
Abstract
Purpose:
Montefiore Medical Center (MMC) in the Bronx, New York, was subjected to an unprecedented surge of critically ill patients with COVID-19 disease during the initial outbreak of the pandemic in New York State in the spring of 2020. It is important to describe our experience in order to assist hospitals in other areas of the country that may soon be subjected to similar surges.
Materials and Methods:
We retrospectively reviewed the expansion of critical care medicine services at Montefiore during the COVID-19 surge in terms of space, staff, stuff, and systems. In addition, we report on a debriefing session held with a multidisciplinary group of frontline CCM providers at Montefiore.
Findings:
The surge of critically ill patients from COVID-19 disease necessitated a tripling of critical care bed capacity at (MMC), with attendant increased needs for staffing, equipment, and systematic innovations to increase efficiency and effectiveness. Feedback from a multidisciplinary group of frontline providers revealed multiple opportunities for improvement for the next potential surge at MMC as well as guidance for other hospitals.
Conclusions:
Given increasing cases and burden of critical illness from COVID-19 across the US, engineering safe and effective expansions of critical care capacity will be crucial. We hope that our description of what worked and what did not at MMC will help guide other hospitals in their pandemic preparedness.
Introduction
As of September 10, 2020, the COVID-19 pandemic caused by the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) has devastated the world with over 27 million cases including 6,365,595 cases and 190,909 deaths in the United States. 1 New York State has been the most severely affected with 44,1154 cases (7%) and 33,019 (17%) fatalities. 2 Since 12%-33% of hospitalized patients have required mechanical ventilation or ICU admission, 3 –5 expansion of critical care medicine (CCM) services is crucial in responding to this pandemic.
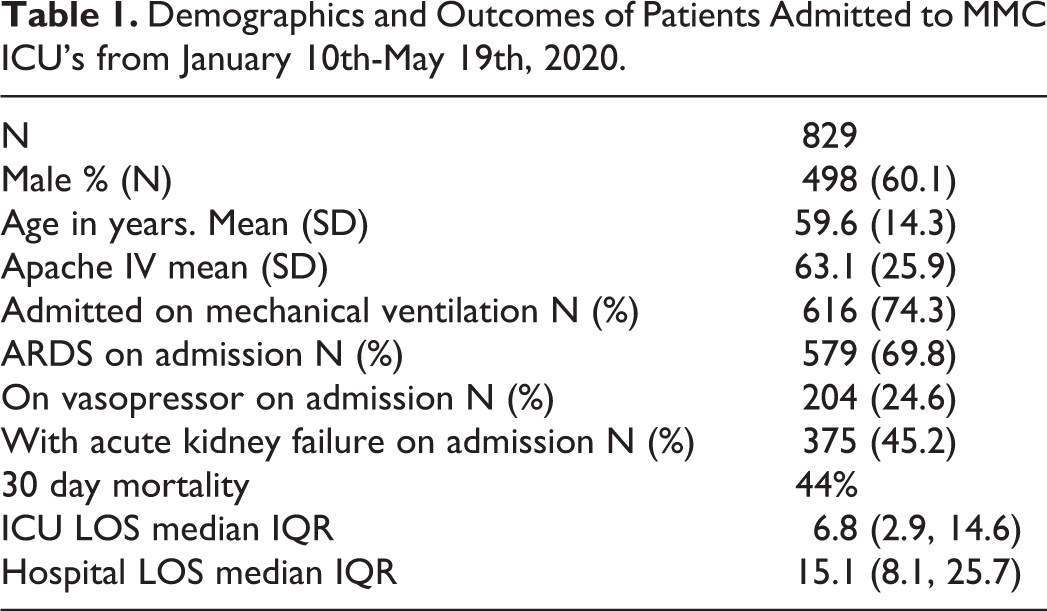
Within New York City, the Bronx was among the most heavily affected by the initial COVID-19 surge in the Spring of 2020 (Figure 1). Montefiore Medical Center (MMC) is the largest medical center serving the Bronx and consists of 4 hospitals: the Moses, Children’s Hospital at Montefiore (CHAM), Weiler, and Wakefield divisions. The demographics and outcomes of the patients admitted during this surge are summarized in Table 1. In this report, we have two aims. The first is to describe the implementation of MMC’s critical care response to the COVID-19 pandemic within the framework of the 4S’s: Space, Staff, Supplies and System. 6 The second is to report on the results from a debriefing session held with a multidisciplinary group of frontline CCM providers. This session occurred over a 90-minute period on June 3, 2020. 50 practitioners directly involved in the critical care response took place in this debriefing. These providers included critical care providers (attendings, fellows and physician assistants) and representatives from nursing, pharmacy, physical medicine and rehabilitation, pediatric critical care, nephrology, respiratory therapy, and non-critical care physicians who were called for deployment in the ICU (non-critical care anesthesiologists, cardiologists, and surgeons). A transcript of the debriefing session with all comments categorized by theme is provided in the supplementary material. With our report, we hope to provide a better understanding of the key aspects of preparing for and implementing a response to future surges of COVID-19.
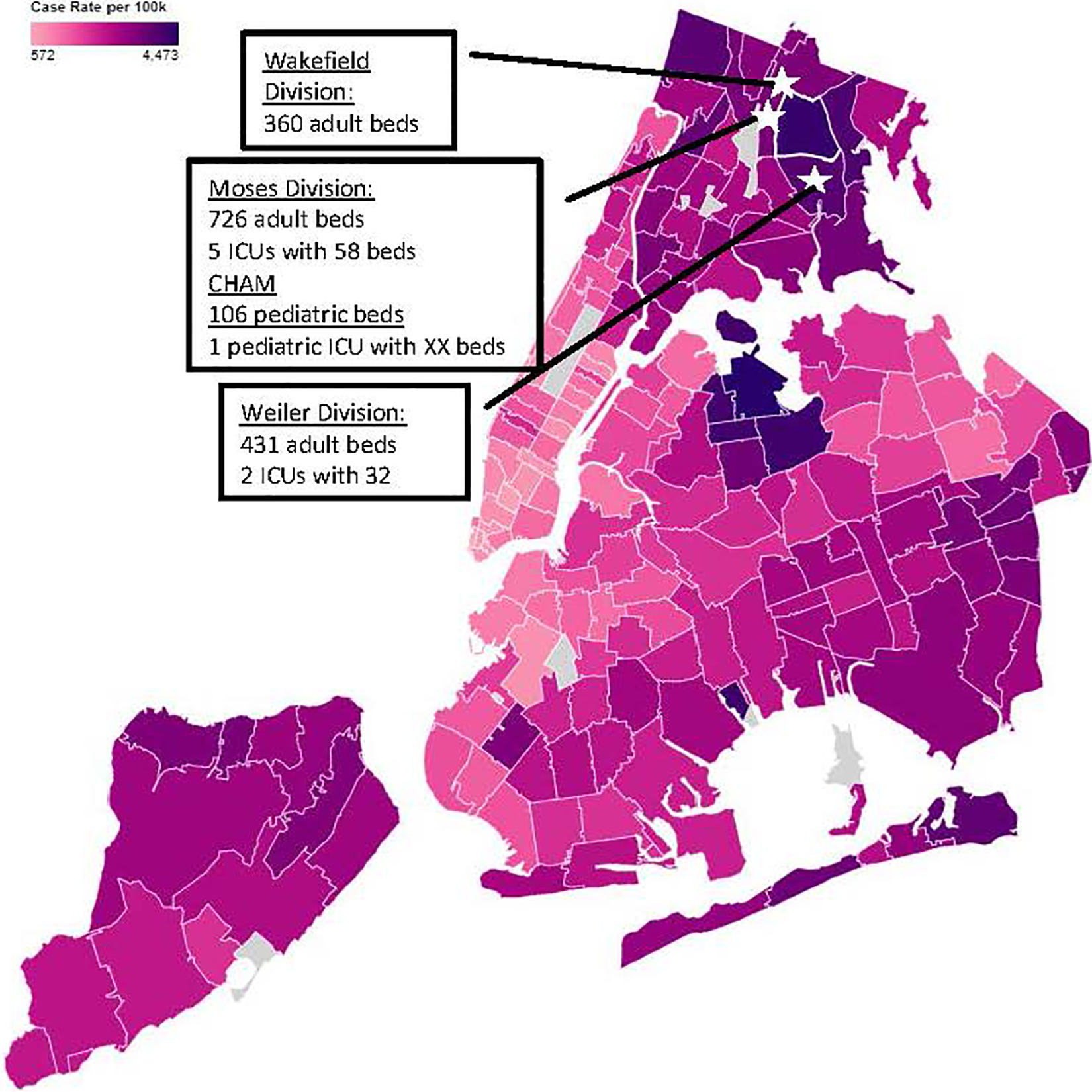
NYC COVID-19 case rate.
Demographics and Outcomes of Patients Admitted to MMC ICU’s from January 10th-May 19th, 2020.
Pre-Pandemic State
Prior to the pandemic, the unified Division of Critical Care Medicine in the Department of Medicine consisted of 49 full time and part time board-certified critical care physicians, 4 medical hospitalists, 21 critical care fellows and 41 critical care physician assistants (PAs). All intensivists hold one or more additional board certification in internal medicine, anesthesiology, surgery, neurology, neurocritical care, pulmonary medicine, palliative care medicine, infectious disease, or nephrology. Working in 12.5 hour shifts, the CCM physicians provide 24/7 coverage for 6 intensive care units (ICUs), including medical, surgical, neuroscience, and cardiothoracic ICUs and 3 intermediate care units. In addition, CCM provides a 24/7 in-house CCM Consult team that responds to all consults for ICU admission, cardiac arrests, rapid response calls and requests for procedural assistance in all areas of each hospital. All intubations outside of the Emergency Department, operating rooms and Post-Anesthesia Care Unit (PACU) are performed by CCM. The Cardiac Care Units are staffed by cardiologists. The Chief of the Division of Critical Care Medicine is also the Chief of the Division of Pulmonary Medicine at MMC. The Pulmonary Division consists of 16 physicians, 9 of whom are board certified in critical care and attend in the medical ICUs and the CCM Consult service.
Space
CCM Bed Capacity Expansion
Preparation for COVID-19 started in late January when the Hospital Incident Command System was activated (Figure 2). In early February, CCM convened a COVID-19 Leadership Committee to plan the CCM response. The first COVID-19 patient was admitted to the ICU at MMC on March 10 and hospital admissions of COVID-19 patients soon increased exponentially (Figure 3A). Within 2 days of the New York Governor’s order to increase hospital bed capacity by at least 50%, addition of ICU beds began (Figure 3B). Consideration for conversion to ICUs was first given to units with existing equipment for continuous monitoring and those with capacity to deliver high intensity critical care interventions such as ECMO and continuous renal replacement therapy (RRT). The Cardiac Care Unit, Cardiac Catheterization Lab, Procedural Units and Pediatric ICU at CHAM, were turned into adult COVID-19 ICUs. Other units with monitoring capacity but without ability to do ECMO and RRT were then added including the pediatric infusion unit and the PACU in an ambulatory surgery building. ICUs with no doors or walls were used to hold COVID-19 negative patients. All existing intermediate care and telemetry units were converted to ICUs. Additional monitors were purchased or repurposed from PACUs. When feasible, infusion pumps and ventilator monitors were positioned outside of rooms to allow rapid adjustments while minimizing practitioner exposure and conserving personal protective equipment.
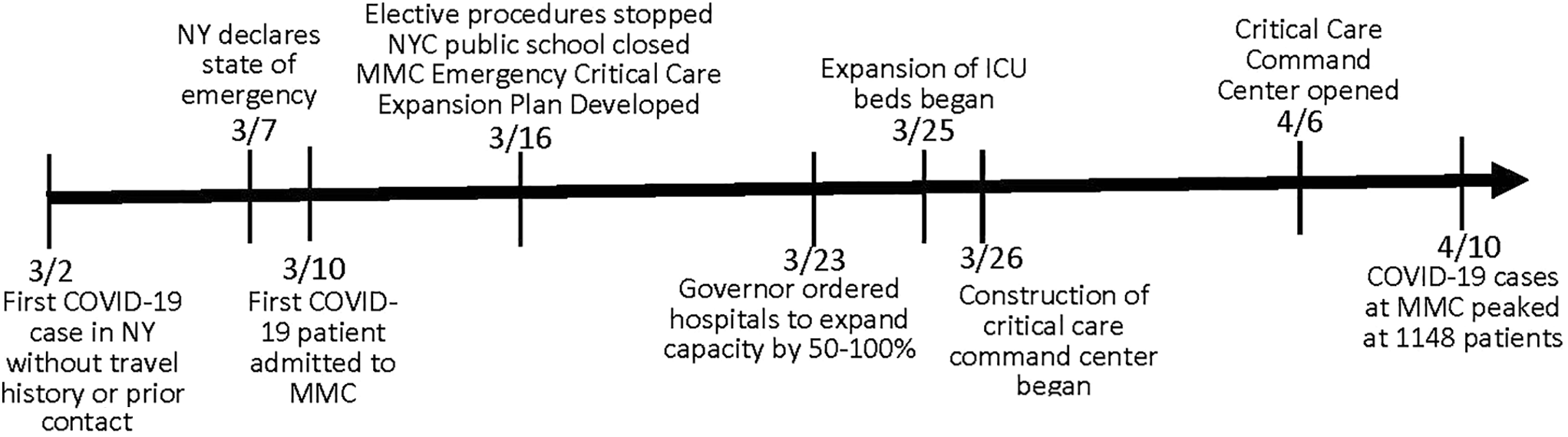
Timeline of Montefiore Medical Center response to COVID-19 surge.
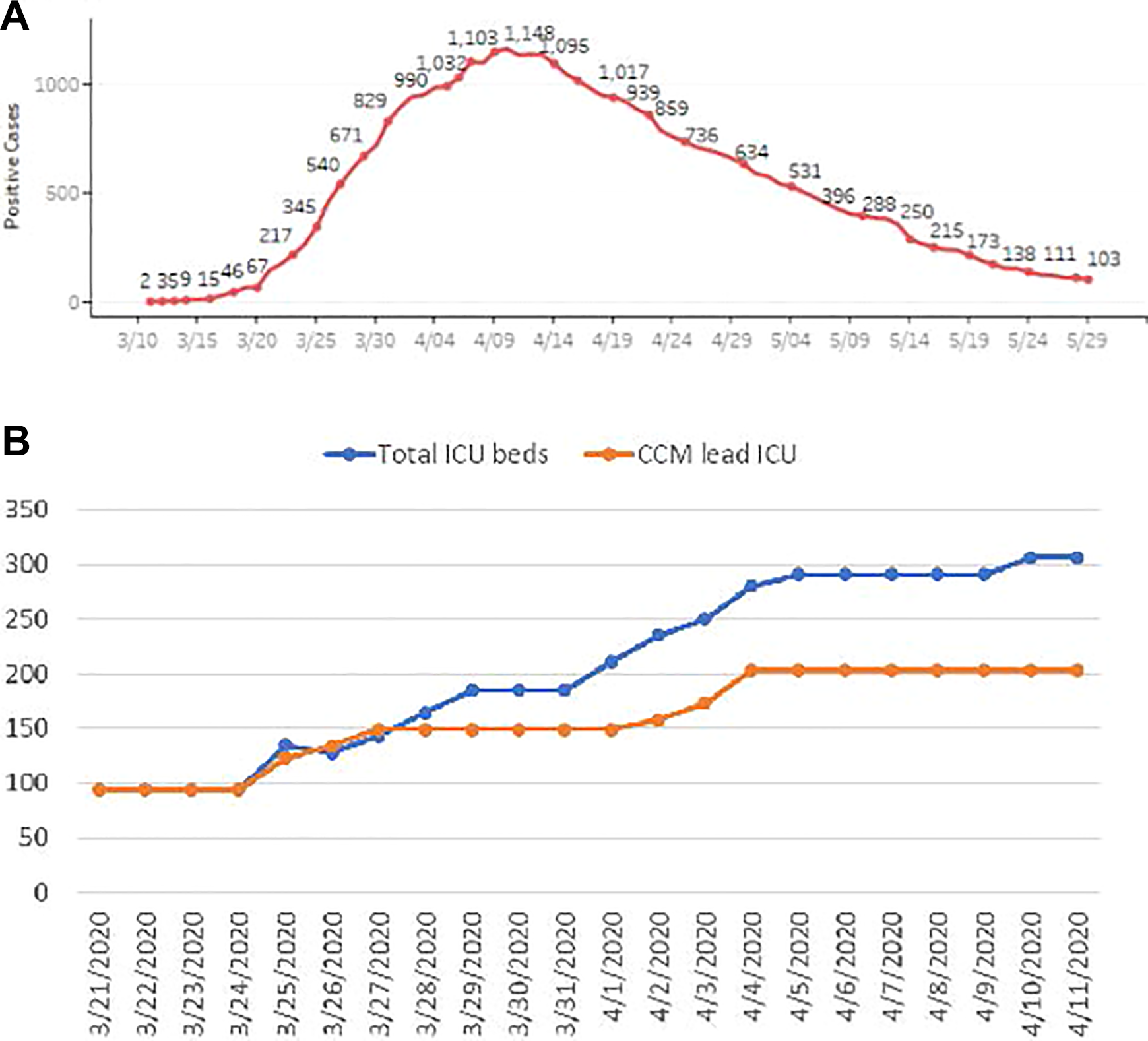
MMC critical care bed expansion during COVID-19 surge.
Engineering converted all possible ICU rooms to negative pressure. Windows were inserted into doors or walls for better visualization of patients. At the peak of the pandemic at MMC on April 10, ICU capacity was increased from a baseline of 106 to 306 adult ICU beds including 285 beds for COVID-19 positive patients and 21 beds for COVID-19 negative patients (Figure 3B).
Feedback on CCM Bed Capacity Expansion
During the debriefing session, the most common challenge mentioned was the inherent limitations of working in units that were not originally designed as ICUs (Supplemental Table). As many participants indicated, some units lacked central monitoring stations so “…the nurses (had) to stay in the rooms a lot for a long period of time.” The pediatric infusion unit could not accommodate adult hospital beds. Stretchers were used and increased skin breakdown was observed. In addition, some of the expanded ICU’s were in locations that were far from essential services such as the laboratory and pharmacy. Also, some areas were converted and opened in such a rapid fashion that some critical supplies were not initially available, especially in those ICUs that had not cared for inpatients in the past.
Staff
CCM Staffing Expansion
Staffing the expanded ICUs was challenging and was made more difficult due to the high rate of COVID-19 disease acquisition by providers with resultant furlough periods. In total 1561 associates at MMC were furloughed including 37% of CCM physician and physician assistant staff. To staff the expanded ICUs, clinical time for all CCM practitioners was increased. Four locum tenens, three volunteer, and two per diem attending intensivists were recruited and assisted with our response. CCM served as the primary physician staffing for 203 (66%) of the total ICU beds during the pandemic (Figure 3B). In addition, CCM served as consulting physicians and critical care back up for all other areas of the hospital.
Certified registered nurse anesthetists (CRNAs), operating room and PACU nurses, nurse practitioners, and experienced ICU nurses were deployed to the new ICUs. Cardiac perfusionists were re-trained and deployed to assist with RRT. Echocardiology technicians were trained to support respiratory therapists with transport and cleaning of equipment, allowing respiratory therapists to concentrate on bedside care. Physical and occupational therapists were trained and redeployed as a patient proning team.
In addition to a need for CCM staffing of the expanded ICUs, daily numbers of rapid response calls, intubations and cardiac arrests greatly increased with as many as 25 emergent intubations performed outside of the ICUs on some days. (Figure 4). Because of multiple simultaneous emergencies, additional intensivists and CRNAs were added to the Critical Care Consult Service.
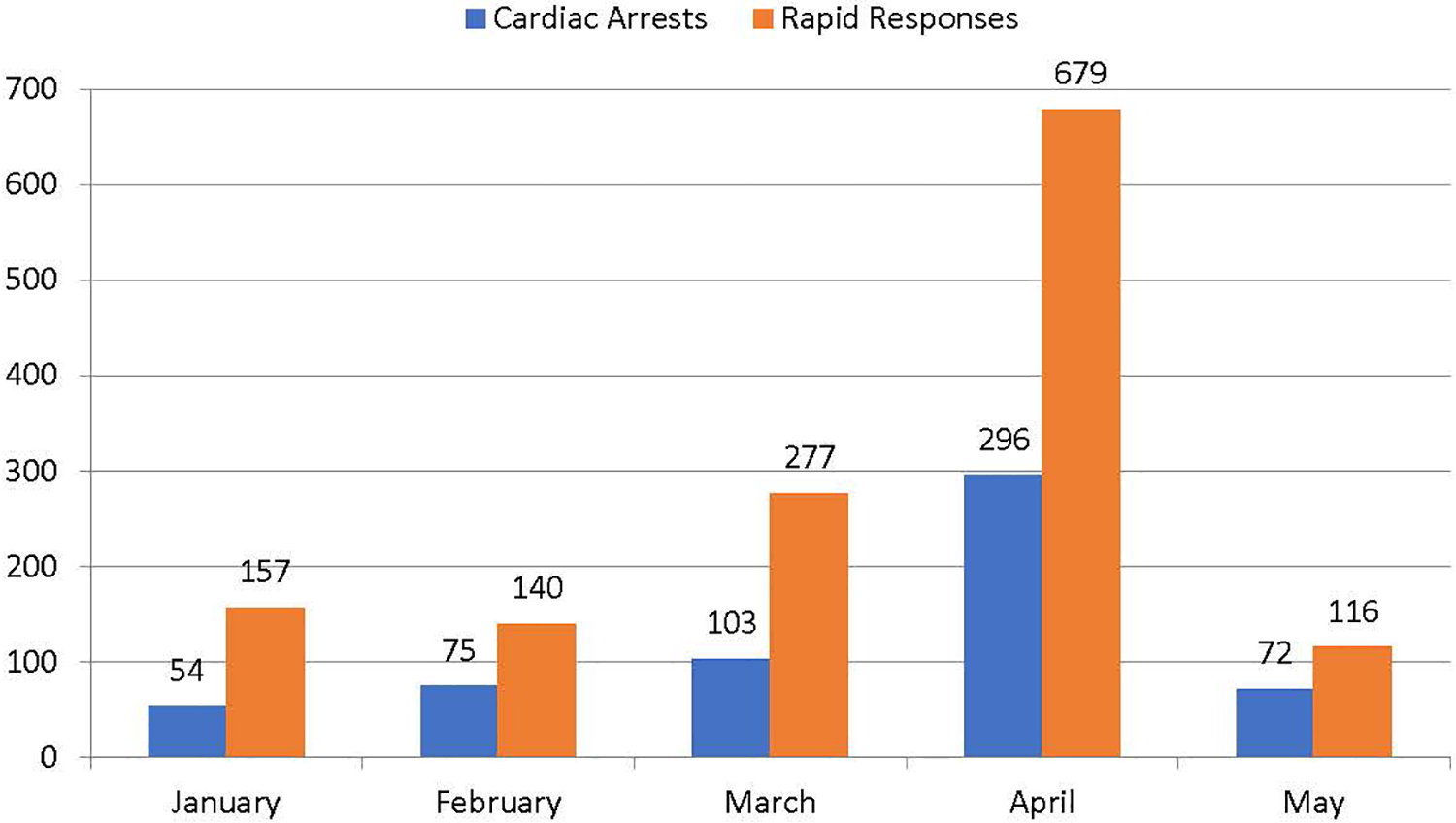
Monthly counts of cardiac arrests and rapid response emergencies.
Feedback on CCM Staffing Expansion
Participating practitioners felt staffing of expanded critical care services was particularly challenging. Even with increased staffing, many felt that they were stressed by the sheer volume and acuity of disease. One participant said that “…during the peak week we were hitting double digits in both consults and intubations. And it was like physically not possible to be in two places at once.” One participant stated, “If you are going to understaff [the ICU] on the physician level you’ve got to have experienced nurses, or vice versa.” One nursing leader indicated that they “…tried to do a little bit of mixing by, you know, half the staff from (an expanded ICU) mixed with half the staff from (an existing) ICU. But that really left everyone thin.” Another said, “There were days when I think I had two to three nurses for 16 patients. So, we couldn’t send our nurses over to the other units, (as) was mentioned earlier, because we just didn’t have the staff.” Similarly, deployment of physical therapists to the proning team helped facilitate proning but reduced ability for early mobilization in the ICU. Recruitment agencies were used to expand the pool of ICU nurses and respiratory therapists but not in time to be available at the peak.
Particularly in units in which intensivists served as consultants rather than as the primary providers, some noted that the roles of each member on the team was not always clearly defined. The result was that in “Every place its own sort of culture developed very quickly in a few weeks. And I think that led to a lot of significant loss of consistency within the system.”
Supplies
Augmentation of Resources
Based upon inventory assessments, augmentation of supplies like video laryngoscopes, intraosseous catheters, and handheld ultrasound machines was started prior to admission of our first COVID-19 patient. Orders were placed for new ventilators and high flow nasal cannulas (HFNCs) but delivery was delayed due to high demand. Phillips V60 BIPAP machines were repurposed to serve as mechanical ventilators for intubated patients. Anesthesia machines were used as ventilators in PACUs and OR’s. 210 Vyaire portable Long Term Ventilators (LTVs) were received from the national stockpile. Despite this, in late March there were less than ten ventilators available in each site on some days. Overall, the number of ventilators in the MMC hospitals were increased from 160 at baseline to 420.
Acute kidney injury was present in 45% of our ICU COVID-19 patients with 26% requiring RRT. Patients were frequently assessed and prioritized for dialysis. Access to RRT was limited by lack of dialysis nurses and machines as well as inadequate plumbing in some units. Additional dialysis machines were purchased, and acute peritoneal dialysis was used in some patients. Outpatient dialysis patients were relocated to another site to allow the dialysis nurses to concentrate on in-patient needs.
Feedback on Augmentation of Resources
Much of the feedback during the debriefing session centered around the inadequacies of the LTVs, repurposed V60 s, and anesthesia ventilators to manage patients with ARDS. Respondents indicated that anesthesia ventilators were “not made for these long-term ventilation scenarios.” Another participant said, “Those (LTV) vents were horrible. We couldn’t tell whether or not the patient got disconnected. There were no alarms on those vents.” Acute peritoneal dialysis was felt to be lifesaving in some patients, but overall less effective than hemodialysis.
Providers reported difficulties with acquiring supplies needed to respond to multiple emergent intubations. Pre-labeled syringes for emergent intubation and IV pumps for sedation of patients intubated on the floors were found to be lacking. Also, due to the sheer volume of emergent intubations, some key components of the airway trays were lacking during the peak days.
Systems
The Critical Care Command Center (CCCC)
Given the expanded ICUs and increased demand for critical care expertise, a Critical Care Command Center (CCCC) was rapidly constructed and staffed with a critical care attending 24/7. The CCCC consisted of 6 computer consoles adequately spaced to allow for social distancing. Dedicated phone lines to each campus were set up for direct access to a CCM physician from anywhere in the system. On request, the CCCC physician rounded remotely in all non-CCM run units. Bedside monitor data and waveforms from units from units with remote capabilities were streamed in real time to the CCCC. In addition, portable monitors that could be viewed in the CCCC were placed on critically ill patients in non-monitored settings. Because radiologic imaging was limited, CCM provided increased point of care ultrasound exams which were uploaded to qPath-- a cloud-based image repository-- and reviewed by CCM faculty in the CCCC .
The CCCC also served to triage ICU beds and critical resources. Requests for transfers from outside hospitals were directed through the CCCC who determined bed availability and stability for transport. The CCCC organized all ICU to ICU transfers when patients needed interventions such as ECMO or RRT that could not be delivered in their unit. When other critical care resources like HFNC became limited, applications of HFNC outside of the ICU required CCCC approval and follow up. A dashboard of HFNC and ventilator use was created to allow for CCM and pulmonary consultants to ensure appropriate utilization and readiness for weaning.
Standardization of Care and Clinical Protocols
Given the limited but rapidly evolving literature on the treatment of severe COVID-19 disease, standardization of evidence-based care across critical care units during the pandemic was challenging. Guidelines were created to standardize infection control practices during high-risk procedures such as intubation, cardiopulmonary resuscitation (CPR), and ventilator maintenance. These were stored on a shared online folder and providers received daily updates from the Leadership Committee. Although clinical protocols were established by other sub-specialty services at MMC for COVID, they were altered frequently. For example, initially hydroxychloroquine and lopinavir/ritonavir were recommended as treatments for severe COVID-19, but these were quickly revised given concerns about their effectiveness and potential harm. 7,8 Given the lack of a solid evidence base, CCM did not create new COVID-specific care protocols. Instead, we relied on existing evidence-based guidelines for the treatment of ARDS and septic shock. 9 –11 During the peak of the surge there was as shortage of certain sedating and neuromuscular blocking agents. Alternative management protocols were developed until supplies were re-established.
Bioethics and Mental Health Support
Given the anticipated ethical issues, regular meetings between MMCs Bioethics Department and the CCM COVID-19 Leadership Committee were scheduled. The potential lack of adequate ventilators and need to enact New York State’s ventilator allocation protocol was anticipated. 12 In 2018, MMC Bioethics had performed focus groups and interviews with bedside clinicians on the barriers to the implementation of crisis standards as established by the National Academies of Medicine. 13 Clinicians consistently expressed concern for their inability to enact crisis standards without state authorization. During the COVID-19 pandemic no such authorization from the Governor was given. Therefore, crisis standards were never formally implemented at Montefiore. 14 Instead, the COVID-19 Leadership Committee and other senior intensivist faculty in concert with the department of Bioethics provided real-time advice to assist clinicians with making decisions regarding appropriate utilization of limited resources.
Clinicians from Psychiatry met regularly with the critical care providers to provide group and individual support for clinicians in need. Clinicians also found novel approaches to boost morale during the most overwhelming periods. At the height of the pandemic, clinicians would take turns emailing out a “Daily Note of Positivity” that highlighted successes such as recent extubations of COVID-19 patients and inspirational patient stories.
Feedback on Systems
There was consensus that the CCCC was a crucial enhancement that allowed for rapid and rational triage of patients, better outreach of CCM expertise to inexperienced providers, recognition of patient deterioration, and efficient transfer of patients between campuses. Although Bioethics was regularly involved with the COVID-19 CCM Leadership Committee, there was agreement that more regular discussions with the bedside critical care clinicians were needed to provide a forum to “to hear your colleagues struggling with the same things and know that you’re like not totally off-base” and to better understand “how people approach cases and having the ethics consultant weigh in on principles of ethics.” But the respondents were divided about whether formal ethical guidelines would have been helpful. One speaker indicated that “it was unfortunate that the ethics group didn’t send us any guidelines because a lot of things that were done during the COVID catastrophe were not usual care. And every physician and provider had their own ideas of what is ethical or appropriate.” However, others indicated that such guidelines may force constraints upon the clinicians that might contribute more moral distress if the individual clinician did not agree with them. One provider stated “I think…the New York State vent allocation guidelines have, you know, very clear algorithm in the setting of limited ventilators. And when we went through them, a lot of us had problems with them not fitting very well for this particular disease…you may end up regretting it if you have an algorithm because the answer you get from it may not be the answer that you feel is right.” The respondents specifically mentioned their appreciation for the presence and availability of psychiatry, the “daily notes of positivity” that were shared, and the support of their colleagues.
Discussion
Our response to the initial surge of COVID-19 in New York City was complex and challenging. While guidelines and recommendations on critical care surge capacities have been published, 6,15 it is important to describe how these perform during this particular pandemic. Given our recent experience and the feedback received, we have proposed a practical guide to addressing Space, Staff, Supplies, and Systems during a COVID-19 surge. (Figure 5).
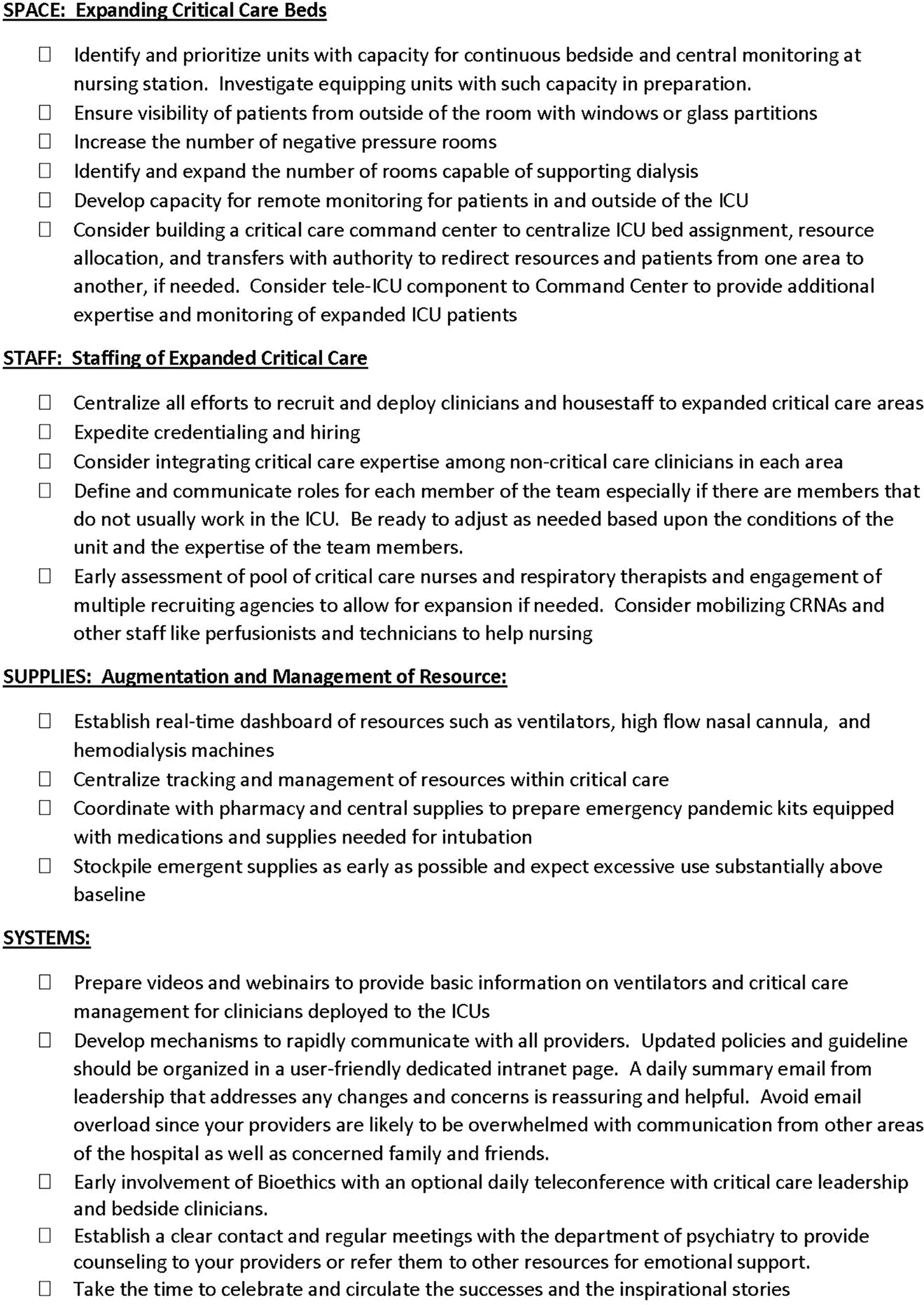
Checklist for critical care surge planning.
We followed many of the established recommendations for critical care pandemic response including employing multidisciplinary planning, using predictive modeling to help plan surge capacity, taking inventory of supplies and stockpiling before the surge, re-deploying and restructuring of healthcare workers in a tiered critical care staffing model, making accessible mental health support to frontline critical care workers, and using technology such as the CCCC to increase critical care delivery and centralize triage of critically ill patients. 6,15 However, our debriefing session revealed that this may not adequately relieve the stress and sense of being stretched “thin” experienced by frontline providers. Given the sheer volume of the initial surge in the Bronx, this may have been unavoidable without substantial additional investments in pandemic preparedness on local, state, and national levels.
Ultimately, augmentation of supplies was more feasible than augmentation of experienced staffing. Our unified Division of Critical Care Medicine may have made it much simpler to centralized critical care and triaging than other institutions that have different services providing care in different ICUs. Nevertheless, we needed to innovate with the creation of a telemedicine command center. While the CCCC was appreciated and found to be helpful uniformly, it could not replace the critical care nurses and respiratory therapists who were needed at the bedside. Similarly, while we anticipated the need for bioethics involvement and psychiatry in planning the response to the pandemic, we found that bioethics guidelines for scarce resources could both alleviate or exacerbate moral distress of the frontline critical care providers. Regular bioethics support for bedside providers should be considered in future pandemic responses.
Although we anticipated and prepared for many of the difficulties that we faced, the size and scope of the surge was at times overwhelming. The ability to be nimble and adaptable to the specifics of the pandemic were vital. We hope that this review and our recommendations may help other centers prepare for and manage future surge conditions from this pandemic.
Supplemental Material
Supplementary_Material - Critical Care Surge During the COVID-19 Pandemic: Implementation and Feedback From Frontline Providers
Supplementary_Material for Critical Care Surge During the COVID-19 Pandemic: Implementation and Feedback From Frontline Providers by Adam B. Keene, Ariel L. Shiloh, Lewis Eisen, Jay Berger, Manoj Karwa, Daniel Fein, Deborah Orsi and Michelle Gong in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.