
Abstract
Background:
Despite the increasing use of high flow nasal cannula oxygenation systems (HFNC) in clinical practice, little is known about its role in all cause respiratory failure as compared to traditional non-invasive ventilation (BiPAP). Furthermore, the effect of HFNC on mortality is unknown.
Methods:
We conducted a retrospective analysis of 49,853 patients with respiratory failure treated with non-invasive respiratory support (HFNC or BiPAP) and/or invasive mechanical ventilation (IMV) between 2017 and 2018.
Results:
Patients initially treated with HFNC who underwent subsequent intubation and IMV had a higher mortality rate as compared to patients who were initially treated with BiPAP and underwent subsequent intubation and IMV (34.8% vs 26.3%, p < 0.0001, OR 1.49, 95% CI 1.26,1.76). Patients first treated with HFNC who underwent subsequent intubation and IMV had a significantly increased mortality compared to patients who underwent immediate intubation and IMV (34.8% vs. 21.5%, p ≤ 0.0001, OR 1.94, 95% CI 1.67, 2.27). Stratified based on ICD-10 diagnosis, patients with a diagnosis of COPD exacerbation or heart failure treated with HFNC and subsequent intubation and IMV had higher mortality as compared to those treated with immediate IMV alone. This trend did not hold true for patients with a diagnosis of pneumonia.
Conclusion:
In a real-world retrospective analysis, use of HFNC was associated with increased mortality as compared to BiPAP and IMV alone. Further study is needed to confirm these associations.
Introduction
Acute respiratory failure results in greater than 2 million hospitalizations at a cost of nearly 55 billion dollars annually to the American health care system. 1 Patients with hypoxemic or hypercapnic respiratory failure that do not require emergent intubation are often treated with non-invasive respiratory support devices. Traditionally, non-invasive positive pressure ventilation (NiPPV) has been the first line treatment and literature supports its use in several disease specific states. NiPPV reduces mortality and rates of intubation in acute exacerbations of COPD and acute cardiogenic pulmonary edema. 2,3 However, the role of NiPPV in hypoxic respiratory failure not due to COPD or acute cardiogenic pulmonary edema is less clear, and its use has been associated with increased rates of failure and resultant intubation as well as increased mortality in these populations. 4 Despite these concerning negative associations, NiPPV plays an ever-increasing role in the management of acute respiratory failure.
Over the past decade, high flow nasal cannula oxygenation systems (HFNC) have emerged as an accepted alternative form of non-invasive respiratory support during acute respiratory failure. By delivering heated and humidified oxygen at high flow rates, these devices reduce dead space, increase end-expiratory lung volume, and create flow-dependent positive pharyngeal pressure, in turn reducing work of breathing and improving patient comfort and tolerance. 5 –8
The FLORALI trial published in 2015 showed a significant reduction in 90-day mortality with HFNC when compared to NiPPV and conventional oxygen in patients with non-cardiogenic acute hypoxic respiratory failure. 9 Several other studies limited by small sample sizes and short-term endpoints suggest HFNC may be effective for all forms of respiratory failure including COPD exacerbations and heart failure. 10,11 Despite the relative weak evidence supporting HFNC use outside of non-cardiogenic acute hypoxic respiratory failure, it is increasingly used in patients with alternative etiologies of respiratory failure such as COPD exacerbation. 12 Little is known regarding the real-world use of HFNC. In the United States, HFNC has no Current Procedural Terminology (CPT) code which limits population-based analyses. In this report, we present the largest retrospective analysis of HFNC for acute respiratory failure outside of a clinical trial setting.
Methods
We conducted a retrospective analysis at a large medical system in the United States from January of 2017 through December or 2018. All patients that required HFNC, NiPPV (BiPAP or CPAP), or IMV were included. Our hospital system utilizes 2 HFNC systems, the Precision Flow by Vapotherm™ and Optiflo by Fisher and Paykel. Using time stamps in the electronic chart, we identified patients that used HFNC or BiPAP/CPAP in isolation (alone) and prior to intubation and IMV. We then determined in-hospital mortality rates for these groups.
Next we stratified patients with respiratory failure based on common diagnoses of acute respiratory failure—pneumonia, COPD, and heart failure—based on ICD-10 codes. We compared mortality rates in these groups between patients first treated with HFNC who underwent subsequent intubation and IMV and patients with the same diagnoses treated with IMV alone.
We used Pearson’s chi square test of independence and calculated odds ratio with 95% confidence intervals. This project was determined by the University of Arizona and Banner Health to represent quality improvement and was exempt from IRB review.
Results
Between January of 2017 and December of 2018, we identified 32,761 patients in our medical system with respiratory failure treated with non-invasive respiratory support. Use of HFNC increased by 28.1% from 2017 to 2018. While BiPAP/CPAP use also increased, the rate was notably lower (9.2%). We also identified 17,092 patients with respiratory failure who underwent immediate intubation and IMV. Patient age between the 2 groups treated with non-invasive support were similar, however patients intubated immediately tended to be younger. Average hospital length of stay differed between groups with a trend toward increased ICU length of stay and hospital length of stay in patients that used HFNC either alone or in combination with IMV (see Table 1).
Average Age and Hospital Length of Stay for Patients With Respiratory Failure Based on Treatment Group.

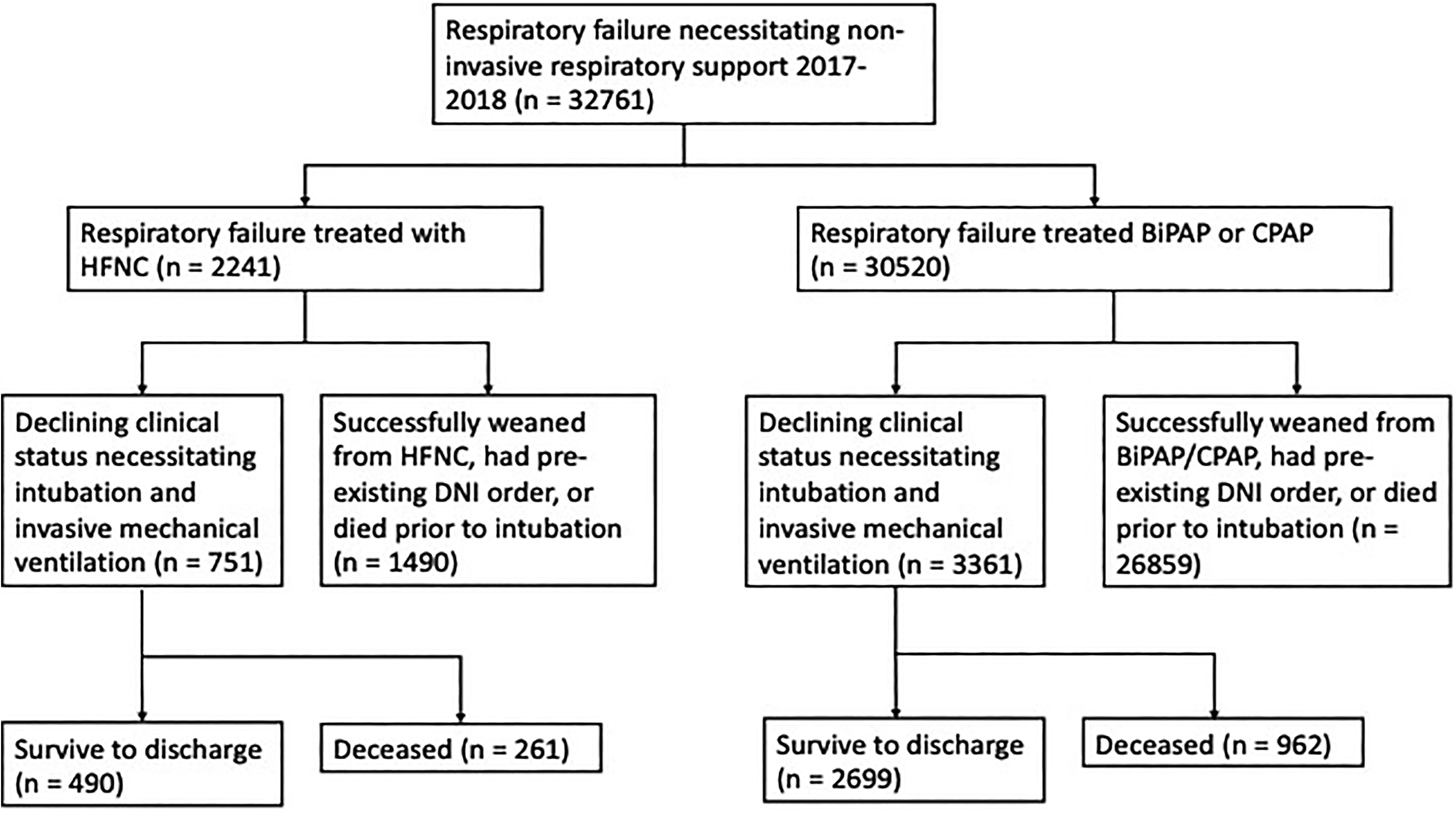
Of 32,761 patients with respiratory failure treated with non-invasive respiratory support, 2241 (6.8%) were treated with HFNC and 30,520 (93.2%) were treated with traditional NiPPV (BiPAP and/or CPAP). Of the HFNC patients, 1490 used HFNC alone and 751 were subsequently intubated and started on IMV. Of the BiPAP/CPAP patients, 26859 used BiPAP/CPAP alone and 3361 were subsequently intubated and started on IMV (Figure 1).
Trends in non-invasive respiratory support from January 2017 to December 2018.
Patients initially treated with HFNC that underwent subsequent intubation and IMV had a higher mortality rate as compared to patients who were initially treated with BiPAP and underwent subsequent intubation and IMV (34.8% vs 26.3%, p < 0.0001, OR 1.49, 95%CI 1.26, 1.76). Patients first treated with HFNC who underwent subsequent intubation and IMV had a significantly increased mortality compared to patients who underwent immediate intubation and IMV (34.8% vs. 21.5%, p < 0.0001, OR 1.94, 95% CI 1.67, 2.27) (Table 2).
In Hospital Mortality of Patients Treated With HFNC Followed by Intubation and IMV as Compared to BiPAP Followed by Intubation and IMV.a

a Pierson Chi square test of independence p-values and associated odds ratio of in-hospital death.
When stratified based on primary diagnosis responsible for acute respiratory failure, patients with COPD or heart failure had higher mortality rates if treated with HFNC before subsequent intubation and IMV as compared to immediate intubation and IMV (COPD: 36.5% vs. 23.9%, p < 0.01, OR 1.8, 95% CI 1.16, 2.98; Heart Failure: 42.53% vs. 30.76%, p = 0.02, OR 1.6, 95% CI 1.08, 2.58). Mortality rates were not significantly different in patients with pneumonia first treated with HFNC before subsequent intubation and IMV as compared to immediate intubation and IMV (25.22% vs. 19.52%, p = 0.138, OR 1.39, 95% CI 0.9, 2.15) (Table 3).
HFNC Followed by IMV and IMV Mortality Stratified by Diagnosis.a
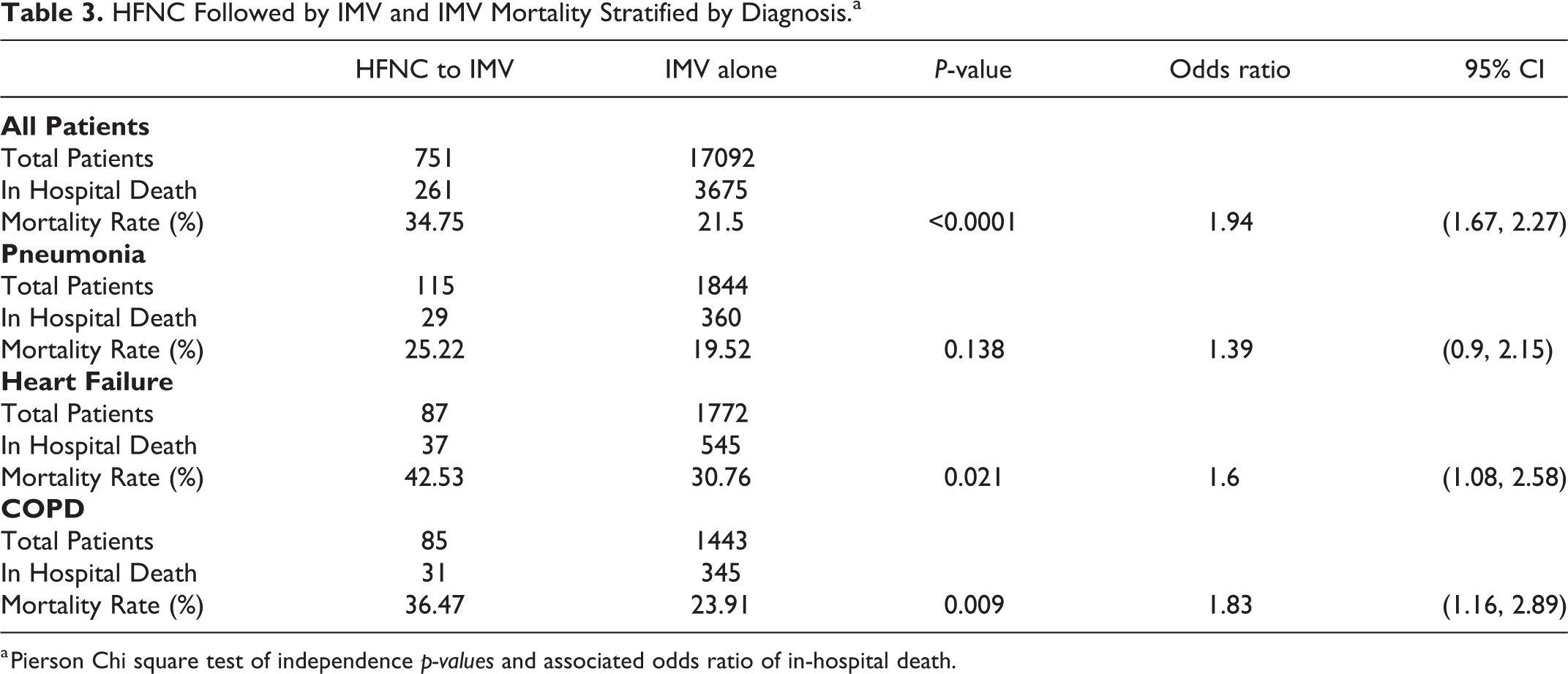
a Pierson Chi square test of independence p-values and associated odds ratio of in-hospital death.
Discussion
Over a 2-year period, there was a 28% increase in HFNC use in our medical system. Our finding is similar to a smaller prior study conducted from 2008-2014 at a single center in Massachusetts where HFNC usage increased faster than other forms of non-invasive ventilation. 12 To our knowledge, this is the largest analysis of HFNC use to date. Banner is one of the largest non-profit medical systems in the United States, comprising 28 hospitals across 6 states. The hospitals include community hospitals, subspecialty focused hospitals, and 3 academic medical centers.
Increased provider awareness of HFNC, reported improved patient comfort and tolerance of HFNC, and general ease of use as compared to BiPAP may have led to increased implementation of the technology. While it is possible that more HFNC units were purchased across the medical system relative to NiPPV systems during the time of our analysis, we do not have access to confirmatory data to support this. Even if more units were purchased, the increase in use itself may have dictated purchasing.
Our finding that patients who failed HFNC and underwent intubation and IMV had higher mortality rates than those who failed BiPAP and underwent intubation and IMV was unexpected. On the surface this seems contrary to the results of FLORALI trial (9). However, our population included all types of respiratory failure rather than only non-cardiogenic acute hypoxic respiratory failure as was the case in the FLORALI study patients. Our population reflects the real-world application of non-invasive respiratory support with HFNC and BiPAP/CPAP before intubation. Given the minimal evidence guiding the use of HFNC, it is possible that this therapy is inappropriately used in certain types of respiratory failure.
In patients with a diagnosis of pneumonia without concurrent heart failure or COPD, a population that could be inferred to have non-cardiogenic AHRF, our results were similar to the FLORALI results; we found no significant difference in mortality rates between these groups. In patients with only COPD or only heart failure as the etiology of respiratory failure—2 populations with limited evidence supporting the use of HFNC and relatively strong evidence favoring NiPPV 2,3 —in hospital mortality was greater in those treated with HFNC and subsequent intubation compared to those undergoing immediate intubation and IMV. These results are similar to a small, retrospective, propensity matched study that found a trend toward increased mortality in patients treated with HFNC > 48 hours who underwent subsequent intubation and IMV as compared to patients that were intubated earlier. 13
The trend toward increased mortality in patients treated with HFNC is concerning. One possible explanation is that practitioners are not yet fully informed as to the best candidate for HFNC use. Based on current prospective studies, it would seem at least equivalent to NiPPV in non-cardiogenic acute hypoxemic respiratory failure. 9 However, weaker evidence that supports a role for HFNC in hypercarbic and hypoxic respiratory failure from cardiogenic etiologies and increasing provider familiarity and comfort with HFNC may lead to incorrect application of the device. Further studies and unified guidelines for the use of HFNC are needed to help determine HFNC responders and non-responders a priori. A recent study suggested the ROX score ([SaO2/FiO2]/Respiratory Rate) >4.88 at hour 12 of HFNC use as a predictor of HFNC success, however this is not yet routinely used in clinical practice. 14 Finally, it is also possible that patients initially treated with HFNC had diagnoses with associated high morbidity and mortality such as end stage lung disease. In these cases, HFNC may have been used as a means to avoid or delay intubation and IMV given the perceived high risk of death with invasive mechanical ventilation though we were not able to assess for this based on our data.
Our data has several noteworthy limitations. First, it is retrospective, reliant on charted documentation and coded ICD-10 diagnoses without internal chart review. Second, we were unable to adjust for important covariates that could bias our results such as age, APACHE scores, and comorbidities. However, despite our inability to adjust for covariates and confounders, given the overall population size and the unexpected mortality trends, the results are important and can lead to significant hypothesis generation for future research.
Conclusion
The use of HFNC is increasing rapidly in our medical system and there is a trend toward increased mortality in patients that fail HFNC and are intubated. The absence of clear usage guidelines or solid evidence in the literature regarding ideal responders to HFNC may lead to misapplication of HFNC and potential patient harm. Further research is needed to guide future use of this technology.
Footnotes
Abbreviations
Authors’ Note
DM, DK, and CB were responsible for study concept and design. JP was responsible for data acquisition and analysis. DM and CB drafted the work. DM takes responsibility for the content of the manuscript, including the data and analysis. All authors revised and approved of the final submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institutes of Health with grant id T32 HL007249 (DM) and K08 HL141623 (CB).