
Abstract
Objective:
Cardiopulmonary complications/stress are well-known phenomena in patients after aneurysmal subarachnoid hemorrhage (aSAH) and might be associated with an elevated serum troponin I (TNI) level. Since the glucocorticoid hormone cortisol is released during stress situations, the present study was conducted to investigate the influence of serum cortisol (SC) on cardiac and pulmonary parameters in patients after aSAH within the first 24 hours of intensive care unit (ICU) treatment.
Patients and Methods:
We retrospectively analyzed a cohort of 104 patients with aSAH admitted to our emergency department between January 2008 and April 2017. Blood samples were taken to determine SC and TNI. Demographics, initial Glasgow Coma Scale (GCS) score, World Federation of Neurosurgical Societies (WFNS) score, and Fisher grade were evaluated retrospectively. Mean norepinephrine application rate (NAR) in µg/kg/min and mean inspiratory oxygen fraction (OF) within the first 24 hours were defined as cardiopulmonary parameters.
Results:
An elevated SC value was found in 44 (42%) patients, and 27 (26%) patients showed an increased TNI value. In patients with initially increased SC value, a significant higher NAR (P = .04) was needed. Furthermore, patients with initially elevated TNI value had a lower GCS score (P = .0013) and a higher WFNS score (P = .003) on admission and required a higher NAR (P = .02) as well as OF (P = .0008) within the first 24 hours of ICU treatment.
Conclusions:
In the current study, initially elevated SC values were associated with a higher need of NAR within the first 24 hours of ICU treatment after aSAH. Moreover, patients with initially elevated TNI values required an increased NAR and a higher OF so that these biomarkers could be useful to improve ICU treatment.
Keywords
Introduction
Cortisol is a glucocorticoid hormone released in response to stress.
1
The release of serum cortisol (SC) follows a circadian rhythm with peaks between 6 and 8
The impact of initially elevated SC value as an early biomarker on cardiopulmonary parameters (CP) within the first 24 hours after aSAH is still unknown. The purpose of the present study was to evaluate the association of initial SC values and CPs within the first 24 hours of ICU treatment in patients after aSAH.
Patients and Methods
We retrospectively analyzed a consecutive cohort of 321 patients with the diagnosis of SAH who were admitted to our emergency department (ED) from January 2008 to April 2017. The study protocol was approved by the ethical committee of the Justus-Liebig-University (No: 26/14).
Study Design
All patients with aSAH, in who determination of SC value and TNI value was performed on admission were included. The determination of TNI value (ADVIA Centaur TnI-Ultra Assay, Siemens, Germany) and SC value (ADVIA Centaur Cortisol Assay, Siemens, Germany) were taken by blood sample directly on admission. The diagnosis of SAH was made by computer tomography (CT) scan or lumbar puncture if the CT scan was negative for SAH. Evidence of intracranial aneurysm was performed with CT angiography and/or digital cerebral angiography. Exclusion criteria were (1) no determination of SC value and/or TNI value on admission (n = 86); (2) acute cardiac injury due to evidenced coronary artery stenosis in coronary angiography or new wall motion abnormality in echocardiography as well as cardiopulmonary reanimation (n = 19); (3) age under 18 years (n = 2); (4) medication of cortisol (n = 59); (5) adrenal diseases (n = 12); (6) pituitary diseases (n = 9); (7) SAH based on another vascular malformation than an aneurysm (n = 25); and (8) patients with SAH and none evidence of intracranial aneurysm (non-aSAH; n = 5), resulting in a total number of 104 patients. Data were collected retrospectively including demographics, baseline GCS score, hemoglobin value in g/dL (XE 5000; Sysmex, Germany) on admission, intrahospital outcome, procedure of aneurysm treatment (interventional vs surgical treatment), systolic blood pressure and heart beat rate within the first 24 hours, medication history, and World Federation of Neurosurgical Societies (WFNS) score. Baseline Fisher grade was extracted from initial CT scan. 20 The WFNS score and GCS score were determined using the first documented neurological examination at the ambulance through the emergency doctor. We defined the average norepinephrine application rate (NAR) in µg/kg/min and average inspiratory OF within the first 24 hours of ICU treatment as CPs. We analyzed the first chest X-ray after admission in all patients concerning the occurrence of (1) pulmonary edema, (2) pneumothorax, (3) pulmonary infiltrate, and (4) pulmonary atelectasis. For occurrence of delayed cerebral ischemia, the last CT scan within inpatient treatment was analyzed. Intrahospital outcome was evaluated with the modified Rankin Scale (mRS) at discharge. 21
Clinical Management
All patients were referred primary to 1 of the 2 EDs of our university hospital (internal/neurological ED or surgical ED). After making the diagnosis of aSAH, all patients were further treated at our ICU. Systolic blood pressure was kept between 100 and 130 mm Hg for patients with aneurysmal SAH before treatment and 140 and 160 mm Hg after surgical or interventional treatment of ruptured aneurysms within the first 24 hours of ICU treatment. In all patients, invasive blood pressure measurement was performed (Combitrans Monitoring Set Arteriell; B. Braun, Melsungen, Germany). Oxygen saturation was measured by a pulse oximeter (Nellcor Adult SpO2 Sensor; Covidien IIc, Massachusetts) and kept ≥95%. Arterial oxygen partial pressure was measured by taken arterial blood samples and using blood gas analysis (ABL 800 FLEX; Radiometer Copenhagen, Krefeld, Germany) every 4 hours. Target arterial oxygen partial pressure was ≥100 mm Hg within the first 24 hours after SAH. Application of intravenous drugs was routinely performed through a central venous catheter (Arrow International, Inc., Reading, Pennsylvania). Intubation and mechanical ventilation in a pressure-controlled mode were started, if the GCS score was lower than 8 or the patients developed respiratory insufficient. Sedation was performed with propofol and sufentanil to a Richmond Agitation-Sedation Scale score of −4 within the first 24 hours of ICU treatment. 22 In all patients with initially increased TNI value, an electrocardiogram and echocardiography was performed. In case of ST-segment elevation or depression in the electrocardiogram and/or new or suspect wall motion abnormality in the echocardiogram as indicator of an acute and real cardiac injury, patients were transferred to coronary angiography and were excluded from the study. All other patients with initial elevation in TNI were treated with best medical care at our ICU, and serial measurements of TNI were not routinely performed based on the lack of therapeutic consequence. Elevation of TNI value in these patients were interpreted as ‘cerebral’ and not cardiac triggered. Initial blood samples were taken at the ED, and determination of troponin I and cortisol was routinely performed in all patients, independent of current clinical somatology, at the ED of internal medicine and neurology (conservative blood sample spectrum). In contrast, the determination of TNI and cortisol at the surgical ED was only performed if it was clinically indicated (eg, ST-segment elevation or depression in the electrocardiogram, cardiac arrhythmia, or angina pectoris).
To analyze the average NAR and OF, we used the continuously digital recorded NAR per minute and inspiratory OF in all patients (n = 104) from admission on ICU up to 24 hours.
Statistical Analysis
For analyzing the impact of initially cortisol value on cardiac and pulmonary parameters within the first 24 hours, patients were stratified into 2 groups, respectively, (1) patients with a SC value >26 µg/dL (SC positive) and (2) patients with a SC value ≤26 µg/dL (SC negative). The cut off level for stratification was calculated by using the average cortisol value of the entire study population (26 µg/dL) on admission. Furthermore, the entire study population was divided into (3) patients with initially elevated TNI value > 0.05 µg/L (TNI positive) and (4) patients with initial negative TNI value ≤ 0.05 µg/L (TNI negative). A cut off value for TNI > 0.05 µg/L is defined as positive at our laboratory test.
Data are expressed as mean (standard deviation) if normally distributed and as median for parameters with non-normal distribution. χ2 test and t test were used to compare the parameters of the different groups. Correlations were assessed by Spearman correlation. For data analysis, the statistic program GraphPad Prism Version 5 (GraphPad Software, Inc, La Jolla, California) was used. A P < .05 was defined as the level of significance.
Results
The study population consisted of a total of 104 patients with a mean age of 57.2 (12.1) years (range: 28-89 years). There were 57 female and 47 male patients. Mean SC level on admission was 26.1 ± 17.9 µg/dL. In the entire study population, 44 (42%) patients had an SC value >26 µg/dL, and 27 (26%) patients had an increased TNI value > 0.05 µg/L. Increased SC value on admission was found in 26 (96%) of 27 patients with initially elevated TNI. The median WFNS score of the entire study population on admission was 3 (range: 1-5), and 70 patients (67%) were intubated and mechanically ventilated within the first 24 hours of ICU treatment. Treatment of ruptured aneurysm was performed within the first 24 hours after admission in all cases. Surgical treatment (clipping) was performed 49 (47%) patients, and 55 (53%) patients were treated with an interventional procedure (coiling). We observed an average systolic blood pressure of 132 ± 14 mm Hg and arterial oxygen partial pressure of 111 ± 30 mm Hg as well as an oxygen saturation of 98% ± 2%. At discharge, the median mRS score was 4 (range: 0-6), and delayed cerebral ischemia occurred in 14 (14%) patients. We identify the occurrence of (1) pulmonary edema (n = 6), (2) pneumothorax (n = 8), (3) pulmonary infiltrate (n = 26), and (4) pulmonary atelectasis (n = 11) in the first chest X-ray after admission. Demographic data are summarized in Table 1.
Baseline Data.
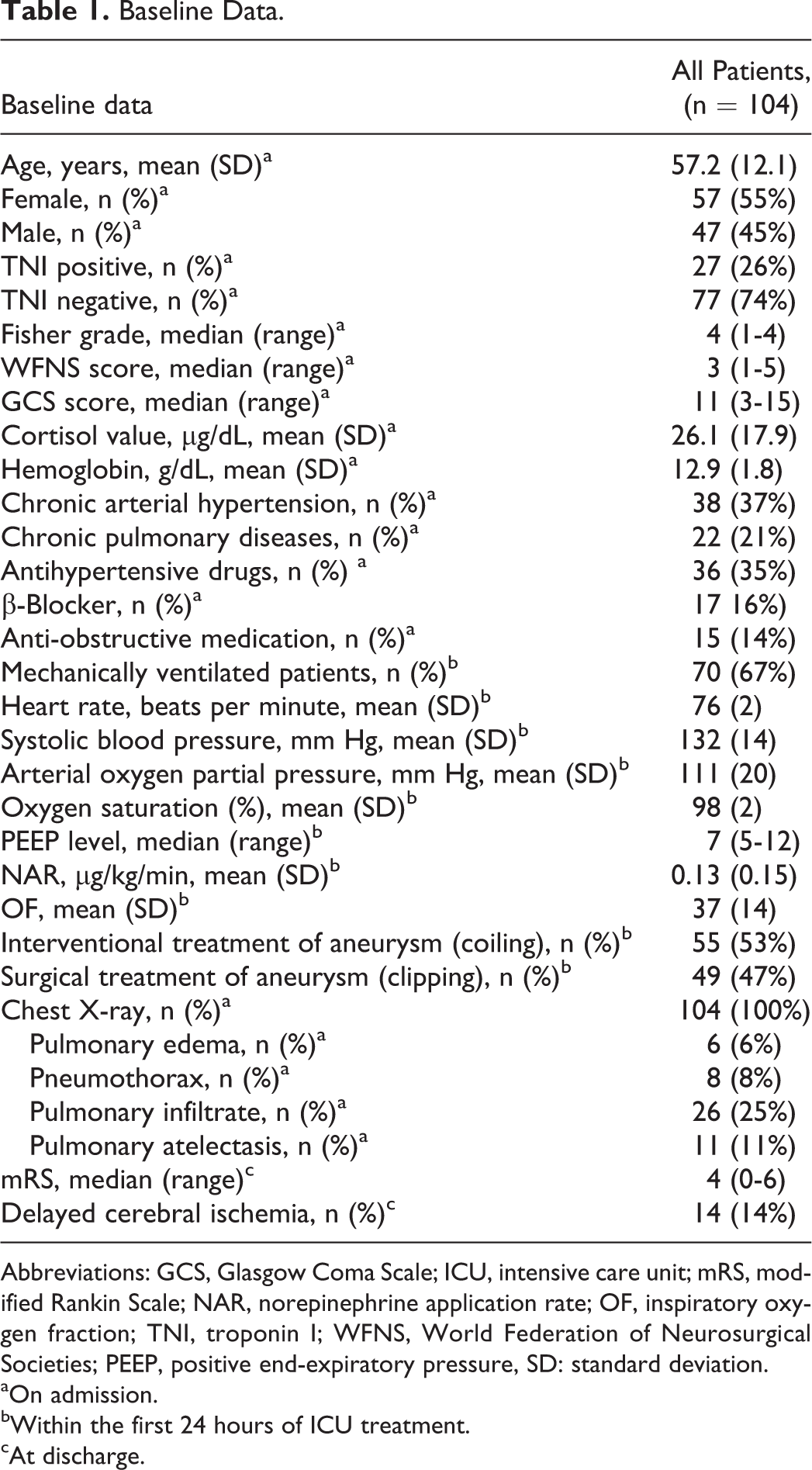
Abbreviations: GCS, Glasgow Coma Scale; ICU, intensive care unit; mRS, modified Rankin Scale; NAR, norepinephrine application rate; OF, inspiratory oxygen fraction; TNI, troponin I; WFNS, World Federation of Neurosurgical Societies; PEEP, positive end-expiratory pressure, SD: standard deviation.
aOn admission.
bWithin the first 24 hours of ICU treatment.
cAt discharge.
Patients with initially higher SC value had a higher Fisher grade (P = .007) on admission. There was no significant difference between the SC-positive group and SC-negative group regarding age (P = .45), gender (P = .45), treatment of ruptured aneurysm (P = .91) as well as WFNS score (P = .6) and GCS score (P = .78) on admission. Furthermore, no significant difference in the preexisting of chronic arterial hypertension (P = .7), chronic pulmonary diseases (P = .88), antihypertensive drugs (P = .7) as well as anti-obstructive medication (P = .45) was found. Moreover, no significant difference in regard of inspiratory OF (P = .43) and median positive end-expiratory pressure (PEEP) level (P = .65) was observed to accomplish target oxygen saturation and arterial oxygen partial pressure in both groups within the first 24 hours. However, a significant higher average NAR was required in patients with a cortisol value >26 µg/dL (SC positive) on admission in comparison to the SC-negative (P = .04) cohort within the first 24 hours of ICU treatment. At discharge, no difference between both groups concerning median mRS score (P = .14) and occurrence of delayed cerebral ischemia (P = .3) was found (Table 2). Moreover, mean cortisol level in patients admitted between 12
Serum Cortisol Value.
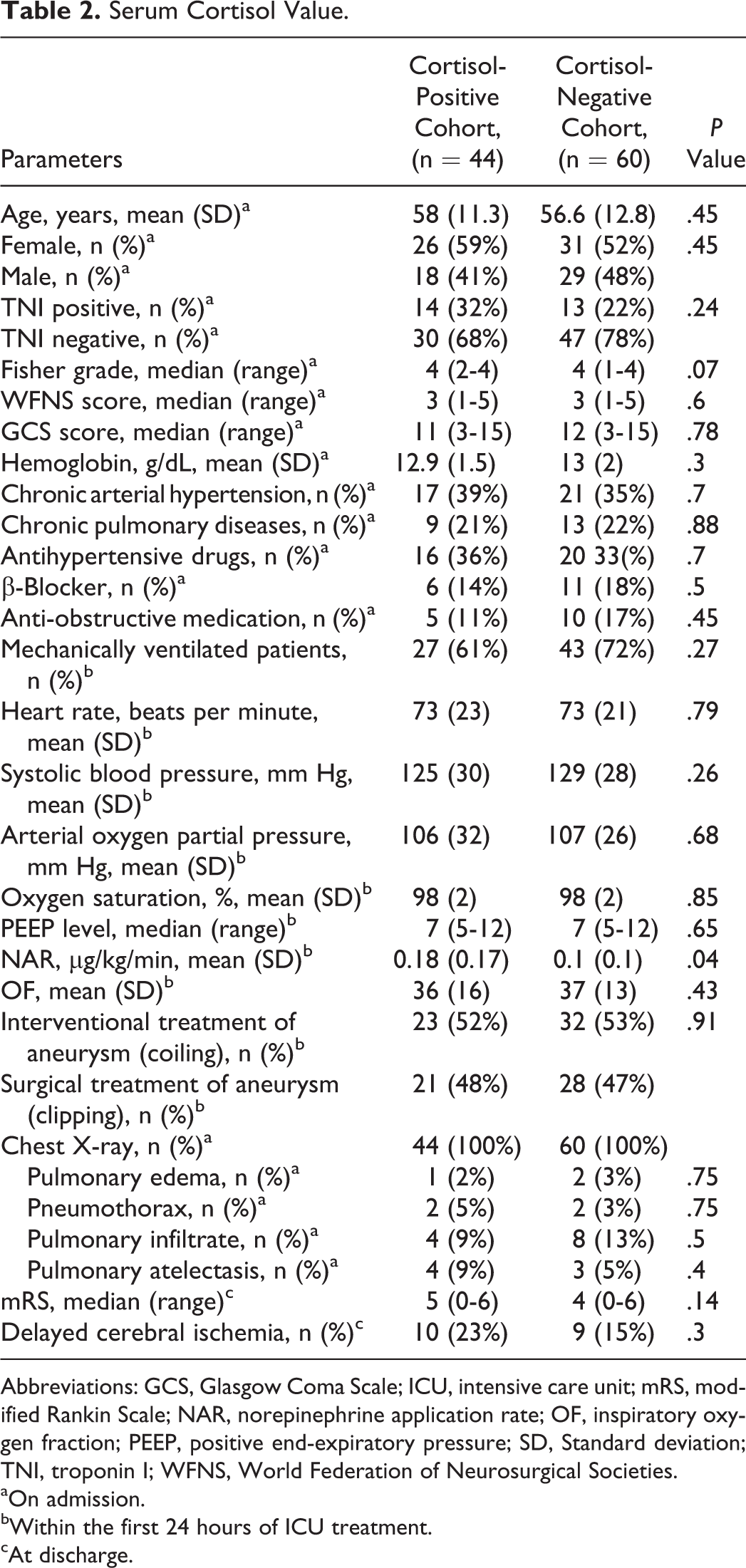
Abbreviations: GCS, Glasgow Coma Scale; ICU, intensive care unit; mRS, modified Rankin Scale; NAR, norepinephrine application rate; OF, inspiratory oxygen fraction; PEEP, positive end-expiratory pressure; SD, Standard deviation; TNI, troponin I; WFNS, World Federation of Neurosurgical Societies.
aOn admission.
bWithin the first 24 hours of ICU treatment.
cAt discharge.
There was no significant difference between the TNI-positive group and TNI-negative group regarding age (P = .75), gender (P = .15), mean cortisol value on admission (P = .12), treatment of ruptured aneurysm (P = .75) as well as preexisting chronic arterial hypertension (P = .9) and chronic pulmonary diseases (P = .48). However, patients with initially elevated TNI value had a significantly higher median WFNS score (P = .003) and lower median GCS score (P = .0013) on admission as well as a higher mRS score at discharge (P = .04). In the TNI-positive cohort, there were significantly more patients intubated and mechanically ventilated (P = .006) within the first 24 hours. In addition, patients with elevated TNI value on admission required a higher average OF (P = .0008) and NAR (P = .02) to accomplish the targets of oxygen saturation, average arterial oxygen partial pressure, and systolic blood pressure within the first 24 hours of ICU treatment after aSAH as shown in Table 3. Furthermore, there was no significant correlation (r = .16, confidence interval: −0.04 to 0.35; P = .1) between TNI value and SC value in the investigated cohorts.
Troponin I Value.
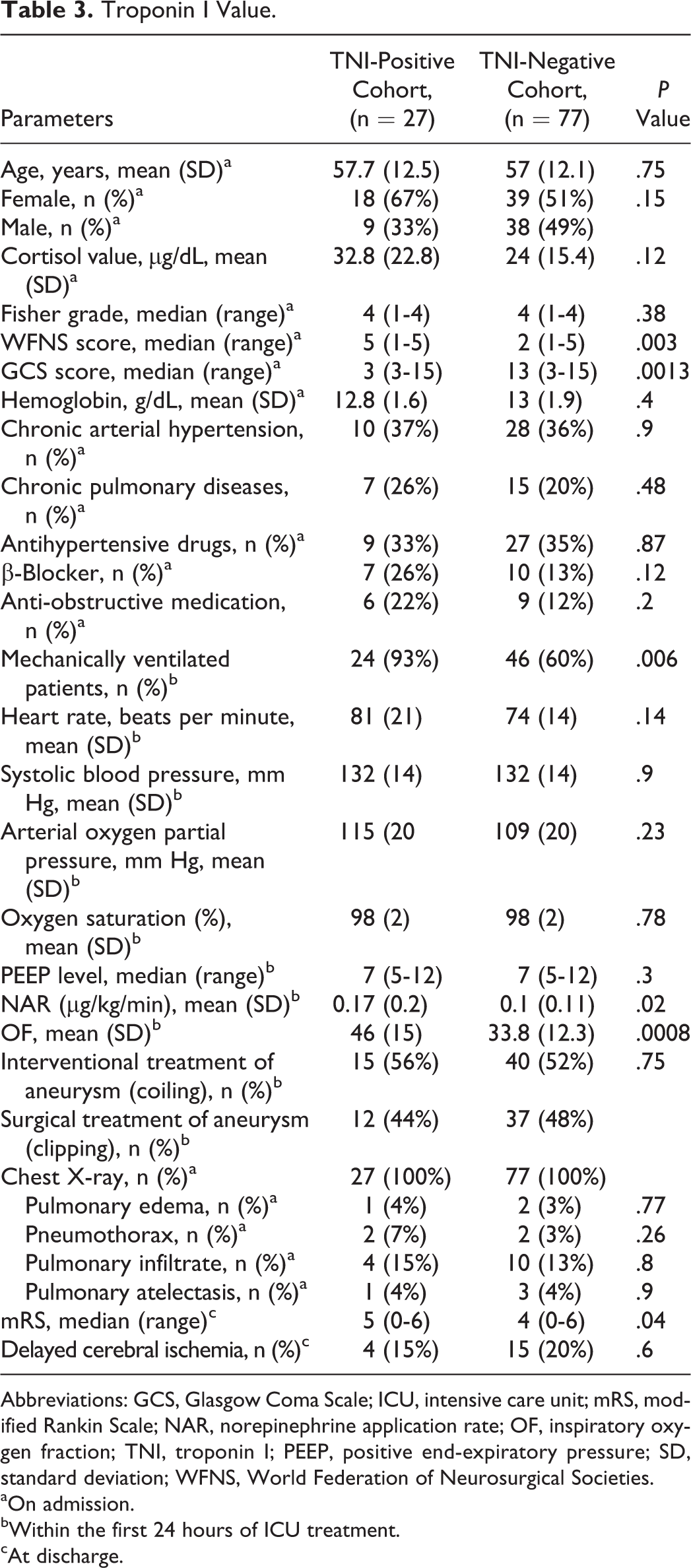
Abbreviations: GCS, Glasgow Coma Scale; ICU, intensive care unit; mRS, modified Rankin Scale; NAR, norepinephrine application rate; OF, inspiratory oxygen fraction; TNI, troponin I; PEEP, positive end-expiratory pressure; SD, standard deviation; WFNS, World Federation of Neurosurgical Societies.
aOn admission.
bWithin the first 24 hours of ICU treatment.
cAt discharge.
Discussion
The hypothalamic–pituitary–adrenal axis is an important part of human’s natural response to acute stress situations. One of the most important stress hormones is cortisol. Hyperglycemia, retention of sodium, and hypertension are physiological functions of cortisol. Several studies reported about increased cortisol levels in patients with SAH and its association with electrocardiographic abnormalities, poor clinical outcome, and mortality. 2,23 Furthermore, elevated TNI value in combination with electrocardiographic and echocardiographic abnormalities could be a sensitive marker for cardiac stress/injury and is found in 20% to 40% of patients after aSAH. 14,16,24 To our knowledge, this is the first study to investigate the association of SC value, as stress biomarker, on cardiac and pulmonary parameters within the first 24 hours of ICU treatment in patients after aSAH.
Cortisol
In the entire study population, elevated cortisol values on admission were observed in 42% (n = 44) of the patients, with no difference concerning time of admission. We identify no significant differences concerning demographic data, baseline clinical scores, preexistence of chronic arterial hypertension and chronic pulmonary diseases, medication history as well as mRS score and occurrence of delayed cerebral ischemia at discharge. Furthermore, no significant difference regarding inspiratory OF and median PEEP level was observed to accomplish target oxygen saturation and average arterial oxygen partial pressure in both groups within the first 24 hours so that cortisol value on admission had no impact on pulmonary parameters within the first 24 hours. However, we identify a significant higher need of NAR within the first 24 hours of ICU treatment for the SC-positive cohort compared to the SC-negative cohort (P = .04). These results indicate that patients with initially increased SC values required more circulatory support. Increased SC values on admission could reveal an acute stress situation. In such stress situations, the pathophysiological response of the hypothalamic–pituitary–adrenal axis releases stress hormones such as cortisol and catecholamine. Furthermore, an initial increase in SC value could indicate a currently acute recompensation mechanism of the hypothalamic–pituitary–adrenal axis due to the acute stress situation after aSAH to stabilize cardiac and pulmonary functions. Therefore, patients with initially increased SC values after aSAH probably need more circulatory support within the first 24 hours of ICU treatment.
Biomarker Troponin I
In comparison to previous studies, our prevalence of 26% patients with an increased TNI value on admission is similar. 14,25 There was no significant difference with respect to demographic data, age, mean cortisol value on admission, preexisting chronic arterial hypertension and chronic pulmonary diseases, medication history as well as occurrence of delayed cerebral ischemia. However, patients with initially increased TNI value required a significantly higher NAR (P = .02) as well as inspiratory OF (P = .0008) to accomplish targets of systolic blood pressure and oxygen saturation and arterial partial pressure within the first 24 hours of ICU treatment after sSAH. Moreover, a significant lower GCS score (P = .0013), higher WFNS score (P = .003) on admission as well as a higher median mRS score (P = .04) at discharge was observed in the TNI-positive group. In addition, a significant higher rate of intubated and mechanically ventilated patients was found in TNI-positive group (P = .006). Regardless of the worse neurological condition and higher rate of intubated and mechanically ventilated patients in the TNI-positive group, the target values of (1) systolic blood pressure, (2) oxygen saturation, (3) arterial partial pressure, and (4) depth of the sedation (Richmond Agitation-Sedation Scale score of −4) were equal in all patients within the first 24 hours so that to our opinion both groups are comparable with regard to NAR and OF. These results suggest that an initially elevated TNI value could be an additional sensitive biomarker for the need of more circulation and pulmonary support in patients within the first 24 hours of ICU treatment after aSAH. Previous studies reported that increased TNI values in patients with aSAH are not associated with coronary stenosis. 14 Moreover, myocardial dysfunction in the absence of coronary stenosis has been reported in animal models of SAH. 26 In addition, Yoneda et al reported about an association of lower cardiac index on day 1 and day 2 in patients with severe SAH. 27 The pathophysiological pathways of cardiac dysfunction without any coronary artery stenosis or decompensated heart failure in cases of consecutive elevated serum TNI values after aSAH are still unknown as well as the pathophysiological pathways of NPE. Obata et al reported that pulmonary edema after SAH determines cardiac failure as well as inflammatory (ie, noncardiogenic) conditions. 28 Previous studies report about a correlation of initial raised cardiac biomarkers and the occurrence of pulmonary complications, for example, NPE, so that cardiac biomarkers could probably be sensitive markers to predict pulmonary complications in patients after aSAH. 16,19 An interpretation for these results could be that patients with initial raised TNI values have more reversible regional wall motion abnormalities with consecutive lower blood pressure and reduced oxygen perfusion of the myocardium. Thus, patients required a higher NAR for blood pressure treatment and inspiratory OF for ventilation.
In addition, there was no significant difference as well as correlation (r = .16, confidence interval: −0.04 to 0.35; P = .1) between TNI value and SC value in the investigated groups, so that SC value and TNI value seem not to affect each other. We found no correlation between SC and TNI values, but in our opinion, both parameters separately could be helpful to identify patients at high risk of cardiac and pulmonary complications.
Limitations
The results of the present study should be interpreted with caution. There are several limitations in the present study. The most important is the retrospective study design with its well-known limitations. Another limitation was the difference in target values of systolic blood pressure within the first 24 hours of ICU treatment after aSAH. In patients, before treatment of a ruptured aneurysm, a lower blood pressure (100-130 mm Hg) to prevent rebleeding was performed than in patients after surgical or interventional treatment (140-160 mm Hg). In such patients, a higher blood pressure was performed to optimize intracerebral perfusion and prevent cerebral ischemia. However, treatment of aneurysm was performed in all patients within the first 24 hours so that management of systolic blood pressure is comparable in all patients. In addition, management of systolic pressure changes frequently during the acute phase after aneurysmal SAH depending on presence of vasospasm, although none of our patients had raised values in transcranial Doppler sonography within the first 24 hours of ICU treatment. Moreover, in this study, only a few of CPs were investigated. To analyze more cardiac and pulmonary parameters (eg, global end-diastolic volume index, pulmonary vascular permeability index, cardiac index, or extravascular lung water), a pulse contour cardiac output system (PiCCO) could be used as described in previous studies. 29 -31 Tagami et al reported about the impact of global end-diastolic volume index on delayed cerebral ischemia and pulmonary edema after SAH during complete inpatient treatment. 31 The PiCCO catheters were routinely used in patients with septic shock at our ICU, however, not in patients after SAH. Furthermore, no determination of SC value or TNI value was performed in 86 patients on admission due to an inhomogeneous admission procedure for laboratory test of internal medicine/neurology and surgical ED. Another limitation is the different time period between admission on the ICU and occurrence of SAH. However, a minute analysis of this important fact is retrospectively very difficult due to an inhomogeneous documentation. Finally, ECG changes could not be evaluated minutely. A 3-lead ECG was performed in all patients at our ICU directly on patients monitor; however, these ECGs were unfortunately not digital recorded. Due to this fact and the retrospective design of the study, an exact analysis of ECG abnormalities with our results was unpleasantly not possible; however, this important fact should be investigated in a further prospective study.
Despite these limitations, this study could be helpful to identify patients who could potentially need more circulation and pulmonary support to accomplish the desired levels of blood pressure, arterial oxygen partial pressure, and oxygen saturation within the first 24 hours of ICU treatment after aSAH. These patients need special attention and could probably benefit from an early intensive and invasive hemodynamic monitoring, for example, using a PiCCO. According to our experience, these biomarkers could be useful to identify critical patients and to improve ICU treatment strategies in patients within the first 24 hours after aSAH.
Conclusion
This study evaluated for the first time the influence of initial SC value on cardiac and pulmonary parameters within the first 24 hours of ICU treatment in patients after aSAH. Our results indicate that initially elevated SC values were associated with a higher need of NAR, and patients with initially increased TNI value required a higher NAR and OF within the first 24 hours of ICU treatment. Early biomarkers such as TNI and SC may improve ICU treatment within the first 24 hours in patients after aSAH. Nevertheless, our preliminary results should be evaluated in a prospective manner with more invasive and noninvasive cardiac and pulmonary parameters.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.