
Abstract
Background:
The management of refractory septic shock remains a major challenge in critical care and its early indicators are not fully understood. We hypothesized that the maximum norepinephrine dosage within 24 hours of intensive care unit (ICU) admission may be a useful indicator of early mortality in patients with septic shock.
Methods:
In this retrospective single-center observational study, patients with septic shock admitted to the emergency ICU of an academic medical center between April 2011 and March 2017 were included. Individuals with cardiac arrest and those with do-not-resuscitate orders before admission were excluded. We analyzed if the maximum norepinephrine dosage within 24 hours of ICU admission (MD24) was associated with 7-day mortality.
Results:
Among 152 patients with septic shock, 20 (15%) did not survive by day 7. The receiver operating characteristic curve analysis for predicting 7-day mortality revealed a cutoff of MD24 of 0.6 μg/kg/min (sensitivity 47%, specificity 93%). In the multivariable regression analysis, a higher MD24 was significantly associated with 7-day mortality (odds ratio: 7.20; 95% confidence interval [CI]: 2.02-25.7; P = .002) but not with 30-day mortality. Using the inverse probability of treatment weighting method in a propensity scoring analysis, a higher MD24 was significantly associated with 7-day (hazard ratio [HR]: 8.9; 95% CI: 3.2-25.0; P < .001) and 30-day mortality (HR: 2.7; 95% CI: 1.2-5.8; P = .012).
Conclusions:
An MD24 ≥0.6 μg/kg/min was significantly associated with 7-day mortality in patients with septic shock and may therefore be a useful indicator of refractory septic shock.
Background
Sepsis is commonly encountered in intensive care units (ICUs) worldwide. 1 Despite improvements in treatment strategies over the past decade, 2,3 it remains the leading cause of the death in patients admitted to noncardiac ICUs. 1 Refractory shock is one of the major causes of death in patients with sepsis, accounting for 40% of deaths. 4 To improve the management of septic shock, early recognition of refractory shock is necessary.
The definition of refractory septic shock varies from persistent shock in spite of optimized therapy 5,6 to a vasopressor requirement of >0.5 to 1 μg/kg/min of norepinephrine or equivalent, 7,8 and no consensus about its criteria has been reached yet. The effect of the norepinephrine dosage on mortality in patients with septic shock is controversial. 9 Several studies have described a subgroup of septic shock receiving high-dose vasopressors (HDVs). 10 –12 Some authors reported that patients with septic shock who received HDVs showed almost 100% mortality. 10,11 Auchet et al analyzed a cohort of 106 patients receiving HDVs and concluded that HDVs may be useful for the management of refractory shock, considering the favorable 28-day survival in their study compared to previous reports, while they underscored that the maximum vasopressor dose should not be used as the sole factor to assess prognosis. 12 Since these studies did not include all patients with septic shock, 10 - 12 a better understanding of the role of catecholamine dosage as an indicator for refractory shock remains to be established. Several articles reported the usefulness of cumulative dose of vasopressors in the prediction of mortality in septic shock, 12 , 13 while its clinical application is currently limited due to the difficulty in calculation especially in the early phase. Conrad et al reported that the hemodynamic response after 6 μg/kg/min of phenylephrine administration can be used to predict refractory septic shock. 14 However, as the clinical application of phenylephrine in patients with septic shock is limited according to current guidelines, 2 another indicator of refractory shock is needed. We hypothesized that the maximum norepinephrine dosage within 24 hours of ICU admission (MD24) may be a useful early indicator of refractory shock.
Methods
Study Setting and Population
In this retrospective single-center observational study, we included patients with septic shock admitted to the emergency ICU of the Fujita Health University Hospital between April 2011 and March 2017. The Fujita Health University Hospital is a tertiary medical center with 1435 beds, including 9 ICUs. The emergency ICU contains 10 beds to provide care for those admitted from the emergency department.
Eligible patients were patients with septic shock aged >18 years. Septic shock was defined according to the Sepsis-3 definition. 15 Individuals with cardiac arrest and those with do-not-resuscitate orders before ICU admission were excluded.
Initial Management of Septic Shock
Patients with septic shock were treated according to the current guidelines for the management of septic shock. 2 After adequate fluid resuscitation (administration of more than 30 mL/kg of crystalloid) that was initiated upon arrival at the hospital, norepinephrine was titrated to obtain a mean arterial pressure >65 mm Hg. Vasopressin 0.02 to 0.03 units/min and hydrocortisone 200 mg/d were administered when considered appropriate by the attending physician at the emergency ICU.
Variables of Interest and Outcome Measurements
Data were retrospectively collected from electronic medical charts. The variables of interest included patient characteristics (age, sex, body mass index, and focus of infection), the sequential organ failure assessment (SOFA) score and Acute Physiology And Chronic Health Evaluation (APACHE) II scores on the day of ICU admission, laboratory data at the time of ICU admission, the MD24, and adjunctive therapy (vasopressin, steroid, renal replacement therapy [RRT]). The MD24 was calculated by dividing norepinephrine dosage by actual body weight.
The primary end point was 7-day mortality; this was chosen to analyze cause-specific mortality due to refractory shock. 4 The secondary end point was 30-day mortality.
Statistical Analysis
Continuous variables are expressed as means ± standard deviations or medians and interquartile ranges (25th-75th percentiles), as appropriate, and were compared using the Student t test or Mann-Whitney U test, respectively. Categorical variables are shown as numbers (%) and compared using the Fisher exact test. Receiver operating characteristic (ROC) curve analysis was performed to assess the optimal cutoff of the MD24. The optimal cutoff was defined as the point of the maximum sum of sensitivity and specificity results. The MD24 was then converted into categorical variables using this cutoff.
The associations between the variables of interest and outcomes were assessed using a multivariable logistic regression model. Clinically and biologically plausible variables, namely the MD24, an SOFA score ≥14, patient age, serum lactate level, steroid and vasopressin use, and RRT were considered in the model. Based on a previous study, the SOFA score was converted into a categorical variable with a cutoff of 14. 14 The effect of the MD24 on mortality was assessed using a Cox proportional hazards model with and without inverse probability of treatment weighting (IPTW), using propensity score adjustment. The R (version 3.4.3) and EZR software (version 1.36) were used for all statistical analyses (Saitama Medical Center, Jichi Medical University, Saitama, Japan). 16
Results
Baseline Patient Characteristics
Of 177 eligible patients, 9 and 16 patients were excluded for having do-not-resuscitate orders and due to cardiac arrest before ICU admission, respectively. Thus, 152 patients were included in the final analysis.
Table 1 shows the baseline characteristics of the patients. The median SOFA score was 11 (9-13), and the median MD 24 was 0.24 (0.16-0.38) μg/kg/min. Vasopressin and steroid were administered in 58 (38%) and 67 (44%) cases, respectively. Twenty (15%) patients died within 1 week and 48 (32%) within 1 month. Patients not surviving by day 7 had a higher MD24, higher APACHE II and SOFA scores, a higher incidence of pneumonia, and a higher rate of vasopressin use.
Patient Characteristics.a
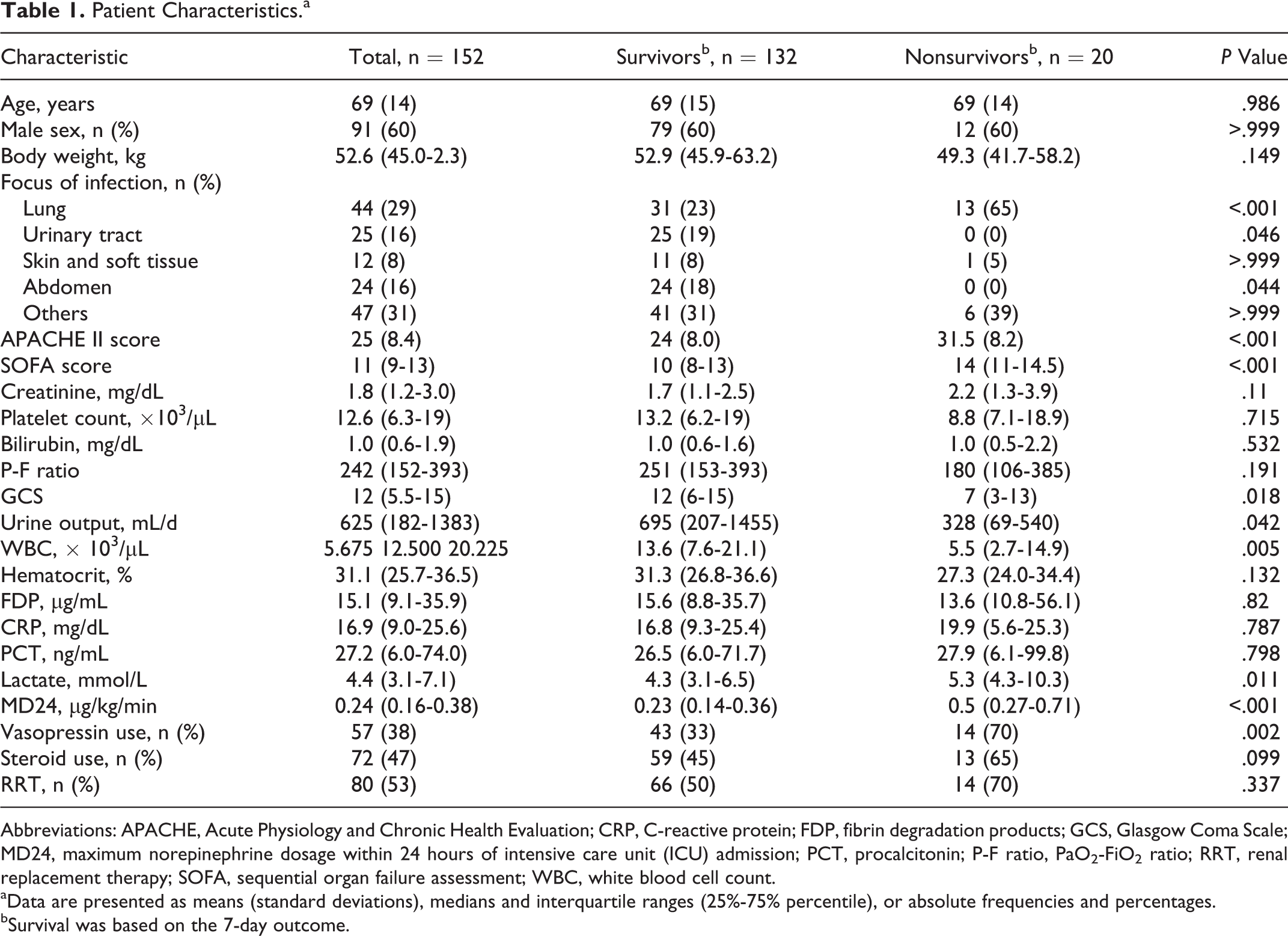
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; CRP, C-reactive protein; FDP, fibrin degradation products; GCS, Glasgow Coma Scale; MD24, maximum norepinephrine dosage within 24 hours of intensive care unit (ICU) admission; PCT, procalcitonin; P-F ratio, PaO2-FiO2 ratio; RRT, renal replacement therapy; SOFA, sequential organ failure assessment; WBC, white blood cell count.
aData are presented as means (standard deviations), medians and interquartile ranges (25%-75% percentile), or absolute frequencies and percentages.
bSurvival was based on the 7-day outcome.
Receiver Operating Characteristic Analysis
The ROC curve of the MD24 to predict 7-day mortality is shown in Figure 1. The area under the curve of the ROC was 0.777 (95% confidence interval [CI]: 0.661-0.894). The optimal cutoff value of the MD24 to predict 7-day mortality was 0.6 µg/kg/min, with a sensitivity of 47% and specificity of 93%. We used this cutoff for all further analyses.
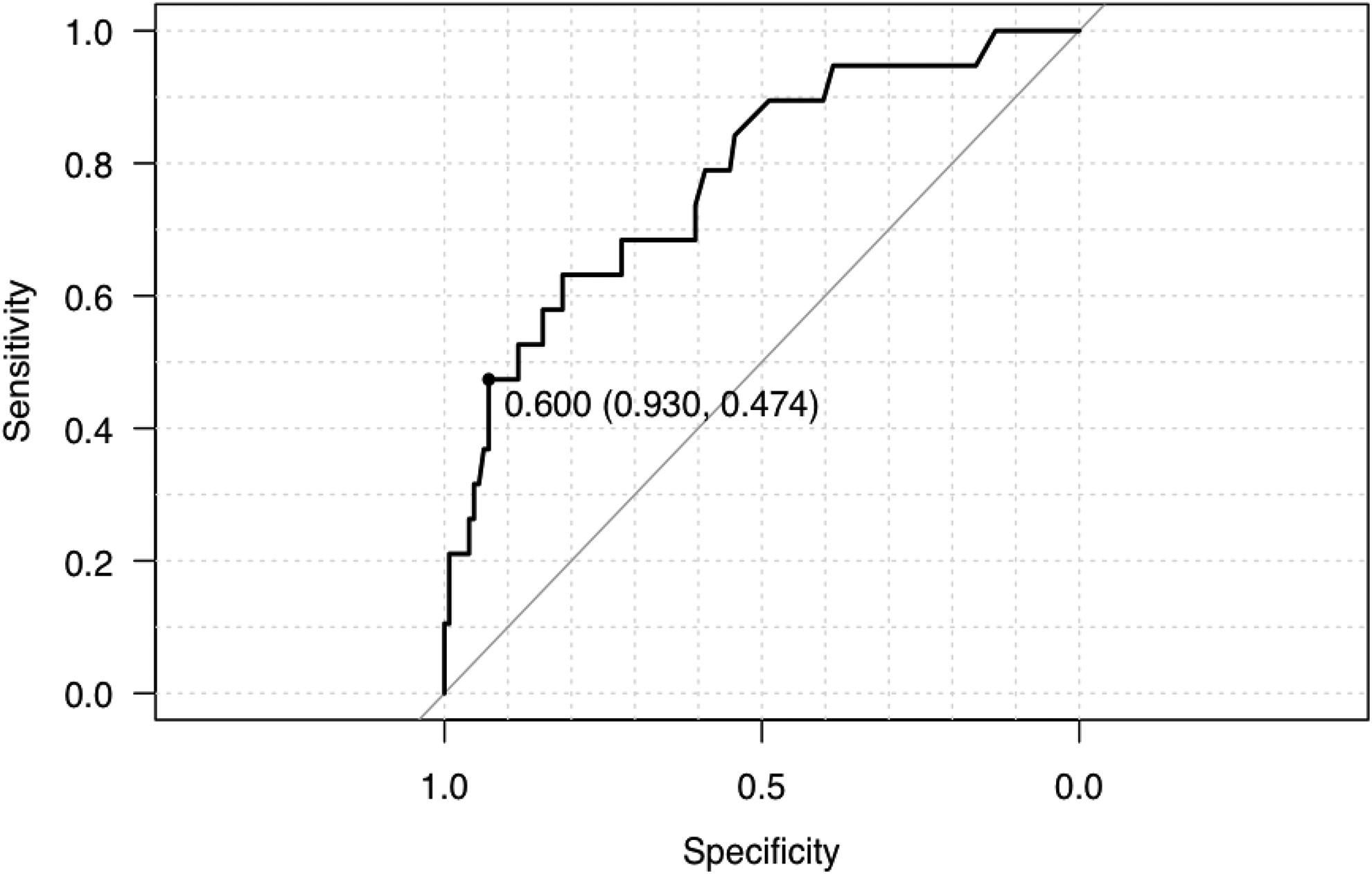
Receiver operating characteristic (ROC) curve using MD24 for predicting 7-day mortality. MD24, maximum dosage of norepinephrine within 24 hours of intensive care unit (ICU) admission.
Association Between the MD24 and Mortality
Table 2 shows the results of the multivariable logistic regression analysis. The MD24 (odds ratio [OR]: 6.98; 95% CI: 1.94-25.2; P = .003) and SOFA score (OR: 5.25; 95% CI: 1.54-17.8; P = .008) were independently associated with 7-day mortality. In contrast, the MD24 did not show a significant association with 30-day mortality.
Multivariable Logistic Regression Analysis.
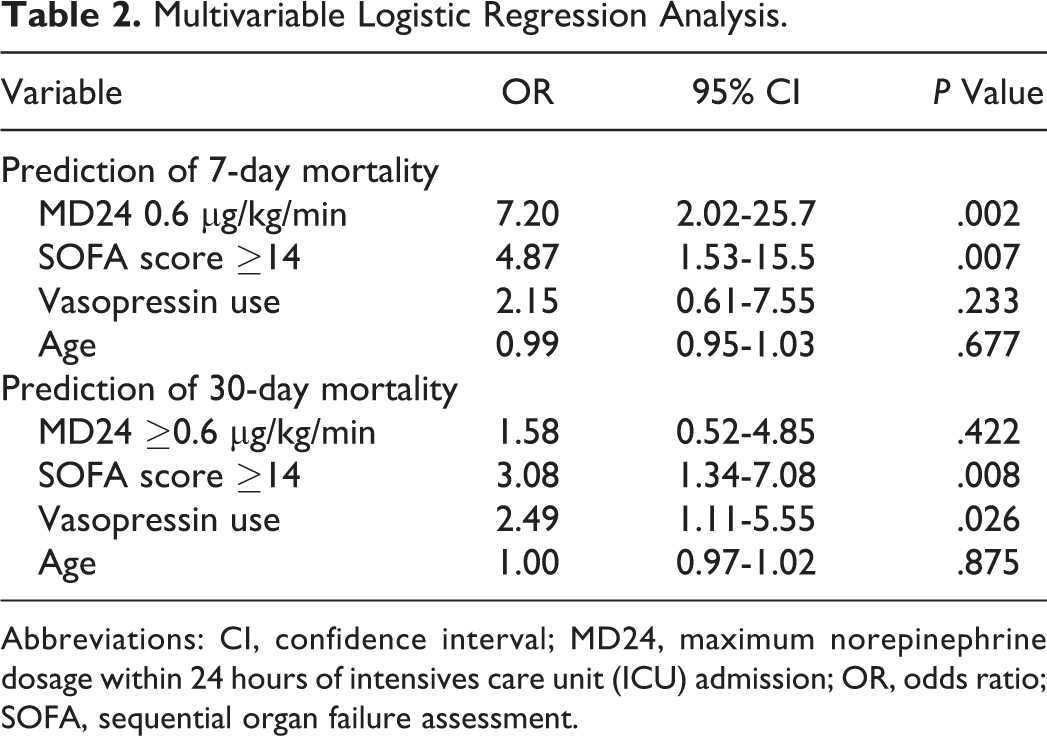
Abbreviations: CI, confidence interval; MD24, maximum norepinephrine dosage within 24 hours of intensives care unit (ICU) admission; OR, odds ratio; SOFA, sequential organ failure assessment.
The adjusted estimated survival curves are depicted in Figure 2. The hazard ratios for 7- and 30-day mortality based on the MD24, adjusted by IPTW using propensity scoring, were 8.9 (95% CI: 3.2-25.0, P < .001) and 2.7 (95% CI: 1.2-5.8, P = .034) respectively (Table 3), suggesting that an MD24 ≥0.6 µg/kg/min was associated with an increased risk of death; this association was more obvious in the first 7 days.
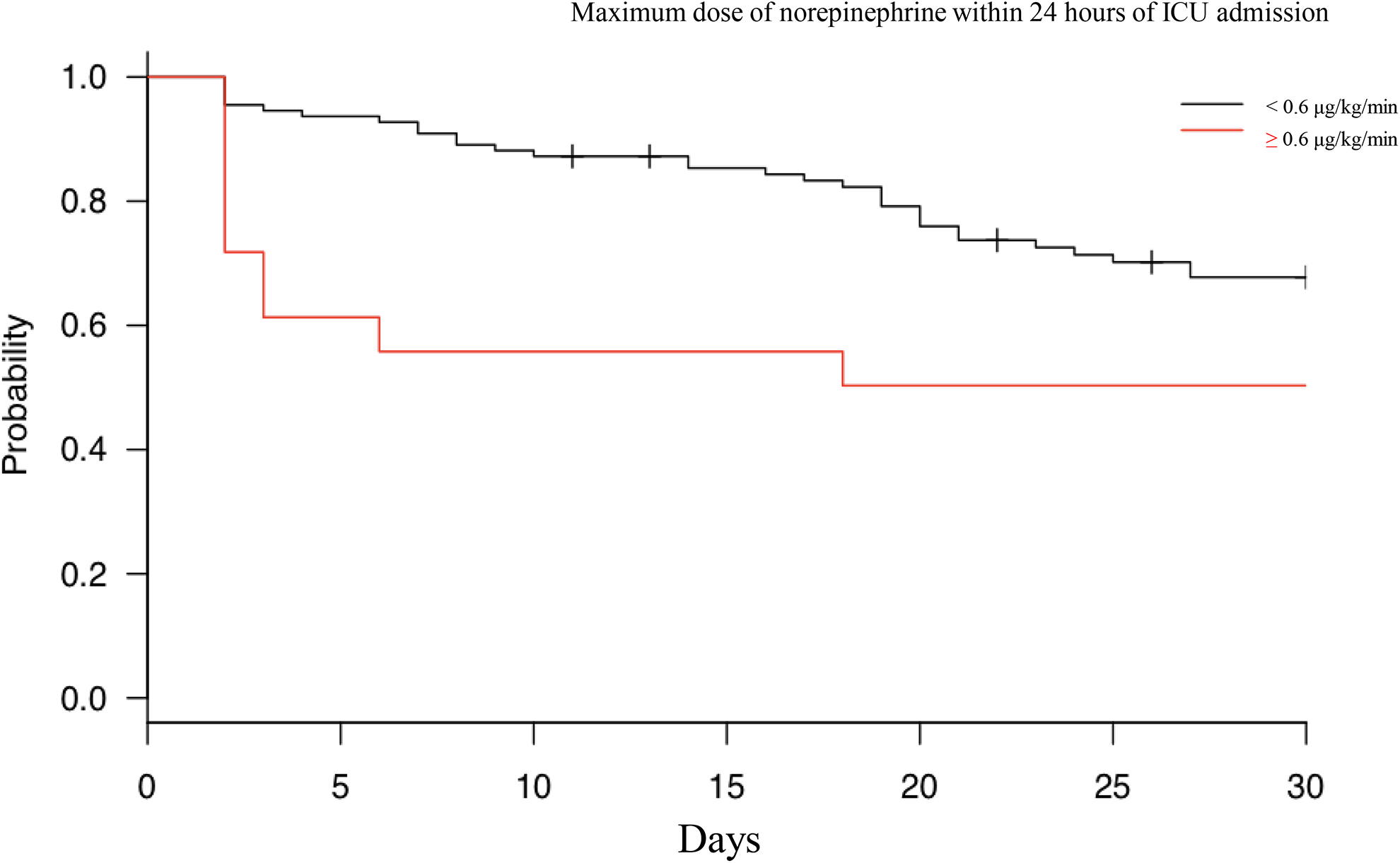
Adjusted estimated survival curves. ICU indicates intensive care unit.
Hazard Ratios for Mortality Based on an MD24 ≥0.6 μg/kg/min.
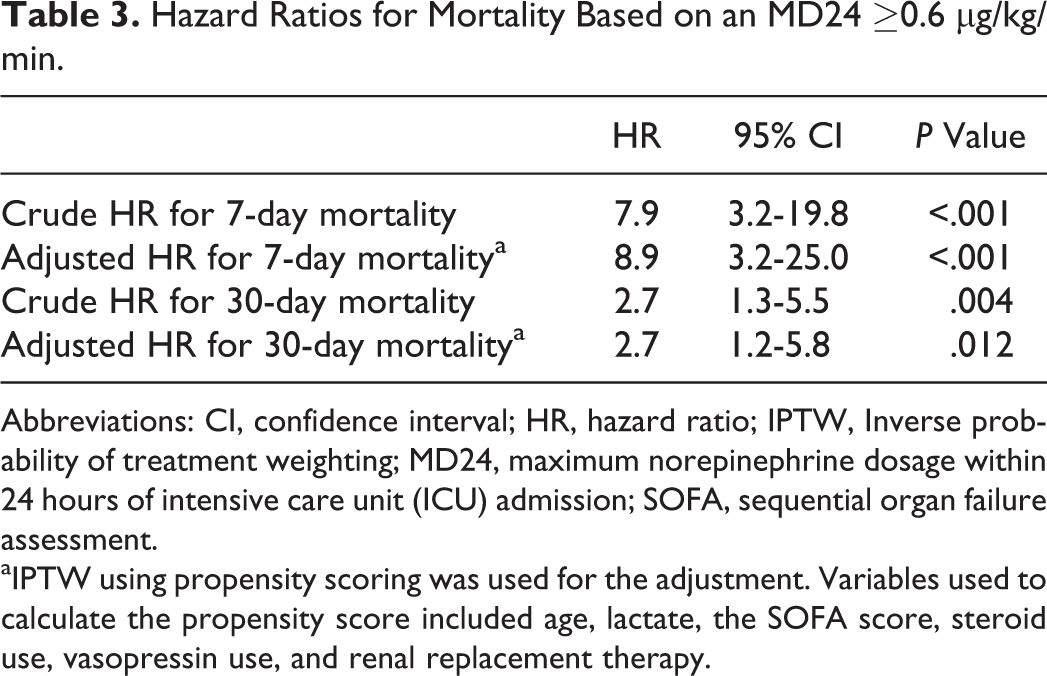
Abbreviations: CI, confidence interval; HR, hazard ratio; IPTW, Inverse probability of treatment weighting; MD24, maximum norepinephrine dosage within 24 hours of intensive care unit (ICU) admission; SOFA, sequential organ failure assessment.
aIPTW using propensity scoring was used for the adjustment. Variables used to calculate the propensity score included age, lactate, the SOFA score, steroid use, vasopressin use, and renal replacement therapy.
Discussion
Refractory shock is a major challenge in the management of septic shock. 4 Although several case-series studies of patients with refractory septic shock described its mortality, 10 –12 little evidence on its indicators exist. To the best of our knowledge, the present study is the first to show that an MD24 ≥0.6 μg/kg/min was significantly associated with early mortality in all patients with septic shock included in the study population.
Effect of the MD24 on Mortality
We found that the MD24 was significantly associated with 7-day but not with 30-day mortality in the multivariate analysis. After propensity scoring adjustment, it was associated with an increased risk of death at 7 and at 30 days, but we initially demonstrated that this association was more evident during the earlier phase. The cause of death in patients with sepsis is multifactorial, 4 and the time of death differs by cause. Death due to refractory shock occurs during the first 7 days of the syndrome. 4 Our findings suggest that, while the MD24 is associated with the severity of the shock, its effect on long-term mortality may be limited. Therefore, the subgroup of patients with refractory shock may have a favorable outcome if they somehow survived beyond shock phase. This may explain the reason for the difference in 28-day mortality between previous reports that analyzed patients with septic shock who received HDVs. 10 –12 Our findings also suggest that, in the management of refractory shock, focusing on the short-term outcome (ie, 7-day mortality) may be more valuable than focusing on the 28-day or longer-term outcome. In any sense, we should consider detailed hemodynamic monitoring and additional therapeutic approaches for those require higher norepinephrine especially in acute phase.
MD24 Cutoff in Refractory Septic Shock
We utilized a threshold of 0.6 μg/kg/min of norepinephrine based on the ROC curve analysis. This is consistent with a study by Conrad et al 14 that reported that 6 μg/kg/min of phenylephrine (an equivalent of 0.6 μg/kg/min of norepinephrine) predicted refractory shock. Based on this high specificity, this threshold may be a useful indicator for refractory septic shock. On the other hand, the sensitivity for early death in our study group was below 50%. Despite the low sensitivity, and given the low rate of early death in patients who received the lower MD24, it may be safe to increase the norepinephrine dosage to 0.6 μg/kg/min without considering early fatal consequences. The low sensitivity may partly be due to not prospectively evaluating the required dose of norepinephrine as an indicator of refractory shock or due to the nonprotocolized administration of vasopressin. Vasopressin administration is known to be associated with a reduction in norepinephrine requirement. 7 In this study, vasopressin administration may have resulted in a lower requirement for norepinephrine in patients with refractory shock and thereby may have increased the number of patients in the false-negative group (ie, those who die due to refractory shock with norepinephrine <0.6 μg/kg/min).
As the management of hemodynamic shock was not protocolized in this study, the MD24 cutoff of 0.6 μg/kg/min requires external validation in a future prospective study using detailed protocols of catecholamine administration.
Limitations
This study has several limitations, including the retrospective study design. Although the norepinephrine dosage was increased according to the severity of the septic shock, it was adjusted based on decision-making by clinicians and not based on protocols. Therefore, further protocol-based validation of our results is needed. In addition, due to the retrospective study design, we cannot exclude that the higher norepinephrine dosage itself worsened the 7-day outcome. Second, the effect of the focus of infection on survival was not evaluated due to the small sample size. Specifically, the incidence of pneumonia was higher in nonsurvivors. Thus, respiratory failure may worsen the severity of the shock and may be associated with a higher rate of early death. Finally, steroids and vasopressin were administered in the study population. The effect of these confounders should be minimized in a future prospective study evaluating if the norepinephrine dosage can be used as an early indicator of refractory septic shock.
Conclusions
Maximum dose of norepinephrine within 24 hours ≥0.6 μg/kg/min was significantly associated with 7-day mortality in patients with septic shock and may therefore be a useful indicator of refractory septic shock.
Footnotes
Authors’ Note
Daisuke Kasugai and Norimichi Uenishi conceived and designed this study. Daisuke Kasugai and Takao Ikeda contributed to the acquisition of the data. Kazuki Nishida, Kunihiko Takahashi, and Shigeyuki Matsui contributed to the data analysis. Akihiko Hirakawa, Masuyuki Ozaki, and Norimichi Uenishi assisted with the interpretation of the data. Daisuke Kasugai was responsible for drafting, editing, and submission of the manuscript. All authors reviewed and revised the manuscript as well as approved the final manuscript. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request. The institutional review board of Fujita health university approved this study. As this was a retrospective study, the need for patient consent was waived.
Acknowledgments
The authors would like to thank all nurses and physicians of the emergency ICU of the Fujita Health University Hospital for providing support during treatment. The authors also thank Misako Hashiguchi, an administrative assistant, for help with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.