
Abstract
A 17-year-old with severe hypertrophic cardiomyopathy (HCM) presented to the emergency department with symptoms of cough, shortness of breath, chest pain, and tactile fevers. She was initially admitted to the cardiac floor, and later transferred to the cardiothoracic intensive care unit on day 5 of illness with deterioration over the next week from BiLevel positive airway pressure to endotracheal intubation. The patient met criteria for severe acute respiratory distress syndrome (ARDS). Standard ARDS lung-protective strategies were refined in consideration of complications caused by her HCM. Such complications included dynamic cardiac outflow obstruction, myocardial ischemia with tachycardia, elevated pulmonary vascular resistance from diastolic dysfunction, and narrow fluid balance window to reduce pulmonary edema while maintaining adequate left ventricular preload. The patient remained refractory despite broad-spectrum antibiotics requiring multiple vasoactive medications, aggressive ventilator management, and inhaled nitric oxide. Social history revealed “vaping” cannabis with butane hash oil prior to symptom onset. Corticosteroids were initiated 2 weeks after initial presentation (day 9 of mechanical ventilation) with rapid recovery and resolution of illness. Acute respiratory distress syndrome is an aggressive disease in the intensive care unit. E-cigarette or vaping product use–associated lung injury is increasingly recognized as a cause of ARDS in adolescents and adults. A complete social history is essential and must be obtained early in all such patients presenting with symptoms of acute respiratory distress and revisited throughout the hospital stay if no other reason for the ARDS is discovered. Disease progression may be subacute with a long interval between onset of symptoms and peak symptoms. The risk of barotrauma is high despite lung-protective ventilation strategies. Management is supportive with resolution over days to weeks. However, other clinical factors may considerably complicate management in cases of underlying comorbidities.
Keywords
Introduction
Acute respiratory distress syndrome represents a complex disease spectrum of acute, severe lung injury leading to respiratory failure. 1 The use of e-cigarettes and “vaping” has recently attracted significant media attention after multiple recent hospital cases have linked it to severe, noninfectious ARDS in adolescents and adults. 2 However, despite a formal Centers of Disease Control and Prevention (CDC) warning, this relatively new source remains underreported in formal medical literature. 3 We report a case of severe ARDS secondary to vaping “Shatter”—a marijuana concentrate produced using butane hash oil (BHO)—in an adolescent female with underlying hypertrophic cardiomyopathy (HCM). We review this emerging etiology of ARDS and highlight important issues in intensive care unit (ICU) management secondary to her underlying condition. Written informed consent for patient information and images to be published was provided by the patient.
Case Report
A 17-year-old female with known severe HCM, status post implantable cardioverter–defibrillator placement, listed status 2A for cardiac transplantation, presented to the emergency department (ED) with one day of shortness of breath, chest pain, and tactile fevers. Patient denied cough, rhinorrhea, nasal congestion, rash, joint pains, fatigue, or myalgias. An echocardiogram confirmed severe HCM with normal systolic function, no left ventricular outflow tract obstruction (LVOTO), and no other changes from previous echocardiograms. In the ED, she was diagnosed with left lower lobe pneumonia, received ceftriaxone, and was admitted to the cardiac floor for observation. Electrocardiogram was unchanged from her baseline ST segment elevations and left ventricular hypertrophy with strain pattern. Her B-type Natriuretic Peptide (BNP) was 1800 pg/mL. Her physical examination upon admission revealed a tired, well-hydrated adolescent female, with nasal flaring, retractions, respiratory rate of 40 breaths per minute, good air entry and bilateral basal rales, heart rate 120 beats per minute without cardiac murmur or gallop, and no hepatomegaly. Capillary blood gas was 7.49/35/58/27/3.4 while on 4 L/min nasal cannula. Chest X-ray (CXR) showed mild left lower lobe opacification, mildly increased interstitial markings, and mild cardiomegaly stable from baseline (Figure 1A). On the cardiac floor, she was started on azithromycin for atypical pneumonia.
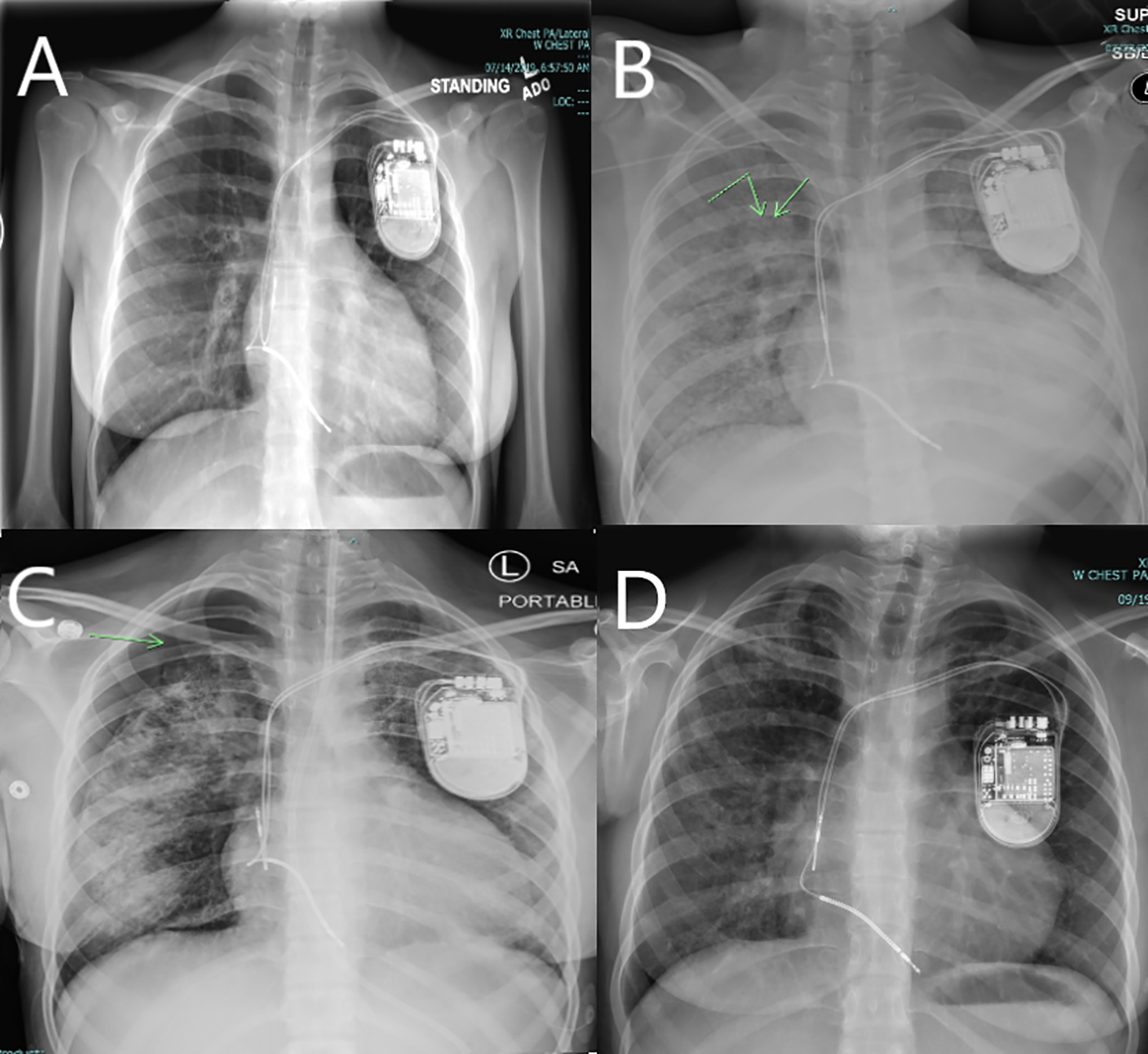
Serial chest X-rays. A, Chest X-ray at admission. The patient has baseline cardiomegaly. Previously placed implantable cardioverter–defibrillator device and leads are in stable position. Lung fields are normal. B, Extensive diffuse bilateral infiltrates with worsening cardiomegaly (day 8). The arrows point to subtle pockets of developing interstitial emphysema. C, Bilateral infiltrates have more consolidated appearance. The arrow shows a prominent right pneumothorax that has developed (day 24). D, Convalescence—bilateral opacities continue to be seen. There is resolving cardiomegaly to baseline (day 66).
Over the next 4 days, she became progressively hypoxemic and tachypneic requiring escalation to non-rebreather mask oxygen. Serial CXR revealed worsening bilateral infiltrates with pulmonary edema and she was transferred to the cardiac ICU on day 5. Over the next 24 hours, the patient rapidly decompensated and was placed on BiLevel positive airway pressure (BiPAP). She developed new fevers to 40 °C and antibiotic coverage was broadened to vancomycin, ceftazidime, and fluconazole. Despite these changes she continued to deteriorate over the next 72 hours with worsening hypoxemia and hypotension requiring endotracheal intubation. She was started on dopamine and milrinone for cardiac support. Flexible bronchoscopy performed immediately after intubation revealed inflamed bronchial mucosa and clear secretions. Bronchoalveolar lavage (BAL) specimen was obtained for diagnostic purposes showing gram stain with rare white blood cells and no organisms; viral studies revealed positive human herpesvirus type 6 (HHV-6) but negative for all other organisms tested. The patient was also started on ganciclovir. Blood and urine cultures were negative.
Acute respiratory distress syndrome lung-protective strategies were initiated targeting low tidal volumes (4-6 mL/kg), permissive hypercapnia, and low airway driving pressure. Her initial ventilator settings were SIMV PC/PS RR: 15, PIP: 28, PEEP: 10, PS: 10, Fi
The patient was hemodynamically labile over the course of her illness; she was maintained on epinephrine and vasopressin. Additionally, due to her HCM heart rates above 120 bpm were associated with worsened hypotension and ST segment elevations. This leads to treatment modifications including an esmolol infusion, use of vasopressin for hypotension, and less aggressive diuresis. Additionally, a pH <7.30 seemed to worsen her hemodynamics so goals for permissive hypercapnia were changed to a pH of 7.30 to 7.35. Nitric oxide was started presuming a component of pulmonary hypertension due to her HCM.
Due to concerns that HHV-6 did not seem a likely etiology, the family was approached multiple times exploring environmental exposures. Over serial conversations with the patient’s friends, a family member discovered the patient had vaped “Shatter” (a cannabis concentrate produced using BHO) the day prior to presentation to the ED.
Due to persistent poor pulmonary and cardiac function and a worsening fever curve without other evidence of infection, methylprednisolone (2 mg/kg/d) was initiated on day 9 of mechanical ventilation for a 28-day course.
4
The ventilator settings immediately prior to initiation of steroids were SIMV PC/PS RR14 PIP 30 PEEP 16 PS 10 Fi
Discussion
“Vaping” is a street term used by individuals to describe the use of vaporizer pens as substance delivery agents. The use of e-cigarettes and “vaping” is increasingly common among adolescents and adults. 5 Novel ways to deliver cannabis are now also emerging using vaporizer pens; a recent report found a significant rise in the use of vaping as an alternative route of administration of cannabis in adolescents and young adults. 5 However, this form of cannabis use may also be an emerging cause of ARDS. Electronic-cigarette, or vaping, product use–associated lung injury (EVALI) is a broad term that has emerged to describe lung injury following the use of e-cigarette or vaping products. A recent CDC report has identified 2807 cases of ARDS attributable to vaping various substances, including cannabis, with 68 confirmed deaths across 29 states. 3 EVALI remains a diagnosis of exclusion at this time. However, a recent study analyzed BAL samples in 51 patients with confirmed or probable EVALI found tetrahydrocannabinol (THC) involvement (detectable THC levels in BAL and/or history of antecedent use) in 94% of patients. 6
The trigger for the ARDS may be due to the exposure to petroleum compounds, specifically BHO. Butane hash oil is used as a solvent to extract more concentrated forms of THC from the marijuana plant. The resultant concentrate can then be inhaled or vaporized via commercially available e-cigarettes and vaporizer pens. 7 Typically, the course following petroleum inhalational injury is an indolent course as was seen in our patient who first developed mild symptoms of lung injury one day after the use of “Shatter” but progressed over the course of more than a week to intubation. Anderson and Zacher recently reported a case of severe lung injury from inhaled BHO an 18-year-old who was regularly using this form of cannabis. Their case showed a similar slow progression of symptoms over several days before the patient presented with hypoxemia to the ED. Their patient was also initially misdiagnosed as an infective pneumonia. 8
Additionally, petroleum-induced lung injury involves a higher incidence of barotrauma. 9 –11 Subtle interstitial emphysema on CXR may be a warning sign as in our patient who developed this finding on CXR 4 days before a spontaneous pneumothorax despite the use of lung-protective ventilation strategies. Friability of the airway mucosa and alveolar surfaces secondary to severe chemical pneumonitis from petroleum compounds (in this case BHO) is the most likely pathophysiology. 12 Tetrahydrocannabinol itself has been shown to carry DNA damaging effects and oxidative stress responses in animal models and is known to acutely increase alveolar macrophages in the respiratory tract. 13 Vitamin E acetate has also been recently implicated after Blount and colleagues recently reported discovering this toxin in 48/51 case samples tested compared to healthy comparators. Vitamin E acetate was subsequently reported as a frequent co-additive agent used to thicken and/or dilute THC oil in vape cartridges. 14 This evidence suggests that vitamin E acetate may be an important modifier that worsens acute lung injury in combination with co-additives such as BHO and/or THC. However, at the time, our case presented this information had not been reported and we did not test for vitamin E acetate in the BAL fluid of our patient.
Our patient’s management was further complicated by the presence of severe HCM which presented unique management challenges. These patients are sensitive to LVOTO from a complex interaction of preload, sympathetic stimulation (myocardial contractility and heart rate), and afterload. Changes in these hemodynamic determinants can precipitate LVOTO in critically ill patients who may not otherwise have LVOTO at baseline. Our patient demonstrated several instances of hypotension with heart rates above 120 bpm. Demand myocardial ischemia with elevated heart rates may be an additional issue. Our patient already had baseline ST segment and troponin elevations that transiently worsened with tachycardia. In general, maintaining adequate preload, preventing tachycardia, and increasing afterload are the cornerstones in preventing dynamic LVOTO. 15,16 In ARDS, these considerations must be counterbalanced with the need to prevent worsening pulmonary edema and typical lung-protective management strategies. We minimized heart rate with an esmolol infusion, maintained afterload with vasopressin instead of a chronotropic agent, and minimized metabolic demands with sedation and paralysis. Appropriate fluid balance was likewise carefully maintained.
An additional consideration is pulmonary hypertension. Patients with HCM are known to have a relatively high incidence of pulmonary hypertension secondary to diastolic dysfunction even in the absence of overt LVOTO. 15,17,18 This baseline postcapillary pulmonary hypertension may worsen acutely with the addition of a precapillary component from severe acute lung injury from interstitial pneumonitis. 19 In such cases, the potential for hyperacute changes to pulmonary vascular resistance secondary to permissive hypercapnia and respiratory acidosis must be kept in mind. In a biventricular patient, these changes may present with hypotension secondary to decreased left atrial and hence left ventricular preload. Inhaled nitric oxide to maintain adequate pulmonary blood flow should be considered in such cases. We also modified pH parameters to maintain pH 7.30 to 7.35 to optimize hemodynamics from a pulmonary vascular resistance standpoint.
The use of steroids for pediatric ARDS remains controversial and steroids have not been routinely recommended for use in these patients. 1,20 However, in practice many clinicians would institute corticosteroids after prolonged illness and Meduri et al have recently recommended a methylprednisolone protocol in moderate-to-severe ARDS which we used in our patient. 4 Interestingly, our patient rapidly improved after initiation of corticosteroids. Sommerfeld et al also reported a case of ARDS in an 18-year-old after e-cigarette use who also demonstrated a rapid improvement after corticosteroids. 21 Other complementary strategies including prone positioning to improve V/Q mismatch and the use of extracorporeal membrane oxygenation may be considered in extremely refractory cases.22
Acute respiratory distress syndrome is an aggressive and potentially fatal disease in the ICU. “Vaping” is increasingly being recognized as a cause of ARDS in adolescents and young adults. A complete social history is essential and must be obtained early in all such patients presenting with ARDS and revisited throughout the hospital stay if no other reasonable trigger is discovered. Disease progression may be subacute with a long interval between onset of symptoms and peak symptoms. The risk of barotrauma is high despite lung-protective ventilation strategies. Management is supportive with resolution over several days. However, special considerations may considerably complicate management in cases of underlying HCM or other chronic illness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.