
Abstract
Purpose:
Etomidate causes adrenal insufficiency. Yet in critically ill patients, it is controversial whether it increases mortality rates above that of comparator anesthetic induction agents. We postulated that etomidate would increase relative mortality rates correspondingly to the severity of illness as defined by SAPS or APACHE scores.
Materials and Methods:
A literature search was performed on Pub Med, SCOPUS, and Cochrane Reviews for human studies, regardless of language, between 1983 and February 2020. The search strategy used keywords, “etomidate,” “adrenal insufficiency,” “glucocorticoid,” and “intensive care.” Both authors reviewed electronic data search titles, abstracts and extracted data, which were checked by the other reviewer. Primary outcome was 28-day survival. Secondary outcome was adrenal insufficiency.
Results:
There were 29 trials of etomidate versus comparators in 8584 patients. Etomidate was associated with adrenal insufficiency (risk ratio (rr) = 1·54, 95% CI; 1·42, 1·67, p < 0.001) and increased overall relative mortality rates (rr = 1.09, CI;1.04,1.16, p = 0.001). Meta-regression showed that with etomidate there was a continuous progressive relative risk of mortality associated with increasing severity of illness (predefined in each article by standard critical illness scores). In those patients who had a predicted mortality rate > the median for this analysis (predicted mortality 44%) the relative mortality rate (rr) = 1.20, Ci;1.12,1.29, p < 0.001, the absolute risk difference (rd) = 0.08, CI;0.05,0.11, p < 0.0001 and the number needed to harm (1/rd) was 12.5. In those with a calculated predicted mortality <44% there was no increase in relative mortality rate.
Conclusions:
Whereas etomidate causes adrenal insufficiency, it was not shown to increase mortality in many analyzed here in ICU settings. However, etomidate associated relative mortality rates increased progressively and correlated with the severity of critical illness scores. Intensivists should anticipate the need for glucocorticoid supplementation after etomidate in those with severe critical illness and in those with acute deterioration of vital signs.
Keywords
Introduction
Adrenal insufficiency may be life threatening, especially in states of critical illness. 1 The Society of Critical Care Medicine and European Society of Intensive Care Medicine have further defined the management of critical illness related corticosteroid insufficiency (CIRCI) as a “dysregulated systemic inflammation from inadequate intracellular glucocorticoid activity relative to the severity of the underlying critical illness.” 2 During the early trials of corticosteroids in management of septic shock it was noted that many patients with CIRCI had received etomidate as an anesthetic induction agent. 3 Etomidate is a preferred anesthetic induction agent for rapid sequence intubation due to low cardiovascular side effects. 4 However, it is well known that etomidate causes adrenal insufficiency by inhibiting the CYP 11β hydroxylase enzyme in adrenal cortisol synthesis. 5 –7 Although there is universal agreement that etomidate causes adrenal insufficiency, there continues to be controversy whether this results in increased mortality in critically ill patients. 8,9 We 10 and others 8,11 have reviewed this relationship of etomidate and showed increased mortality in patients with septic shock whereas another review did not show this relationship of etomidate with increased mortality. 12 Trials with the addition of corticosteroids to those who received etomidate have shown mixed outcomes. Two studies had no survival benefit 13,14 and 1 post hoc analysis showed a 30% improvement in those with a very high risk of mortality. 15
Corticosteroid levels are physiologically increased in proportion to the level of severity of illness as measured by clinical severity scores. 16,17 Etomidate does not completely block the synthesis of cortisol when compared to a standardized metyrapone challenge test. The latter is expected to achieve complete adrenal suppression (i.e., a serum cortisol <138 nmol/L and an 11-deoxicortisol level > 193nmol/L). 6 In 1 study in children, 18 etomidate uniformly lowered cortisol levels. In that study, cortisol levels were “inappropriately” lower in those after etomidate compared to those with similar severity of illness scores who received alternate agents. There was increased mortality in those with very high clinical severity scores, but not in patients with lower severity scores. This suggested that etomidate induced partial adrenal insufficiency may increase mortality in those with greater severity of illness. We therefore undertook this evaluation in patients with sepsis who received etomidate, to question whether etomidate was associated with increased risk ratios (rr) and increased risk differences (rd) of mortality in association with higher underlying severity of illness.
Materials and Methods
Electronic search. An electronic literature search was performed on Pub Med, SCOPUS, and Cochrane Reviews for human studies, regardless of language, between 1983 (the earliest report on etomidate’s effect on adrenal function) and January 2020. All studies after 1983 used a single intravenous bolus etomidate dose of 0·3 mg/kg. The search strategy first started with keywords, “etomidate” and “adrenal” in Cochrane reviews. Four meta-analyses were found and the primary studies were combined and reviewed. 8,10 –12 Further search was performed using keywords: (“intensive care” or “critical care” or “intensive care unit”) and “etomidate” and (“adrenal insufficiency” or “glucocorticoid” or “corticosteroid”) (Figure 1). All primary comparator trials were included in the analysis if there was data on 28-day survival. Both authors reviewed electronic data search titles and abstracts to identify potential trials. Both reviewers extracted data, which were checked by the other reviewer.
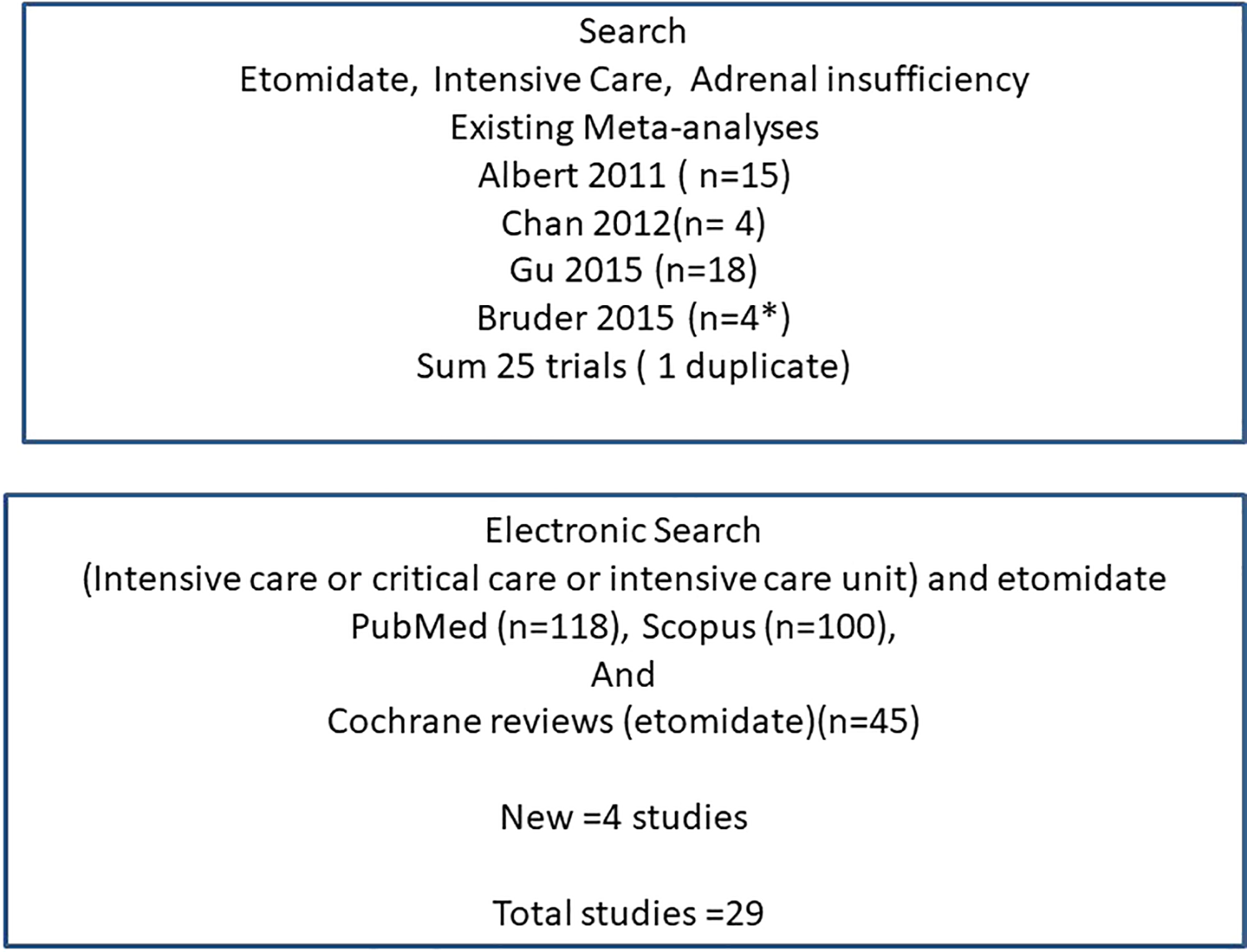
Search Criteria. Effects of etomidate in critical illness on adrenal insufficiency and 28 day survival.
Data Analyses
The primary outcome for the meta-analysis was 28-day all-cause mortality. Secondary outcome was the rate of adrenal insufficiency. Adrenal insufficiency was defined per the primary study author
Quality of Studies
Quality of studies was considered according to the PRISMA guidelines
19
Grade recommendations
20
and is included in
Meta-Analyses
Meta-analyses were performed for studies involving adults using the statistical program of Bax. 21,22 Heterogeneity of studies was calculated by I 2 where 0% to 30% is considered low heterogeneity and 30% to 60% may represent moderate heterogeneity. 23 Risk ratio (relative risk) and rate differences (rd) were performed using fixed effects model of Mantel-Haenszel for data considered to be of low and moderate heterogeneity. For data considered to have high degree of heterogeneity data was evaluated by random effects model of DerSimonian and Laird. Evidence of publication bias was assessed using funnel plots. 23
Statistical Analyses
Analyses of proportions were performed by the chi-square test (Statistica for Windows, V7.1 Stat Soft, Inc.2005, Tulsa, OK). Data are reported as weighted means ± standard deviation or 95% confidence intervals. Statistical significance is defined as a P < 0·05 by 2-tailed testing. Power calculation were performed for estimated frequencies. 24
Results
There were 29 trials (5 randomized controlled, 9 post hoc and 15 retrospective trials) in 8584 patients (5003 men, 3581 women) (mean age 61 ± 6 years) with critical illness in an ICU settings in which there were evaluations of mortality data of etomidate versus comparator anesthetic induction agents. The inclusion criteria for individual trials were sepsis in 20, critical illness in 6, trauma in 2 and emergency in 1 (see eTABLE 1 in the online data supplement).
Adrenal insufficiency was pre-defined in 14 trials (e TABLE 1) and occurred at a risk ratio (rr) = 1·54, 95%confidence interval (CI); 1·42, 1·67, p < 0·001, I 2 = 60%) (Figure 2). There was no apparent bias by funnel plot (see e Figure 1 in the online data supplement).
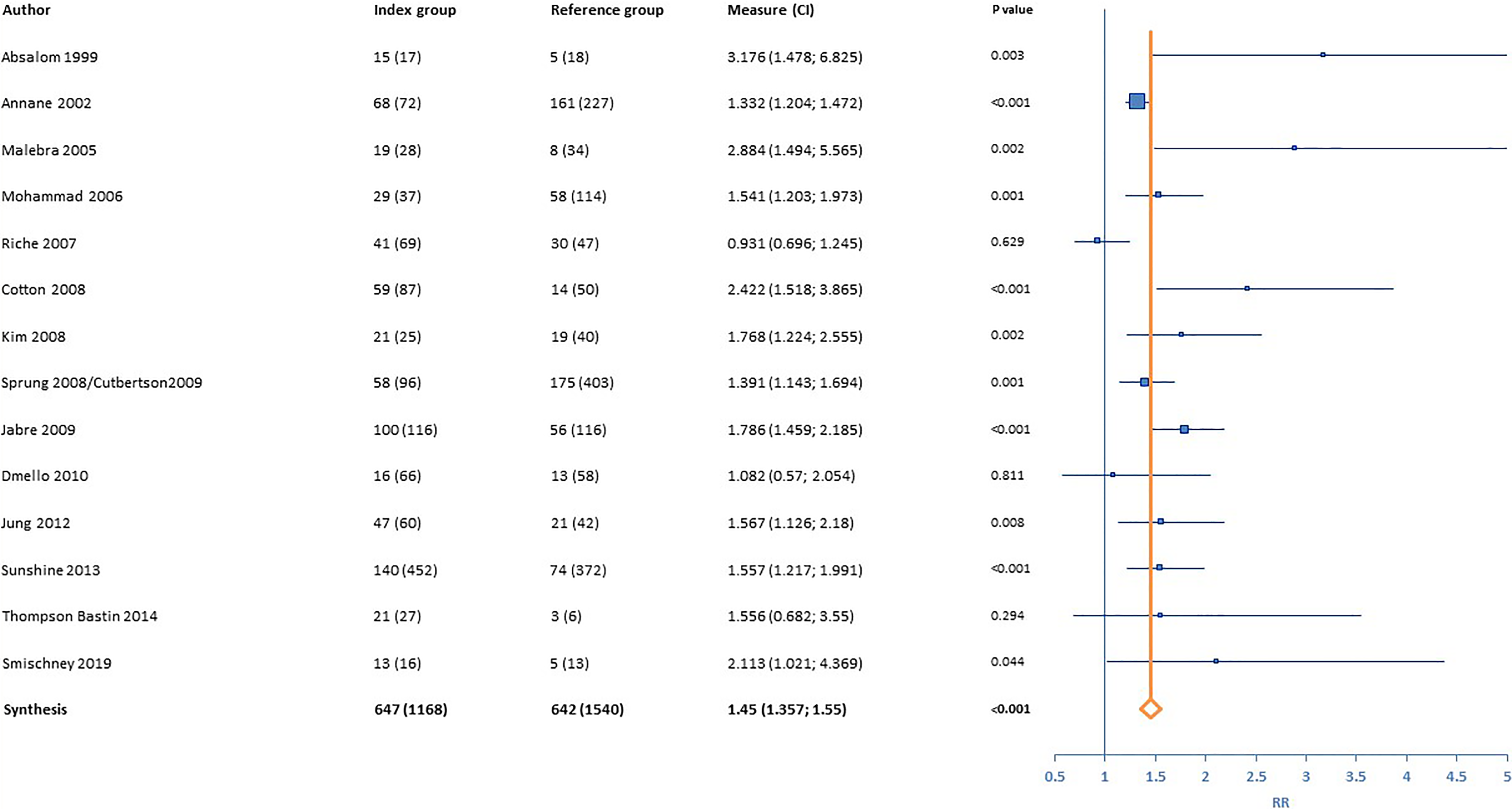
Forest plot of the risk ratio (RR) of the effects of etomidate on adrenal insufficiency (Fixed effects model, I 2 = 60%).
There was increased mortality overall in those who received etomidate (rr = 1·09 CI; 1·04;1·16, p = 0·001, I 2 = 48%) (Figure 3), without apparent trial bias by funnel plot (see eFIGURE 2 in the online data supplement).
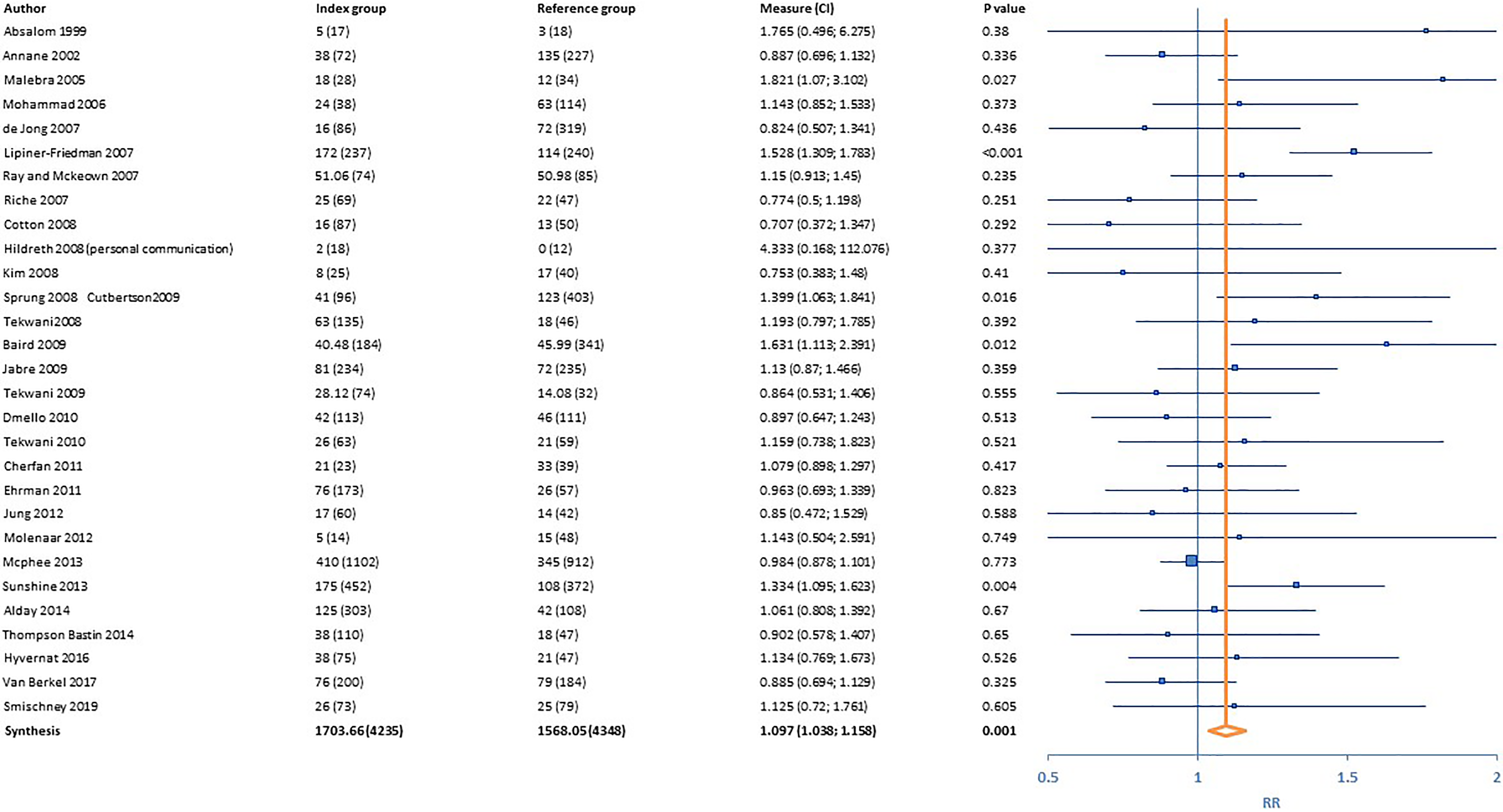
Forest plot of the risk ratio (RR) of the effects of etomidate on mortality. (Fixed effect, I 2 49%).
The effect of etomidate was further analyzed as to severity of illness by converting the specified severity scores (SAPS II, APACHE 2,3 or 4) to comparable predicted mortalities (e Table). Meta- regression showed that there was a progressive relative risk (rr) of mortality with the predefined predicted mortalities (Figure 4A). Similarly, meta regression showed that there was a direct correlation with etomidate of absolute risk difference (rd) and the number needed to harm (NNH = 1/rd) for mortality with the increasing severity of disease scores (Figure 4B). In this study population, we arbitrarily evaluated those above and below the median for predicted mortality (44%, which would be comparable to a SAPS II score of 49, and an APACHE 2 score of 22). There was a significant increase in relative rate of mortality in those receiving etomidate versus the controls in those with a predicted mortality >44% (rr = 1.20, CI;1.12,1.29, p < 0.001) and a significant relative difference (rd = 0.08, CI;0.05,0.11, p < 0.00001, NNH = 12.5). For those patients with predicted mortality less than 44%, there were no significant differences in relative rates (rr = 1.00, CI; 0.91,1.09, p = NS, rd = -0.001 Ci; -0.03,0.02, p = NS).
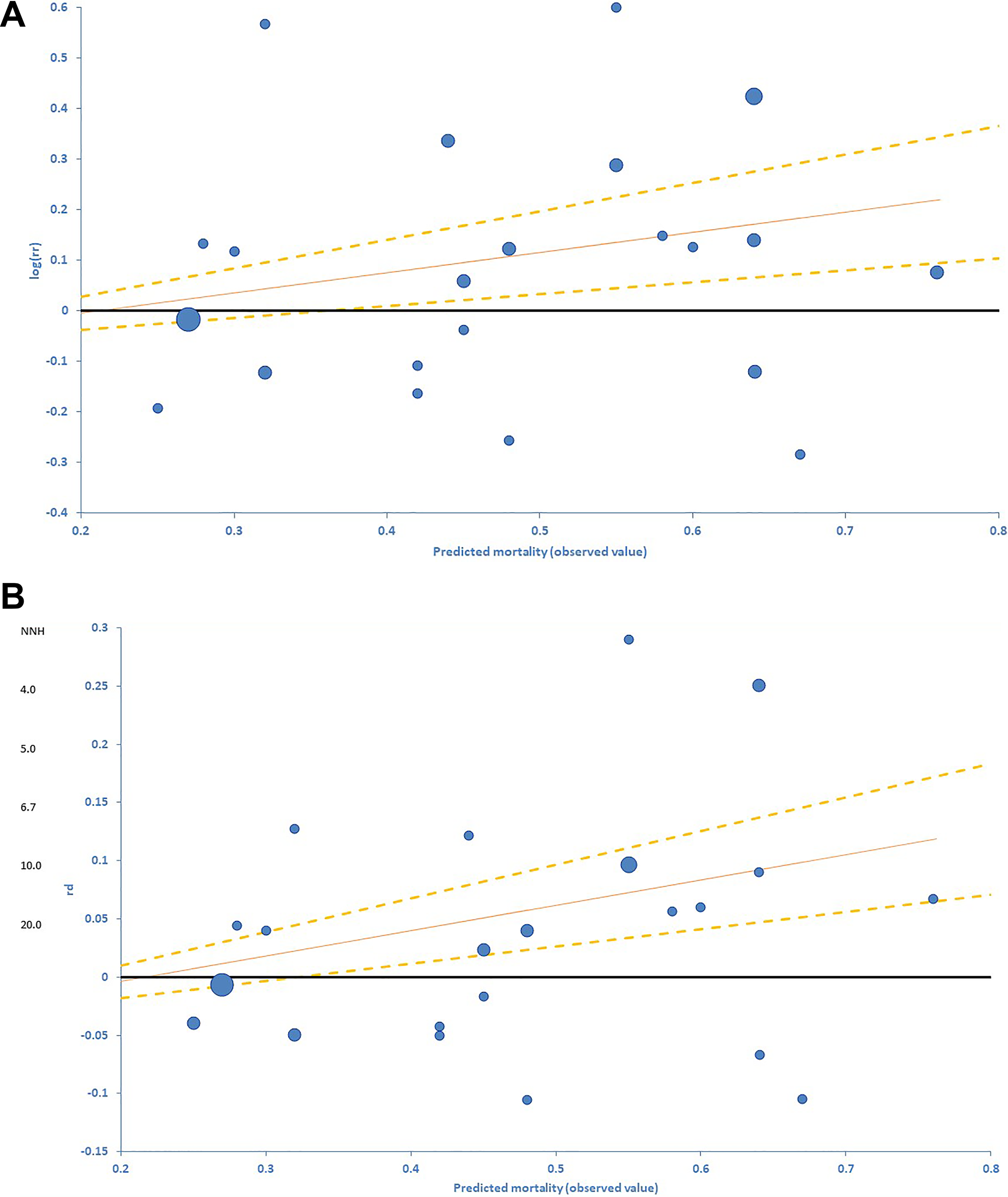
Meta-regressions of excess risk of mortality of etomidate over comparators with regard to predicted mortalities (derived from predefined scores of SAPS II, APACHE II, II or IV). A. Relative risk (RR) of etomidate versus comparators (Log (RR) = 0.40*predicted mortality-0.08, p = 0.01). B. Rate difference (RD) of etomidate versus comparators (RD = 0.22*predicted mortality-0.05, p < 0.002). NNH = number needed to harm). Size of circle is related to sample size. Shown are the regression line (solid line) ± SEM (dashed lines)
Discussion
Although it is accepted that etomidate causes adrenal insufficiency, there is controversy whether the adrenal insufficiency may be associated with a poorer outcome in critically ill patients in intensive care units. 8,10 –12 Etomidate has many benefits as the potential anesthetic induction agent of choice for rapid sequence intubation. 4 It is widely used without vascular compromise, and therefore physicians are reluctant to adjust for its use. Here we have addressed one of the paradoxes that although etomidate causes adrenal insufficiency it continues to be widely used. We believe that for the vast majority of patients undergoing intubation for elective procedures and those with a lower severity of illness score (i.e., predicted mortality <44%) etomidate may not cause clinically significant increase in mortality. However, in states of more extreme critical illness, such as with a predicted mortality >44%, there may be an increase of 20% in relative mortality and 8% in absolute mortality.
There have been extensive studies of corticosteroids as supplements to those with septic shock to reverse critical illness related corticosteroid insufficiency (CIRCI) 25,26 . In CIRCI, it is presumed that although the adrenal glands may produce corticosteroids, the intracellular levels are insufficient to prevent the inflammatory state and vascular collapse. 1,3 In this study, we took this concept further. Etomidate compromises adrenal function in most patients, which is associated with an increased mortality rate in those with a very high clinical illness score (e.g. predicted mortality >44%). The difference in outcome was due to an increase in the relative mortality rate with increase in severity of predicted mortality by regression analysis. The progressive increases in mortality rates were not just due to our ability to demonstrate significant changes in a population with baseline higher mortality rates.
There are limitations to this analysis. The primary studies were mostly moderate and low in Grade criteria (i.e., retrospective and post hoc studies), although they did encompass over 8000 patient comparisons. There is little data whether corticosteroids may alleviate this increase in mortality. From previous studies, adrenal insufficiency occurs within 3 to 6 hours and recovers from 12 to 24 hours 6 but the effect may persist for 48 to 72 hours 27,28 Three studies have compared clinical outcomes with the use of supplemental corticosteroids added to etomidate, and overall, there was no clinical benefit for the use of corticosteroids. In the 2 post hoc evaluations, the study by Annane 15 showed a benefit when subject had a SAPS score of 55 (± 10) and the steroids were administered within 7·33 (±3·5) hours, whereas there was no benefit in the Corticus trial 29 in those with a SAPS score of 49·5 (±18) in which the steroids were administered at a mean of 14 hours. In the randomized controlled trial by Payen, 14 corticosteroids were administered at 6 hours to a limited number of patients with a predetermined SAPS score of 44 without any clinical outcome difference.
With a relative increase in mortality rate of 20% overall above comparators (rr = 1·20, rd = 0.08), it would be difficult to perform an adequately powered study in a single center to evaluate whether corticosteroids added to etomidate would be protective. To design a prospective study, it is estimated that it would require both a specified inclusion of those with a predicted mortality score >44% and for these high risk individuals using approximations of rr = 1.20 or rd = 0.08, a power analysis suggests it would take 495 subjects in each group of etomidate vs comparators to demonstrate a statistical difference at an α = 0.05 and β = 0.8.
Conclusion
Etomidate causes partial adrenal insufficiency in most subjects studied. In those who are critically ill, with a predicted mortality >44% there is a higher relative mortality rate (20%) with etomidate versus comparator anesthetic induction agents. Rather than restrict etomidate use, there is evidence that adrenal insufficiency occurs within 3 to 6 hours after the dose and may last for 24 to 48 hours. Early institution of steroids may be protective. 30 Further trials of steroid supplementation with etomidate in high risk individuals are not in progress (as of August 18, 2020 ClinicalTrials.gov). Also, clarification of the effect of etomidate may not be forthcoming, as more recent prospective trials of corticosteroids in septic shock have specifically excluded patients receiving etomidate. 30,31 Although there were recommendations in 2008 to use corticosteroids in CIRCI, the use of corticosteroids in sepsis itself continues to be controversial. 1,17 It may be advisable that Intensivists should anticipate the need for physiologic “stress” glucocorticoid supplementation after etomidate bolus (i.e., hydrocortisone at 150-200 mg day and continuing for 2- 3 days of anticipated adrenal inhibition) in those with sepsis and a predicted mortality >44% (e.g., SAPS II score >49 or APACHE II score >22) and in those patients with acute deterioration of vital signs. There has been controversy over whether alternative anesthetic induction agents be considered in critically ill hemodynamically unstable patients. 32 Successful ICU intubation ultimately comes down to careful clinical judgment as to who and when, technical experience and skill and judicious use of anyone of a number of supplementary medications.
Supplemental Material
On_line_supplement - Etomidate, Adrenal Insufficiency and Mortality Associated With Severity of Illness: A Meta-Analysis
On_line_supplement for Etomidate, Adrenal Insufficiency and Mortality Associated With Severity of Illness: A Meta-Analysis by Stewart G. Albert and Sujata Sitaula in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.