
Abstract
Objective:
There is paucity of data about prevalence of pediatric acute respiratory distress syndrome (PARDS) in children with pulmonary contusion (PC). We intend to evaluate PC in children with chest trauma and the association between PC and PARDS.
Design:
Retrospective review of Institutional Trauma Registry for patients with trauma.
Setting:
Level 1 trauma center.
Patients:
Age 18 years and younger with a diagnosis of PC.
Interventions:
None.
Measurements and Main Results:
Of the 1916 children with trauma, 50 (2.6%) had PC. Patients with PC and PARDS had lower Glasgow Coma Scale (GCS) score (7 [3-15] vs 15 [15-15], P = .0003), higher Injury Severity Scale (ISS) score (29 [22-34] vs 19 [14-22], P = .004), lower oxygen saturations (96 [93-99] days vs 99 [98-100] days, P = .0009), higher FiO2 (1 [1-1] vs 0.21 [0.21-0.40], P < .0001), lower oxygen saturation/FiO2 (S/F) ratios (97 [90-99] vs 457 [280-471], P < .0001), need for invasive mechanical ventilation (IMV; 86% vs 23%, P < .0001), and mortality (28% vs 0%, P = .006) compared to those without PARDS. Forty-two percent (21/50) of patients needed IMV, of these 61% (13/21) had PARDS. Patients who needed IMV had significantly lower GCS score (8 [3-11] vs 15 [15-15], P < .0001), higher ISS score (27 [22-34] vs 18 [14-22], P = .002), longer length of stay (LOS; 7.5 [4-14] days vs 3.3 [2-5] days, P = .003), longer hospital LOS (18 [7.0-25] vs 5 [4-11], P = .008), higher PARDS rate (62% vs 7%, P < .0001), and lower S/F ratios (99 [94-190] vs 461 [353-471], P < .0001) compared to those who did not require IMV. Lower GCS score was independently associated with both PARDS and need for IMV.
Conclusions:
Pediatric ARDS in children with PC is independently associated with lower GCS score, and its presence significantly increased morbidity and mortality. Further larger studies are needed to explore association of lower GCS and higher injury score in children with PARDS and PC.
Introduction
Thoracic injuries occur in 4% to 6% of children hospitalized for trauma but are responsible for up to 25% of pediatric trauma deaths. 1 Almost a third of patients with chest trauma are found to have pulmonary contusions (PCs). 2 The compliant chest wall in children makes PC a common consequence of chest trauma even in the absence of rib fractures. Pulmonary contusions are serious injuries frequently resulting in respiratory failure requiring endotracheal intubation and mechanical ventilation (MV). Acute respiratory distress syndrome (ARDS) is reported in 1% to 8% of patients with trauma and 20% to 25% of patients with PCs. 3 –8 Reported risk factors for development of ARDS in trauma patients include age, lower Glasgow Coma Scale (GCS) score, higher Injury Severity Scale (ISS) score, the presence of PC, and/or rib fractures. 9 –15 The presence of PC is independently associated with ARDS in some studies, 9,14,15 though specific risks are still poorly understood. Although few studies have described ARDS in children with trauma, 6 pediatric acute respiratory distress syndrome (PARDS) in children with chest trauma and PC has not been well described. In this study, we examined the incidence of PARDS and need for MV in pediatric trauma patients with PC and explored risk factors for these outcomes.
Study Methods
We conducted an institutional review board approved retrospective, single-center cohort study on trauma admissions to an urban level 1 trauma center. Data on pediatric trauma admissions between 2010 and 2015 with a diagnosis of PC aged 18 years and younger were obtained from our institution’s trauma registry.
Inclusion Criteria
Infants and children with chest trauma sustaining PC secondary to blunt or penetrating trauma with an Abbreviated Injury Scale (AIS) score of 2 16 or greater in any body region were included. Pulmonary contusion was identified in the trauma registry using International Statistical Classification of Diseases, Ninth Revision code.
Exclusion Criteria
We excluded patients who were transferred to another hospital or home directly from the emergency department and those who were dead on arrival.
Measurement of Clinical Variables
The trauma registry provided admission systolic blood pressure (SBP) and diastolic blood pressure (DBP), admission GCS, mechanism of injury, ISS, chest AIS, head AIS, abdomen AIS, hospital length of stay (HLOS), pediatric intensive care unit (PICU) LOS, and in-hospital complications (cardiac arrest, pneumonia, pleural effusion, deep vein thrombosis [DVT], infection, urinary tract infection [UTI], rash, acute blood loss, brain death) and mortality, and demographic information, such as, age, gender, and race/ethnicity. The following information was obtained from the patient’s chart: the presence of rib fractures and/or pneumothoraces, need for transfused blood products, oxygen saturations (SaO2), supplemental oxygen requirement (FiO2), need and duration of MV, positive end-expiratory pressure (PEEP), mean airway pressure (MAP), and peak inspiratory pressure. Pediatric acute respiratory distress syndrome was defined according to the Pediatric Acute Ling Injury Consensus Committee (PALICC) criteria: findings of new infiltrate(s) consistent with acute pulmonary parenchymal disease and PaO2/FiO2 (P/F) ratio <300 or oxygen saturation/FiO2 ratio (S/F) ≤265. 17 We did not use oxygenation index to define PARDS due to nonavailability of MAP data.
Statistical Analysis
Variables were expressed as median with interquartile range or as frequencies and percentages. Tests of bivariate associations were performed using Wilcoxon rank-sum tests for continuous variables and Pearson χ 2 tests or Fisher exact tests for categorical variables. Univariate analysis consisted of 3 sets of comparisons of patient characteristics among patients with PC: PARDS versus no PARDS; patients who required MV versus no MV; and within the subgroup requiring MV—those with PARDS versus no PARDS. In order to identify independent risk factors for the outcomes PARDS and need for MV, multivariable logistic regression analyses were conducted. In the first model of each outcome, all potential risk factors with less than 10% missing data and categories large enough to estimate odds ratios (ORs; age, gender, race/ethnicity, SBP, DBP, rib fracture, GCS, ISS, and mechanism of injury) were included. A second model of each outcome retained only variables with P < .05 after a backward stepwise selection procedure. In all analyses, a 2-tailed P value of less than .05 was considered statistically significant.
Results
In all, 1916 children with trauma were identified, of which 50 (2.6%) patients met the inclusion criteria and were included in the study. Table 1 displays the demographic and clinical profile of the entire cohort. The median age of the cohort was 10.7 (6.8, 14.4) years, with males comprising 58% of the cohort. African American and Hispanic patients comprised 70% of the patients. Median HLOS was 8.5 (4-18) days. Blunt trauma was main type of injury (94%), while the most common mechanism of injury was being a pedestrian struck by a motor vehicle. Median scores for GCS, AIS chest, and ISS were 15 (8-15), 3 (3-3), and 21.5 (17-29), respectively. The reported complications were pneumonia in 4 patients, cardiac arrest in 2, pleural effusion in 1, DVT in 1, sepsis in 1, UTI in 1, hypoxia 1, rash 1, acute blood loss requiring massive transfusion in 2, and brain death in 2. Overall mortality in the entire cohort was 8%.
Characteristics of Patients With Pulmonary Contusion.
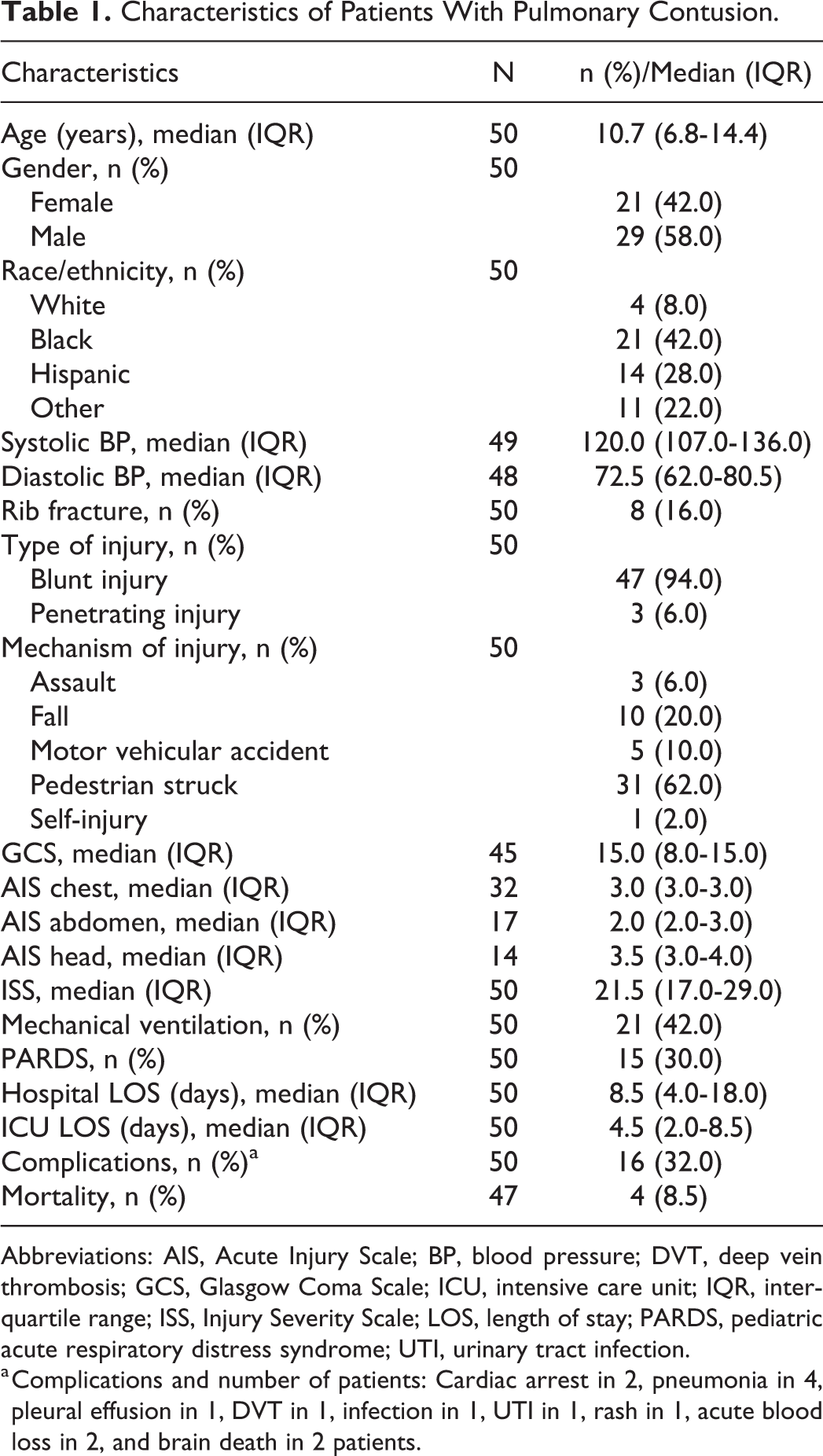
Abbreviations: AIS, Acute Injury Scale; BP, blood pressure; DVT, deep vein thrombosis; GCS, Glasgow Coma Scale; ICU, intensive care unit; IQR, interquartile range; ISS, Injury Severity Scale; LOS, length of stay; PARDS, pediatric acute respiratory distress syndrome; UTI, urinary tract infection.
a Complications and number of patients: Cardiac arrest in 2, pneumonia in 4, pleural effusion in 1, DVT in 1, infection in 1, UTI in 1, rash in 1, acute blood loss in 2, and brain death in 2 patients.
Pediatric Acute Respiratory Distress Syndrome and PC
Fifteen (15/50, 30%) patients had PARDS according to PALICC criteria, of whom 11 (22%) had ARDS per Berlin criteria (Table 2). Nine (9/15, 60%) had severe PARDS, 4 (26%) had moderate PARDS, and 2 (14%) had mild PARDS. The presence of PARDS was significantly associated with lower GCS score (7 [3-15] vs 15 [15-15], P = .0003), higher ISS score (29 [22-34] vs 19 [14-22], P = .004), lower oxygen saturations (96% [90-99] vs 99% [98-100], P = .0009), higher FiO2 (1 [1-1] vs 0.21 [0.21-0.35], P < .0001), lower S/F ratio (97 [90-99] vs 457 [280-471], P < .0001), and need for invasive MV (13/15 [87%] vs 8/35 [23%], P < .0001). All patients with mortality had PARDS (29% vs 0%, P = .006).
Characteristics of Patients With and Without PARDS.
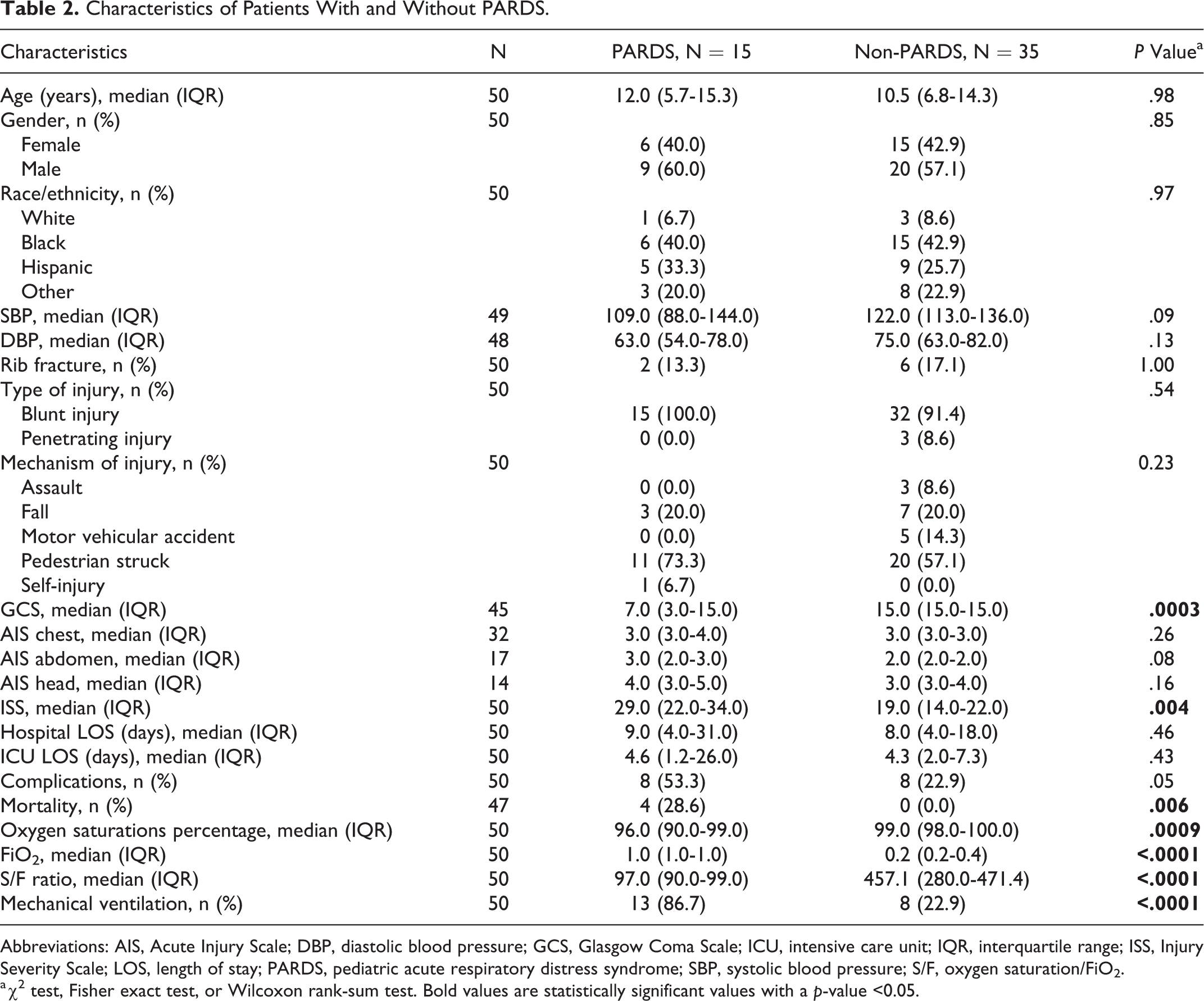
Abbreviations: AIS, Acute Injury Scale; DBP, diastolic blood pressure; GCS, Glasgow Coma Scale; ICU, intensive care unit; IQR, interquartile range; ISS, Injury Severity Scale; LOS, length of stay; PARDS, pediatric acute respiratory distress syndrome; SBP, systolic blood pressure; S/F, oxygen saturation/FiO2.
a χ2 test, Fisher exact test, or Wilcoxon rank-sum test. Bold values are statistically significant values with a p-value <0.05.
Pulmonary Contusion and Mechanical Ventilation
Twenty-one (21/50, 42%) patients with PC required invasive MV, with the median duration of ventilatory support being 3 (2-6) days (Table 3). Sixty-two percent (13/21) of patients who needed ventilatory support had PARDS. The median P/F ratio among MV patients was 264 (93-431). Patients with PC who needed invasive ventilatory support had significantly longer ICU LOS (7.5 [4-14] days vs 3.3 [2-5] days, P = .003), longer HLOS (18 [7-25] days vs 5 [4-11] days, P = .008), lower GCS score (8 [3-11] vs 15 [15-15], P < .0001), higher ISS score (27 [22-34] vs 18 [14-22], P = .002), presence of PARDS (62% vs 7%, P < .0001), lower oxygen saturations (97% [94-99] vs 99% [98-100], P = .009), higher FiO2 requirement (1.0 [0.5-1] vs 0.21 [0.21-0.28], P < .0001), lower S/F ratios (99 [94-190] vs 462 [354-471], P < .0001), and lower DBP (62.0 [58.5-77.5] vs 76.0 [66.0-83.0], P = .03) compared to those who did not require ventilatory support. All patients with mortality were in the MV group (21% vs 0%, P = .02).
Characteristics of Patients With and Without Mechanical Ventilation.
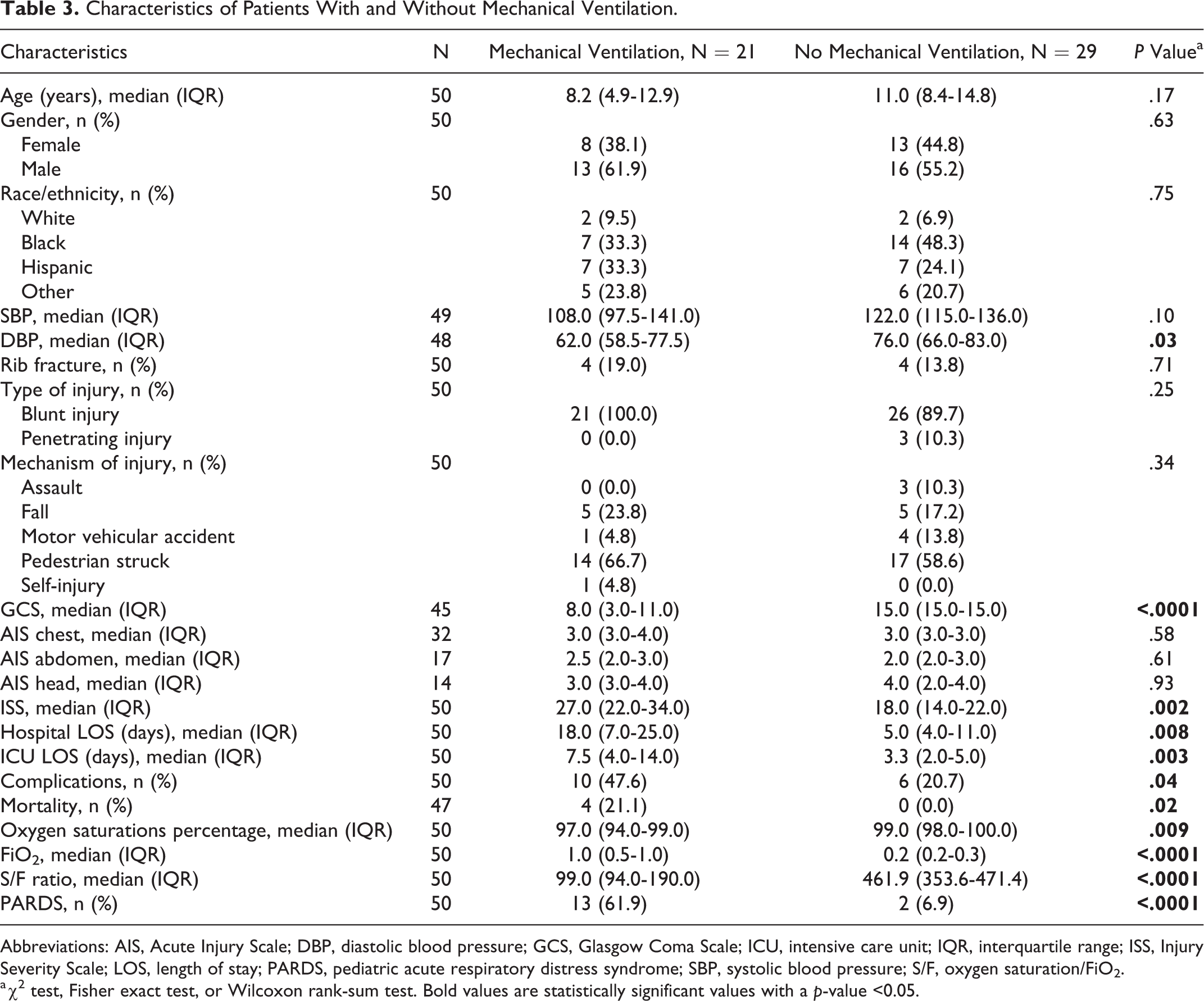
Abbreviations: AIS, Acute Injury Scale; DBP, diastolic blood pressure; GCS, Glasgow Coma Scale; ICU, intensive care unit; IQR, interquartile range; ISS, Injury Severity Scale; LOS, length of stay; PARDS, pediatric acute respiratory distress syndrome; SBP, systolic blood pressure; S/F, oxygen saturation/FiO2.
a χ2 test, Fisher exact test, or Wilcoxon rank-sum test. Bold values are statistically significant values with a p-value <0.05.
Further analyses of patients requiring MV support showed 62% to have PARDS (Table 4). Mechanical ventilation patients with PARDS were acidotic with lower pH (7.24 [7.19-7.31] vs 7.36 [7.30-7.37], P = .01) and had higher PaCO2 levels (47 [40-58] vs 38 [33-45], P = .06), lower PaO2 levels (93 [72-133] vs 245 [202-427], P = .009), higher PEEP (6 [5-8] vs 5 [5-55], P = .06), and lower P/F ratio (120 [72-196] vs 442 [411-465], P = .0003) compared to those without PARDS. All 4 patients with mortality were in the PARDS and MV group. Of the patients who died, 1 had associated severe traumatic brain injury (TBI; such as subarachnoid hemorrhage (SAH), subdural hemorrhage, and cerebral contusion), cervical spine injury, vertebral fracture, tension pneumothorax, and lung contusion and subsequently progressed to brain death. Second patient had intracranial fracture, splenic injury, pelvic fracture, rib fracture, and traumatic hemothorax who progressed to brain death. Third patient had open wound of shoulder, PC, and traumatic pneumothorax; had a cardiac arrest; and could not be revived. The fourth patient who died had severe TBI (cerebral contusion, SAH), flail chest, and splenic laceration extending into parenchyma.
Characteristics of Mechanically Ventilated Patients With and Without PARDS.
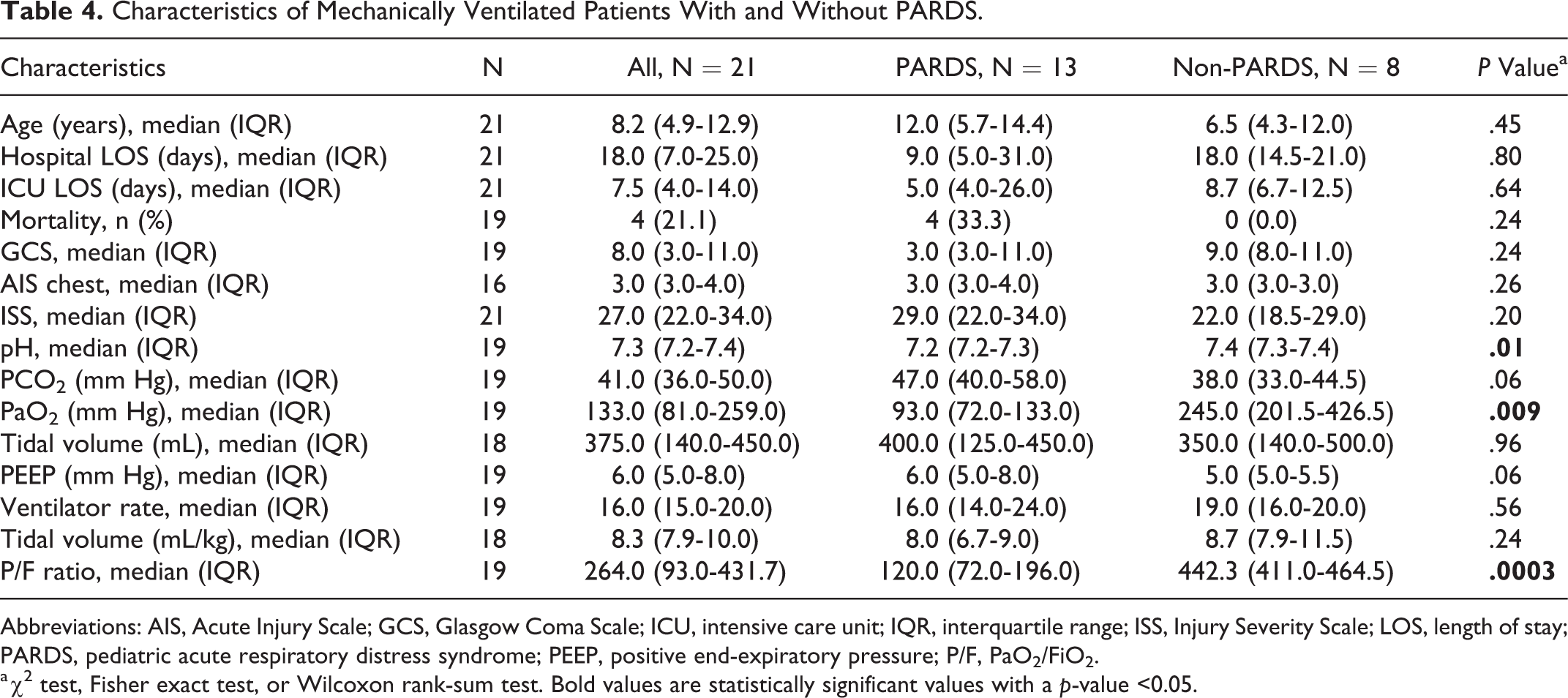
Abbreviations: AIS, Acute Injury Scale; GCS, Glasgow Coma Scale; ICU, intensive care unit; IQR, interquartile range; ISS, Injury Severity Scale; LOS, length of stay; PARDS, pediatric acute respiratory distress syndrome; PEEP, positive end-expiratory pressure; P/F, PaO2/FiO2.
a χ2 test, Fisher exact test, or Wilcoxon rank-sum test. Bold values are statistically significant values with a p-value <0.05.
Multivariable Analyses of Risk Factors for PARDS and MV
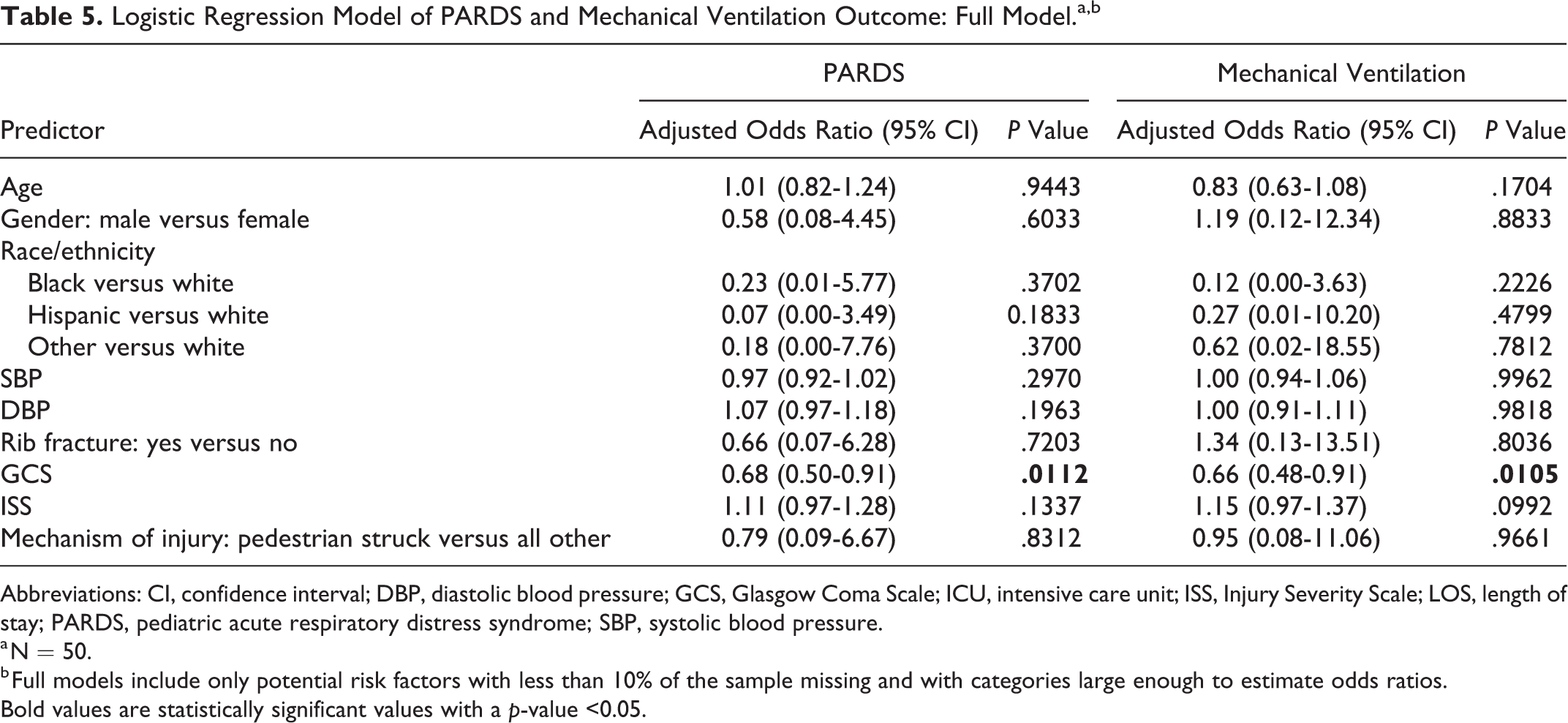
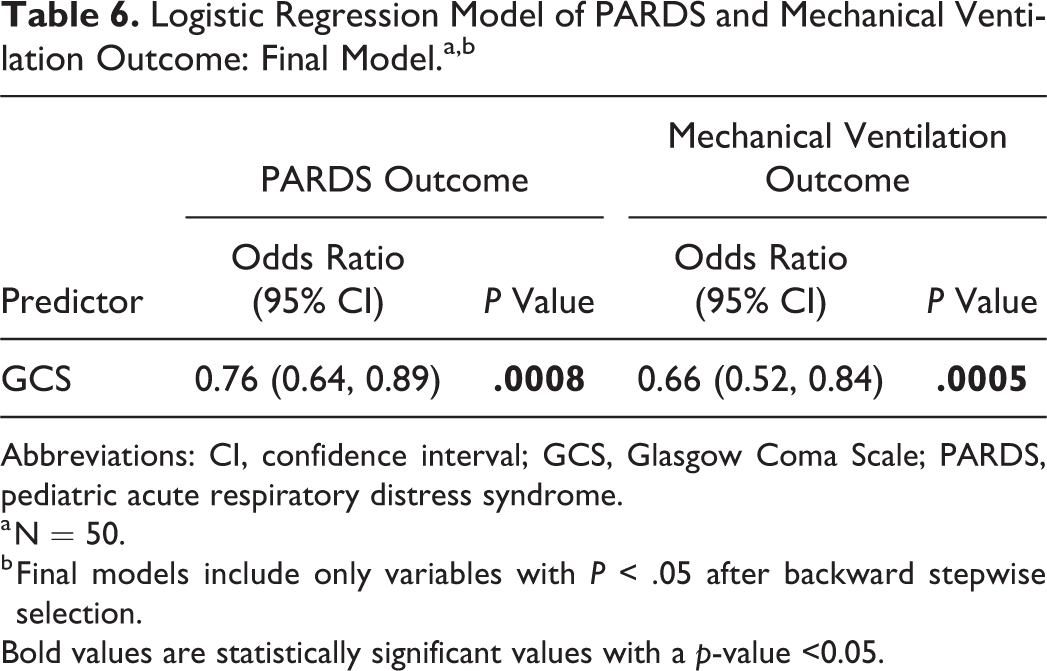
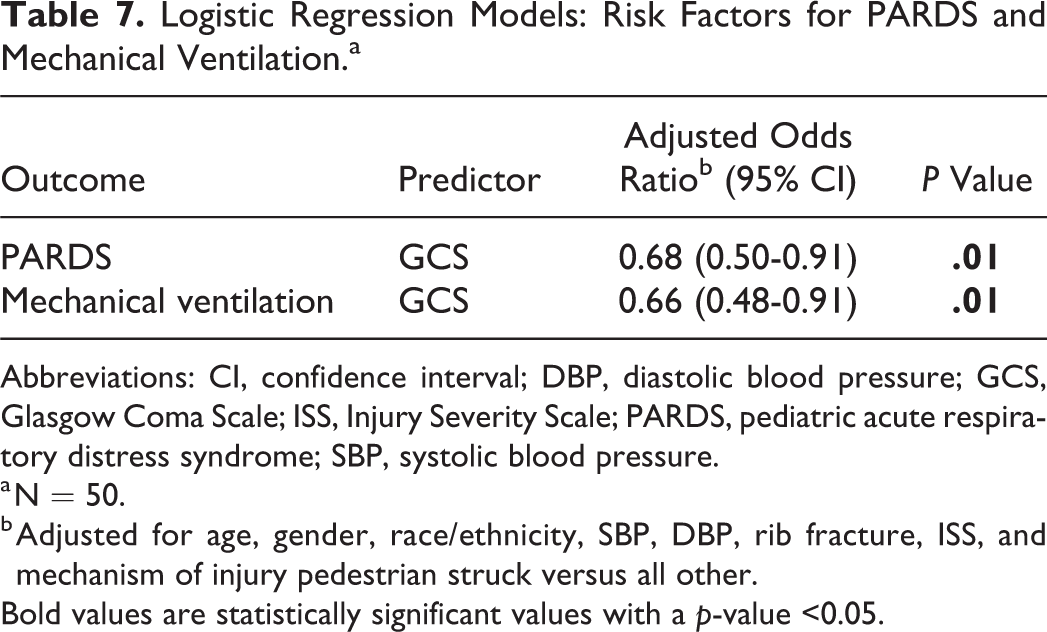
An initial multivariable logistic regression model including age, gender, race/ethnicity, SBP, DBP, rib fracture, GCS, ISS, and mechanism of injury identified lower GCS score on admission (adjusted odds ratio [AOR]: 0.68; 95% confidence interval [CI], 0.50-0.91; P = .01) as the only independent risk factor associated with the development of PARDS (Table 5). After a backward stepwise model selection procedure was applied, only GCS was retained in the model (OR: 0.76; 95% CI, 0.64-0.89; P = .0008; Table 6). Similarly, multivariable analysis found only lower GCS score to be independently associated with MV in both the full model (AOR: 0.66; 95% CI, 0.48-0.91; P = .01) and final model (OR: 0.66; 95% CI, 0.52-0.84; P = .0005; Table 7).
Logistic Regression Model of PARDS and Mechanical Ventilation Outcome: Full Model.a,b
Abbreviations: CI, confidence interval; DBP, diastolic blood pressure; GCS, Glasgow Coma Scale; ICU, intensive care unit; ISS, Injury Severity Scale; LOS, length of stay; PARDS, pediatric acute respiratory distress syndrome; SBP, systolic blood pressure.
a N = 50.
b Full models include only potential risk factors with less than 10% of the sample missing and with categories large enough to estimate odds ratios.
Bold values are statistically significant values with a p-value <0.05.
Logistic Regression Model of PARDS and Mechanical Ventilation Outcome: Final Model.a,b
Abbreviations: CI, confidence interval; GCS, Glasgow Coma Scale; PARDS, pediatric acute respiratory distress syndrome.
a N = 50.
b Final models include only variables with P < .05 after backward stepwise selection.
Bold values are statistically significant values with a p-value <0.05.
Logistic Regression Models: Risk Factors for PARDS and Mechanical Ventilation.a
Abbreviations: CI, confidence interval; DBP, diastolic blood pressure; GCS, Glasgow Coma Scale; ISS, Injury Severity Scale; PARDS, pediatric acute respiratory distress syndrome; SBP, systolic blood pressure.
a N = 50.
b Adjusted for age, gender, race/ethnicity, SBP, DBP, rib fracture, ISS, and mechanism of injury pedestrian struck versus all other.
Bold values are statistically significant values with a p-value <0.05.
Discussion
In this study of children with PC, we found PARDS to be present in 30% of patients and that the presence of PARDS is found to be significantly associated with lower GCS score, higher ISS score, lower oxygen saturations, lower S/F ratio, and need for MV. We also found need for MV in children with PC to be associated with the presence of PARDS, longer HLOS and PICU LOS, lower GCS score, higher ISS score, lower oxygen saturations, and lower S/F ratio. Lower GCS score was independently associated with both PARDS and need for MV after adjusting for age, gender, race/ethnicity, SBP, DBP, rib fracture, ISS, and mechanism of injury.
Pediatric ARDS is reported to present in around 3.2% of children in PICU and has an estimated mortality of about 17%, whereas it is reported in 1% to 8% of patients with trauma. 18 Berlin definition of ARDS is known to underestimate PARDS and was found to identify only 32% of children with PARDS. 18 In our study, using PALICC criteria, an additional 36% of patient met criteria for PARDS similar to reports by others. In our study, we had an incidence of 30% for PARDS for patients with PC. Incidence for ARDS in adult trauma patients is about 1% to 8%, while 1.8% to 3% incidence in pediatric patients. 6, 19 Killien et al 19 reported significantly higher incidence of ARDS in children less than 4 years and ARDS mortality of 25% in this age group. We did not find an association of PARDS in our study with age, though our mortality rate was similar (4/15, 29%). Also, mortality in patients with PARDS was significantly higher compared to those without PARDS, similar to findings reported by others.6,8,9
Children with trauma may develop ARDS from a variety of causes, such as lung contusions, pneumonia, sepsis, shock, and blood transfusion/transfusion–associated lung injury. Our rate of 30% PARDS in our patients is likely higher than that reported by others since our study sample size is relatively small—only including children with PCs and not all trauma patients. Acute respiratory distress syndrome in patients with PC has been previously reported in multiple studies. Miller et al 15 found PC size more than 20% (quantified using chest computed tomography scan) to be significantly associated with ARDS and pneumonia. A study by Wu et al 20 found PC to be a significant factor in predicting early and not late mortality in patients with post-traumatic ARDS along with acute physiology and chronic health evaluation (APACHE) II score. We found mortality to be associated with PARDS and need for MV. In a recent study to look for risk factors of ARDS in patients with trauma, Tignanelli et al 3 found direct thoracic injury to be the strongest risk factor for ARDS. They further reported higher ISS score, lower GCS score, and rib fractures 6 or more to be associated with ARDS in patients with trauma induced lung contusion. Higher ISS and lower GCS scores as independent predictors of mortality have also been reported by others. 5 These results are similar to our findings of association of lower GCS score and higher ISS score with PARDS and need for MV. Poor GCS score may be secondary to intoxication, shock, or TBI. Altered mental status may put patients at risk of aspiration and leading to ARDS or PARDS may develop in patients with TBI as part of multiorgan dysfunction. In a study by Huang et al, 21 patient with greater degree of shock, worse neurological status, and more severe injury were more likely to develop moderate-to-severe ARDS and patients with ARDS without chest trauma had a 10-fold higher risk of mortality. In contrast, another study 22 showed the presence of ARDS in patients with TBI did not change the mortality, though it increased HLOS and ICU LOS and complication rate. So, the association of poor GCS/TBI with ARDS remains unclear and needs to be explored further.
The association of higher injury scores and the development of ARDS have been described in multiple studies. 3,5,8,9,14,21,23,24 Afshar et al 23 showed an ISS score of 16 or above had a sensitivity and specificity of 85% and 76%, respectively, in predicting ARDS and was superior predictor of ARDS development than thoracic injury score or GCS score. The ISS score suggests the overall degree of injury, which is more important in the patient’s prognosis than the mere development of ARDS. Hence, though patients with chest trauma or PC are more likely to develop PARDS, the effect of PARDS on morbidity and mortality is largely related to the degree of injury in other organ systems as suggested by ISS and the presence of multi-organ dysfunction syndrome. 24
Studies in adults 12,13,25 have found rib fracture to be one of the risk factors for PC and the development of ARDS. In our study, only 16% of children with PC had rib fractures and we did not find them to be associated with PARDS or need for MV. Bony thorax in children probably confers much less protection to underlying lungs since ribs of a child are more compliant than adults, allowing for significant trauma in the absence of overlying fracture. Therefore, it is not surprising that we did not see a significant association between rib fractures and either PARDS or need for MV. Skinner et al 25 reported that children with chest trauma are more likely to develop PC and less likely to have rib fractures or flail chest compared to adults and are likely to have PC even in the absence of rib fractures. Interestingly, however, we did not see an appreciable difference in median chest AIS score between those children who developed PARDS and those who did not in our study. Although this again could be related to our small study sample size.
Although children with trauma can develop ARDS in the absence of PC, ARDS in patients with PC increases the LOS both in PICU and hospital and increases morbidity and mortality. The presence of PC is associated with increased rate of ventilator-associated pneumonia. 26 Patients with PC have higher incidence of ARDS than chest trauma patients without PC. We showed that it’s probably the development of PARDS and not the mere presence of PC that leads to longer PICU and HLOS and mortality.
Jin et al 5 in their retrospective study of PCs reported an ARDS incidence of 10% and mortality rate in patients with PC to be 3%, though in the presence of ARDS, the mortality rate increased to 30%. Acute respiratory distress syndrome was independently associated with poor prognosis and mortality. Risk factors for ARDS were shock on presentation, coagulation disorder, emergency surgery, infection, blood transfusion, chest tube insertion, and MV. This suggests other factors associated with mortality, rather than just the presence of ARDS. Their lower incidence of ARDS is probably explained by their use of Berlin definition, which needs use of invasive markers such as PaO2 to define ARDS, as opposed to the new PALICC criteria, which helps define and categorize PARDS using titrated oxygen saturations and FiO2 levels obviating the need for PaO2 levels. This highlights one of the advantages of the newer PALICC criteria to define PARDS: the ability to define and categorize PARDS without the need for PaO2 levels.
Our results should be considered acknowledging some limitations. The study design of single-center retrospective introduces inherent bias beyond clinician’s control. Data derived from large registries are limited by what’s entered with little information to the actual timeline of events. Patients with PCs were identified using administrative/diagnostic coding as no set clinical/radiological criteria were in place to define PC during the period of the study. Additionally, given this a single-center study, our sample size is relatively small compared to other reference studies and this may have introduced some inaccuracy in our results. Despite these limitations, our study offers further insight into the nature of PARDS in a homogeneous cohort of children with PC—a subcategory where there exists presently only a paucity of literature. We collected data for a 5-year period, so we don’t think the era factor leading to change in treatment or diagnosis has introduced any bias. The use of extracorporeal membrane oxygenation (ECMO) as a rescue therapy in patients with PC and blunt trauma has been described in literature. 27 Details on discussion about ECMO therapy are not available in view of the retrospective nature of the study, though ECMO as a therapy during the period of the study was unavailable at our center and we are in the midst of building an ECMO program at our center.
Conclusions
In this cohort of children with PCs, the burden of PARDS was relatively high, the presence of PARDS was associated with significantly higher ISS and lower GCS score. In regard to clinical outcomes, the presence of PARDS was significantly associated with increased HLOS and ICU LOS, in addition to mortality. More study with larger sample size is warranted to verify our results and further elucidate the risk factors associated with PARDS and its impact on morbidity and mortality in children with PC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.