
Abstract
Background/Objective:
Blood pressure optimization and maintenance of cerebral and spinal perfusion pressure are mainstays in the treatment of a neurocritically ill patient. Traditionally, central venous access has been required for vasopressor administration, with risk of inherent complications. The authors have previously reported pilot data on the safety of peripheral administration of phenylephrine in a neurocritical care unit. In this follow-up, we report the safety, feasibility, and potential efficacy of peripheral administration of low-concentration phenylephrine in a more robust cohort.
Methods:
A retrospective chart review was conducted on all consecutive patients who received peripheral phenylephrine in a tertiary care hospital neurocritical care unit.
Results:
A cohort of 125 patients were identified and included in the final analysis. The average age was 59.3 years, with an average intensive care unit (ICU) length of stay of 7.61 days. The most common indication for phenylephrine use was spinal perfusion (both with/without neurogenic shock) in 38.4% of cases, followed by postsurgical/anesthesia resuscitation in 16.8% of cases; 25.6% of patients in our cohort required escalation to central venous access (central venous catheter + peripherally inserted central catheter). A total of 2880 patient-hours were recorded with peripheral phenylephrine infusion, of which 73.9% were at goal blood pressure (either systolic or mean arterial pressure). Only one major complication of thrombophlebitis and 8 minor complications were recorded.
Conclusions:
Protocol-driven peripheral administration of lower concentration phenylephrine in an ICU setting is safe and feasible. This strategy is potentially effective at achieving hemodynamic targets in the majority of patients avoiding the need for central venous access.
Keywords
Introduction
Vasopressor administration and blood pressure (BP) support are central tenets of critical care delivered in intensive care units (ICUs) around the world. 1 In the neurocritical care unit (NCCU), the treatment of hypotension is of paramount importance to maintain cerebral perfusion pressure (CPP) and spinal perfusion pressure (SPP) to prevent secondary injury due to energy delivery failure. 2 Additionally, BP augmentation with normal hemodynamic function (without hypotension/shock) is routine in the NCCU to ensure cerebrospinal perfusion and neuroprotection. 2
Administration of vasopressor agents has traditionally necessitated placement of central venous access, either with a central venous catheter (CVC) or a peripherally inserted central catheter (PICC). This practice is driven by concerns of skin and tissue injury as a result of vasopressor extravasation or tissue ischemia due to vasospasm even without extravasation. 3 Placement of central venous access has inherent risks to the patient, largely due to inadvertent structural injury and complications during placement, as well as infectious and thrombotic complications with prolonged use. Recognized minor and major complications of CVC insertion or maintenance may occur in more than 15% of patients with a CVC. 4
Placement and maintenance of a peripheral intravenous catheter (PIV) is comparatively simpler, safer, and faster for medication delivery. Peripheral intravenous catheters have a lower risk of complications compared with CVCs. 5 Peripheral intravenous catheter–associated thrombotic complications are extremely rare and PIV-related bloodstream infections are 40 times less frequent than CVC. 6 However, PIV-delivered vasoactive medications can lead to tissue hypoperfusion injury, skin and tissue necrosis, and gangrene. 3,7
Approval from the institutional review board (IRB) and the pharmacy and therapeutics committee at the University of Utah was obtained for the use of low-concentration phenylephrine (40 μg/mL) through PIVs in the NCCU. Waiver of written informed consent was approved by the IRB. Phenylephrine (PE) was chosen due to its absence of cardiac (inotropic) effects and pure vasoconstrictor profile, which is ideal in an NCCU setting where augmentation of BP is routinely employed in the absence of shock. The reduced concentration of PE and limited infusion rate were chosen to minimize the risk of vascular and tissue injury in case of extravasation of vesicant solution. The initial experience and pilot data on 20 patients were published in 2016. 8
Methods
Study Design
An observational, retrospective cohort study was conducted in an NCCU at a tertiary care academic medical center between May 2014 and February 2016 among patients who received peripheral administration of PE. Peripheral PE was administered to patients who met criteria for hemodynamic support and BP augmentation (both with and without hypotension) as deemed necessary by the treating neurocritical care physician.
The primary objective of our study was to evaluate the safety and feasibility of PE administration through a PIV in the NCCU. Secondary objectives included identification of individual complications and assessment of potential efficacy and failure rates, which were not addressed in the initial pilot cohort.
A cohort of 125 consecutive patients were identified, who received peripheral PE in our NCCU during the specified time period (according to consecutive convenience sampling). A chart review was performed using the electronic medical record to identify demographic data, physiologic data, clinical indication for vasopressor use, PIV infusion characteristics, documented complications, complications management, and treatment escalation. Treatment escalation included use of additional vasopressors and placement of central venous access (CVC or PICC insertion). The hourly PE infusion rate and hemodynamic parameters were recorded (starting 1 hour before and extending to 3 hours after PE administration). From these data, total, peak, and average PE infusion and hemodynamic parameters were calculated.
Peripheral Intravenous Catheter Vasopressor Protocol
Administration of peripheral PE was implemented in the NCCU with a 2:1 patient to nurse ratio at a concentration of 40 μg/mL and an infusion limit of 2 μg/kg/min. Infusions were administered via an 18-G or larger PIV which was in the upper extremity, proximal to the wrist. The NCCU nurses administering peripheral PE had to review our institution’s extravasation policy at the start of each shift (Online Appendix A). Our institution has more than 5 years of experience in using PE vasopressor through a PIV route, and there is comfort and familiarity among pharmacy, nursing, and physician personnel (Online Appendix B—peripheral vasopressor policy).
Complications
Complications of peripheral infusion of a vasopressor were evaluated in detail and classified as minor or major based on currently published literature. 3,5,8 Complications were classified minor if they were local to PIV sites, without permanent sequela, did not impact medical care of the patient (require additional testing or escalation of care), and were addressed by routine ICU nursing care. Complications were classified as major if they had permanent sequela, impacted medical care of the patient (requiring additional tests or treatment), could not be addressed by routine ICU nursing measures, or necessitated discontinuation of peripheral vasopressor infusion. Both minor and major complications were addressed according to our institutional extravasation guideline (Online Appendix A). The predefined complications are listed in Table 1.
Classification of Complications.
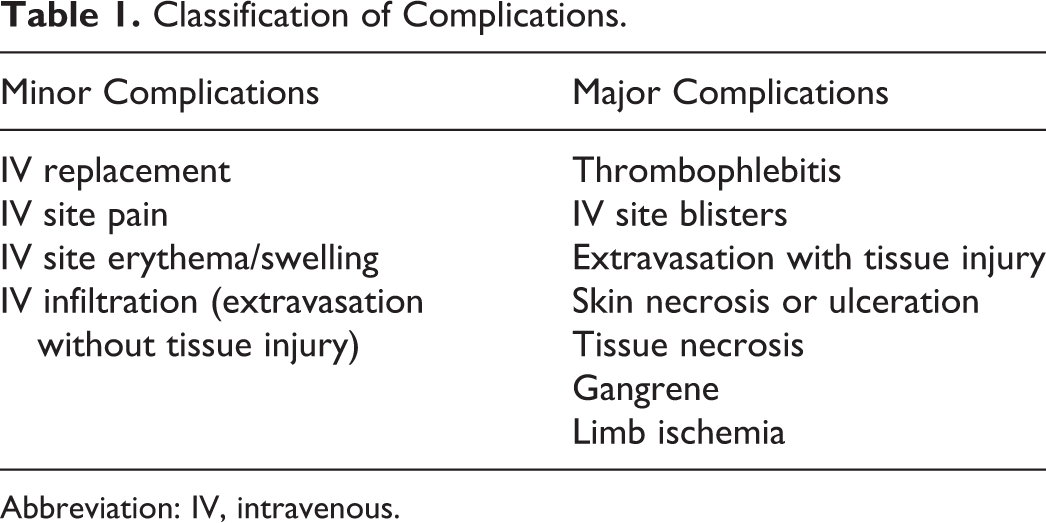
Abbreviation: IV, intravenous.
Statistical Analysis
Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the University of Utah. 9 REDCap is a secure, web-based application designed for deidentified data capture for research studies. REDCap data were exported to IBM SPSS Statistics software (version 24) and Microsoft Excel (release 2016) in a deidentified fashion, where the data were analyzed.
Results
A total of 125 cases of peripheral administration of PE were available within our time period and included in our retrospective cohort. The characteristics of our patient cohort are depicted in Table 2. Of note, our cohort had a predominantly homogenous racial distribution relevant to our geographic population demographic.
Characteristics of Study Population.
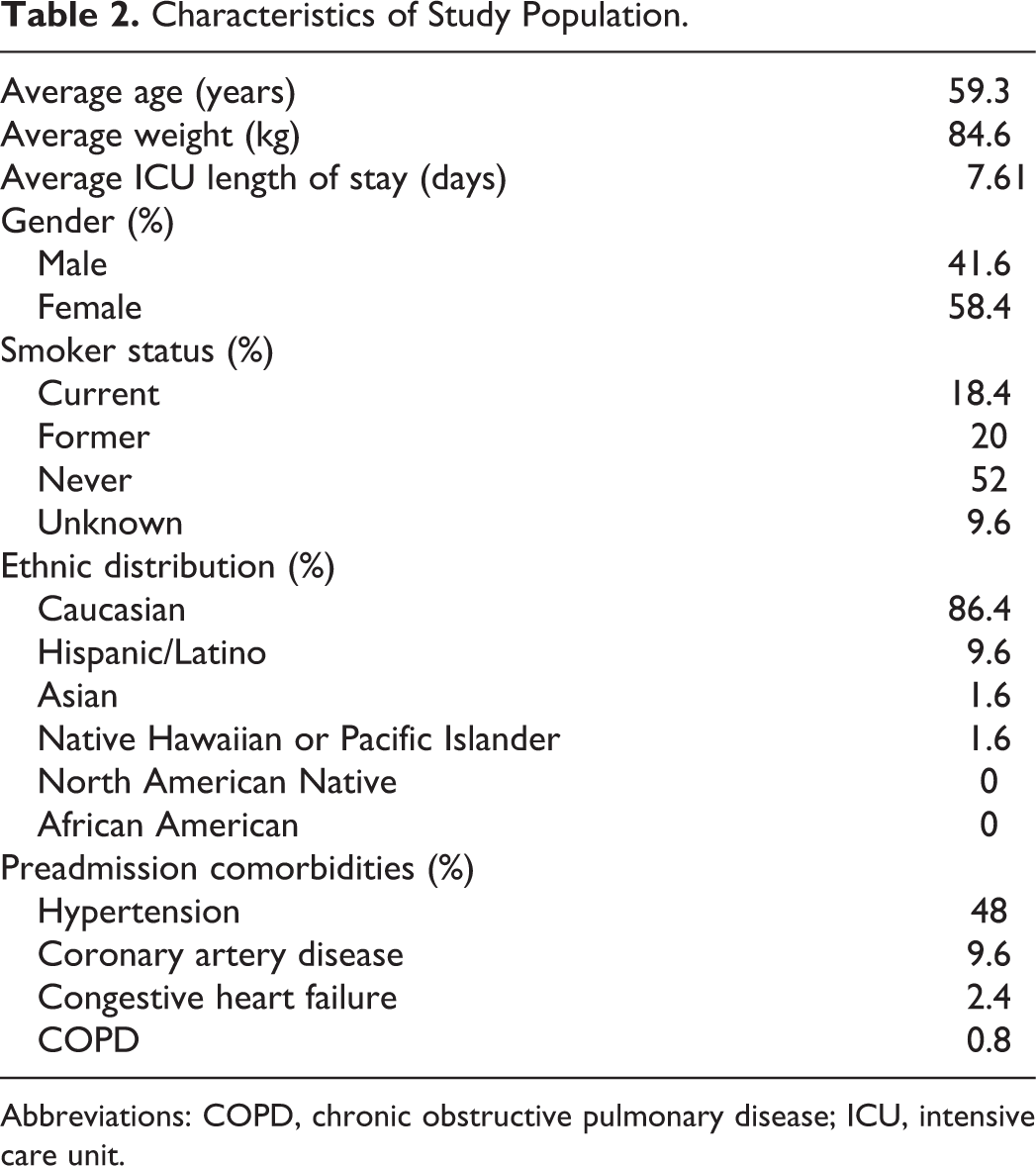
Abbreviations: COPD, chronic obstructive pulmonary disease; ICU, intensive care unit.
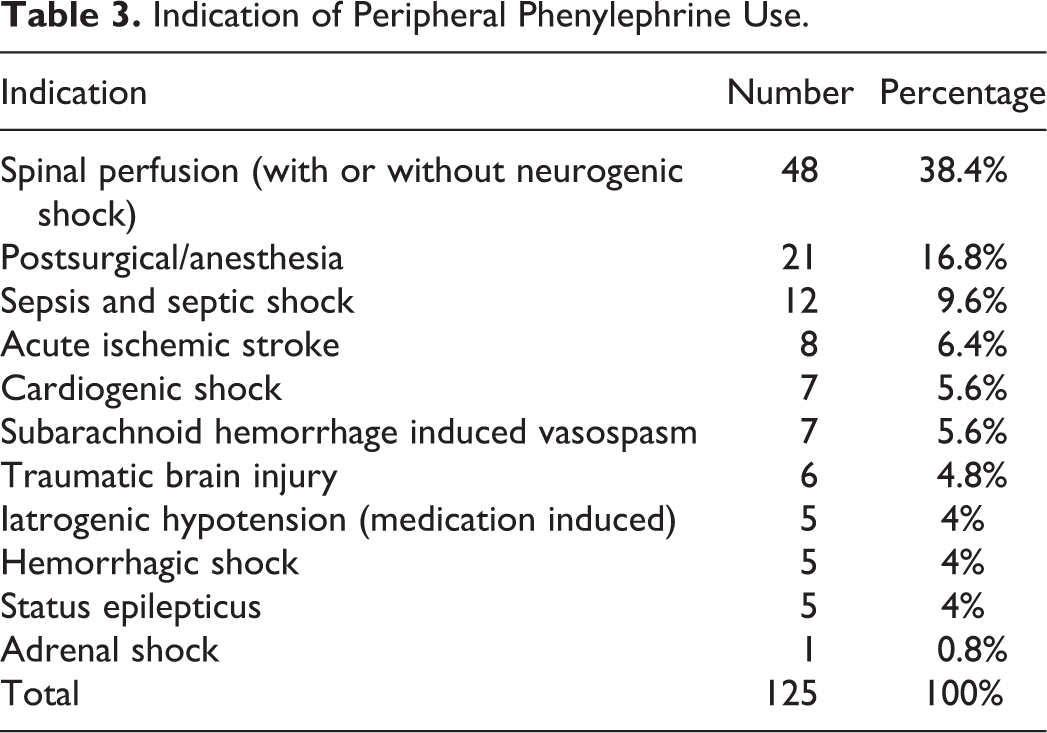
Indications for PE administration are depicted in Table 3. The most common indication was spinal perfusion (both with and without neurogenic shock) in 38.4% of cases, followed by postsurgical/anesthesia resuscitation in 16.8% of cases. Sepsis and septic shock were relatively less common in 9.6% of cases.
Indication of Peripheral Phenylephrine Use.
Target BP was defined as either a systolic blood pressure (SBP) or a mean arterial blood pressure (MAP). Data for target BP were available from chart review in 91.2% (114/125) of patients. No target BP data (SBP or MAP) were available in 8.8% (11/125) of patients. The target BP was expressed in SBP for 58.4% of patients (73/125) and in MAP for 32.8% of patients. Average SBP target was 122 mm Hg (range: 90-180, interquartile range [IQR] = 40), and average MAP target was 74 mm Hg (range: 60-100, IQR = 20).
The most common gauge of intravenous (IV) used for PE administration was 18 G, placed in the right antecubital position. The average duration of peripheral PE infusion was 22:37 hours (range: 2:40-91:58 hours); 83.2% (104/125 patients) of our cohort had an arterial line placed for accurate beat-to-beat BP measurements during PE infusion. All documented arterial lines were inserted prior to PE infusion (104 patients). Of the patients without arterial line placement (21/125), the average duration of infusion was 14 hours and 48 minutes (range: 2:23-47:23 hours, IQR of 14 hours and 27 minutes).
Prior to initiation of peripheral dose PE, the patients in our cohort had an average heart rate of 77.3 bpm (range: 38-128 bpm), an average SBP of 113 mm Hg (range: 49-172 mm Hg), and an average pH of 7.37 (range: 7.099-7.611). The average rate of PE administration was 0.64 μg/kg/min (range: 0.155-2.521 μg/kg/min, IQR = 0.5 μg/kg/min), with a peak infusion rate of 3.06 μg/kg/min. The average total dose of PE administered to a patient was 69 528.5 μg (range: 2325-325 725 μg, IQR = 86 825 μg].
Complications from peripheral PE infusion were recorded from thorough chart review of physician/nursing documentation and pharmacy adverse event reporting. In our cohort, 6.4% (8/125) of patients had a minor complication and 0.8% (1/125) had a major complication. Of the minor complications reported, 4.8% (6/125) had local skin erythema/swelling and 1.6% (2/125) had IV infiltration (extravasation without tissue injury). The only major complication reported was thrombophlebitis in 1 patient. This complication resolved rapidly with removal of the PIV, heat application, and elevation, and the patient had complete recovery without any permanent sequela. There were no reported IV site blisters, extravasation with tissue injury, skin necrosis, tissue necrosis, and gangrene or limb ischemia; 92.8% of patients in our cohort had no complications, and 99.2% had no major complications.
Of 125, 22 (17.6%) patients received a CVC during their peripheral PE infusion. The CVC was inserted a mean of 12 hours and 29 minutes after initiation of the peripheral PE. Peripherally inserted central catheters were placed in 8% (10/125) of patients. Therefore, 25.6% of patients in our cohort required escalation to central venous access (CVC + PICC), with indications depicted in Table 4. Of the different indications, 6.4% (8/125) required a second vasopressor in their medication regimen. From those 8 patients, 4 received norepinephrine as a second vasopressor, 2 patients received dopamine, and 2 patients received vasopressin or epinephrine.
Indication for Central Venous Access Insertion.
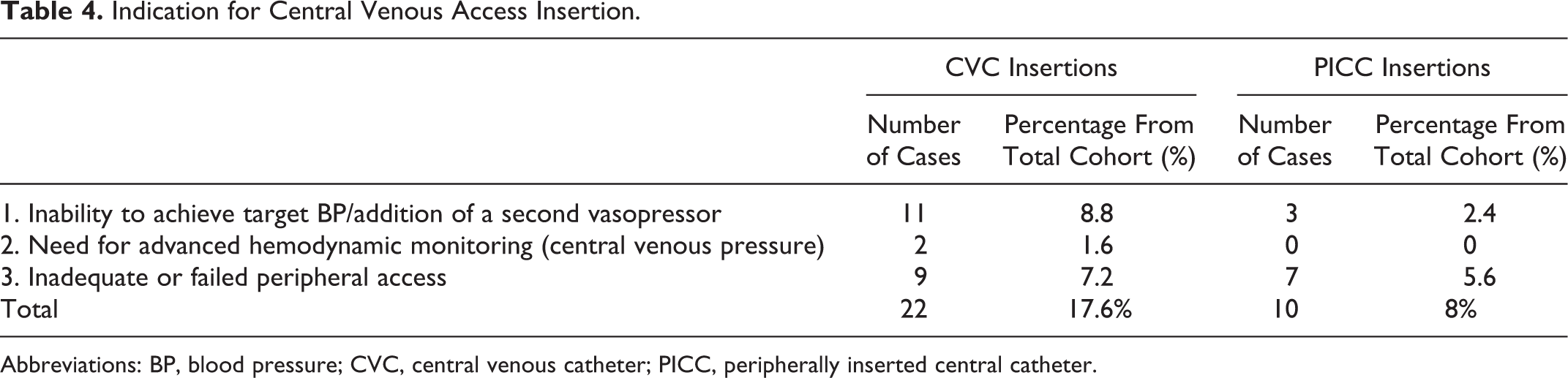
Abbreviations: BP, blood pressure; CVC, central venous catheter; PICC, peripherally inserted central catheter.
A total of 2880 patient-hours were recorded with peripheral PE infusion. During this peripheral infusion time, patients achieved target BP (SBP or MAP) 73.9% of the time. These data had to be subgrouped according to the type of BP target. There were a total of 1907 patient-hours with a target SBP, of which 1,324 hours were at target (69.4%). There were a total of 973 patient-hours with a target MAP, of which 807 hours were at target (82.9%; Table 5).
Patient-Hours Meeting Blood Pressure Targets.
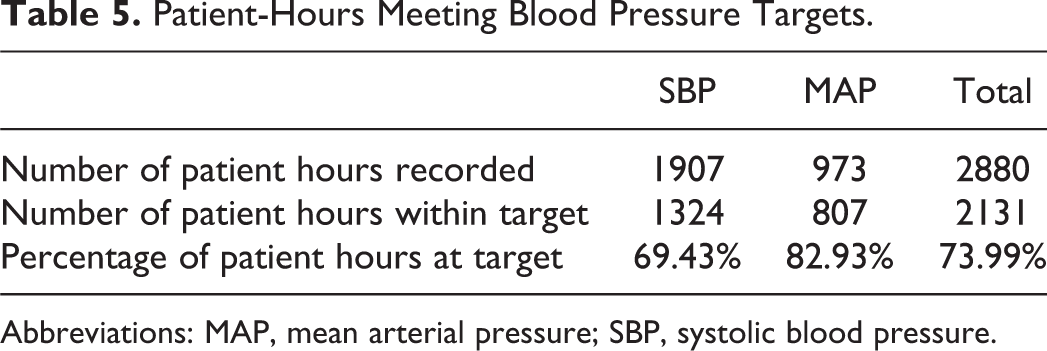
Abbreviations: MAP, mean arterial pressure; SBP, systolic blood pressure.
Discussion
Our study shows that protocol-driven peripheral administration of PE is safe and feasible with a low complication rate. In the majority of patients, this treatment successfully avoids need for central venous access, which has significant complications both at the time of insertion and with continued use. These complications include, but are not limited to, vascular injury, pneumothorax, hemothorax, air embolism, cardiac arrhythmias, hematoma formation, brachial plexus/neural injury, bloodstream infections, and cellulitis, and so on. Although complications associated with central venous access can be reduced (with ultrasound guidance, antimicrobial-impregnated catheters, avoidance of femoral site, CVC care bundles, avoidance of routine catheter changes, and early removal), the definitive route to avoid these complications is to avoid CVC/PICC insertion altogether. 4 This delivery method allows for faster administration and reduces time required to achieve hemodynamic stability and its concomitant clinical benefits. 3 Insertion of central venous access always incurs a delay compared to PIV insertion, and insertion during emergency circumstances may increase the risk of adverse events. 10 Use of vasoactive agents through a PIV has its own risk of complications, most important of which is extravasation and tissue/skin injury. 3,5,8 Infiltration is the inadvertent leakage of nonvesicant solution into perivascular soft tissue and extravasation is the leakage of a vesicant solution. 11 Phenylephrine, like all vasopressors, is a vesicant solution with vasoactive properties. 12 Due to the retrospective nature of our study, we considered documentation of “IV Infiltration without additional interventions required” to be synonymous with “IV extravasation without tissue injury.” This can be readily managed with routine ICU nursing measures after PE administration has been switched to another PIV. 11 Administration of vasopressor through a PIV can also predispose to fluctuations in dose delivery with manipulation of the PIV with arm movement. Our cohort used proximal PIVs (antecubital and upper arm) with close monitoring to prevent this problem.
There is one systematic review of complications from central and peripheral administration of vasopressors with a total of 318 patients by Loubani and Green, which showed that despite extravasation being the most common complication, further injury was not precipitated in 75% of cases. 3 In this study, tissue injury from extravasation was correlated with a distal location of PIV (distal to cubital fossa) and infusions exceeding 24 hours. 3 Although our cohort had infusion times exceeding 24 hours, we had proximal placement of PIVs and a very low extravasation and complication rate.
In the only randomized controlled trial that compared patients who received CVC versus PIV, there was a marginally higher rate of major complications with PIVs. 5 However, this difference disappeared if “difficulty to insert PIV” was excluded as a major complication. 5 Since this difficulty does not fulfill our criteria for a major complication, reclassification of this would remove any statistical difference between CVC and PIV. We predefined major and minor complications such that major complications were limited to those that impacted patient care, caused skin or tissue injury, affected outcomes, or necessitated discontinuation of peripheral PE infusion. Vasopressor extravasation without tissue injury is readily addressed with routine ICU nursing care as directed by our institutional extravasation policy and was classified as a minor complication. 11,13 We have previously reported pilot data from our institution, comprising 20 patients who received peripheral PE in an NCCU without any major complications. This cohort adds to the pilot data, is of robust size, and provides detailed information about escalation to central venous access. The indications for vasopressor use are reflective of a NCCU population where spinal/neurogenic shock and shock after anesthesia (under-resuscitation) are the most common etiologies. Phenylephrine is a pure peripherally acting vasopressor (without inotropic effect) and is therefore an ideal agent in this population. It is also important to note that in our cohort, PE was used for patients with normal hemodynamics to augment CPP or SPP, which is unique to the NCCU population. Septic and cardiogenic shock were relatively uncommon (9.6 and 5.6%, respectively) and the authors acknowledge that PE is not an ideal first-choice in this patient population. Low incidence of septic/cardiogenic shock is not typical of a medical or surgical ICU, so these data should be used with caution outside an NCCU (Table 3).
The minor complication rate in our cohort was 9.6% and these complications were easily addressed by ICU nursing. The medical team provided assistance with serial clinical monitoring and evaluation but did not need to intervene beyond that role. There was only one patient who developed a major complication (thrombophlebitis), which required intervention by the medical team (antibiotics and deep vein ultrasound imaging). None of the minor or the one major complication had any permanent sequela on the patients’ ICU course or hospital stay. We observed that the maximum infusion rate and duration specified in our peripheral vasopressor guideline (2 μg/kg/min and 48 hours, respectively) was exceeded with the approval of the neurocritical care physician (Online Appendix B). The highest peak rate of infusion (3.06 μg/kg/min) and longest duration (91:58 hours) in our cohort were not associated with any complication (minor or major), which adds to the robustness of our data.
In the vast majority of our patients who received peripheral PE, central venous access was avoided but was required in 25.6% (32/125). The most common indications for escalation to central venous access were inability to achieve target BP goals, need for central venous pressure monitoring, or inadequate/failed PIV access (Table 4). There were 14 patients who required central venous access due to inability to achieve BP targets. Of these 14 patients, 8 required the addition of a second vasopressor agent and 6 patients were switched to central venous dosing of PE alone. Achieving hemodynamic targets is of paramount importance in patients with shock (of any cause) and in patients requiring hemodynamic augmentation for cerebral/spinal perfusion. Patients who required escalation of treatment were easy to identify and received central venous access without delay, to avoid prolonged hypotension or failure to meet cerebrospinal perfusion targets. Mean timing of central venous access was at 12 hours and 29 minutes with ongoing infusion of PE. This allowed placement of central venous access in a nonemergent, relatively controlled and carefully planned fashion, with its concomitant benefits. 3
The overwhelming majority of our cohort (74.4%) avoided the complications and risks associated with central venous access. Our cohort achieved target hemodynamic goals in 73.99% of patient-hours, which correlates well with need for escalation to central venous access. This indicates that peripheral administration of PE was safe and effective in the majority of our cohort. It is safe to assume that our patients achieved their hemodynamic target and its concomitant medical benefit sooner than patients who had a delay in vasopressor administration awaiting central venous access. 3
It is important to acknowledge that our patient cohort was typical for an NCCU population and had less cardiopulmonary failure than would be found in a medical or surgical ICU. This is reflected by the low rate of septic shock (9.6%), and near-normal average SBP, heart rate, and pH prior to administration of peripheral PE. Degree of shock was likely to be mild to moderate only and severe shock would have led the treating physician to place central venous access at commencement. Normal cardiopulmonary physiology in the majority of our patients facilitated our choice of vasopressor (PE) and enabled low doses of vasopressor administration, while adequately achieving hemodynamic targets in the majority. In comparison, the randomized controlled trial by Ricard tested CVC versus PIV in a population with much higher rates of critical illness and predicted mortality and respiratory failure. 5 Our results are encouraging but should be applied only with judicious care in patients outside an NCCU. In these patients, it may be safe and feasible to use peripheral PE temporarily, enabling nonemergent placement of central venous access. Such a strategy would have a good safety profile due to short duration of use and provide earlier vasopressor benefit to this patient population with its inherent benefits.
Our study results are similar to data published by Datar et al in 2018. 14 The authors published their experience with peripheral PE administration in an NCCU, with similar indications and treatment strategy (though they used a higher concentration of PE, 120 μg/mL). Although they reported a larger cohort of 277 patients, our study has the advantage of predefined complications, data on PICC placement, and time-at-target data. The results between the 2 studies are comparable with low central venous access and complication rates, which lends credibility to our data.
Our study is limited by the retrospective nature of data collection, which is inherent in all retrospective reviews. This exposes our study to reporting bias, selection bias, information bias, documentation errors, and inaccuracies in chart-driven data collection. Since this a retrospective cohort, patient selection was consecutive and not randomized. It is reasonable to acknowledge that certain patients received central venous access from the beginning, without any attempt at peripheral administration, at the discretion of the NCCU physician. The strength of this study lies in its robust sample size, consecutive patient selection, protocol-driven administration of PE, predefined complications, and measures of outcome which were not assessed in the pilot study. 8 Combined with the cohort by Datar, there are now 402 patients in the modern literature indicating that peripheral administration of PE is safe and feasible in an NCCU.
Conclusion
Our study shows that protocol-driven peripheral administration of low-concentration PE, with appropriate patient selection, in an NCCU setting, is safe and feasible. We also demonstrate that this strategy is effective at achieving hemodynamic targets in the majority and enables safer (nonemergent) central venous access placement in the remainder. This enables quicker administration of vasopressor while preventing delays associated with and drastically reducing the need for central venous access. The authors intend to follow this retrospective cohort with a prospective study testing multiple vasopressors administered through peripheral access in an NCCU setting.
Supplemental Material
Supplemental Material, Appendices - Safety and Feasibility of Phenylephrine Administration Through a Peripheral Intravenous Catheter in a Neurocritical Care Unit
Supplemental Material, Appendices for Safety and Feasibility of Phenylephrine Administration Through a Peripheral Intravenous Catheter in a Neurocritical Care Unit by Paul Ballieu, Yasaman Besharatian and Safdar Ansari in Journal of Intensive Care Medicine
Footnotes
Acknowledgments
The authors wish to acknowledge Dr Robert Hoesch who initiated the peripheral vasopressor policy at the University of Utah Healthcare. The authors also thank all key personnel in the NCCU who were involved in the delivery of peripheral dosed PE. This included but is not limited to nursing, resident, and pharmacy personnel.
Author Contributions
Both Paul Ballieu and Yasaman Besharatian are first authors as they have both contributed equally to all sections of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.