
Abstract
Background:
Patients with a history of alcohol use disorder are at an increased risk of hematoma expansion following intracranial hemorrhage (ICH) due to the effects of alcohol on platelet aggregation. Desmopressin (DDAVP) improves platelet aggregation and may decrease hematoma expansion in patients with ICH. However, DDAVP may also increase the risk of hyponatremia and thrombotic events. Evidence is limited regarding the safety and efficacy of DDAVP in alcohol use (AU)-associated ICH.
Methods:
This was a retrospective chart review of adult patients with radiographic evidence of ICH and a confirmed or suspected history of alcohol use upon admission. Patients were categorized into groups based on DDAVP administration. Safety outcomes included hyponatremia (serum sodium <135 mEq/L or decrease in serum sodium of ≥ 5 mEq/L for patients with baseline sodium <135 mEq/L) within 24 hours of ICH and thrombotic events within 7 days of ICH. The primary efficacy outcome was the incidence of hematoma expansion, defined as any expansion of the hemorrhage noted on repeat imaging within 32 hours.
Results:
In total, 52 patients were included in the safety analysis (27 DDAVP and 25 non-DDAVP). Although hyponatremia was numerically higher in the DDAVP group, there was no significant difference between groups (19.2% vs 4.2%, P = 0.192). Thrombotic complications were similar between the DDAVP and non-DDAVP groups (11.1% vs. 8%, P = 1.0). Thirty-nine patients met criteria for hemostatic efficacy analysis. There was no difference in hematoma expansion between the DDAVP and non-DDAVP groups (23.1% vs 34.6%, P = 0.71) and these findings were consistent after adjusting for differences in baseline characteristics (OR 0.63, 95% CI 0.1-3.3).
Conclusion:
The administration of DDAVP was not associated with adverse safety events, but did not significantly reduce the incidence of hematoma expansion in patients with AU-associated ICH.
Introduction
Intracranial hemorrhage (ICH) is a neurologic emergency. 1,2 Hematoma expansion on follow-up imaging occurs in over one-third of patients, and independently predicts neurological deterioration and less favorable outcomes. 1,3 To minimize the risk of hematoma expansion, blood pressure management and reversal of coagulopathy are the cornerstones of treatment. 1
Alcohol use and alcohol use disorder (AUD) may increase the risk of hematoma expansion via interaction of alcohol with von Willebrand Factor and platelet aggregation. 4 –6 Acute alcohol intoxication can trigger platelet apoptosis, thereby reducing platelet count and function. 4 Additionally, chronic alcohol use can inhibit thrombopoiesis leading to thrombocytopenia. Patients with AUD may have platelet dysfunction despite undetectable serum alcohol levels, with platelet function typically recovering after 1-2 weeks of abstinence. 7 Furthermore, cirrhosis alters platelet function through reduced transmembrane signaling and intracellular messengers leading to a decrease in platelet aggregation. 8
Desmopressin, or 1-deamino-8-D-arginine vasopressin (DDAVP), increases the release of von Willebrand factor, a mediator of platelet aggregation, and may decrease hematoma expansion in patients with ICH. 9 Guidelines for the reversal of antithrombotics in ICH state that desmopressin can be considered for patients with antiplatelet-associated ICH or in those deemed appropriate for platelet transfusion (e.g. undergoing neurosurgery). 10 Patients with AUD who develop ICH are often excluded or not separately reported in trials examining the effects of DDAVP in patients with ICH. In the present study, we sought to evaluate the safety and efficacy of desmopressin in patients with alcohol use (AU)-associated ICH.
Methods
This was a retrospective chart review at a large academic medical center. Institutional review board approval and waiver of informed consent were obtained prior to study initiation. Patients admitted to the neuroscience or surgical intensive care units (ICU) at New York-Presbyterian Hospital/Weill Cornell Medical Center between January 2015 and December 2019 were screened in several phases in order to maximize the efficiency of chart review and to identify patients for inclusion that may have been improperly coded. The first phase of screening evaluated patients with ICD 9 or 10 codes for AUD and ICH. The second phase of screening evaluated patients with ICD 9 or 10 codes for ICH who received DDAVP, where administration data was obtained via pharmacy database. The third phase of screening evaluated all patients with an ICD 9 or 10 code for ICH. The final phase of screening evaluated patients in the pre-specified ICUs who were receiving levetiracetam as it is routinely prescribed for seizure prophylaxis following a traumatic brain injury.
Adult patients with documented radiographic evidence of ICH were included if they had a confirmed or suspected history of alcohol use upon admission. Alcohol use was identified primarily through documentation in progress notes. Given the challenges of identifying the psychosocial aspects of AUD in a retrospective chart review, patients were included if they had a documented history of alcohol use disorder or if they were intoxicated at presentation. Patients with antithrombotic therapy exposure within 7 days of the ICH, pregnancy, or incarceration were excluded. Patients who received neurosurgical intervention between initial and follow-up imaging were included in the safety outcome analysis; however, these patients were excluded from the efficacy outcome (hematoma expansion).
The main safety outcomes included hyponatremia within 24 hours and thrombotic events within 7 days of the ICH. Hyponatremia was defined as a serum sodium <135 mEq/L or a decrease in serum sodium of ≥ 5 mEq/L for patients with baseline sodium <135 mEq/L. Thrombotic events included deep vein thrombosis, defined as any new thrombosis observed on Doppler or compression ultrasonography; pulmonary embolism, defined as any new thrombosis observed on chest computed tomography (CT) or magnetic resonance imaging (MRI) or fluoroscopy; ischemic stroke, defined as any new change on head CT or MRI demonstrating infarct; and myocardial infarction, defined as any new electrocardiography (ECG) changes with troponin elevations, requiring intervention.
The efficacy outcome was the incidence of hematoma expansion, defined as any hemorrhage expansion noted on repeat imaging within 32 hours. Stability imaging is frequently conducted within 24 hours of the initial scan, and an additional 8-hour window was selected to allow for any delays in imaging. Hematoma expansion and location of injury on imaging was assessed by a neurologist who was blinded to the treatment groups. Hematoma expansion was defined as any increase in hematoma volume on follow up imaging. For each hemorrhage subtype, the following objective criteria were used to determine the presence or absence of expansion on follow up imaging. Intraparenchymal hematoma expansion was quantified using the ABC/2 method. 11 Subdural and epidural hematoma expansion were quantified using hematoma thickness and midline shift. Subarachnoid hemorrhage expansion was quantified using hemorrhage thickness, number of involved cisterns, and expansion of intraventricular hemorrhage. Multifocal hemorrhage expansion was quantified using a combination of these approaches as well as the emergence of new foci of hemorrhage on follow-up imaging.
Patients who were transferred from an outside hospital were included in the efficacy analysis if initial imaging was available; otherwise, these patients were only included in the safety analysis. Patients who received DDAVP after follow-up imaging were designated to the DDAVP group for the safety analysis to ensure these outcomes would be reflective of all patients who received DDAVP. However, these patients were designated to the non-DDAVP group for the efficacy outcome as hematoma expansion was assessed on follow-up imaging prior to DDAVP administration.
Descriptive statistics were performed for all variables. Continuous variables were analyzed using Wilcoxon rank-sum test and categorical variables using Chi-squared or Fischer exact test where appropriate. P value of less than 0.05 was used to designate statistical significance. Logistic regression was used to analyze factors associated with hematoma expansion. Variables with P values < 0.2 in univariate analysis were analyzed in a multivariate analysis. The primary covariate, namely DDAVP administration, was included in the final multivariate model. Statistical analyses were conducted using STATA version 14.2 (College Station, TX).
Results
A total of 93 patients were eligible for inclusion and 41 patients were excluded because of antithrombotic therapy within 7 days of ICH (Figure 1). Fifty-two patients were included in the safety analysis (27 DDAVP and 25 non-DDAVP). Both groups were similar in age, sex, race, and comorbidities with a median age of 57.5 (IQR, 50-67.5) years and 80.8% male among the combined cohort. The location of initial injury was similar between groups with subdural hematoma being the most common injury (74.5%), followed by intraparenchymal hemorrhage (56.9%), and a majority of patients (80.4%) presented with a traumatic brain injury (TBI). Most patients had a blood alcohol level (BAL) collected on admission, and the DDAVP group had a higher median BAL than the non-DDAVP group (207 mg/dL vs 47.5 mg/dL, P = 0.106). Baseline platelets were significantly lower in the DDAVP group (184 × 103/µL vs 226 × 103 /µL, P = 0.03). The severity of illness was similar between groups [Glasgow Coma Scale (GCS) 14 (IQR, 10-14), ICH score 1.5 (IQR, 0-2), and Hunt-Hess score 4 (IQR, 1-4)]. Twenty patients (12 DDAVP, 8 no DDAVP) underwent neurosurgical intervention, and of these, 8 patients (5 DDAVP, 3 no DDAVP) required craniectomies. Additional baseline characteristics are described in Table 1. The median DDAVP weight-based dose was 0.29 mcg/kg (IQR, 0.27-0.31) and patients received intravenous DDAVP 3.9 (IQR, 1.5-6.6) hours after their initial imaging. DDAVP was administered within 24 hours of the initial imaging and was not given more than once in any patient.
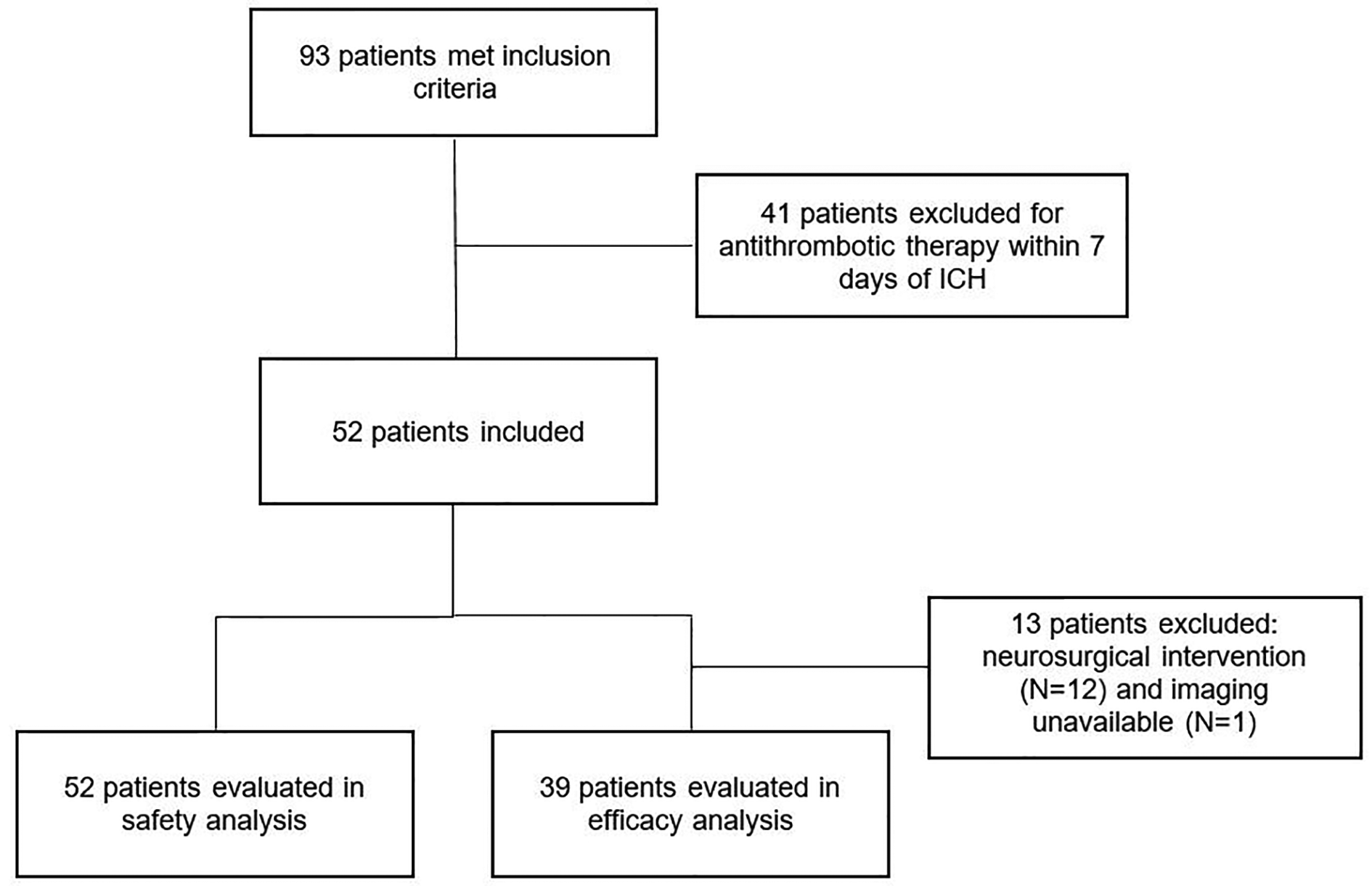
Screening process. ICH indicates intracranial hemorrhage.
Baseline Characteristics.a
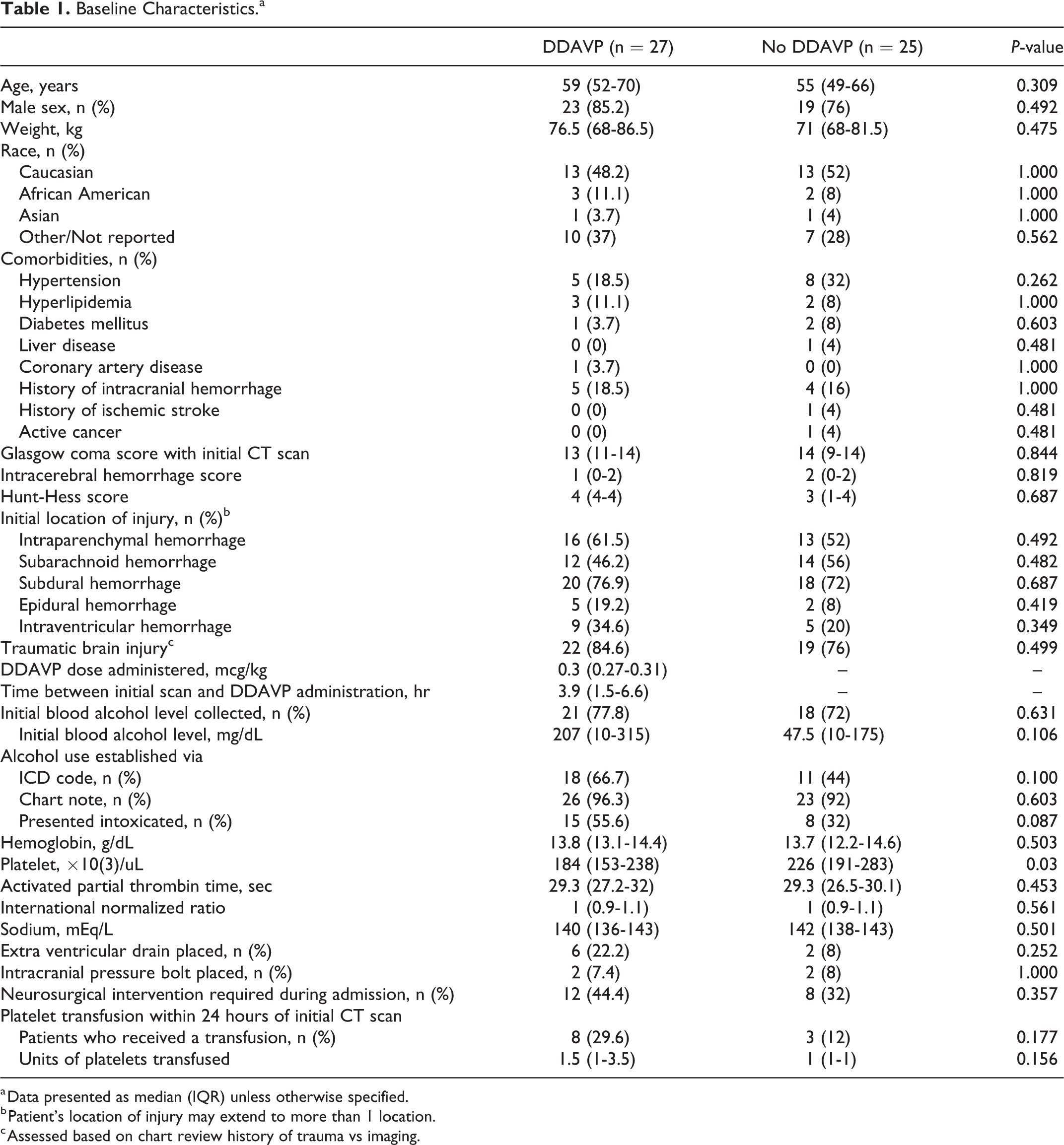
a Data presented as median (IQR) unless otherwise specified.
b Patient’s location of injury may extend to more than 1 location.
c Assessed based on chart review history of trauma vs imaging.
The incidence of hyponatremia and frequency of hypertonic saline administration were numerically higher in the DDAVP group as compared to the non-DDAVP group, however, the differences were not significantly different (19.2% vs. 4.2%, P = 0.192 and 29.6% vs 20%, P = 0.423, respectively). There was no difference in the incidence of thrombotic complications (DDAVP 11.1% vs non-DDAVP 8%, P = 1.0). Safety outcomes are described in Table 2.
Hypertonic Saline Administration and Safety Outcomes.a
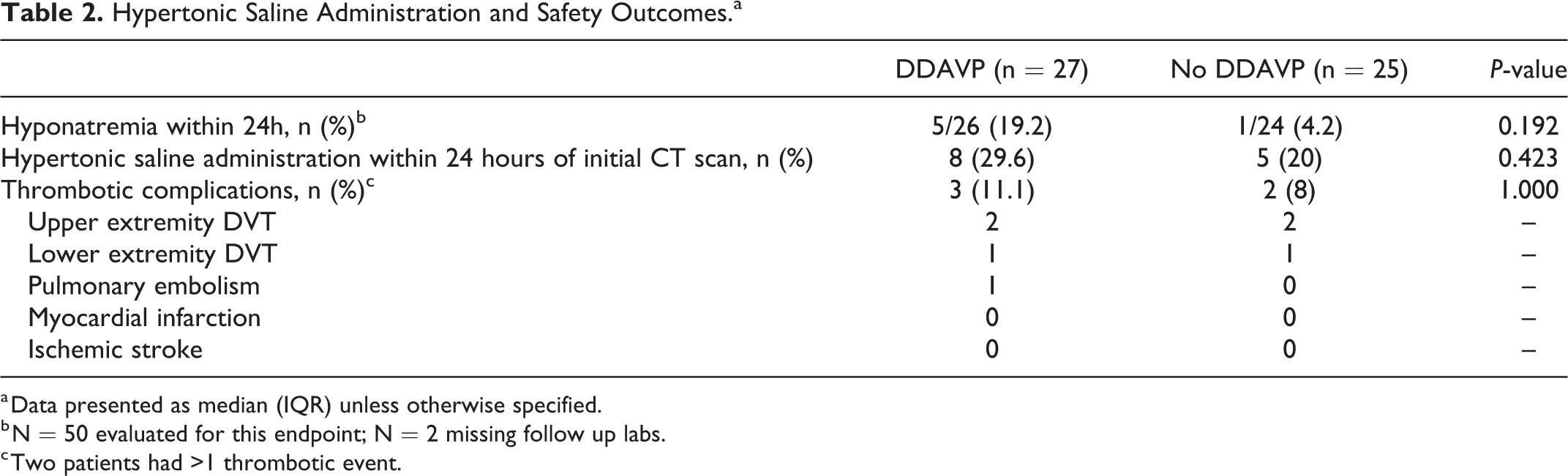
a Data presented as median (IQR) unless otherwise specified.
b N = 50 evaluated for this endpoint; N = 2 missing follow up labs.
c Two patients had >1 thrombotic event.
Thirty-nine patients met criteria for hemostatic efficacy evaluation (13 DDAVP and 26 non-DDAVP). Patients in this group received DDAVP 1.8 (IQR, 1.3-3.9) hours after their initial imaging. There was no difference in the rate of hematoma expansion between groups (DDAVP 23.1% vs non-DDAVP 34.6%, P = 0.714). There was no difference in ICU or hospital length of stay or mortality. The median modified Rankin Score (mRS) at discharge was similar (DDAVP 3 vs non-DDAVP 2, P = 0.631), however more patients who received DDAVP were discharged home (76.9% vs 38.5%, P = 0.041). Additional study outcomes are noted in Table 3.
DDAVP Administration and Efficacy Outcomes.a
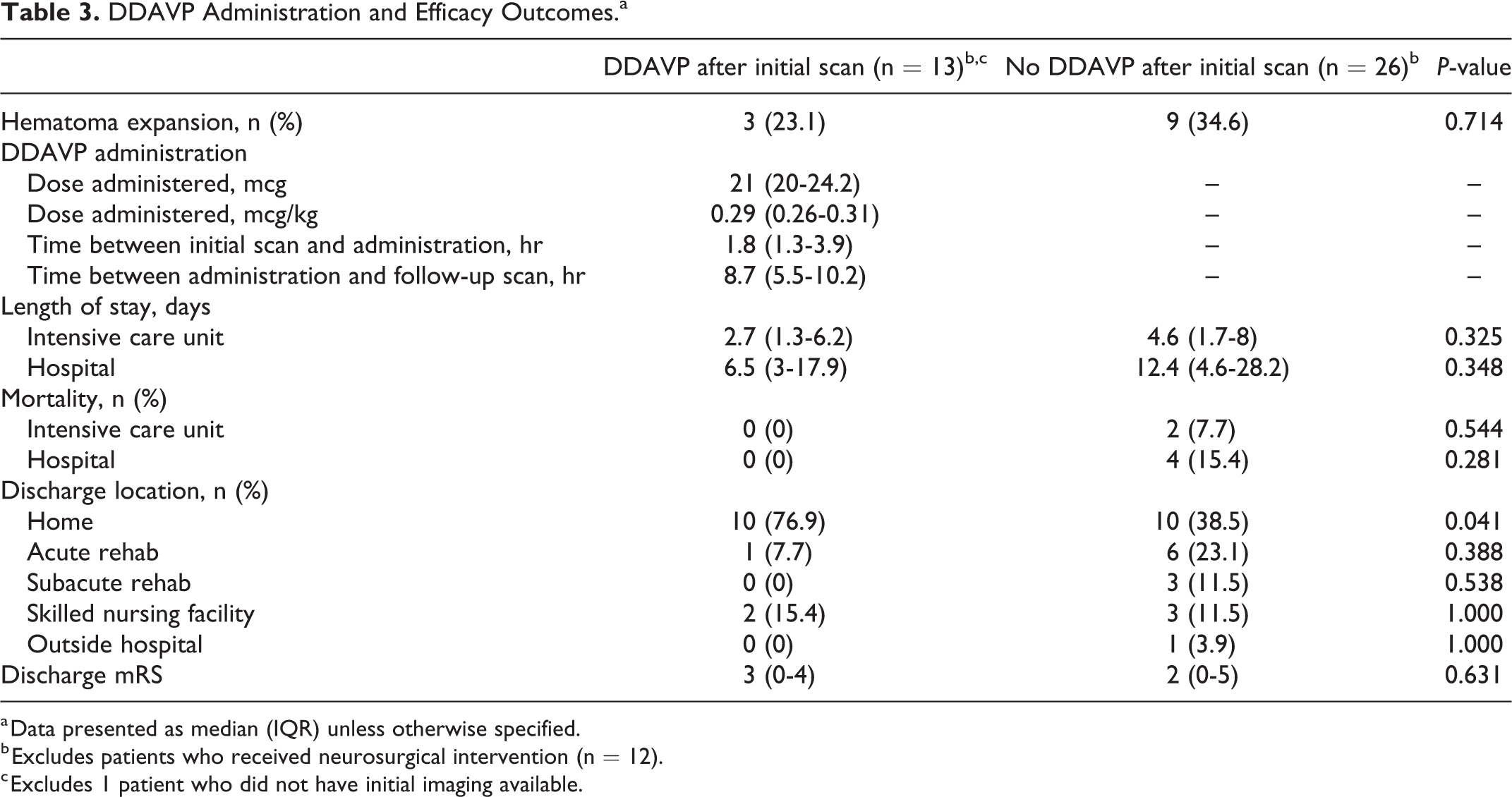
a Data presented as median (IQR) unless otherwise specified.
b Excludes patients who received neurosurgical intervention (n = 12).
c Excludes 1 patient who did not have initial imaging available.
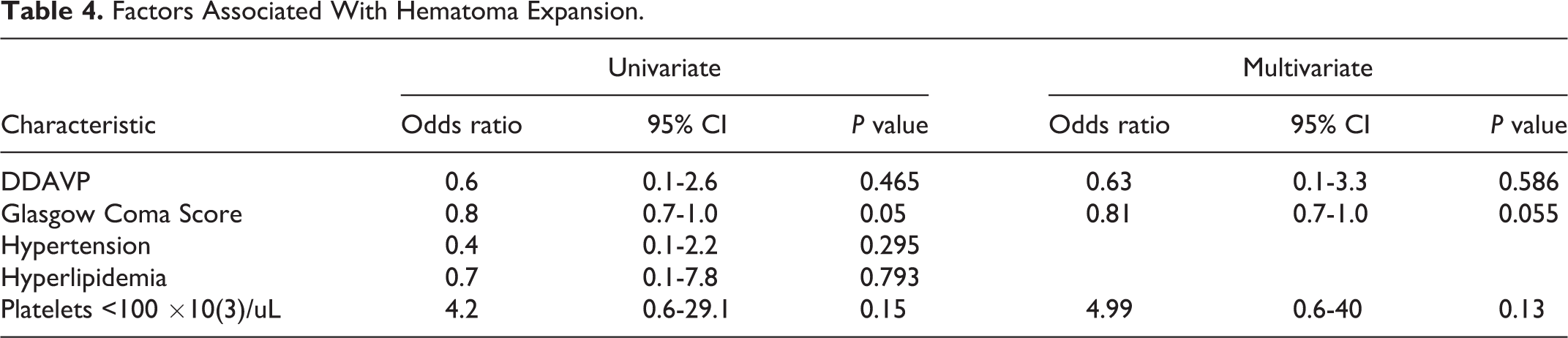
Logistic regression was utilized to identify factors associated with hematoma expansion in the evaluable cohort. Variables assessed included DDAVP administration, GCS score at presentation, hypertension, hyperlipidemia, and a serum platelet count <100,000 × 103 /µL. No characteristics were identified to be independently associated with hematoma expansion (Table 4).
Factors Associated With Hematoma Expansion.
There were 8 patients who received DDAVP after initial follow-up imaging. The weight-based dose of DDAVP administered in this subgroup of patients was 0.3 mcg/kg (IQR, 0.27-0.31) and time to DDAVP administration was 2.5 (2.1-3.6) hours after the follow-up imaging. Hyponatremia occurred in 1 (12.5%) patient, and no thrombotic complications were noted. Three of these patients were unable to be evaluated for hematoma expansion as they either had a neurosurgical procedure or never had additional imaging. Of the 5 evaluable patients, 2 patients received DDAVP despite not having hematoma expansion on the first follow-up image, the other 3 received DDAVP subsequent to hematoma expansion on follow up imaging. Four of the 5 evaluable patients (80%) had hematoma expansion upon further imaging after DDAVP administration. The mRS at discharge was numerically higher in this subgroup compared to the DDAVP group (subgroup 5 vs DDAVP 3), and more patients were discharged to a skilled nursing facility versus home.
Discussion
To our knowledge, this is the first study assessing the use of DDAVP for AU-associated platelet dysfunction in ICH, and these findings suggest that DDAVP does not significantly increase the risk of hyponatremia or thrombotic complications. Additionally, we did not find an association with DDAVP administration and a reduction in hematoma expansion.
Previous studies in antiplatelet-associated ICH have reported variable outcomes in hematoma progression and hyponatremia and no significant increase in thrombotic events with the use of DDAVP. 12 -16 The initial study evaluating the effects of DDAVP on hemostasis time demonstrated an improvement from baseline to 1 hour, although this study evaluated patients with known aspirin use or reduced platelet function. Safety outcomes reported a mean change of 0.6 mEq/L in sodium and no reported thrombotic complications. 9 Kim et al assessed DDAVP and platelets on hematoma progression in patients with a history of hypertension (16%-41%), antiplatelet use (6%-30%), and alcoholism (9%-11%). There was a non-significant increase in hematoma expansion in the intervention group and a venous thromboembolism rate <1%. A subgroup analysis of patients with alcoholism was not performed to assess if these patients responded differently to the intervention compared to the general population. 12
Three recent retrospective analyses demonstrated similar outcomes to previous studies in hematoma expansion, platelet dysfunction, hyponatremia, or thrombosis when DDAVP was administered. 17 -19 Mengel et al found similar hematoma expansion in patients who received platelets and DDAVP for antiplatelet associated ICH, and serious thromboembolic events were low in both groups. 17 Barletta et al showed a significant decrease in hematoma expansion when DDAVP was administered to patients experiencing a traumatic, antiplatelet-associated ICH (DDAVP 14% vs non-DDAVP 30%, P = 0.015) without an increase in thrombotic events; however, there were less patients with concomitant anticoagulation exposure in the DDAVP group (5.7% vs 18%, P = 0.008) and more patients in the DDAVP group who received a platelet transfusion (41% vs 23%, P = 0.03). 18 Furay et al demonstrated a decrease in platelet dysfunction, defined as adenosine diphosphate inhibition of 60% or greater on thromboelastography–platelet mapping, without a significant difference in change in sodium in patients with severe TBI who received DDAVP 0.3 mcg/kg compared to 1 unit of apheresis platelets. 19 Overall, the patient populations mentioned above significantly differ from this current study population, which primarily consisted of traumatic ICH associated with alcohol use. Additionally, it is unclear if patients in any of these studies had a history of alcohol use as it was not listed as an exclusion criteria nor mentioned in the patient demographics. Due to the limited data in patients with AU-associated ICH, it is unclear if desmopressin provides a benefit in preventing hematoma expansion; however, these studies demonstrate no significant increase in hyponatremia or thrombotic complications.
DDAVP is an attractive hemostatic agent worth continued investigation given its mechanism on von Willebrand factor, ease of administration, and low rates of major adverse events. Despite differences in patient characteristics and etiology of ICH in this study compared to previous studies, the rates of hematoma expansion were similar (30%-43.7%). 12,14 Similar to previous studies, there was no difference in hematoma expansion, hyponatremia, or thrombotic complications between groups. 12,15,17 However, hyponatremia and hypertonic saline administration were numerically higher in the DDAVP group, although these findings did not reach statistical significance.
The subgroup of patients who received DDAVP after a follow-up scan had a higher rate of hematoma expansion. Numerous factors likely contributed to these patients receiving DDAVP, including lower platelet count, worse initial injury severity scores, and hematoma expansion on initial follow up imaging. As previously mentioned, 2 patients in the subgroup received DDAVP after follow-up imaging that did not demonstrate hematoma expansion. These patients were likely sicker at baseline contributing to the use of DDAVP to stop future expansion. It is unclear if DDAVP provides an added benefit after hematoma expansion has already occurred as these patients subsequently developed hematoma expansion after DDAVP administration.
Recent guidelines suggest administering DDAVP 0.4 mcg/kg in patients with antiplatelet-associated ICH; however, in this study the median DDAVP dose was 0.3 mcg/kg. 10 Published outcomes data have assessed both doses of DDAVP and the data does not support 1 dosing regimen over another. 9,13,14 Additionally, adverse effects, including hyponatremia and thrombotic events, were similar in this study compared to previous studies. 12 -16 One of the primary factors that may have influenced the use of DDAVP in patients with alcohol use was their BAL on admission as the DDAVP group had a higher median BAL (DDAVP 207 mg/dL vs non-DDAVP 47.5 mg/dL, P = 0.106). Given the higher median BAL, the concern for platelet dysfunction, potentially during neurosurgery, may have contributed to the decision to administer of DDAVP. An elevated admission BAL does not imply a history of alcohol use as some patients may have presented intoxicated upon admission; therefore, the degree of platelet dysfunction associated with AUD would not be present.
This study has several limitations. As this was a retrospective chart review, we were unable to control for unmeasured variables assessed by the treating clinician. This was a small, single center study and the administration of DDAVP for AU-associated ICH was not protocolized; its use was based on the treating provider’s discretion. DDAVP administration may have been influenced by the higher alcohol level, as well as hematoma expansion despite alternative interventions. The lack of protocolization may have contributed to selection bias where potentially sicker patients received DDAVP. Additionally, several patients were transferred from an outside hospital following initial imaging and laboratory draws. Exact details about these diagnostic procedures (e.g. time of the scan or lab draw) were not always available in the chart; therefore, information had to be extrapolated from chart notes. Identifying patients with AU-associated ICH was challenging given the lack of consistent documentation in the medical record. AUD is defined by a problematic pattern of alcohol consumption with an impaired ability to control or discontinue alcohol use despite adverse social, occupational, physiological, or psychological consequences and not by a blood alcohol level cutoff. 20 Due to the complexity of AUD diagnosis, patients were identified as having alcohol use by obtaining ICD codes, reviewing chart notes, and assessing blood alcohol levels; however, not all patients were confirmed to have AUD. Although, the pragmatic design and inclusion of patients with acute alcohol use and alcohol use disorder may increase the generalizability of the study, due in part, to the emergent use of DDAVP before a detailed social history can be obtained. Several baseline characteristics may have impacted the risk of ICH. Limited literature suggests higher alcohol intake may increase the risk of ICH; however, it is unclear if a dose-dependent relationship exists between alcohol consumption and ICH. 21 -23 Additionally, the risk of ICH in the setting of alcohol-use may also vary among different racial and ethnic groups. 21 The severity of hepatic dysfunction may not have been well-detected using the current coagulation tests and may have also affected the risk of ICH and expansion. 24 -26 Safety endpoints were assessed starting with the initial imaging rather than DDAVP administration. Hyponatremia was not assessed precisely 24 hours after DDAVP administration; however, the time to DDAVP administration was brief (median 3.9 hours). Given the short half-life and prompt administration of DDAVP, this allowed for an adequate evaluation of hyponatremia within 24 hours of initial imaging. Treating providers did not routinely perform screening assessments, and only ordered diagnostic procedures for symptomatic thrombosis. Therefore, the thrombotic complication rate may be underestimated due to limited thrombosis workup. Finally, due to the irregular distribution on imaging, the ICH volume was not quantifiable. The sample contained predominantly traumatic ICH and only a low rate of primary intraparenchymal hemorrhage. Location of the intraparenchymal hemorrhage was not further delineated into lobar, deep, or infratentorial.
Conclusion
There was no difference in hyponatremia, thrombosis, or hematoma expansion in patients who received DDAVP for alcohol use-associated ICH compared with those who did not. Despite the small sample size, this study adds value to the limited evidence assessing the use of DDAVP in alcohol use-associated ICH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.