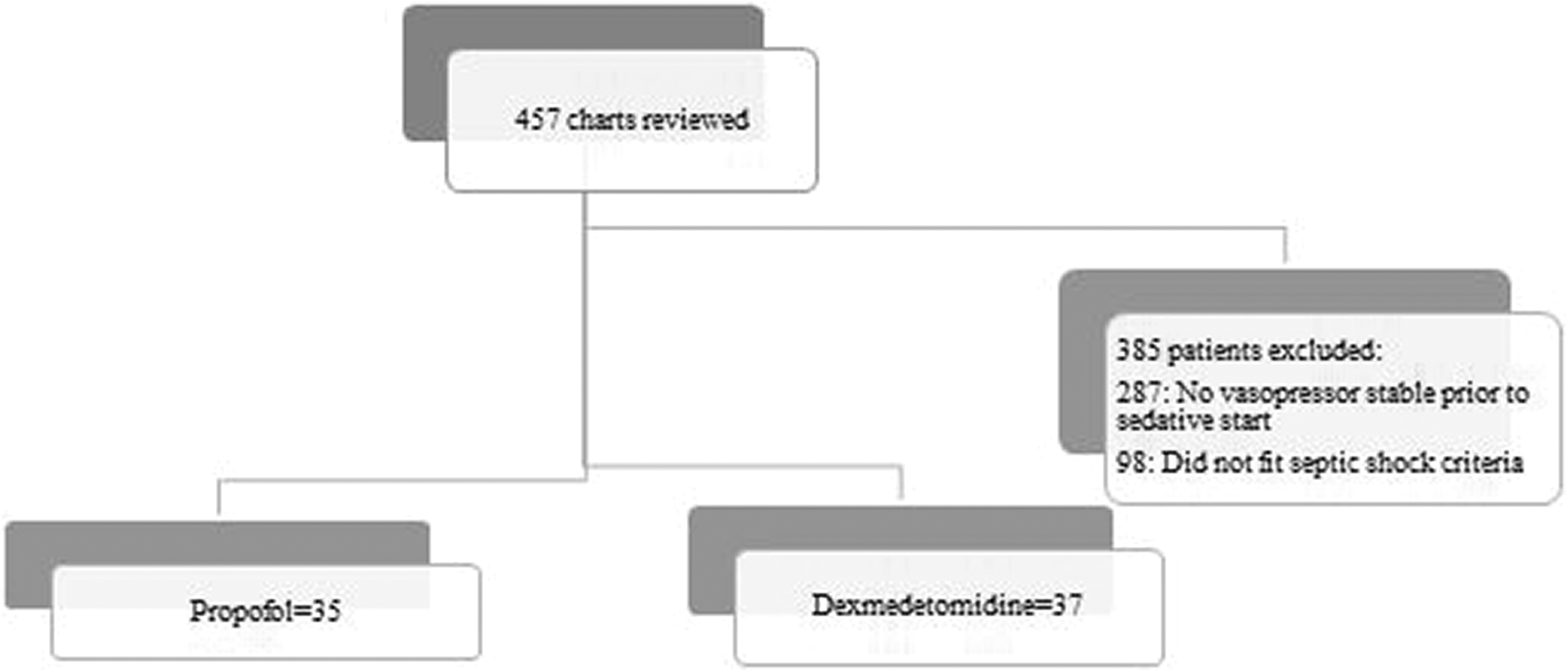
Patient inclusion and exclusion.
Baseline Characteristics.
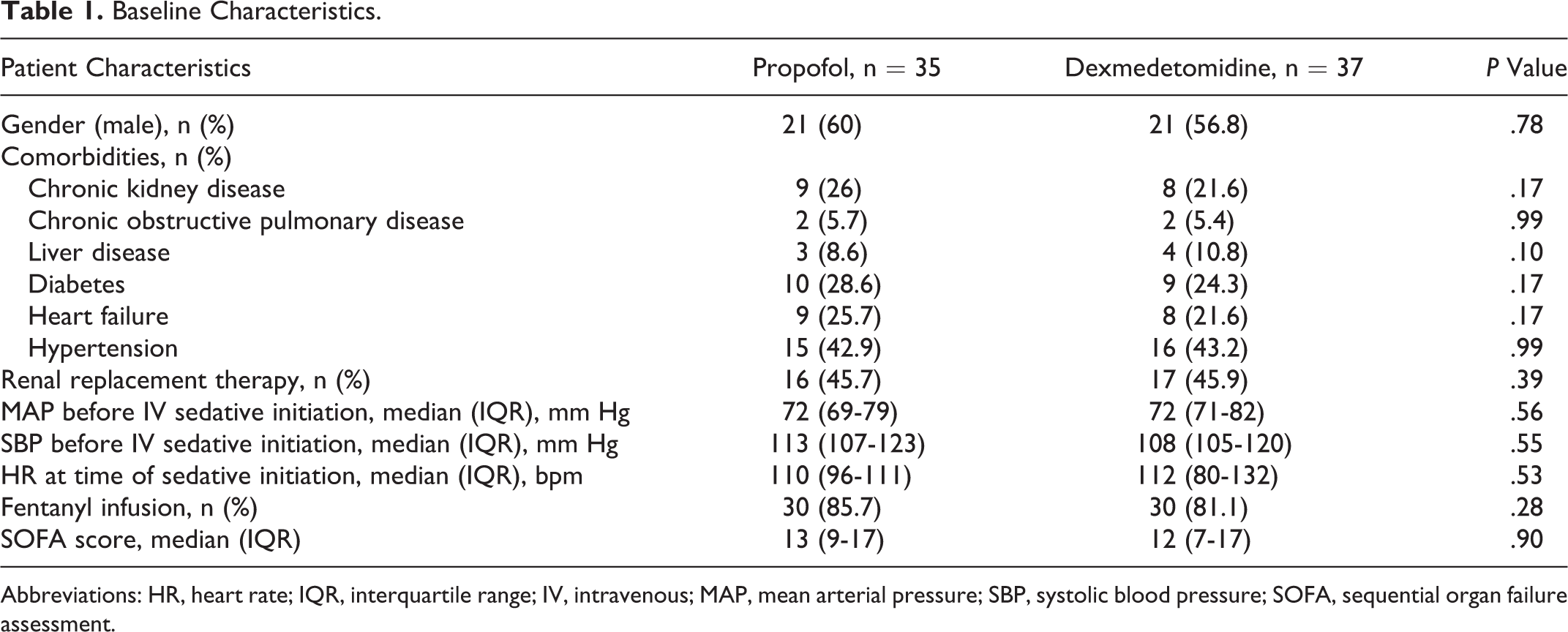
Abbreviations: HR, heart rate; IQR, interquartile range; IV, intravenous; MAP, mean arterial pressure; SBP, systolic blood pressure; SOFA, sequential organ failure assessment.
Patients in the propofol and dexmedetomidine groups developed a clinically significant hemodynamic event at similar frequencies (31.4% vs 29.7%, P = .99). There was no difference in time to hemodynamic event between treatment groups (propofol median 1 hour [IQR: 0.5-9.9 hours] vs dexmedetomidine median 2 hours [IQR: 1.5-11.1 hours], P = .85). Patients generally developed a hemodynamic event in both treatment groups within the first couple of hours of therapy (Figure 2). Each event was characterized by clinically significant hypotension, whereas 2 of the patients in the dexmedetomidine group developed both clinically significant hypotension and bradycardia. All patients had an increase in their vasopressor rate subsequent to a decrease in systolic blood pressure and/or MAP for hypotensive events. Dexmedetomidine dosage was decreased following bradycardic events. The median dosages of propofol and dexmedetomidine at the time of the event were 20 μg/kg/min and 0.8 μg/kg/h, respectively. The majority of patients in both groups (70% vs 90%) were receiving an escalating dose of the sedative, and almost half (42.9%) of patients in the dexmedetomidine group had the sedative dosage increased more frequently than every 30 minutes. No dosage increase in an adjunctive sedative or analgesic was provided at the time of hemodynamic events. One patient in each group was receiving continuous renal replacement therapy when the hemodynamic event occurred. The duration of mechanical ventilation was similar between groups (5.6 vs 9.7 days, P = .34). Patients in both groups had similar ICU (24.1 vs 24.3 days, P = .98) and hospital (37.9 vs 29.7 days, P = .29) lengths of stay. Mortality at 28 days was similar between the groups (40% vs 59.5%, P = .16; Table 2).
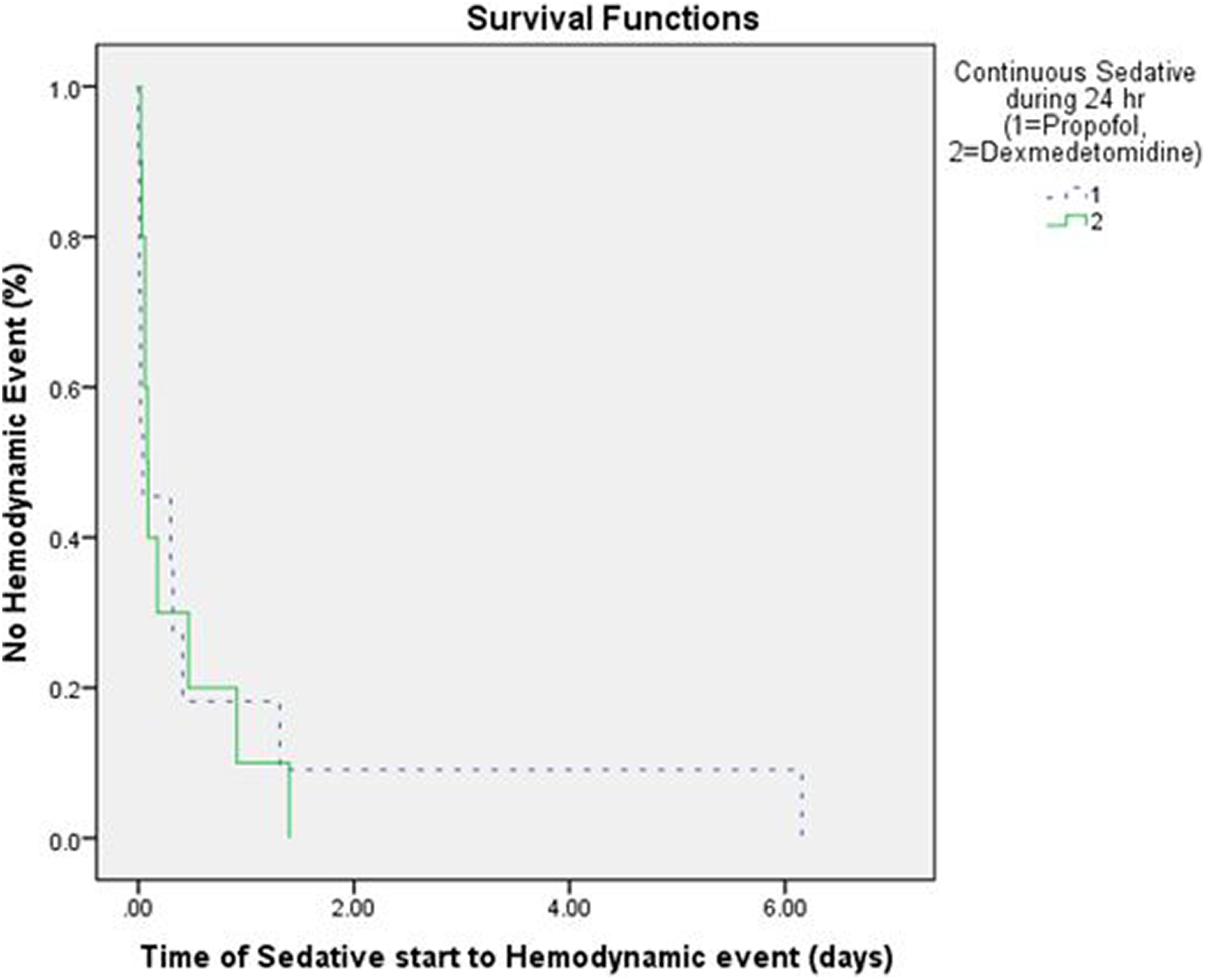
Kaplan-Meier curve.
Study Outcomes.
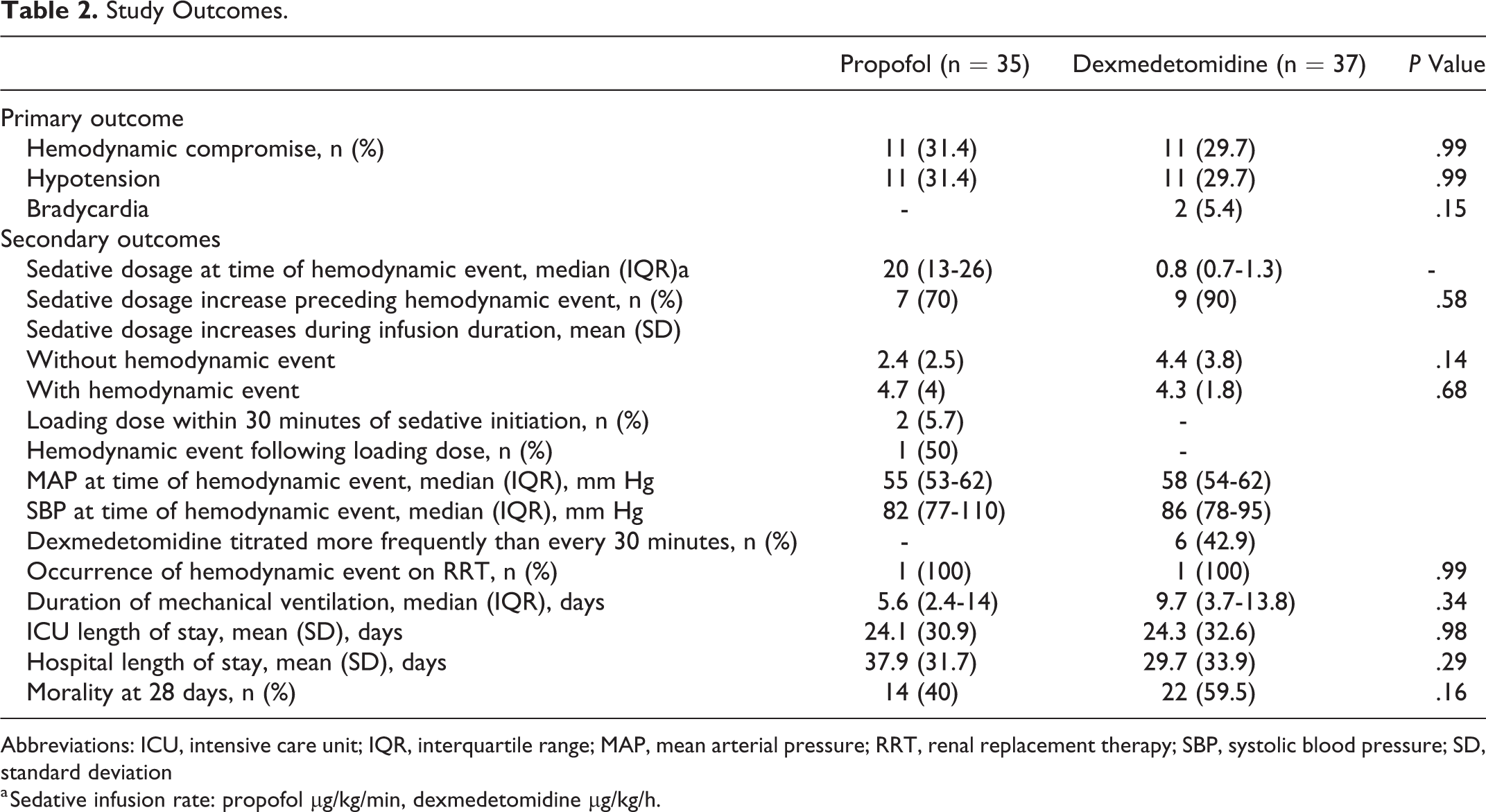
Abbreviations: ICU, intensive care unit; IQR, interquartile range; MAP, mean arterial pressure; RRT, renal replacement therapy; SBP, systolic blood pressure; SD, standard deviation
a Sedative infusion rate: propofol μg/kg/min, dexmedetomidine μg/kg/h.
Discussion
This is the first study to compare the effects of propofol and dexmedetomidine on development of hemodynamic compromise in a homogenous cohort of adult patients experiencing septic shock. The rates of clinically significant hypotension and bradycardia were similar between propofol and dexmedetomidine with at least 1 event occurring in 30% of patients. The majority of events developed within the first couple of hours of sedative therapy with no difference in time to the hemodynamic compromise between sedatives.
These rates of hypotension are similar to or higher than previously published in most heterogeneous populations of critically ill patients. 2,3,5,7,9 In a cohort of neurocritical care patients, 34% versus 28% of patients on propofol and dexmedetomidine, respectively, experienced clinically significant hypotension. Less than 5% of these patients were on a vasoactive agent when sedation was initiated and less than 10% had a MAP less than 70 mm Hg, suggesting systemic vasodilation was not present in most patients. 3 Patients in the Dexmedetomidine Versus Propofol for Continuous Sedation in the Intensive Care Unit (PRODEX) trial experienced similar rates of clinically significant hypotension in the propofol and dexmedetomidine groups (13.4% vs 13%). Although one-half of the patients in this trial were infected and two-thirds had some degree of cardiac failure, explicit percentages of patients who experienced sepsis or septic shock were not provided. 2 In a multicenter, retrospective cohort study, half of the patients with sepsis who received a propofol infusion, progressed to requiring vasopressor support. This higher percentage may not represent the actual incidence of hypotension from propofol, as many of these patients could have progressed to septic shock. 7 Hypotension has been seen in up to 92% of patients following a loading dose of dexmedetomidine. 10 Although no patients in the dexmedetomidine group received a loading dose, almost half of the patients had dosage increases more frequently than every 30 minutes, which in some instances included an increase from 0.2 to 1.2 μg/kg/h within a few hours. This practice effectively resembles a loading dose and may explain some of the hypotension from dexmedetomidine because 90% of events had a dosage increase preceding the event. It appears the effects of sepsis and particularly septic shock on endothelial dysfunction and vasodilation predispose these patients to hypotension from propofol and dexmedetomidine to at least a similar or possibly a slightly greater extent than other critically ill patients. 11 These alterations should be considered for patients in who hypotension would be significantly detrimental. However, because of the short-acting nature of these sedatives, 1 there use still should be strongly considered in most adult patients with septic shock.
No patients with septic shock who received propofol and almost 20% of those who received dexmedetomidine developed clinically significant bradycardia. In a cohort of neurocritical care patients, bradycardia with propofol and dexmedetomidine occurred at similar frequencies (6.3% vs 7.4%). 3 No patients in the dexmedetomidine group received a bolus dose, although 21% had dosage increases more frequently than every 30 minutes, which was significantly lower than the 42.9% seen in our study. This practice, along with the average dexmedetomidine dosage of 0.8 μg/kg/h, may reflect the more agitated nature of critically ill, intubated patients with septic shock and explain the higher rate of bradycardia seen with dexmedetomidine in our study. The rates of bradycardia in the PRODEX trial were similar between propofol and dexmedetomidine as well (10.1% vs 13%), 2 which suggests the rate of bradycardia from propofol in our study may represent either a new or a spurious finding that should be confirmed in another, prospective study of patients with septic shock. The baseline heart rates for patients in both groups were at least 110 beats/min. Because all bradycardia in the study met the definition of a decrease in heart rate by at least 30 beats/min and none resulted in a heart rate less than 50 beats/min, clinicians may not be overly concerned with bradycardia from dexmedetomidine or propofol in this cohort of patients. Nevertheless, in the critically ill patient with septic shock, measures should be implemented to prevent dosage increases more frequently than every 30 minutes whenever possible in order to reduce the likelihood of bradycardia with dexmedetomidine.
A few patient-specific factors have been independently associated with the development of clinically significant hemodynamic events in neurocritical care patients sedated with propofol or dexmedetomidine that warrant consideration in patients with septic shock. In patients sedated with propofol, propofol infusion rate (odds ratio [OR]: 1.04), baseline MAP 60 to 70 mm Hg (OR: 4.79), and need for renal replacement therapy (OR: 12.35) were associated with clinically significant hypotension. 12 In our study, the average propofol rate was relatively low when an event occurred (20 μg/kg/min), which may reflect the lower dosages of propofol used at our institution or tolerated by patients with septic shock rather than a dosage-specific effect. A single person in each group received continuous renal replacement therapy, which precluded evaluation of this variable as a predictor of an event in our study. Every patient in both groups was on at least 1 vasopressor agent, which does correlate with the lower baseline MAP seen by previous investigators. For patients sedated with dexmedetomidine, MAP <70 mm Hg (OR: 0.97) and increased Acute Physiology and Chronic Health Evaluation (APACHE) II score (OR 1.06) were associated with clinically significant hypotension 13 as well as low baseline blood pressure (hazard ratio: 2.42). 9 Although APACHE II scores were not calculated for this study, the SOFA scores above 10 in both groups suggest a very sick cohort of critically ill patients. Lower baseline MAP and more pronounced critical illness were previously established factors for distinctly different groups of critically ill patients, and these findings are now supported by hypotension and bradycardia development in this cohort of critically ill patients with septic shock.
The median times to a hemodynamic event were similar between propofol (1 hour) and dexmedetomidine (2 hours). This was quicker than times found in a study of neurocritical care patients (9.5 vs 13 hours). 3 These differences may reflect the frequent dosage increases for patients receiving dexmedetomidine or the couple of patients who received a loading dose of propofol prior to initiating the infusion. Hypotension and bradycardia following rapid sequence intubation have been shown to occur in one-third and one-quarter of patients, respectively, although the effects from specific medications have not been quantified. 14 These types of bolus doses may reflect the potential for early hemodynamic events in patients and explain some of the findings in our study. For patients with septic shock who are trialed on propofol or dexmedetomidine, if a hemodynamic event does not occur within the first couple of hours, these patients appear less likely to develop such an event and may be safely continued on the therapy in most cases.
There was no difference in the duration of mechanical ventilation between patients sedated with propofol or dexmedetomidine. Both propofol and dexmedetomidine have been shown to reduce duration of mechanical ventilation when compared to other agents 2,15,16 but have similar effects on heterogeneous cohorts of critically ill patients. 2 Similarly, the agents have not shown differences in ICU or hospital lengths of stay or mortality when compared. 2,6 These findings were confirmed in our study. Although dexmedetomidine appears to prevent neuroapoptosis through activation of alpha-2 adrenoceptors, and these neuroprotective effects may be more pronounced in patients with sepsis, 17,18 the specific effects in septic shock in humans have yet to be definitively established. Critically ill adult patients with septic shock do not appear to experience additional benefit with propofol compared to dexmedetomidine in these meaningful clinical outcomes and both can be considered effective options for sedation in this these patients.
This study has specific limitations that were mitigated whenever possible. There are several factors that have the potential to influence hemodynamics that was not controlled for within our study. Assessment of fluid resuscitation after vasopressor and sedative initiation was not assessed within our population, which may have an effect on titration of these agents and potential hypotension development. Concomitant fentanyl use was assessed within our study for potential impact on hypotension, but the rate of fentanyl infusions was not assessed. Similarly, the rate and duration of vasopressors prior to sedative use and hemodynamic event development were not assessed. It is possible that a planned decrease in a vasopressor dosage could have been miscoded as a hypotensive or bradycardic event. Vasopressor agent use was similar between treatment groups. The ICU length of stay may also have been affected by additional variables, which include patients available for care in an intermediate care unit who were boarded in the ICU because of bed availability; however, this should have artificially prolonged ICU length of stay in both groups. This outcome should be evaluated in a larger study. Additionally, the retrospective, observational design of our study may allow for differences in baseline characteristics, and the potential for selection bias with sedative agent selection based off provider preferences or other patient characteristics does exist.
Conclusion
Patients with septic shock receiving continuous infusions of propofol or dexmedetomidine experienced a similar frequency of clinically significant hemodynamic events. The majority of patients with septic shock receiving either of these sedatives did not experience an event, and those patients who did experience an event most frequently did so in the first couple of hours of therapy. Prospective evaluation of risk factors associated with development of hypotension and bradycardia with propofol and dexmedetomidine in patients with septic shock is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.