
Abstract
Background:
Pharmacogenomic (PGx) testing has the potential to provide information on specific drug-metabolizing enzymes that may lead to an absence, reduction, or increase in medication effect in patients. There is a paucity of prospective studies examining PGx testing in the intensive care unit (ICU) setting.
Research Aims:
To (1) obtain a PGx panel in a sample of cardiovascular (CV) surgical patients with a planned ICU stay and identify phenotypes, and (2) identify PGx variants that may inform treatment regimens and may warrant prescribing adjustments.
Design and Methods:
Descriptive, single cohort cross-sectional design. Adult (≥18 years) CV patients with an anticipated postoperative ICU stay were enrolled from a large Midwestern tertiary academic medical center. Eligible patients provided informed consent at the time of their CV clinic appointment; PGx testing was then ordered. Pharmacogenomic testing consisted of the Focused Pharmacogenomics panel which included 10 genes and 55 medications.
Results:
Of the 272 patients screened, 100 (68% male) patients completed PGx testing (mean age 66.2 ± 9.6 years, mean Acute Physiology, Age and Chronic Health Evaluation III score 76.1 ± standard deviation). Pharmacogenomic results were available in the medical record within a median of 52.4 hours (interquartile range: 33.4-80.3). Pharmacogenomic testing results identified 5 CYP2C19 poor metabolizers, 26 CYP2C19 rapid metabolizers, 5 CYP2C19 ultrarapid metabolizers, 6 CYP2D6 poor metabolizers, 5 CYP2D6 poor to intermediate metabolizers, and 2 CYP2D6 rapid metabolizers identified. Overall, 98% of patients had actionable or potentially actionable PGx results, including 82% for warfarin, 65% for propafenone, 65% for tramadol, 46% for oxycodone, 45% for metoprolol, 33% for clopidogrel, 32% for proton pump inhibitors, 25% for statins, and 12% for haloperidol.
Conclusions:
A significant portion of patients had identified genetic variants that may warrant changes in medication management during and after CV-ICU stay. It remains to be seen if PGx testing leads to improvements in ICU patient outcomes.
The National Institutes of Health All of Us research program was launched in 2016 to accelerate health research and medical breakthroughs, enabling individualized prevention, treatment, and care for all persons. 1 Data from one million participants will be used to learn about individual differences, including lifestyle, environment, and biology, that influence health and contribute to disease. 1 The Precision Medicine Initiative aims to develop individualized care based on biology, behavior, genetics, environment, and data science. Although an exciting new horizon in health care, the immediate application of individualized, precision health care for all Americans may be years away.
One area of immediate importance to critical care clinicians is the extreme variability in patients’ responses to medication therapies. Pharmacogenomics (PGx) is an emerging field in precision health care generally concerned with genetic polymorphisms in drug-metabolizing enzymes, transporters, receptors, and drug targets that explain interindividual variation in drug efficacy and toxicity. 2 Pharmacogenomics has a prominent place in cardiovascular (CV) medicine due to well-documented biomarkers of altered efficacy and safety for frequently used medications including clopidogrel (CYP2C19) and warfarin (CYP2C9/VKORC1). 3 Unfortunately, application of testing to determine genomic variability in drug metabolism among critically ill intensive care unit (ICU) patients has received little attention, 4 likely due to PGx test results not being readily available at the time of admission to the ICU for most patients. Furthermore, the turnaround time from test order to result reporting can range from days to weeks, making testing impractical in the ICU setting.
A large number of PGx variants with demonstrated clinical utility are known and have been incorporated into drug labeling by the United States Food and Drug Administration (FDA); this table includes 385 entries (270 unique drugs) as of January 2020. 5 In fact, the FDA recently updated the Table of Pharmacogenetic Associations supported by scientific evidence (Delete and query 2/20/2020 reference link here). 6 Among critically ill patients, known factors that influence responses to medication therapy include sex, age, severity of critical illness, and concomitant medications. 4 Pharmacogenomic testing has the potential to provide information on specific drug-metabolizing enzymes that may lead to an absence, reduction, or increase in medication effect. 4 Given the extreme heterogeneity of responses to medications among critically ill patients, PGx testing may have the potential to improve care for these patients. However, there is a paucity of prospective studies investigating the influence of PGx testing on ICU patient outcomes.
Laboratory technological advances have allowed for multiplexing and higher throughput, resulting in significant decreases in the cost of genetic testing and increased access to genetic information for patients and their providers. Integration of genetic data into the clinical decision-making process has the potential to significantly advance the practice of precision medicine and, in the case of PGx, ultimately affect every patient including those receiving care in the ICU. Thus, to begin to address these shortcomings, the specific aims of our study were to (1) obtain PGx testing in a sample of CV surgical patients with a planned ICU stay and describe phenotypes, and (2) identify PGx variants that may inform treatment regimens and may warrant prescribing adjustments among CV-ICU patients.
Methods
A descriptive, single cohort cross-sectional design was used to address the aims of our study. Approval for the use of human subjects in research was secured from the institutional review board of Mayo Clinic prior to enrollment (IRB# 18-001691). Patients were screened for enrollment eligibility from the Mayo Clinic, Rochester Cardiovascular Surgery clinic through electronic patient appointment calendars. Inclusion criteria included any patient age ≥18 years scheduled for CV surgery with an anticipated stay in the ICU for postoperative care who was able to provide written informed consent. Patients aged <18 years, scheduled for a ventricular assist device implantation, with known pregnancy, uncontrolled concurrent illness including documented psychiatric illness, or who lacked capacity to provide own informed consent (ie, documented dementia), or planned surgery occurring <24 hours from consent time, were not approached for participation. A target sample of 100 patients was established a priori to provide sufficient data to address our aims and inform future investigations. Eligible patients provided written informed consent at the time of their initial Cardiovascular Surgery clinic appointment. Patients were provided a brochure explaining PGx testing. A blood sample was drawn for PGx testing with other preoperative labs or testing was added to a previously drawn blood sample.
Variables and Their Measurement
Data were extracted from the electronic health record (EHR) into a Research Electronic Data Capture (REDCap). These data included demographic characteristics (age, sex, race, ethnicity), type of CV surgical procedure, ICU clinical data including length of mechanical ventilation, length of ICU stay, illness severity, medications received, and the PGx panel results.
Description of focused PGxs panel
The Focused Pharmacogenomics Panel was developed and performed in the Personalized Genomics Laboratory at Mayo Clinic. This laboratory test includes CYP1A2, CYP2C19, CYP2C9, CYP2D6, CYP3A4, CYP3A5, CYP4F2, SLCO1B1, VKORC1, and rs12777823, which is a single nucleotide polymorphism located in the CYP2C gene cluster associated with warfarin response in individuals of African descent.
Pharmacogenomic testing
Testing was performed using an open array based on TaqMan chemistry on a QuantStudio 12K Flex instrument (Thermo Fisher Scientific). For CYP2D6, copy number analysis was performed using a real-time polymerase chain reaction–based method that evaluates the promoter, intron 6, and exon 9. Depending on the CYP2D6 results, rare samples required Sanger sequencing for precise resolution of genotype and phenotype. When variants were present, the allele detected was given a name, represented by an asterisk (*) followed by a number. The results of individual variants for each gene were combined to determine the star alleles present, based on data available at PharmVar and/or PharmGKB. 7,8 For example, when CYP2D6 testing reveals a heterozygous c.100C>T and a heterozygous and c.506-1G>A variant, the 2 variants are assumed to be in cis (on the same allele), based on population allele frequency data, and a genotype call of *1/*4 is made. 7 A genotype of *1 is assigned in the absence of detected variants. Next, a phenotype was predicted based on current knowledge found in the literature, PharmVar, and CPIC guidelines 9 of the functional consequences of the identified variants. Finally, medication recommendations were provided on the report, based on information found in FDA labels, 5 CPIC guidelines, and the literature. Recommendations presented to providers included 55 medications across a broad range of indications that have strong evidence to support the use of PGx to guide their administration, in the FDA label, practice society guidelines, or from strong literature. 7 –9 Pharmacogenomic results were categorized as “actionable or non-actionable” based on whether or not a provider should consider a medication change based on the report.
Statistical Analysis Plan
Descriptive statistics (mean, standard deviation, counts, percentage, median, interquartile range [IQR]) were used to describe the patients’ demographic and clinical characteristics, to report PGx testing results (counts, percentage), and to summarize any identified genetic variants by medications.
Results
Demographic and Clinical Description of Patients
A total of 272 patients were screened between July 2018 and October 2018. Of these, 119 patients met the inclusion criteria and were identified as eligible for the study. Within this group, 108 patients provided written consent (90.7% consent rate). Eight patients were withdrawn due to lab collection issues or cancelation of CV surgery. One hundred patients completed the blood collection and testing which comprised our study sample. Of these 100 patients, the mean age was 66.2 years and the average illness severity as measured by the Acute Physiology, Age and Chronic Health Evaluation III score was 76.1. The demographic characteristics of the sample were 68% male, 85% Caucasian race, and 80% non-Hispanic (Table 1). In this patient sample, 77% underwent valvular surgery including 48% in an open-chest procedure and 29% in a minimally invasive procedure; 12% underwent a coronary artery bypass procedure. The remainder of the patient sample underwent a variety of other CV surgical procedures (Table 2). Results from the PGx test were available in the EHR within a median of 52.4 hours (IQR: 33.4-80.3 hours).
Demographic and Clinical Characteristics of Patient Sample.a
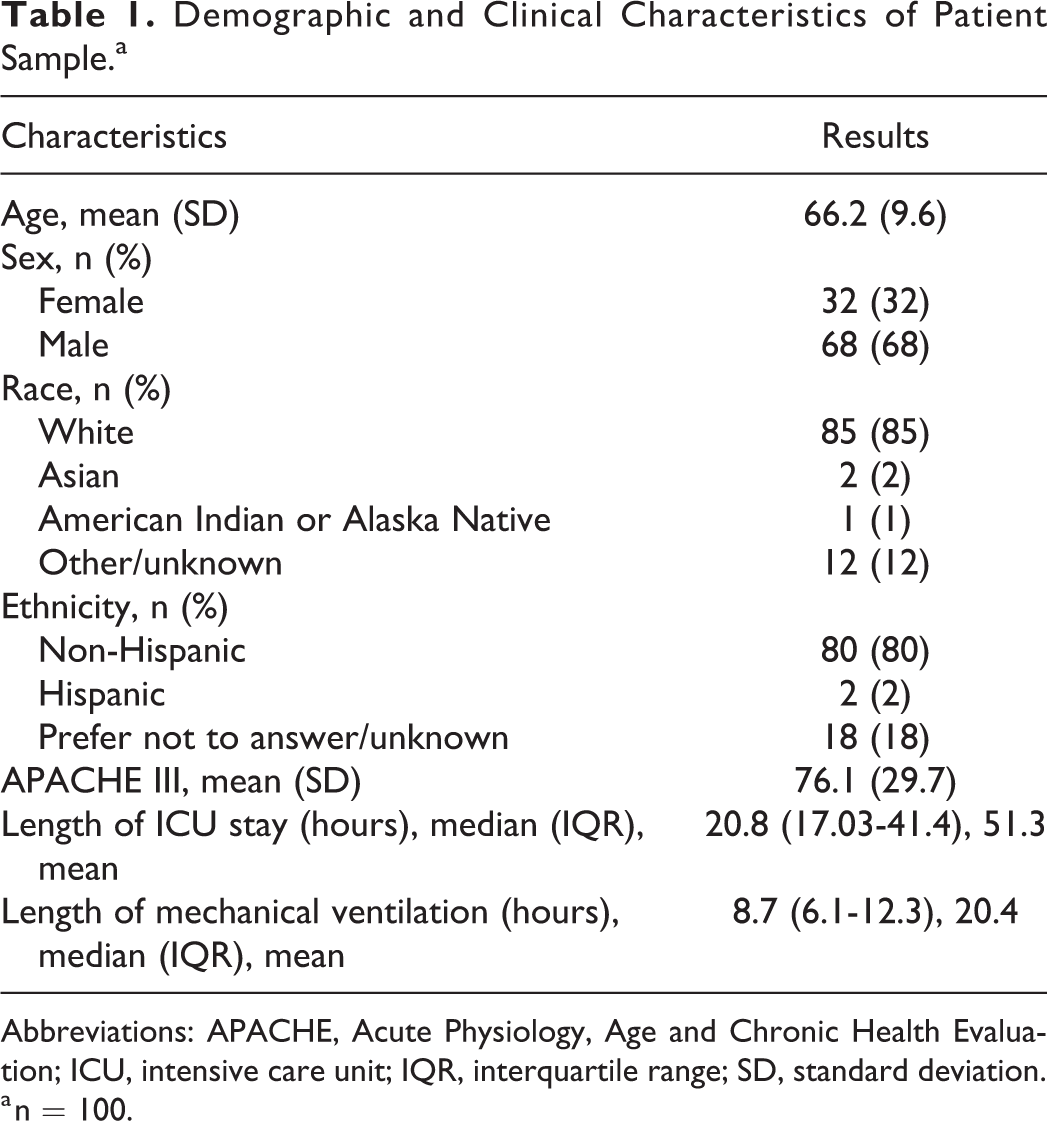
Abbreviations: APACHE, Acute Physiology, Age and Chronic Health Evaluation; ICU, intensive care unit; IQR, interquartile range; SD, standard deviation.
a n = 100.
Cardiovascular Surgical Procedures.a
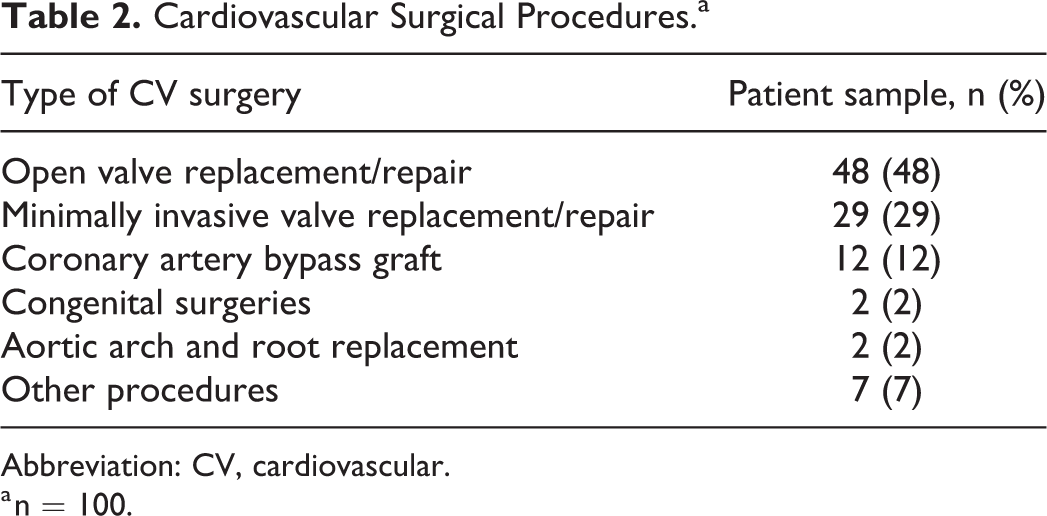
Abbreviation: CV, cardiovascular.
a n = 100.
Description of PGx Testing Phenotypes and Actionable Variants
Pharmacogenomic phenotypes
Table 3 summarizes the predicted phenotypes reported for the cohort. The observed phenotypes were consistent with expectations for a predominantly Caucasian population. 10 Phenotypes corresponding to markedly decreased metabolism (eg, poor metabolizers or poor to intermediate metabolizers) or increased metabolism (eg, rapid or ultrarapid metabolizers) often have the most pronounced clinical impact, particularly for CYP2C19 and CYP2D6, which are involved in metabolism of many medications. In our cohort, there were 5 CYP2C19 poor metabolizers, 26 CYP2C19 rapid metabolizers, 5 CYP2C19 ultrarapid metabolizers, 6 CYP2D6 poor metabolizers, 5 CYP2D6 poor to intermediate metabolizers, and 2 CYP2D6 rapid metabolizers.
Phenotypes of Patients by Gene.a
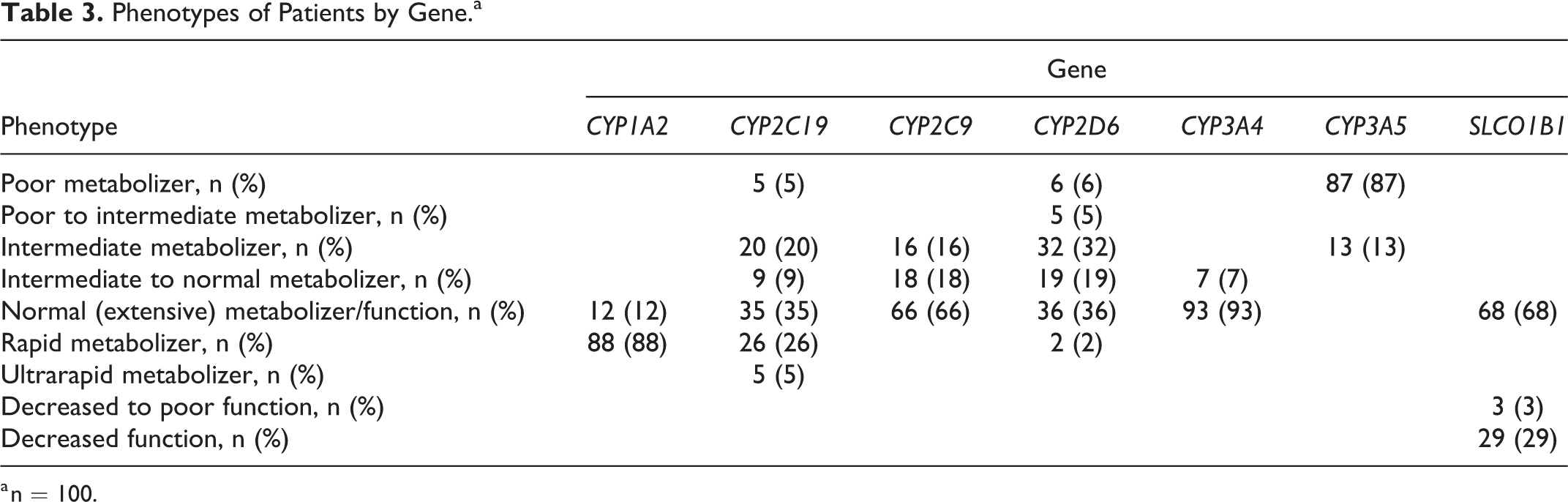
a n = 100.
Description of actionable variants by medications
Overall, 98% of patients had actionable or potentially actionable results. Actionable results include a recommendation to increase or decrease a medication dosage, alert for adverse event potential, recommendation for alternative medication, or recommendation for additional PGx testing. Among medications commonly used in the CV-ICU, 82% of patients had a result suggesting warfarin dose adjustment on initiation. In addition, many had variants that predicted a potential PGx interaction relevant to other commonly used medications: 65% for propafenone, 65% for tramadol, 46% for oxycodone, 45% for metoprolol, 33% for clopidogrel, 32% for proton pump inhibitors, 25% for statins, and 12% for haloperidol.
Discussion
To our knowledge, this is the first prospective study to report PGx testing, including a description of phenotypes and clinically relevant implications of PGx testing results, in a cohort of CV surgical ICU patients. Recent articles have focused on describing PGx and the potential usefulness of precision medicine in critical care. 11,12 Although we are not aware of any comparable studies describing PGx testing in the ICU, our results demonstrate that genomic testing can be accomplished within the setting of critical care, albeit limited to those patients with a planned ICU stay. Actionable variants in our patient sample have the potential to influence clinical practice. Patients undergoing CV surgery typically require anticoagulation or antiplatelet therapy. Within this sample, 82% had a result suggesting a warfarin dosing adjustment may be required on initiation of therapy. 13 The combination of CYP2C9, VKORC1, CYP4F2, and rs12777823 results was used to provide this recommendation. Consequently, these patients may benefit from a different warfarin protocol, such as one that decreases the starting dose on therapy initiation. A third of our patients had clopidogrel results that indicate reduced metabolism to active medication. This could result in a subsequent reduction in platelet inhibition and a poor CV outcome. 14
Although statins are recommended after CABG, 15 one-fourth of the patients in our sample were at risk for adverse events based on altered hepatic transport of statins, potentially leading to adverse events. Additionally, 11% of sample patients were at risk for ineffective lowering of their lipid levels based on the processing of pravastatin. Knowledge and understanding of actionable PGx results may warrant providers to consider prescribing an alternate statin.
The majority of patients with actionable results for propafenone, metoprolol, and haloperidol indicated a lower dose may be needed due to reduced clearance. The results for proton pump inhibitors and ondansetron also indicated the potential of suboptimal response secondary to increased metabolic clearance of these drugs. For the prodrugs oxycodone and tramadol, most of the results indicated a potential risk for insufficient analgesia due to reduced activation.
There are a number of limitations to this study. The first limitation is that not all medications relevant to the ICU setting have been studied for PGx interactions. The PGx lab panel used in our study is currently limited to 55 medications, based on evidence supporting actionable results. The specific PGx test utilized in our study contains a discrete number of genotypes and actionable medication recommendations not specific to ICU patients. Therefore, our results do not include all medications typically administered to patients in the ICU. Future PGx testing panels may contain more genes that would allow for inclusion of more medications. Patients included in the study sample were limited to those with scheduled, nonemergent CV surgery with an expected postoperative ICU stay in order to provide sufficient laboratory processing to post results to the EHR. In most critical care scenarios with emergent admission to an ICU, real-time testing may be beneficial but complicated by no point-of-care capabilities at this time. Operationally, there are many logistical challenges to achieving a quick test result turnaround time. Future studies could optimize preanalytical processes to reduce time to specimen collection, facilitate rapid delivery of the specimen to the laboratory, and to potentially increase the frequency of test setup in the laboratory to multiple runs per day to further decrease the turnaround time. This study was also limited by the descriptive design and single cohort nature of the study with findings that are not generalizable. Lastly, we did not investigate whether providers utilized the PGx results in their ICU patient care.
Implications of Results for Research and Practice
The use of PGx testing in critical care has significant implications for future research and practice. Future research should focus on the integration of PGx information to guide precision-based care of critically ill patients. It is imperative that studies be conducted regarding actionable recommendations derived from PGx testing and how that information contributes to outcomes among ICU patients. Currently, there is no point-of-care testing available for rapid reporting of PGx results, beyond CYP2C19 that is limited to detection of 3 alleles. 16 However, patients may already have PGx results contained in their EHR which can be accessed to guide both medication therapy and clinical decisions for optimal management during and after an ICU stay. As the practice of preemptive testing grows and results are readily available at the time of ICU admission, the use of these results will be increasingly feasible.
All members of the ICU care team will need to acquire basic knowledge of PGx as another source of data to inform practice. This may require education and training of ICU providers in genomics broadly and PGx testing more specifically. Understanding a patient’s drug-metabolizing profile informed by PGx testing has not only the potential to improve individual therapy but to also avoid serious side effects leading to prolonged length of stay, additional laboratory testing expense, or unnecessary interventions. Lastly, precision-guided symptom management could be realized through the application of PGx testing. Availability of PGx testing results in the EHR and knowledge of how a patient may metabolize and eliminate a medication has vast potential to better equip clinicians to manage patients and improve outcomes.
Conclusions
Results of this single-center cohort descriptive study indicate that patients receiving care in the CV-ICU have a number of genotypes and phenotypes that warrant medication treatment considerations. Pharmacogenomic testing results in the EHR have the potential to be an important source of information to guide individualized prescribing and administration of medications to manage symptoms and improve patient outcomes throughout a patient’s care trajectory. Although current available laboratory testing is limited by use of a targeted genotyping approach, availability of evidence for a subset of medication, and turnaround time to report results, future research integrating PGx data into patient care is on the horizon to inform individualized, precision care for all patients including those in ICUs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported, in part, by the Mayo Clinic Center for Individualized Medicine and by Mayo Clinic Research Funds.