
Abstract
Spontaneous intracranial hypotension typically manifests with orthostatic headaches and is caused by spinal dural tears, ruptured meningeal diverticula, or CSF-venous fistulas. While most patients are diagnosed and treated in the outpatient setting, some patients will occasionally present in the emergent ICU setting due to subdural hematomas, coma, or downward brain herniation. In this review paper, we will discuss the diagnostic and treatment steps that intensivists can undertake to coordinate a team approach to successfully manage these patients. A brief general overview of spontaneous intracranial hypotension will also be discussed.
Background
Spontaneous intracranial hypotension (SIH) is a well-recognized and treatable cause of headaches. SIH is secondary to spontaneous spinal CSF leaks, and there are 3 recognized types: dural tears from calcified disc protrusions or spiculated osteophytes, ruptured meningeal diverticula, and CSF-venous fistulas. 1,2
SIH is not typically a condition that requires urgent medical attention. The majority of patients with SIH can be safely managed and treated in an outpatient setting. Furthermore, because SIH is sometimes difficult to diagnosis, a significant number of patients live with the condition for months to years before treatment. A minority of patients; however, can become acutely obtunded or comatose, 3 and SIH can even be fatal in in a small percentage of patients. 4 While most of the existing literature on SIH focuses on the diagnostic and treatment plans, there is relatively little discussion of the specific workflow that pertains to the critical patient. Moreover, because SIH is prevalent throughout small and large hospitals, not all critical patients will be managed in a dedicated neurointensive care unit or a center that specializes in SIH. The purpose of this paper is to provide a clinical workflow for the critical SIH patient that can be managed in most intensive care units, which will be based on a literature review and the authors’ clinical experience.
General SIH Overview
Clinical Symptoms
Headaches are the most common feature in SIH and are usually positional. Headaches can worsen in the second half of the day and with Valsalva maneuvers. In addition, headaches can wane with time or be absent altogether, making the diagnosis challenging. Additional symptoms can include neck pain, nausea, tinnitus, cranial nerve palsies, and even a frontotemporal-like dementia. 5
MRI Brain Findings
In patients with clinical concern for SIH, contrast-enhanced brain MR imaging is performed and typical findings include brain sag, dural enhancement, venous distension, and subdural collections. 6 The brain MRI is positive in the majority of SIH patients and has always been abnormal in the critical patient in our experience. Subdural collections can be seen with SIH and are invariably bilateral. In the absence of trauma, bilateral subdural collections should raise suspicion for SIH.
Spine Imaging
The spinal imaging approach to SIH can differ depending on the institution, and the nuances are beyond the scope of this discussion but will be briefly described. After SIH is confirmed clinically and on MRI brain imaging, the spine should be imaged to evaluate the spinal leak. MR imaging of the total spine is performed and typically includes T2 fat-suppressed images in the sagittal and axial planes. The whole goal of imaging is to identify a CSF leak; therefore, additional T1 sequences and contrast administration are unnecessary. 7 If the spine MRI shows an extradural collection, the leak is either from a dural tear from a calcified disc or a ruptured meningeal diverticulum. A dynamic CT myelogram is then performed in either the prone position (for ventral disc-related leaks) or lateral decubitus position (for ruptured meningeal diverticula) to identify the exact leak site. 7 If the spine MRI does not show an extradural collection, a CSF-venous fistula should be suspected, which is typically an abnormal connection between a meningeal diverticulum and a vein that shunts out CSF fluid and results in SIH. The actual CSF-venous fistula cannot be seen on routine MR spine imaging, but meningeal diverticula can be seen on the spine MRI. In this scenario, a lateral decubitus CT or digital subtraction myelogram are performed to identify the CSF-venous fistula, as the decubitus position permits contrast to flow into the CSF-venous fistula on the dependent side of the thecal sac via gravity. 8,9 In our experience, the laterality of the decubitus myelogram is usually predicated on which side has a greater number of meningeal diverticula on the spine MRI, and this side is placed down on the procedure table. If the meningeal diverticula are approximately equal, we typically choose to start with a right lateral decubitus myelogram, as we have seen more CSF-venous fistulas on the right side in our experience. If there is no CSF-venous fistula on the first lateral decubitus myelogram, we bring the patient back the next day and image the contralateral decubitus myelogram. 8 During any of the various types of myelogram, an opening pressure can be performed, and a pressure of 6 cm of water or less is a diagnostic criterion for SIH. Nonetheless, the opening pressure is normal in the majority of SIH patients, as the pathophysiology of CSF leaks is better described as low CSF volume rather than low pressure. 2 Of note, SIH is typically secondary to spinal CSF leaks and not skull base leaks, the latter entity usually seen with intracranial hypertension. Thus, imaging of the skull base is not typically warranted in patients with SIH. 10
Spinal CSF Leak Treatment
Treatment of the underlying spinal leak can vary from conservative to percutaneous to surgical. Conservative treatments include bed rest to permit the CSF leak to “self-patch” on its own. Other conservative measures include oral hydration and caffeine administration. While some patients can certainly improve with these conservative measures, there are limited data on the efficacy and specific duration of bed rest. Non-targeted epidural blood patches are the next treatment and typically entail administering autologous blood in the lumbar spine. The efficacy of non-targeted epidural blood patches is variable, with a 52% success rate in one study. 11 The advantages of a non-targeted epidural blood patch are that it can typically be performed at most hospitals, does not typically need image guidance, and can be performed irrespective if the specific leak site is identified. On the other hand, we prefer image-guided targeted percutaneous treatments directly at the leak site origin with either blood or fibrin sealant, as our experience and prior literature both show that targeted treatments can increase the chance of sealing the leak compared to non-targeted treatments. 11 In the setting of CSF-venous fistulas, CT-guided fibrin sealants and endovascular transvenous embolization have been recently shown to be effective treatment options. 12,13 Lastly, surgery is typically a last resort option but is an effective treatment for all types of spinal leaks. Neurosurgical operations include removing calcified discs, repair of dural tears, and coagulation of CSF-venous fistulas. 14 –16
SIH in the Critical Patient
SIH With Small or Large Subdural Collections and Clinically Stable
Subdural collections in SIH can vary in consistency from CSF-filled effusions to hematomas with various ages of hemorrhage. Given the loss of CSF volume in SIH, subdural effusions are presumably related to compensatory enlargement and are a reflection of the Monro-Kellie doctrine. 2 Subdural hematomas, on the other hand, are possibly related to tearing of the bridging veins or bleeding of enlarged veins in the subdural space. 17
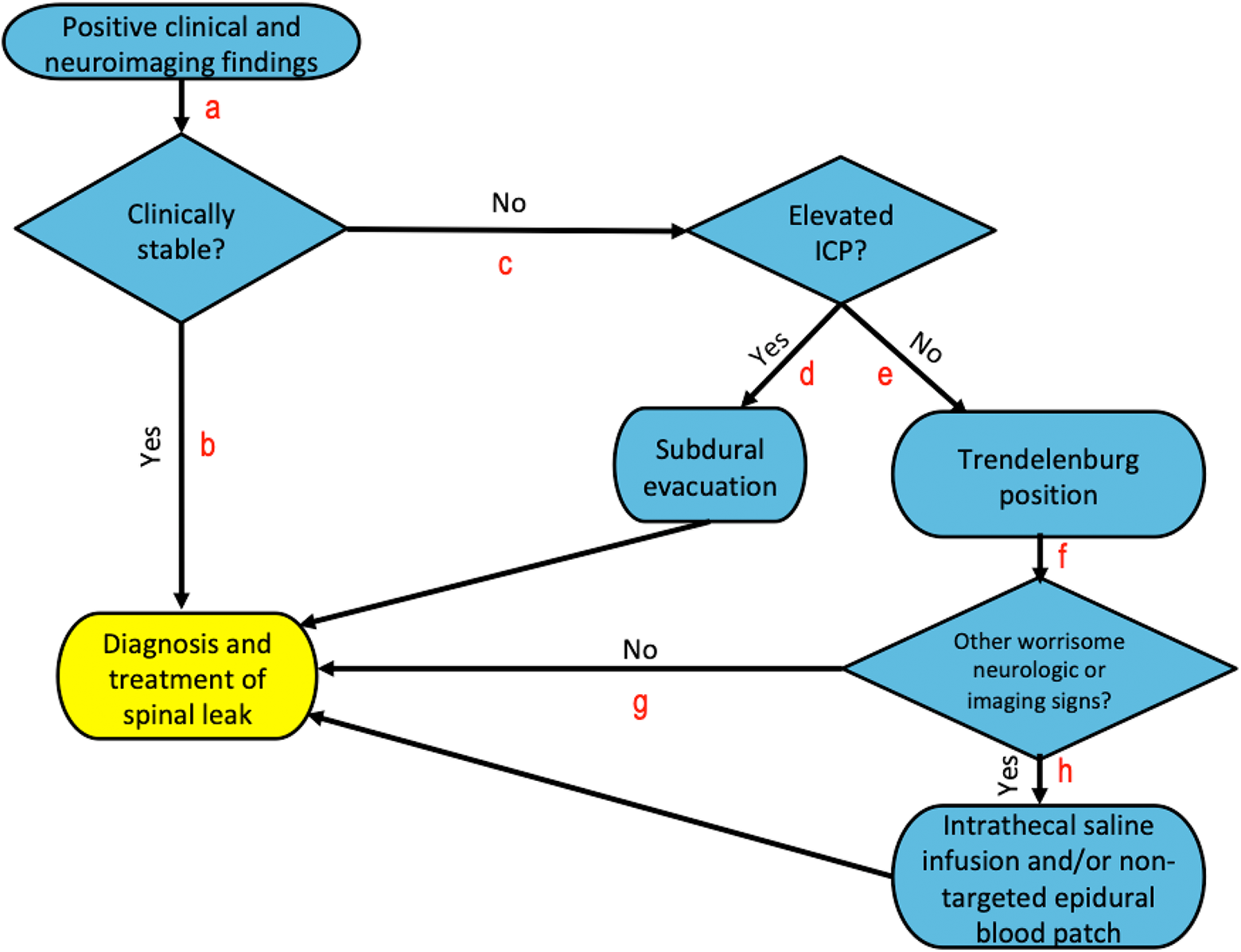
SIH algorithm in the critical patient. The algorithm begins with identifying a patient with positive clinical and neuroimaging findings of SIH. The patient is first assessed if clinically stable (a). If yes (b), then diagnosis and treatment of the spinal leak should be performed. If the patient is not clinically stable (c), then the patient is assessed for physical exam findings suggestive of elevated intracranial pressure. If yes, and there are subdural collections (d), then subdural evacuation should be performed, followed by addressing the spinal leak. If there is no elevated intracranial pressure (e), then the patient should be placed in the Trendelenburg position. Clinical and imaging assessment should be made if there are other worrisome neurologic signs besides coma (f). If no (g), then the spinal leak should be addressed. If there is additional clinical concern, and there is severe central downward herniation (h), then intrathecal saline infusion and/or non-targeted blood patching should be performed, followed by addressing the spinal leak.
Treatment of the subdural collections should be guided by the patient’s neurological stability (Figure 1). If the patient is clinically stable, diagnosis and treatment should focus on the spinal leak and not drainage of the subdural collections for multiple reasons. First, it is important to remember that the subdural collections are an effect of SIH, not the cause. Second, in many cases, the subdural collections are chronic and there are no resultant neurologic deficits. Third, there are multiple reports that state that subdural collections can recur if surgically evacuated and the underlying spinal leak is not addressed. 4,17 –19 Lastly, there is some evidence that treating the subdural hematoma in isolation of SIH may even be harmful, as the craniotomy can decrease the intracranial pressure after being exposed to atmospheric pressure. 20 For these reasons, subdural collection evacuation should be avoided if the patient is not directly symptomatic from the subdural collections. Instead, identifying and treating the spinal leak should be the focus using the steps outlined in the previous section and can either be performed in the inpatient or outpatient setting, depending on the clinical status of the patient and availability to perform the workup (Figure 2).
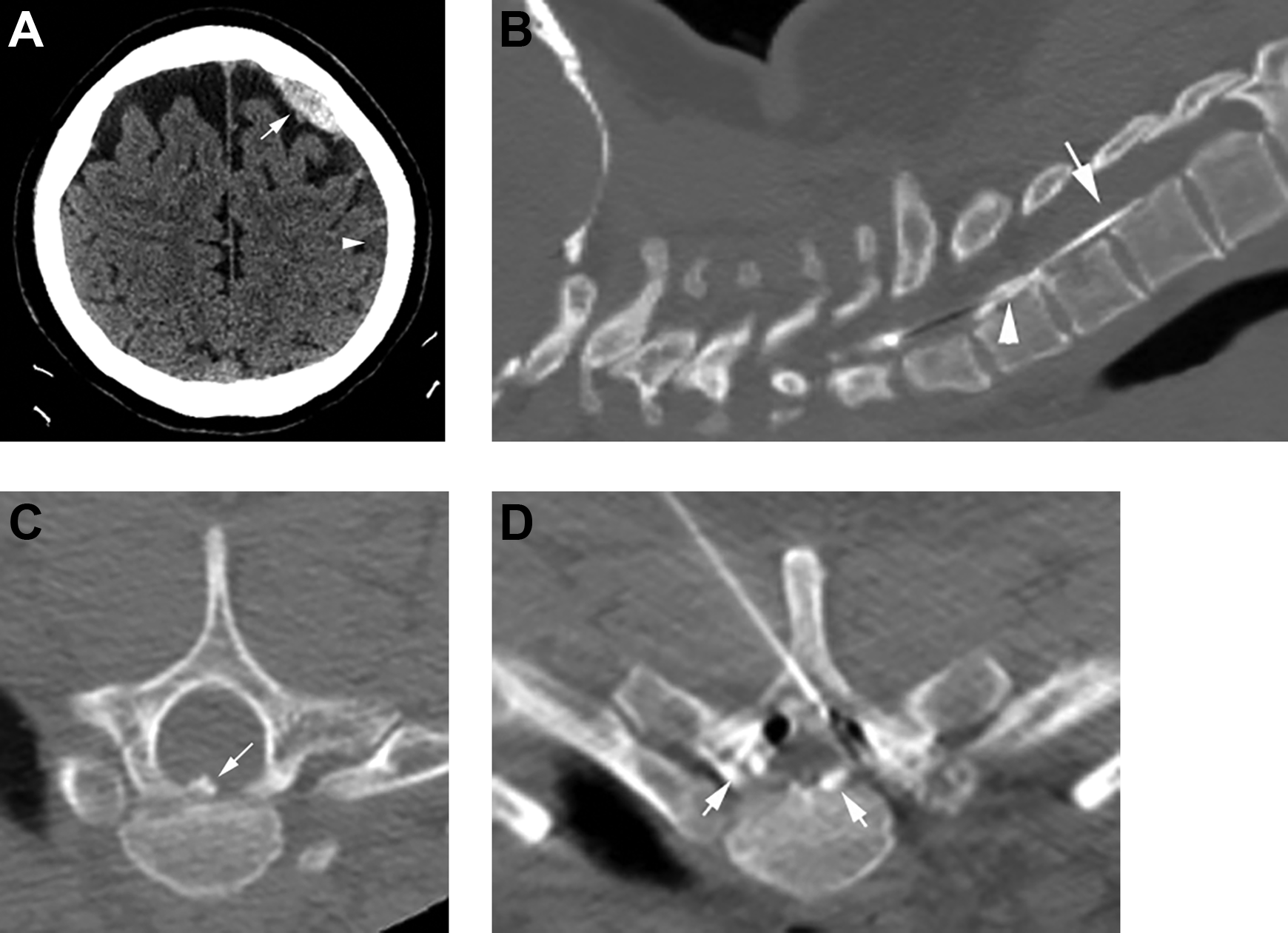
Subdural collections in a clinically stable 33-year-old woman who had abrupt orthostatic headaches after kickboxing class. (A) Axial noncontrast CT head shows a left frontoparietal convexity subdural collection with acute (arrow) and chronic (arrowhead) hemorrhage. (B) Sagittal CT image of a dynamic myelogram in the prone position shows normal intrathecal contrast (arrow) and a ventral extradural CSF leak (arrowhead) at the T1-T2 level, which was secondary to a calcified disc (C, arrow). (D) CT-guided epidural blood patch was performed with circumferential contrast-enhanced blood in the epidural space (arrows), which cured the patient. Air is also noted in the epidural space from the prior epidurogram (not shown) that was performed to confirm the epidural space prior to injection of blood.
SIH With Large Subdural Collections and Clinically Unstable
One major difficulty in this group of patients is determining if the patient is clinically unstable from the large subdural collections or from downward herniation related to SIH. As described in the previous section, many subdural collections can be managed without drainage and by addressing the spinal leak (Figure 3). There are reports that state subdural evacuation should be performed in the setting of uncal herniation and loss of consciousness 21 ; however, both of these features can be seen with severe SIH resulting in central herniation and brainstem compression and are discussed in the subsequent sections. Thus, we propose that subdural evacuation should solely be performed if there are distinct physical exam signs of increased intracranial pressure that are directly attributed to the subdural collections. In the event that subdural evacuation is done, we have empirically placed a drain in the subdural space and maintained a negative pressure using a subdural evacuating port system. This negative pressure can be obtained using standard materials, such as Jackson-Pratt or Blake bulbs. In our experience, ventricular drains at gravity provide insufficient negative force for these circumstances. Also, keeping the patient supine or even in intermittent Trendelenburg positions while draining can be beneficial. We generally maintain this negative pressure drainage while the patient is undergoing targeted or non-targeted percutaneous treatment for the spinal leak. Finally, unlike other subdural evacuations, a clamp and reimage trial of the brain can be entertained prior to removal of the drain.
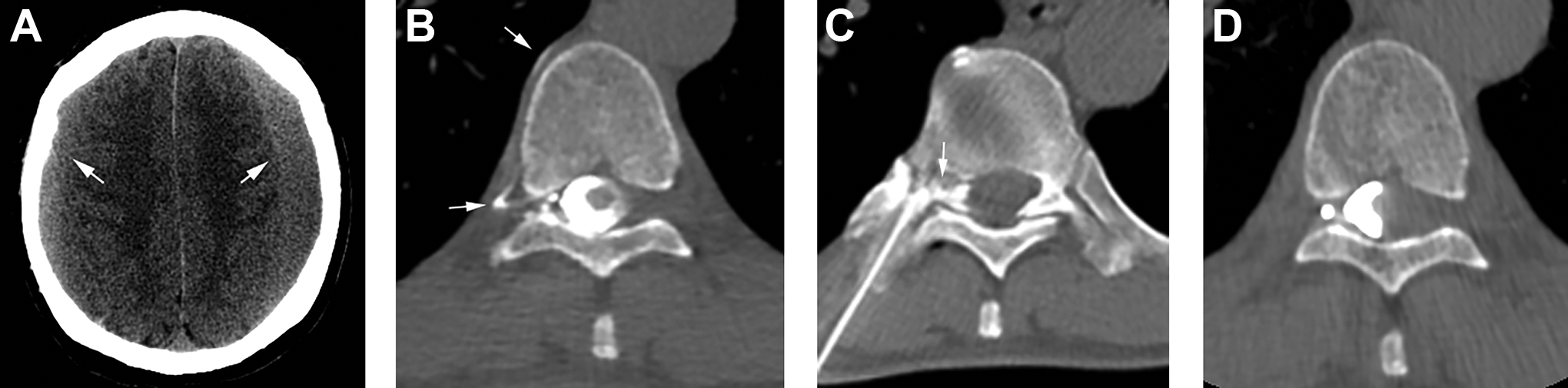
Large subdural hematomas in a 64-year-old man that was clinically stable and endorsed orthostatic headaches. A, Axial noncontrast CT head shows bilateral holohemispheric subacute subdural hematomas (arrows), left greater than right. Subdural evacuation was not performed, as there were no physical exam findings to suggest elevated intracranial pressure. B, Right lateral decubitus CT myelogram was performed after a normal spine MRI (not shown) and reveals a right T9-T10 CSF-venous fistula with a paravertebral course (arrows). C, CT-guided fibrin glue occlusion was performed with contrast-enhanced glue injected in the neural foramen and epidural space (arrow). D, Post-treatment right lateral decubitus CT myelogram 1.5 months later shows resolution of the CSF-venous fistula. The patient’s symptoms also clinically resolved, including a frontotemporal-like dementia.
SIH With Coma and/or Central Herniation
This subset of patients is the most life threatening and challenging to clinically address. Clinically, patients can present with lethargy, confusion, coma, fixed pupils, Cheyne-Stokes breathing, and decerebrate posturing. Coma is an uncommon clinical presentation in patients with SIH and is invariably seen with brain sagging although not all patients with brain sagging manifest with coma. 3 A recent study that evaluated brainstem lesions found the left pontine tegmentum to be the potential anatomic location to induce coma if affected. 22 In SIH patients with brain sag, the pons is flattened and this could potentially result in disruption of the pontine tegmentum. While coma is an alarming feature in the SIH patient, it is typically reversible if the underlying spinal leak is treated.
The first step in treatment is to place the patient in the Trendelenburg position, which is the exact opposite positioning for central herniation not related to SIH and could be life-saving. 4 Because of the acuity of the condition, the authors suggest to only proceed with the spinal imaging diagnostic workup if the patient is clinically stable. If the patient is clinically unstable with additional neurologic symptoms besides coma, and there is severe central herniation with complete CSF effacement of the basilar cisterns on brain imaging, maneuvers to raise intracranial pressure and volume are preferred. This can be done by an intrathecal saline infusion via a lumbar drain placement. One group has administered large boluses up to 163 cc of saline, 23 while another group had a constant infusion rate of 20 cc/hour. 24 Both groups used simultaneous intracranial pressure monitoring to gauge the effectiveness of the saline infusion. Alternatively, a non-targeted large volume epidural blood patch can also be performed. No studies have compared the 2 techniques in this specific population but both have likely similar effectiveness. In addition, both techniques could also theoretically be performed at the same time as well. There may be some concerns of performing a lumbar puncture for intrathecal saline administration or the myelogram in the setting of brain sagging, with particular concern for worsening the herniation; however, a spinal leak is already present and the CSF pressure is generally low. In one study, no reports of clinical or radiologic worsening were seen after the lumbar puncture in patients with coma. 3 The authors’ experiences also coincide with this as well. Lastly, it is important to note that when performing a lumbar puncture to ensure the needle is in the subarachnoid space prior to intrathecal saline administration or contrast injection for a myelogram, CSF return may be limited or absent altogether due to the low pressure and volume in these patients and make it challenging to ensure correct needle placement. Image guidance can help mitigate this potential obstacle in these cases.
Urgent CT or MR imaging of the brain should be performed to determine if there is central downward herniation characterized by medial displacement of the uncus beyond the tentorial incisura. If a CT scan of the head is performed, pseudo-subarachnoid hemorrhage is a potential imaging feature and manifests as increased attenuation in the basilar cisterns and vessels, the tentorium cerebelli, or along the falx cerebri, mimicking subarachnoid hemorrhage. 25 Pseudo-subarachnoid hemorrhage is often seen in patients with cerebral edema and is likely secondary to vascular engorgement. Identification of other features seen in SIH, such as sagging of the brainstem or cerebellar tonsils and subdural collections, should direct the provider to the diagnosis of pseudo-subarachnoid hemorrhage.
Many of the SIH patients with this severe complication of the condition have subdural collections that are often small and disproportionate to the degree of central herniation and the aforementioned clinical signs. Subdural evacuation should be avoided in this group of patients, and if performed, the subdural collections can recur or even worsen the degree of herniation. 4,18,20
Steroids may be another helpful treatment to stabilize the patient in this precarious situation. In one reported patient with central herniation and coma, intravenous dexamethasone was administered and decreased the brain herniation and the patient regained consciousness. 26 The authors also have witnessed a similar experience with steroid treatment (Figure 4); however, further studies are needed to validate these findings.
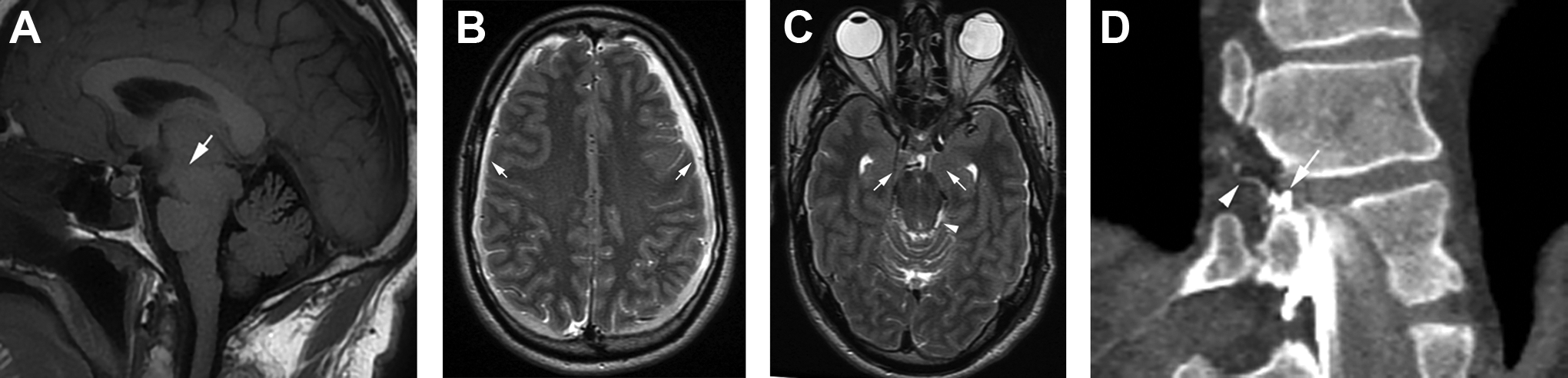
Coma in a 57-year-old man with a CSF-venous fistula. A, Sagittal T1-weighted imaging of the brain shows midbrain sag (arrow) that is in keeping with SIH. B, Axial T2-weighted image at the vertex shows small subdural effusions (arrows) without significant mass effect. C, Axial T2-weighted image at the base of the brain shows bilateral uncal herniation (arrows). There is still some CSF present in the left ambient cistern (arrowhead), suggesting incomplete central herniation. Steroids were administered, and the patient regained normal consciousness. D, Right lateral decubitus CT myelogram in the coronal plane performed the next day shows an irregular meningeal diverticulum (arrow) at the right T11-T12 level that communicates with a vein (arrowhead), which is compatible with a CSF-venous fistula. This patient was treated with fibrin glue occlusion (not shown), similar to the previous figure, and was cured.
If the central herniation progresses without or with the aforementioned stopgap treatments, the prognosis is very poor and often fatal. Surgical options are limited, and the herniation can result in acute infarction in the posterior cerebral artery distribution or brainstem and death (Figure 5). 4
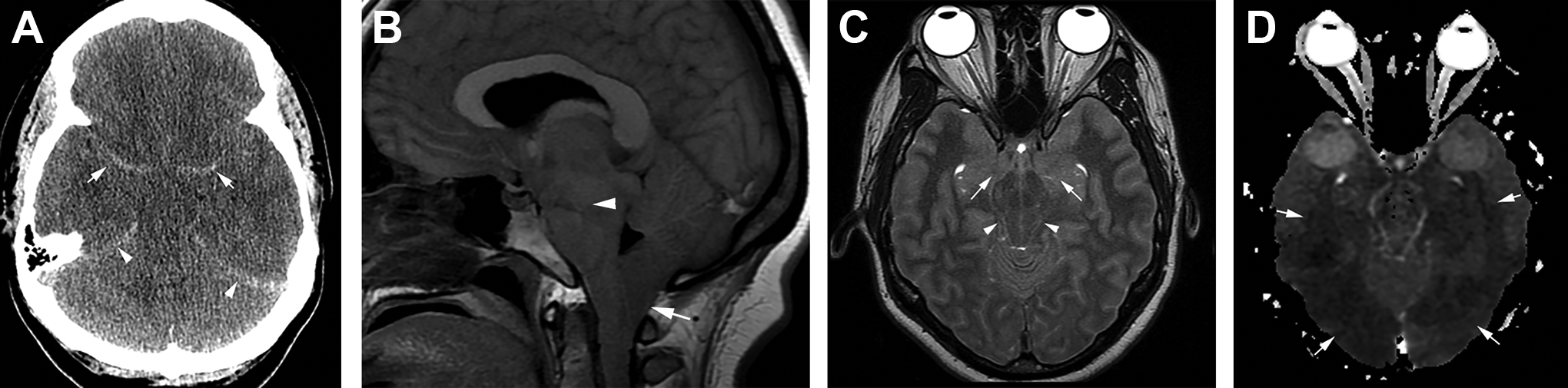
Fatal case of SIH in a 35-year-old woman with severe central herniation. A, Axial noncontrast CT head shows hyperdensity along the bilateral middle cerebral arteries (arrows) and tentorium cerebelli (arrowheads), which is compatible with pseudo-subarachnoid hemorrhage. B, Sagittal T1-weighted image of the brain shows severe sagging of the cerebellar tonsils (arrow) and midbrain (arrowhead). C, Axial T2-weighted image shows bilateral uncal herniation (arrows) and complete CSF effacement of the basal cisterns (arrowheads). In addition, the gray matter is diffusely hyperintense and the sulci are effaced, which are consistent with cerebral edema. D, Apparent diffusion coefficient image of the brain shows hypointense signal in the bilateral posterior cerebral artery distributions (arrows) that is compatible with acute infarction secondary to narrowing of the posterior cerebral arteries (not shown). This patient was declared brain dead shortly after, despite intrathecal saline infusion. An undiagnosed CSF-venous fistula was likely the cause of the SIH.
Conclusion
Spontaneous intracranial hypotension can occasionally necessitate urgent medical attention and manifest with various clinical and imaging signs. In many of these settings, first identifying and treating the spinal leak is paramount. Subdural collections are a common manifestation in this group of patients but evacuation is often unnecessary and care should be made when considering subdural treatment in isolation of the SIH syndrome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.