
Abstract
Purpose:
Chronic obstructive pulmonary disease (COPD) is a common condition, accounting for a significant number of intensive care unit (ICU) admissions. However, little is known about outcomes and costs among ICU patients admitted with acute exacerbations of COPD (AECOPD). We studied predictors of inhospital mortality and costs of ICU admissions for AECOPD.
Methods:
Data were obtained from a prospectively maintained registry from 2 ICUs from 2011 to 2016, including adult patients (age ≥ 18) with an ICU discharge diagnosis of AECOPD. The primary outcome was hospital mortality. Secondary outcomes included ICU length of stay, resource utilization, total hospital costs, and cost per survivor.
Results:
We included 390 patients, of which 27.2% died in hospital. Independent predictors of inhospital mortality included age (odds ratio [OR]: 1.95, CI: 1.58-2.67) and the presence of clinical frailty (OR: 4.12, CI: 2.26-6.95). The mean total hospital costs were Can$35 059, with a cost per survivor of Can$48 191. Factors associated with increased cost included transfer from an inpatient setting, severity of illness, and previous ICU admission.
Conclusions:
Approximately a quarter of patients admitted to ICU with AECOPD died during hospitalization, and these patients accrued significant costs. This study identifies important factors associated with poor outcome in this at-risk population, which has value in risk stratification and patient or family discussions addressing goals of care.
Introduction
Chronic obstructive pulmonary disease (COPD) has a significant global burden on health care systems, affecting 8% to 22% of adults older than 40 years, and is the third leading cause of death worldwide. 1 –3 In Canada, the prevalence of COPD in 2017 was estimated to be 1.2%, 4.2%, and 8.3% in patients aged 35 to 49, 50 to 64, and older than 65 years, respectively, highlighting that although the incidence of COPD increases with age, it is not solely a disease of the elderly individuals. 4
Approximately 1 in 10 hospitalized patients experiencing an acute exacerbation of COPD (AECOPD) will require critical care interventions, specifically in the form of respiratory support and therefore need admission to the intensive care unit (ICU). 5 A meta-analysis that examined predictors for mortality after ICU admission for AECOPD found a cumulative incidence of inhospital mortality ranging between 17.6% and 48.8%. 6 This study identified age, low Glasgow Coma Scale, and respiratory acidemia as factors associated with a higher risk of dying following ICU admission, although significant heterogeneity was noted between studies.
Beyond mortality, health care utilization among patients with this disease remains important. Patients with COPD have 85% higher rates of emergency department (ED) encounters when compared to those without COPD, and both the prevalence of COPD and associated ED visits are increasing. 7 –9 Nationally, it is estimated that the cost to manage patients with moderate and severe AECOPD is between Can$646 and Can$736 million/year. 10 This evidence supports the fact that people with COPD consume a large proportion of overall health care resources. The ICU is a major source of hospital resource use and accounts for a significant proportion of total hospital costs, yet little is known regarding resource use and costs among patients with AECOPD admitted to the ICU, particularly in Canada. 11 A recent Canadian study reported a statistically significant number of patients admitted to ICU with AECOPD meeting criteria for high-cost admissions compared to other primary diagnoses. 12 A large observation study from France with over 600 000 patients with AECOPD demonstrated a trend toward increased admissions, proportion of AECOPD requiring ICU level care, and cost per admission. 13 Similarly, a small study from Greece found that there was an association between both length of admission and ICU level care with higher cost of admission. 14
The aim of this study is to examine survival, resource utilization, and costs among patients admitted to the ICU with AECOPD and additionally determine the factors associated with inhospital mortality and hospital cost.
Methods
Study Design, Setting, and Participants
This study was conducted at 2 hospitals within The Ottawa Hospital Network (Ottawa, Ontario, Canada). The total network has a combined 1163 beds and handles over 160 000 ED encounters annually. Both hospitals have a mixed medical-surgical ICU, each with 28 ICU beds, and approximately 2500 combined ICU admissions per year. Decisions related to ICU admission are made by the attending ICU physician, in consultation with the referring physician.
We conducted a retrospective cohort study between 2011 and 2016 using The Ottawa Hospital Data Warehouse, a health administrative database that has been widely used in previous health services research. 15,16 Data quality assessments were performed during development and are executed routinely as new data are included. We included adult patients (age ≥ 18 years) if they had a primary ICU admission or discharge diagnosis of AECOPD, coded using International Classification of Diseases, 10 Revision (ICD-10). All ICD codes were based on the diagnosis determined by the attending ICU physician. Patients with an admission diagnosis of AECOPD were excluded if there was a more probable diagnosis noted on discharge, such as congestive heart failure. We included all patients regardless of whether they were admitted directly from the ED, transferred from the ward to the ICU, or sent from a peripheral hospital.
We obtained ethics approval for this study from The Ottawa Health Science Network Research Ethics Board.
Data Collection
Hospital clerical staff collected demographic data, comorbidities, Elixhauser Comorbidity Score, and illness severity (scored with the Multiple Organ Dysfunction Score [MODS]) at the time of patient admission, and these data were subsequently stored in the Data Warehouse. 17,18 A single reviewer (MW), blinded to patient outcome, retrospectively abstracted additional variables from the electronic medical record such as most recent pulmonary function test results, use of home oxygen, and disposition (eg, home or long-term care) at time of discharge.
We used a Clinical Frailty Scale (CFS) value of ≥5 to identify patients with frailty. 17 This CFS cutoff has been used by other investigators as a threshold for clinically important frailty in the ICU. 16,19,20 The CFS is a validated scale from 1 to 9, with higher scores corresponding to higher degree of dependency on others for activities of daily living and is derived from global functional status, including activity level and mobility. We generated CFS scores from occupational therapy and physiotherapy notes documenting patients’ baseline function prior to admission and index illness. We used these staff assessments to score each patient on the CFS, using a standardized data abstraction tool. This method has been used previously in critically ill patients and been shown to be reliable in prospective assessments. 16,21,22 We performed data abstraction from patient charts according to the accepted standards. 23 To evaluate reproducibility in abstraction, 2 independent investigators (MW and SMF), blinded to each other’s score, individually evaluated a random sample of 20% of patient records. As inter-rater reliability was excellent (κ = 0.941), a single investigator (MW) completed the remaining records.
The primary outcome was hospital mortality. Secondary outcomes included ICU length of stay (LOS), total hospital LOS, resource utilization (including invasive mechanical ventilation, noninvasive mechanical ventilation, and renal replacement therapy), total hospital costs, and cost per survivor.
Cost Analysis
We determined costs attributed to each patient’s admission using the case-costing system in The Ottawa Hospital, developed by the Ontario Case Costing Initiative and modeled on the Canadian Institute for Health Information Management guidelines. 24 The total cost for each hospital admission is comprised of direct and indirect hospital costs, which includes direct and indirect ICU costs. “Direct” costs refer to all costs that are linked directly to the patient identification number. This includes salaries and benefits for unit producing and management staff, equipment, and screening and procedure materials but do not include physician costs (as physician remuneration is provided by the Government of Ontario and not the individual hospitals). “Indirect” hospital costs refer to any overhead operation fees associated with the service being provided to the patient, such as the cost of the room they occupy. Cost per survivor is calculated by dividing total costs by the number of patients surviving to hospital discharge. All patient costs are compiled and stored in The Ottawa Hospital Data Warehouse. All costs are indexed and displayed in 2018 Canadian dollars.
Statistical Analysis
We conducted all statistical analyses using R (Version 3.3.3; R Foundation for Statistical Computing) and IBM SPSS (Version 24.0; SPSS Inc). We present data as either mean values, with standard deviation (SD), or medians, with interquartile range (IQR). The Student t test (parametric values), Mann-Whitney test (for nonparametric values), and χ2 (categorical values) were performed to determine between-group baseline differences. To evaluate predictors of mortality, we used a logistic regression model based on a priori selection of clinically important variables, as recommended by the PROGRESS guidelines. 25 We included important continuous (age, illness severity [MODS]) and categorical (sex, use of home oxygen prior to admission, frailty, “no cardiopulmonary resuscitation” order at the time of ICU admission, use of invasive mechanical ventilation, and noninvasive ventilation during the index hospitalization) variables. As recommended, we specifically chose to include pre-ICU predictors, rather than post-ICU variables that are already used to estimate cost, such as mechanical ventilation. 26
We assessed variation in total hospital costs using a multivariable generalized linear model with a gamma distribution and a log link function to identify factors that associated with hospital costs and 95% CIs. Generalized linear models are the recommended methodology for modeling the impact of covariates in cost analyses of health services, as they can account for significant skew without the need for retransformation. 27,28 We used a P value of ≤.05 to designate statistical significance.
Results
During the study period, 17 173 consecutive patients were admitted to one of the participating ICUs. Of these, 390 (2.3%) patients were categorized as having a diagnosis of AECOPD. Full demographics of included patients are summarized in Table 1. The majority of patients were residing at home prior to admission (68.7%). Of note, 112 (28.8%) patients were using home oxygen therapy prior to admission, and 147 (37.8%) were categorized as having frailty.
Patient Characteristics.
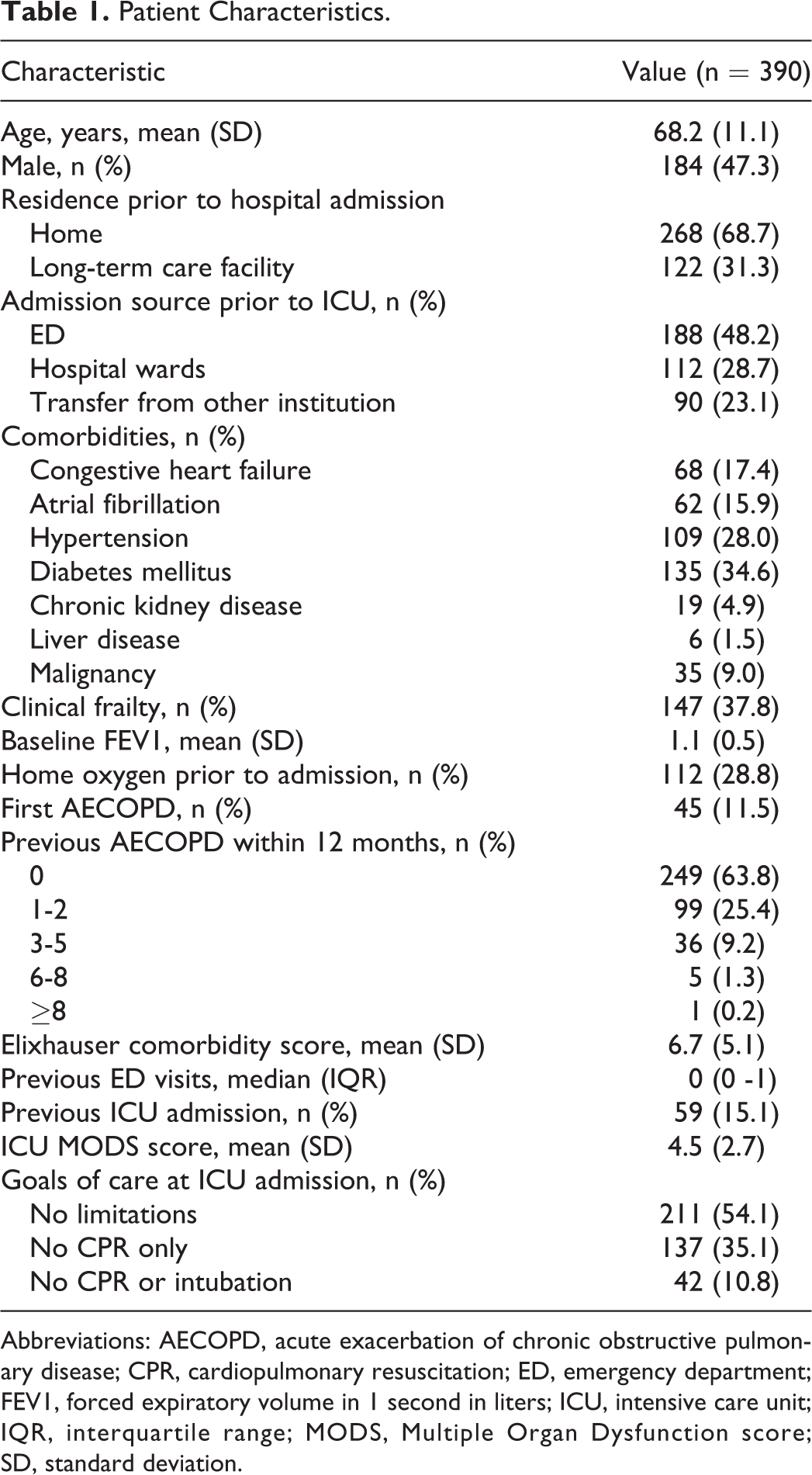
Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; CPR, cardiopulmonary resuscitation; ED, emergency department; FEV1, forced expiratory volume in 1 second in liters; ICU, intensive care unit; IQR, interquartile range; MODS, Multiple Organ Dysfunction score; SD, standard deviation.
Outcomes and resource utilization are outlined in Table 2. Of the patients enrolled, 106 (27.2%) died during hospitalization. The median length of ICU admission was 5 days (IQR: 3-9), during which 126 (32.3%) and 215 (55.1%) of patients required noninvasive and invasive mechanical ventilation, respectively. Among survivors to hospital discharge (n = 284), 129 (45.4%) were discharged home, while the remaining were discharged to a long-term care facility. Independent predictors of hospital mortality included older age (OR: 1.95, 95% CI: 1.58-2.67 for every increment of 10 years) and presence of preadmission frailty (OR: 4.12, 95% CI: 2.26-6.95; Table 3).
Outcomes and Resource Utilization.
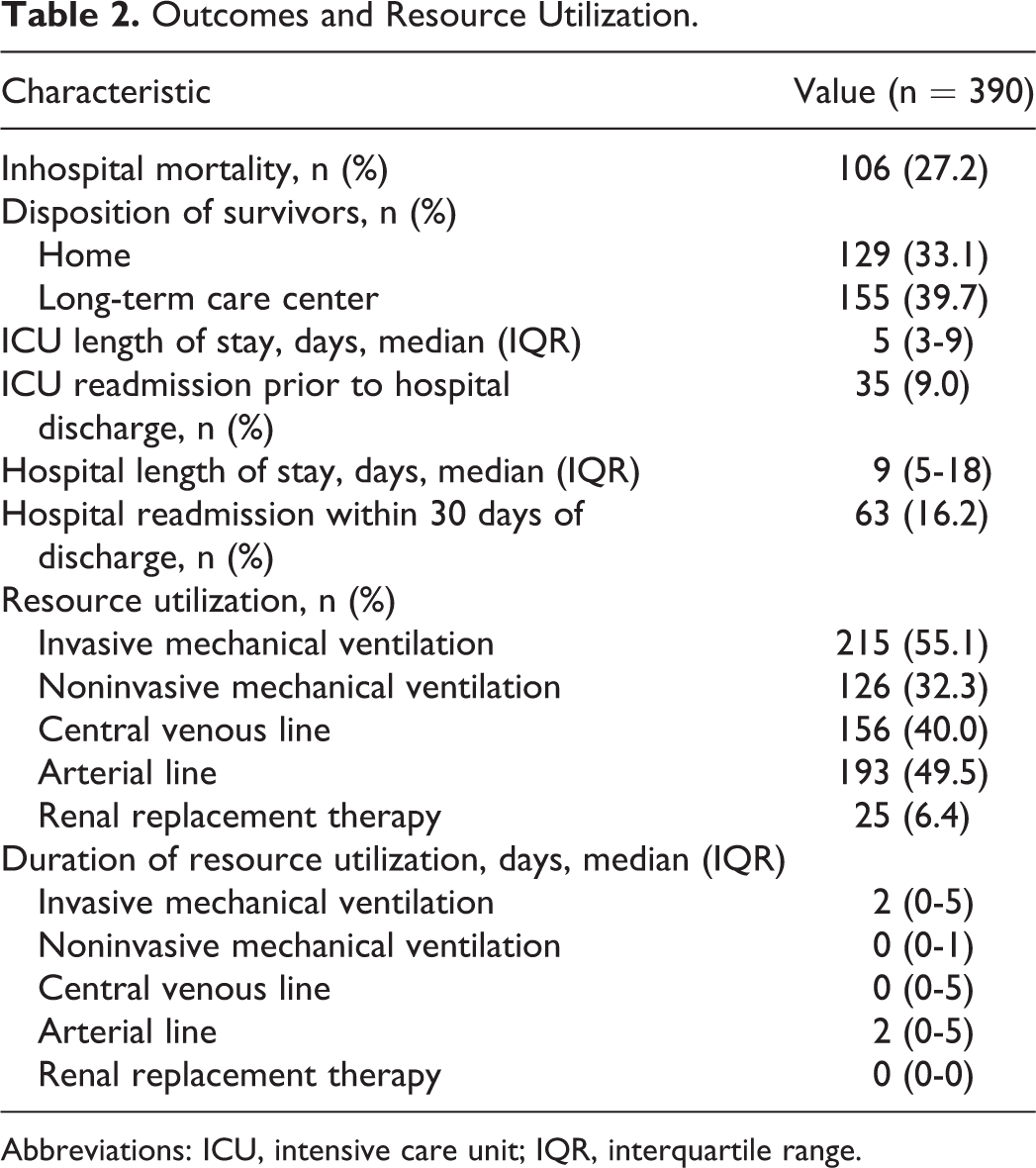
Abbreviations: ICU, intensive care unit; IQR, interquartile range.
Multivariable Logistic Regression for Prediction of Hospital Mortality.
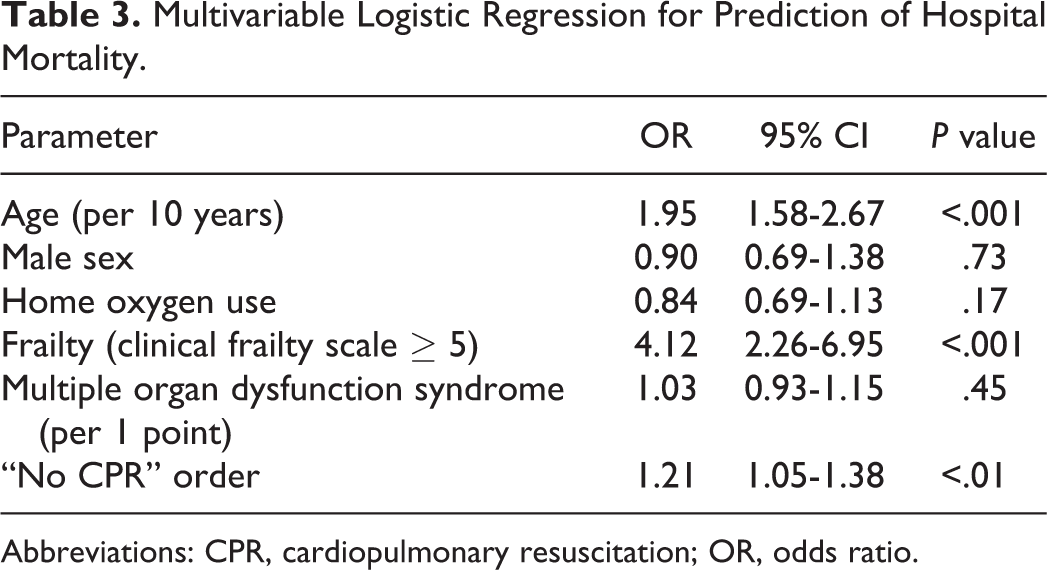
Abbreviations: CPR, cardiopulmonary resuscitation; OR, odds ratio.
The mean total cost per patient admitted to the ICU for AECOPD was Can$35 059 (SD: Can$35 481), and the mean cost per survivor was Can$48 191 (Table 4). Factors associated with increased cost included severity of illness, transfer from an inpatient setting (in contrast to conventional admission through the ED), severity of illness (by MODS), and previous ICU admission (Table 5).
Patient Hospital Costs.
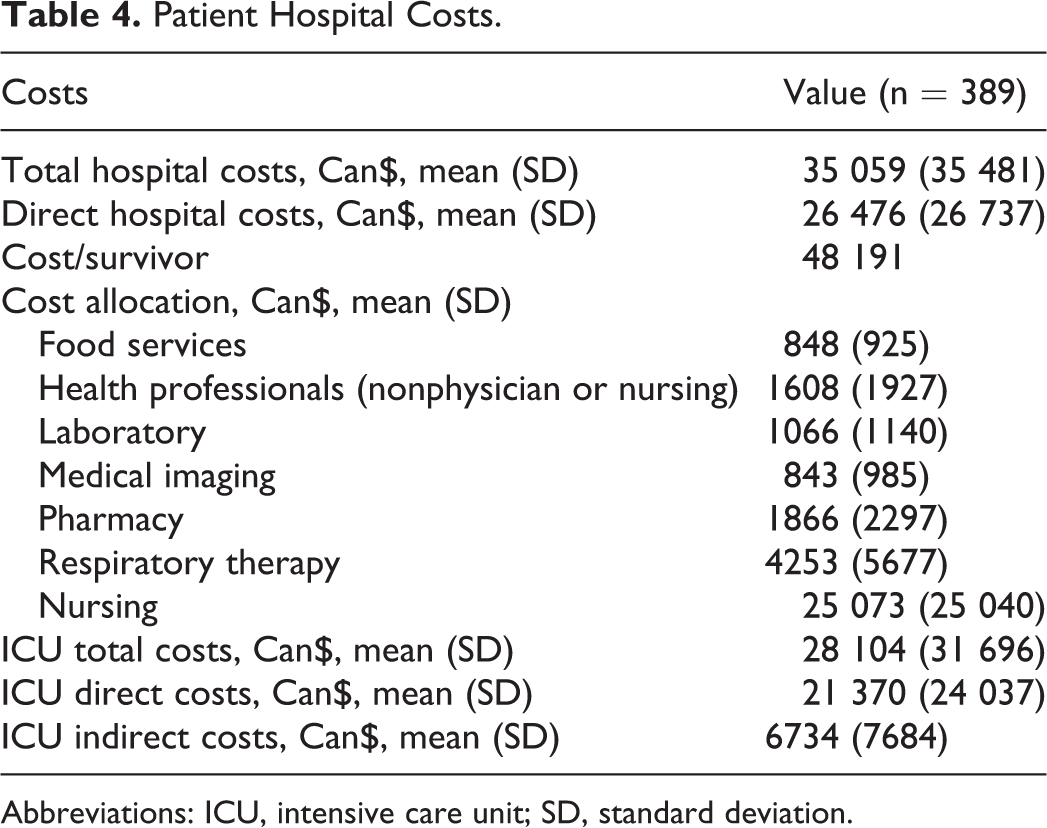
Abbreviations: ICU, intensive care unit; SD, standard deviation.
Multivariable Generalized Linear Model for Total Hospital Costs, Ran With Gamma Distribution and Log Link.
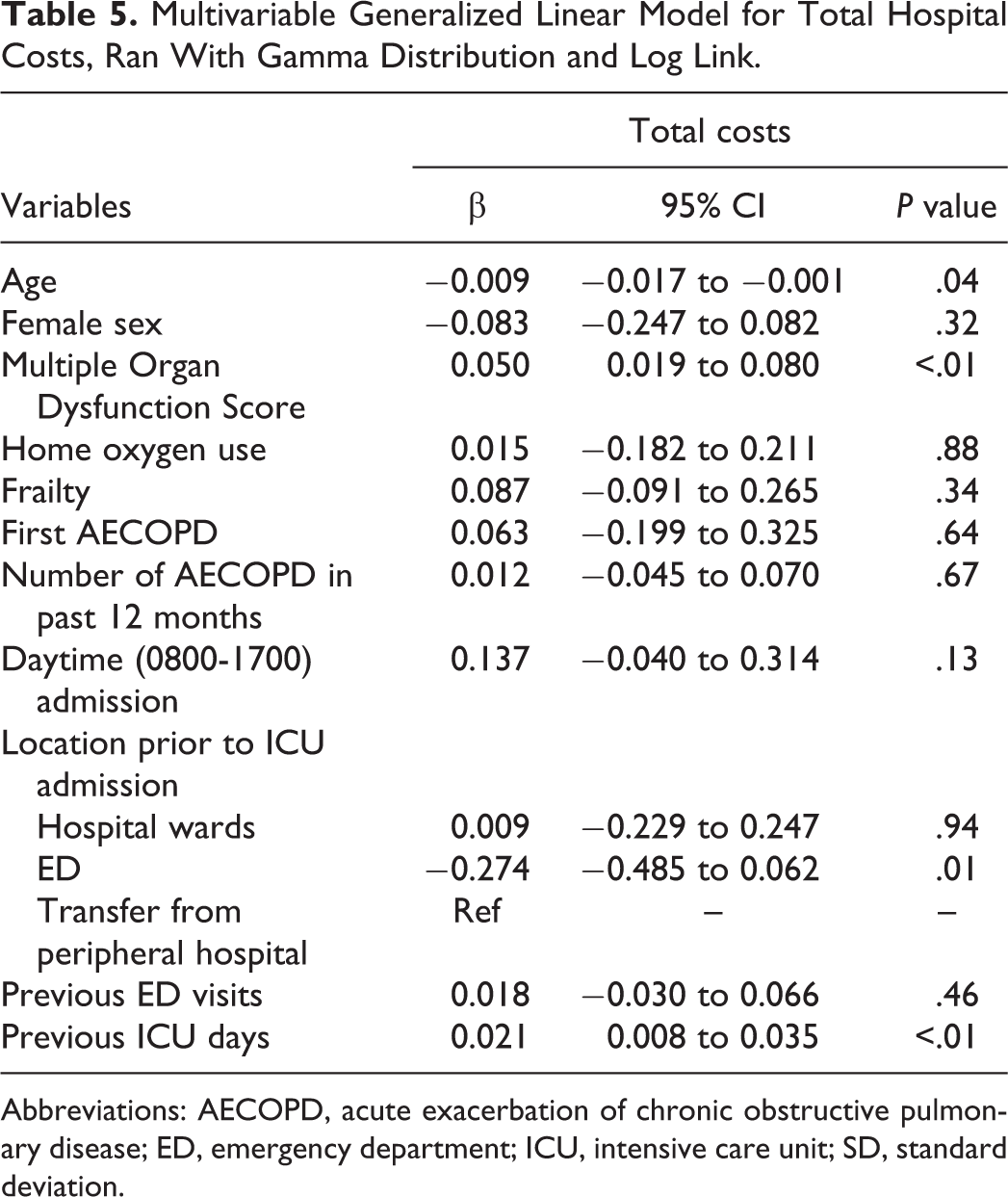
Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; ED, emergency department; ICU, intensive care unit; SD, standard deviation.
We further evaluated differences between patients having AECOPD with frailty and those without (Supplemental Table S1). Patients with frailty were more likely to use preadmission home oxygen and more likely to have had a previously documented admission for AECOPD.
Discussion
Among patients admitted to ICU for AECOPD, we found that over one-quarter died in hospital and that this patient population consumed significant hospital resources. Increased age and the presence of frailty predicted higher odds of dying, however severity of illness at the time of ICU admission did not. Prolonged ICU or hospital LOS was associated with total hospital costs. Taken together, our results provide important prognostic and resource utilization information for clinicians who care for this high-risk ICU patient population.
During the study period, patients with AECOPD accounted for 2.3% of ICU admissions, but 27.2% of these patients died in hospital, which is consistent with previous reports. 29 Identification of factors associated with mortality yielded several important findings. Unsurprisingly, increasing age predicted mortality. However, independent of age, we also found that frailty, a multidimensional syndrome of loss of reserves that gives rise to vulnerability, was strongly associated with hospital mortality. 30 While frailty is more common among older patients, it is also seen among younger hospital patients, and in particular among patients with severe comorbidities, such as COPD. 31 Previous ICU-based studies have shown that frailty is associated with both short- and long-term mortality among critically ill patients. 16,19,20,22 Given dyspnea has a profound impact on many patients’ mobility and functional status, it would be anticipated that those living with COPD would have higher rates of frailty and this may predispose such patients to worse outcomes during exacerbation and when critically ill. 32 Approximately one-third of patients in the study were classified as frail, mirroring results from previous critical care studies looking at patients admitted to ICU regardless of primary diagnosis. 33 The clinical implication of this finding is 2-fold. First, frailty represents a potentially modifiable risk factor that could be improved in patients with COPD through interventions such a pulmonary rehabilitation programs. 34 Second, knowledge of a patient’s functional status can help guide discussions around goals of care and prognosis between patients, families, and the health care team in both the inpatient and outpatient settings.
Interestingly, home oxygen therapy prior to admission was not found to be predictive of mortality, which was unexpected given that these patients likely have more severe pulmonary disease. The reason for this is unclear. Patients on home oxygen with AECOPD and require slightly more oxygen than baseline may need ICU monitoring and different oxygen delivery interfaces allowing for more oxygen delivery than can be conducted with nasal cannulas. When patients with comparatively mild disease who are not on home oxygen have an AECOPD necessitating ICU monitoring, this likely represents a larger departure from baseline and theoretically a more severe exacerbation. Alternatively, this may represent selection bias in our cohort, as patients with home oxygen may have such severe and irreversible disease that only a small proportion are ultimately admitted to the ICU.
The mean cost for admission was Can$35 059, with a higher cost of Can$48 191 for each patient surviving to discharge. Older age was associated with lower cost for admission, perhaps secondary to earlier mortality during hospital stay, and reduced utilization of invasive therapy compared to younger patients. In contrast, illness severity, admission from the ward (as opposed to ED), and previous ICU admission were all associated with increased cost. The increased expenditure associated with transfer from an inpatient ward to the ICU may be due to higher risk of resistant or hospital acquired pathogens as triggers for the exacerbation (which are more expensive to treat), or due to a higher burden of deconditioning secondary to an already prolonged hospital admission. 35
Although we used a large, multicenter data registry of ICU patients admitted with AECOPD, this study has limitations. Most importantly, outcomes among critically ill patients are influenced by advanced care directives; and while we included such directives from ICU admission in our models, we do not have data related to how goals of care changed during ICU and hospital admission. Second, while data were collected and stored prospectively, they were retrospectively gathered and analyzed, which has the potential to influence both reliability and validity. Further prospective analysis may be useful in deriving predictive models for risk stratification of patients admitted to ICU with AECOPD. Third, we screened for frailty retrospectively using the CFS, however this tool was designed for prospective application. 30 While this has the potential to introduce bias, we used previously described methods, and such retrospective methods have been shown to have strong concordance with prospective CFS measurements. 16,21,22
A fourth limitation is that patients were not stratified based on presence of infection (ie, positive blood cultures, clinical suspicion). It would be anticipated that patients who were septic at the time of admission would likely have had worse outcomes. This represents an important target for future studies. Finally, the sample size of our cohort was relatively small, and while our data were gathered from 2 hospitals, they exist within the same city, and therefore may potentially be biased by regional practice variation.
Conclusion
We found that patients with AECOPD admitted to ICU had high hospital mortality and total costs. We identified novel and important predictors of mortality in this population, including age and clinical frailty. This study also highlights the significant cost of AECOPD admissions in Canada. Collectively, these findings have the potential to inform future resource allocation and may be used to guide discussions with patients having COPD and their families prior to AECOPD.
Supplemental Material
Supplemental Material, COPD_ICU_Supp_Table_1 - Outcomes and Resource Utilization Among Patients Admitted to the Intensive Care Unit Following Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Supplemental Material, COPD_ICU_Supp_Table_1 for Outcomes and Resource Utilization Among Patients Admitted to the Intensive Care Unit Following Acute Exacerbation of Chronic Obstructive Pulmonary Disease by Madeleine Warwick, Shannon M. Fernando, Shawn D. Aaron, Bram Rochwerg, Alexandre Tran, Kednapa Thavorn, Sunita Mulpuru, Daniel I. McIsaac, Laura H. Thompson, Peter Tanuseputro, Kwadwo Kyeremanteng and On Behalf of the Resource Optimization Network in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Peter Tanuseputro is supported by a PSI Graham Farquharson Knowledge Translation Fellowship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.