
Abstract
Introduction
The benefits of extracorporeal membrane oxygenation (ECMO) have been well described among critically ill patients with acute respiratory distress syndrome (ARDS) during the 2009 H1N1 influenza and 2014 Middle East respiratory syndrome (MERS) outbreak.1–5 Early observational studies published from China reported that up to 31% of hospitalized coronavirus disease 2019 (COVID-19) patients and up to 90% of critically ill COVID-19 patients developed ARDS; however, ECMO support was utilized in only 2%-5% of cases.6–9 The Extracorporeal Life Support Organization (ELSO) registry reported 90-day in-hospital mortality up to 40% among 1035 COVID-19 patients requiring ECMO support between January 16, 2020, and May 1, 2020. 10 However, the clinical characteristics and risk factors between survivors and nonsurvivors were not thoroughly examined. Nevertheless, multiple studies have since been published detailing the clinical features and mortality risk factors among COVID-19 patients receiving ECMO support. The 2017 ELSO guidelines describing ECMO support for critically ill patients with refractory respiratory failure were recently updated to the ELSO 2020 COVID-19 guidelines to provide better guidance on clinical decision-making when initiating and managing COVID-19 patients requiring ECMO support.11,12 The purpose of our systematic review and meta-analysis is to discuss the clinical characteristics between survivors and nonsurvivors of COVID-19 patients receiving ECMO support based on the evidence in the existing literature.
Methods
This systematic review was presented in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. PRISMA checklist was provided in the Supplemental Material. Ethical approval and informed consent were not required for this study as it was a systematic review of previously published studies. The protocol for this review was registered and published in the International Prospective Register of Systematic Reviews under reference number CRD42021247852.
Search Strategy and Selection
A literature search was performed through the Pubmed, Cochrane, Embase, Scopus, and Web of Science databases using search terms of “COVID-19,” “severe acute respiratory syndrome coronavirus 2,” “ECMO,” “extracorporeal life support,” “venovenous extracorporeal membrane oxygenation (VV-ECMO),” and “venoarterial extracorporeal membrane oxygenation (VA-ECMO).” Complete search strategies for each database used were provided in Supplemental Material Table 1. We included studies published in peer-reviewed journals between December first, 2019, to June first, 2021. We simultaneously searched the reference lists of all retrieved articles for potentially eligible studies to detect additional studies that met our inclusion criteria. Two authors (W.C. and B.S.) independently reviewed the titles and abstracts of all search results for eligibility. If an article was considered potentially eligible, both authors independently examined the full article for inclusion. A consensus-based discussion resolved disagreements between the authors.
Inclusion Criteria
Articles that met the following criteria were included in our study: (1) all research study types, such as case series, observational studies, and randomized controlled trials (RCTs) that compare the clinical characteristics between survivors and nonsurvivors of COVID-19 patients requiring ECMO support; (2) studies in which diagnosis of COVID-19 infections was made via real time reverse transcription-polymerase chain reaction from nasopharyngeal or oropharyngeal swabs, or lower respiratory tract specimens of endotracheal secretions or bronchoalveolar lavage; and (3) studies published in a peer-reviewed journal.
Exclusion Criteria
The exclusion criteria were specified as follows: (1) articles discussing other infectious outbreaks; (2) studies on animals; (3) in vitro studies; (4) case reports, systematic reviews, literature reviews, editorials, meta-analyses, and opinion articles; (5) studies published in languages other than English were excluded if no translated versions of the manuscript were available.
Data Collection and Synthesis
Two researchers (W.C. and B.S.) independently screened the articles’ full texts for descriptive statistics, reported as means and standard deviations (SDs). The collected data are summarized in Table 1. All-cause in-hospital mortality was used to represent nonsurvivors. If in-hospital mortality was not described among the included studies, but intensive care unit (ICU) mortality was, we accepted ICU mortality rate as the most suitable replacement. We used the lengthiest interval of mortality to determine the in-hospital mortality rate for studies that comprehensively described mortality at different intervals of 28-day, 30-day, 60-day, 90-day, or 180-day. COVID-19 patients who remained hospitalized with and without ECMO support at the end of the respective study follow-up period were excluded from the analysis. Comorbidities were defined as a preexisting history of hypertension, hyperlipidemia, diabetes, malignancy, stroke, peripheral arterial disease, chronic kidney disease, chronic lung disease, chronic liver disease, and coronary artery disease. Thromboembolisms were defined as pulmonary embolism, deep vein thrombosis, and ischemic stroke. Secondary infections were defined as any etiologies of nosocomial/hospital-acquired infections such as pneumonia and bacteremia that required antibiotics administration. Finally, “bleeding” indicated a life-threatening hemorrhage such as an intracranial bleed, pulmonary/pleural hemorrhage, any bleeding requiring intervention, or multiple blood transfusions, or hemorrhagic shock. Any disagreements or discrepancies in the extracted data were resolved via discussion between authors. The primary outcome was the clinical characteristics among COVID-19 survivors and nonsurvivors requiring ECMO support. The secondary outcome was the complication rates between COVID-19 survivors and nonsurvivors included in our meta-analysis.
A Summary of the 16 Studies Included in the meta-Analysis.
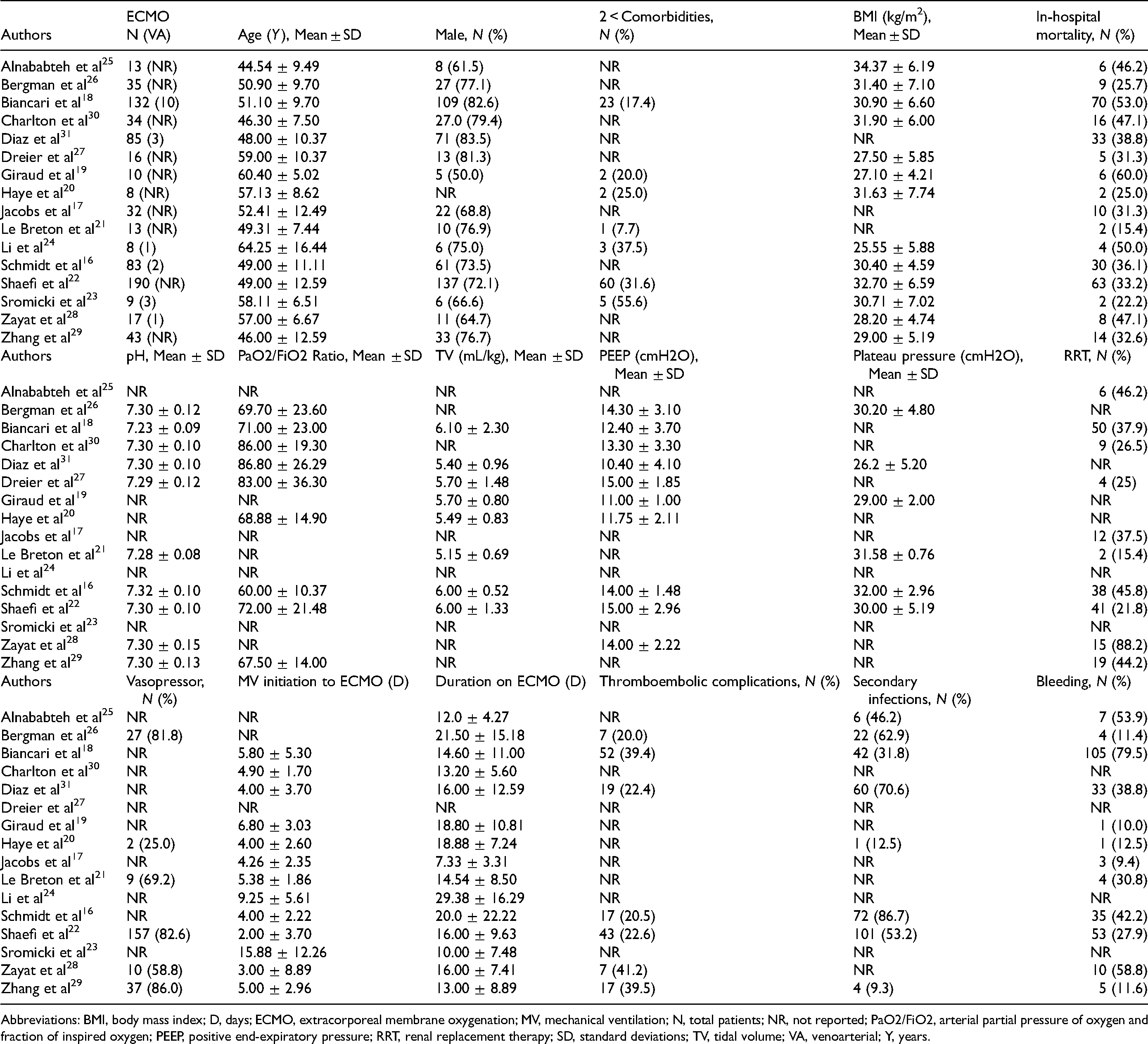
Abbreviations: BMI, body mass index; D, days; ECMO, extracorporeal membrane oxygenation; MV, mechanical ventilation; N, total patients; NR, not reported; PaO2/FiO2, arterial partial pressure of oxygen and fraction of inspired oxygen; PEEP, positive end-expiratory pressure; RRT, renal replacement therapy; SD, standard deviations; TV, tidal volume; VA, venoarterial; Y, years.
Quality Assessment
Studies selected for inclusion were independently assessed for methodological quality by two independent reviewers (W.C. and B.S.) using the 9-item Newcastle-Ottawa Scale (NOS, Table 2). 13 Briefly, the NOS scale assesses three important features of the study such as adequacy of the selection of exposed and nonexposed cohorts, the comparability of groups, and the adequacy of outcomes assessment with a total score ranging from 0 to 9. During the quality assessment of the included studies, any disagreements were resolved by discussion between the authors.
The Table Shows the Results of Newcastle-Ottawa Scale (NOS) 13 Performed for 16 Cohort Studies.
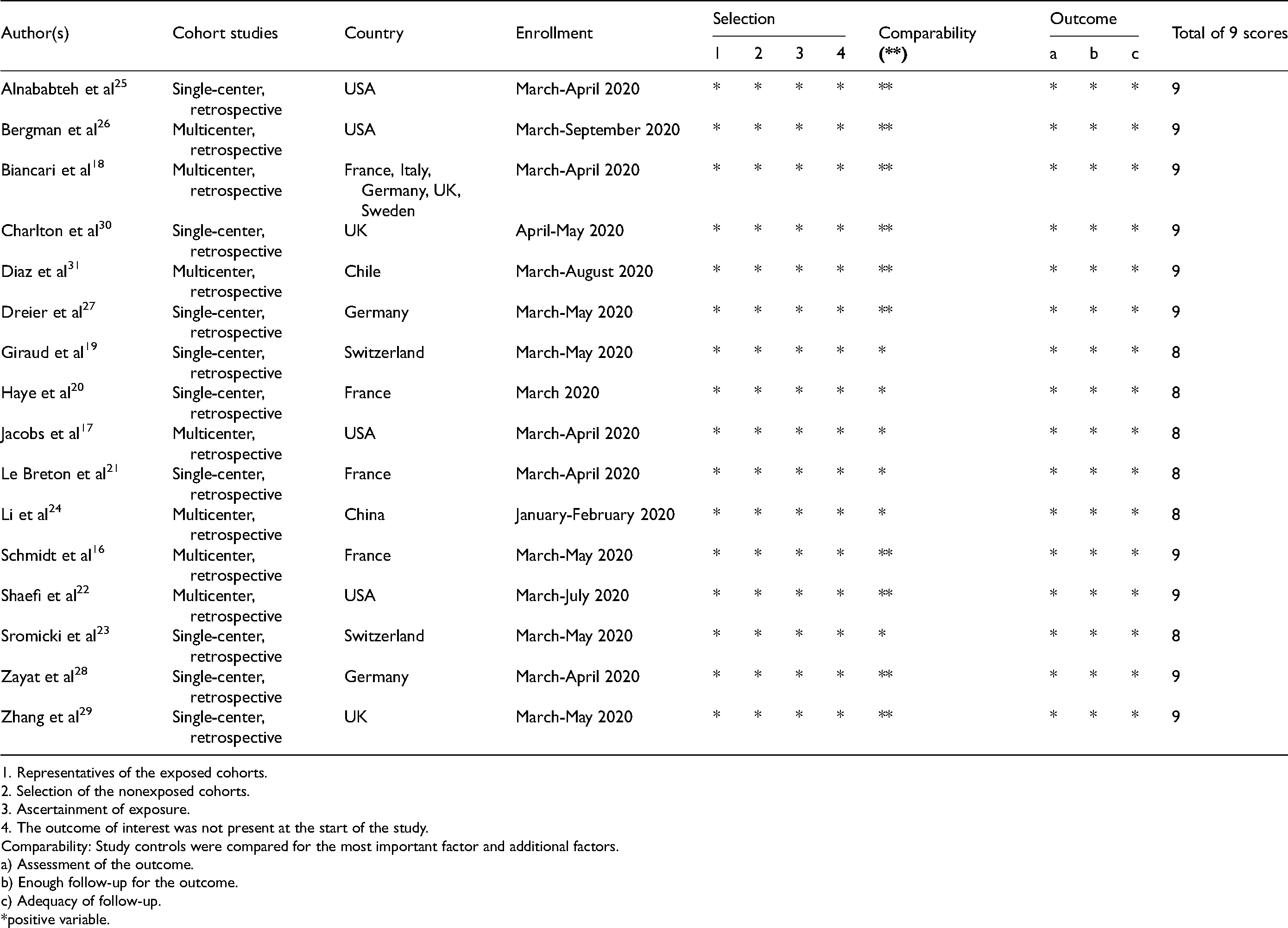
1. Representatives of the exposed cohorts.
2. Selection of the nonexposed cohorts.
3. Ascertainment of exposure.
4. The outcome of interest was not present at the start of the study.
Comparability: Study controls were compared for the most important factor and additional factors.
a) Assessment of the outcome.
b) Enough follow-up for the outcome.
c) Adequacy of follow-up.
*positive variable.
Statistical Analysis
A meta-analysis was performed for the primary and secondary outcomes using the Review Manager (RevMan) software, Version 5.4, The Cochrane Collaboration, 2020. Dichotomous variables were assessed using the Mantel-Haenszel statistical method and measured in odds ratios (ORs). The difference in continuous variables was evaluated by the inverse variance (IV) statistical method and measured in standard mean difference (SMDs). The IV method accounts for differing sample sizes of individual studies by weighting the studies by the variance of their estimates. As a result, small studies with large variance have less weighting, and large studies with small variance have more weighting. Using DerSimonian and Laird’s random-effects model, pooled ORs, SMDs, and 95% confidence intervals (CIs) were calculated, and extracted outcomes were pooled by weighted averages. 14 The random-effects model was preferred over the fixed-effects model as we suspected that clinical heterogeneity might be present due to the variability across the included studies regarding differences in patient population characteristics, criteria for ICU admission, and clinical practices for initiating and managing ECMO support. Statistical heterogeneity among studies was assessed using the I2 statistic. I2 statistics greater than 50% were considered indicative of the presence of substantial heterogeneity. 15 A P value of <.05 was considered statistically significant. Publication bias was examined by visualization inspection of the funnel plot (Supplemental Material Figure 1).
Results
Study Selection
Following the initial search, 3543 studies were identified (Figure 1). Following methodological quality assessment, 16 eligible articles involving cohort studies were included in the meta-analysis. The summary of the risk of bias in each of the included studies is listed in Table 2. Their overall quality was good, with ten cohorts had quality scores of 9/9, and the remaining six cohorts had quality scores of 8/9.
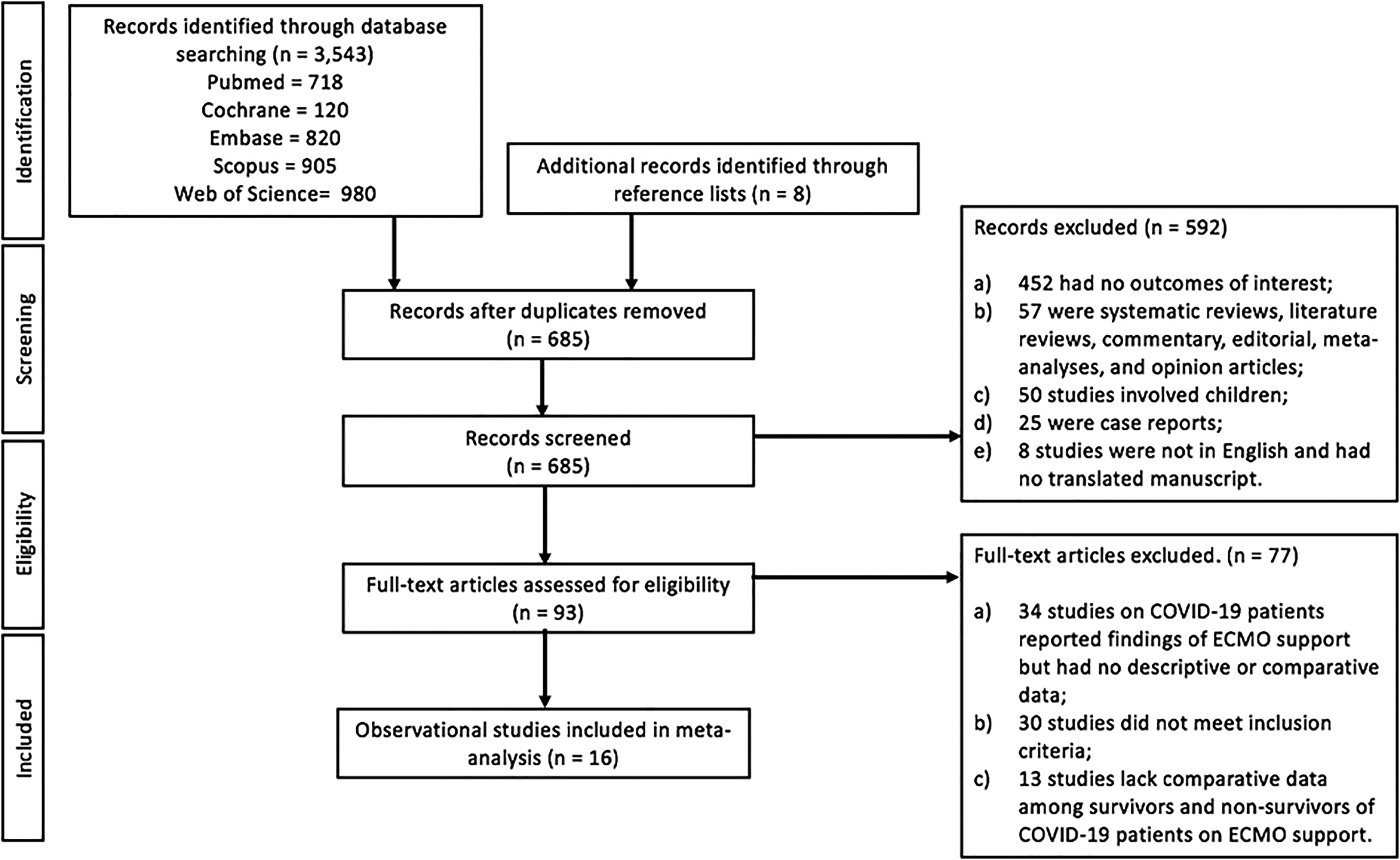
Flow diagram of study selection.
Study Characteristics
A total of 728 COVID-19 patients requiring ECMO support from 16 retrospective cohort studies were assessed (Table 1). Only 3% (20/728) of COVID patients received VA-ECMO and the overwhelming majority received VV-ECMO. However, comparative data on survival was present in 97% (706/728) COVID-19 patients on ECMO support. We excluded 22 COVID-19 patients who were still alive and remained in the ICU with or without ECMO support during the end of the follow-up period.16,17 Among COVID-19 patients on ECMO support included, 60% (426/706) survived, and the remainder, 40% (280/706), did not survive.
Age, Gender, and Comorbidities
COVID-19 patients requiring ECMO support who survived were younger (mean 51.28 vs 55.15 years; SMD − 0.45; 95% CI [ − 0.61, − 0.29]; I2 = 0%; P < .001) than nonsurvivors (Figure 2). No difference in gender was observed between COVID-19 survivors and nonsurvivors requiring ECMO support (OR 0.72; 95% CI 0.50-1.03; I2 = 26%; P = .07) (Figure 3). Seven studies reported data on COVID-19 patients suffering from two and more comorbidities (Figure 3).18–24 COVID-19 patients requiring ECMO support with less than two comorbidities had lower mortality (23% vs 31%; OR 0.55; 95% CI 0.34-0.90; I2 = 0%; P = .02) than those with two and more comorbidities. 12 cohorts contained comparative body mass index (BMI) data for COVID-19 survivors and nonsurvivors receiving ECMO support (Figure 2).16,18–20,23–29 The BMI was comparable among COVID-19 survivors and nonsurvivors requiring ECMO support (mean 30.07kg/m2 vs 30.86kg/m2, SMD 0.06; 95% CI [ − 0.23, 0.34]; I2 = 43%; P = .70).
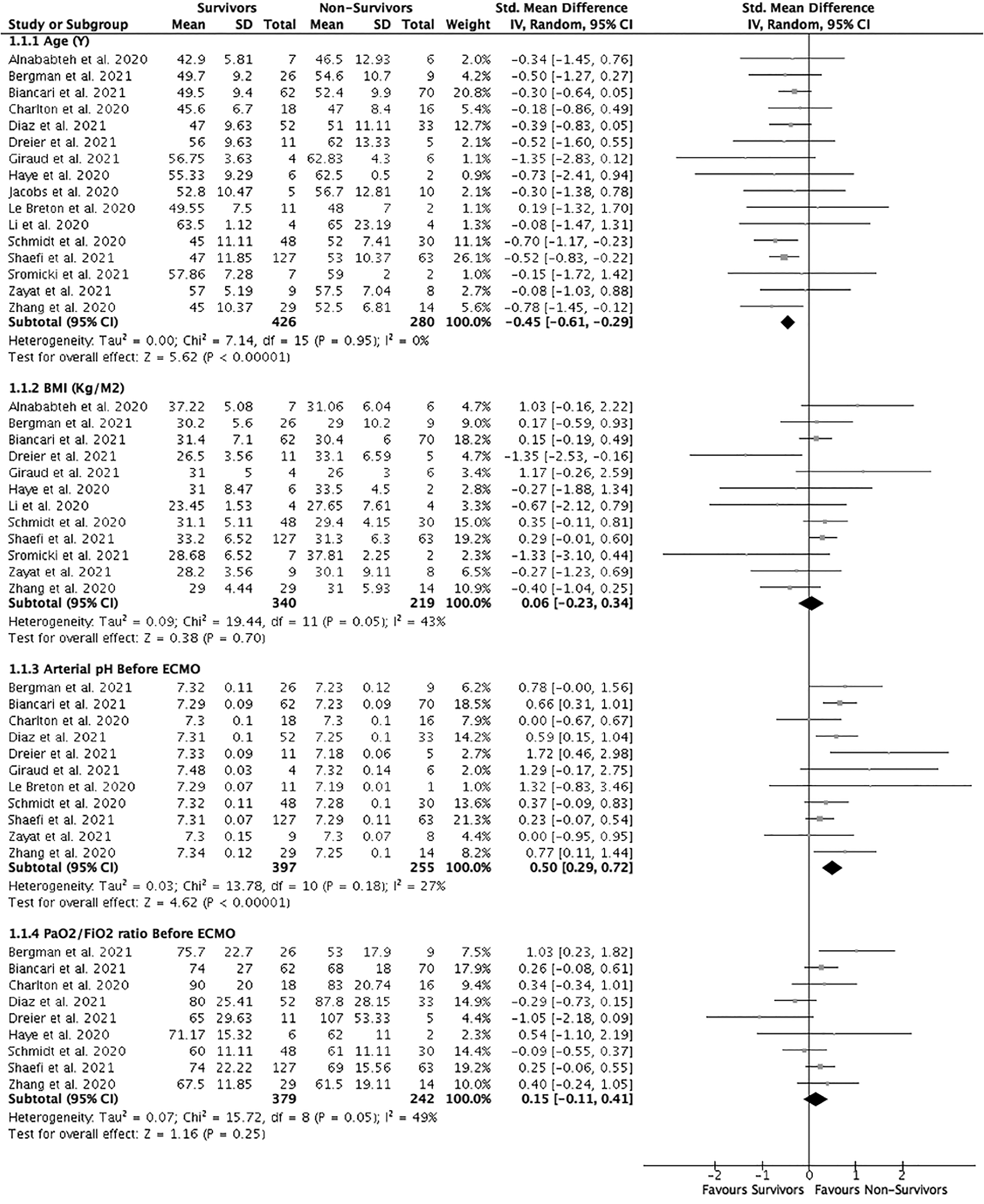
Forrest plot of COVID-19 patients requiring ECMO support divided into survivors versus nonsurvivors. Clinical characteristics of age, BMI, pre-ECMO (24 h before ECMO support initiation) arterial pH and PaO2/FiO2 ratio were assessed. Standard mean differences were calculated by the inverse variance statistical method with a random-effects model.
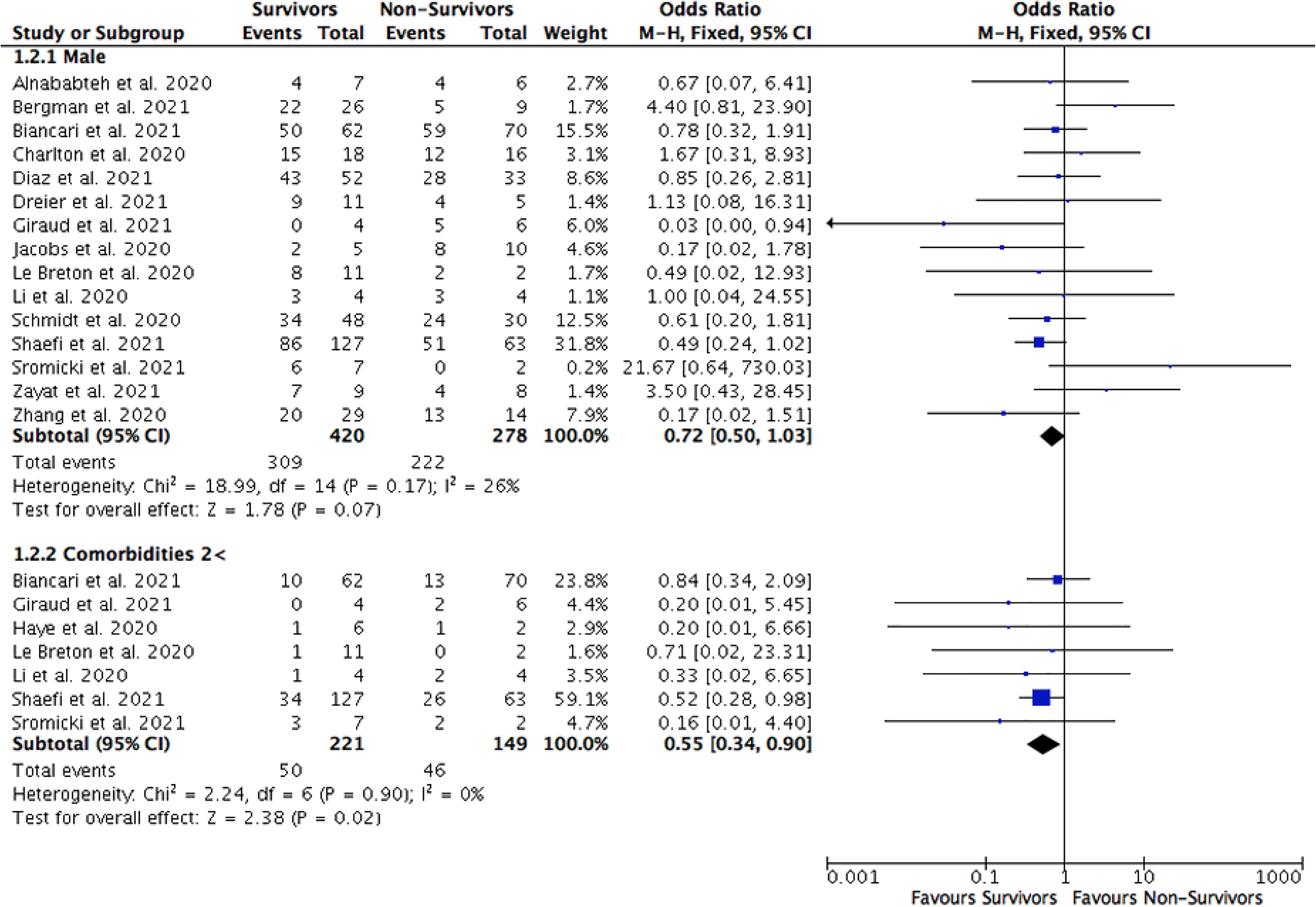
Forrest plot of COVID-19 patients requiring ECMO support divided into survivors versus nonsurvivors. Clinical characteristics of age, and 2 and more comorbidities were assessed. The odds ratio was calculated by the Mantel-Haenszel method with a random-effects model.
Total Days on Mechanical Ventilation (MV) Before ECMO Support Initiation and ECMO Duration
According to 13 cohorts, the duration of MV before ECMO support initiation in COVID-19 patients were comparable (mean 5.51 vs 6.68 days; SMD − 0.19; 95% CI [ − 0.44, 0.05]; I2 = 39%; P = .12) among survivors and non survivors (Figure 4).16–24,28–31 In 13 cohorts, the total duration of ECMO support received by COVID-19 patients was similar (mean 15.39 vs 16.62 days; SMD − 0.07; 95% CI [ − 0.30, 0.15];I2 = 15%; P = .51) between survivors and nonsurvivors (Figure 4).17–26,28–30
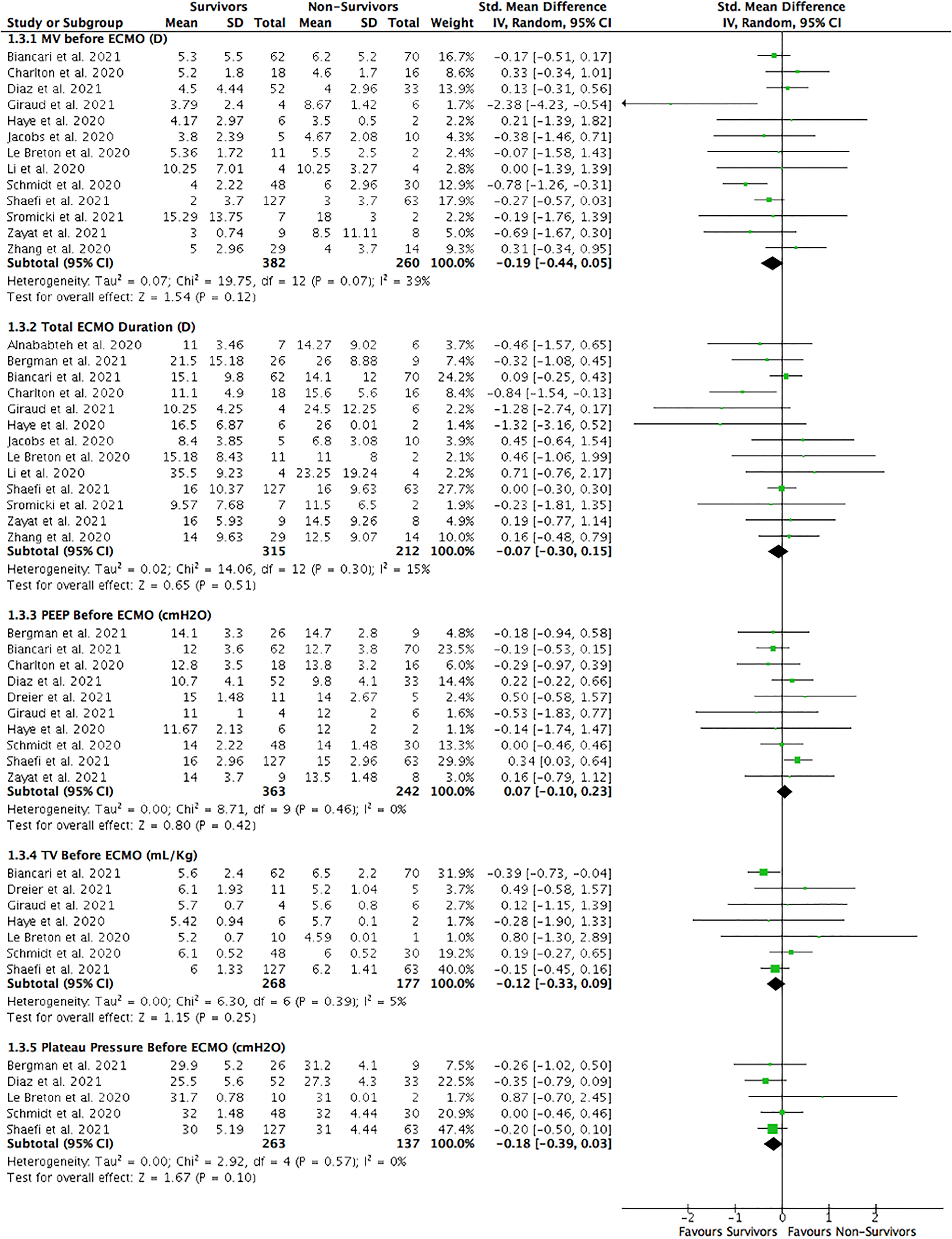
Forrest plot of COVID-19 patients requiring ECMO support divided into survivors versus nonsurvivors. Clinical characteristics of the duration of mechanical ventilation before ECMO support initiation, total ECMO support duration, pre-ECMO (24 h before ECMO support initiation) parameters of positive end-expiratory pressure, tidal volume, and plateau pressure were assessed. Standard mean differences were calculated by inverse variance statistical method with a random-effects model.
Respiratory Parameters Within 24 h Before ECMO Support Initiation
Multiple parameters such as pH, partial pressure of arterial oxygen over fraction al inspired oxygen (PaO2/FiO2) ratio, tidal volume (TV) in mL/kg, positive end-expiratory pressure (PEEP), and plateau pressure were assessed in COVID-19 patients within 24 h before ECMO support initiation (Table 1). According to 11 cohorts, arterial pH was higher (mean 7.33 vs 7.26; SMD 0.50; 95% CI [0.29-0.72];I2 = 27%; P < .001) among survivors than nonsurvivors before ECMO support initiation (Figure 2).16,18,19,21,22,26–31 In nine cohorts, the PaO2/FiO2 ratio was similar (mean 73.04 vs 72.48; SMD 0.15; 95% CI [ − 0.11, 0.41];I2 = 49%; P = .25) between COVID-19 survivors and nonsurvivors requiring ECMO support (Figure 2).16,18,20,22,26,27,29–31 Before ECMO support initiation, ten studies demonstrated that PEEP was equal (mean 13.13 vs 13.15 cmH20; SMD 0.07; 95% CI [ − 0.10, 0.23];I2 = 0%; P = .42) in both COVID-19 survivors and nonsurvivors (Figure 4).16,18–20,22,26–28,30,31 Among seven studies describing TV before ECMO support initiation, no difference (mean 5.63 vs 5.68 mL/kg; SMD − 0.12; 95% CI [ − 0.33, 0.09];I2 = 5%; P = .25) in TV was observed between survivors and nonsurvivors (Figure 4).16,18,19,21,22,27 Lastly, five studies reported comparable plateau pressure (mean 29.82 vs 30.5 cmH20; SMD − 0.18; 95% CI [ − 0.39, 0.03];I2 = 0%; P = .10) among COVID-19 survivors and nonsurvivors before ECMO support initiation (Figure 4).16,21,22,26,31
Renal Replacement Therapy (RRT) and Vasopressor Requirement
Nine studies reported that COVID-19 survivors requiring ECMO support needed less RRT (21% vs 39%; OR 0.41; 95% CI 0.21-0.78;I2 = 33%; P = .007) than nonsurvivors (Figure 5).16–18,21,22,25,27–29 COVID-19 survivors requiring ECMO support also required less vasopressors (76% vs 92%; OR 0.35; 95% CI 0.16-0.76;I2 = 0%; P = .008) than nonsurvivors although the data were limited to six observational studies (Figure 5).20–22,26,28,29
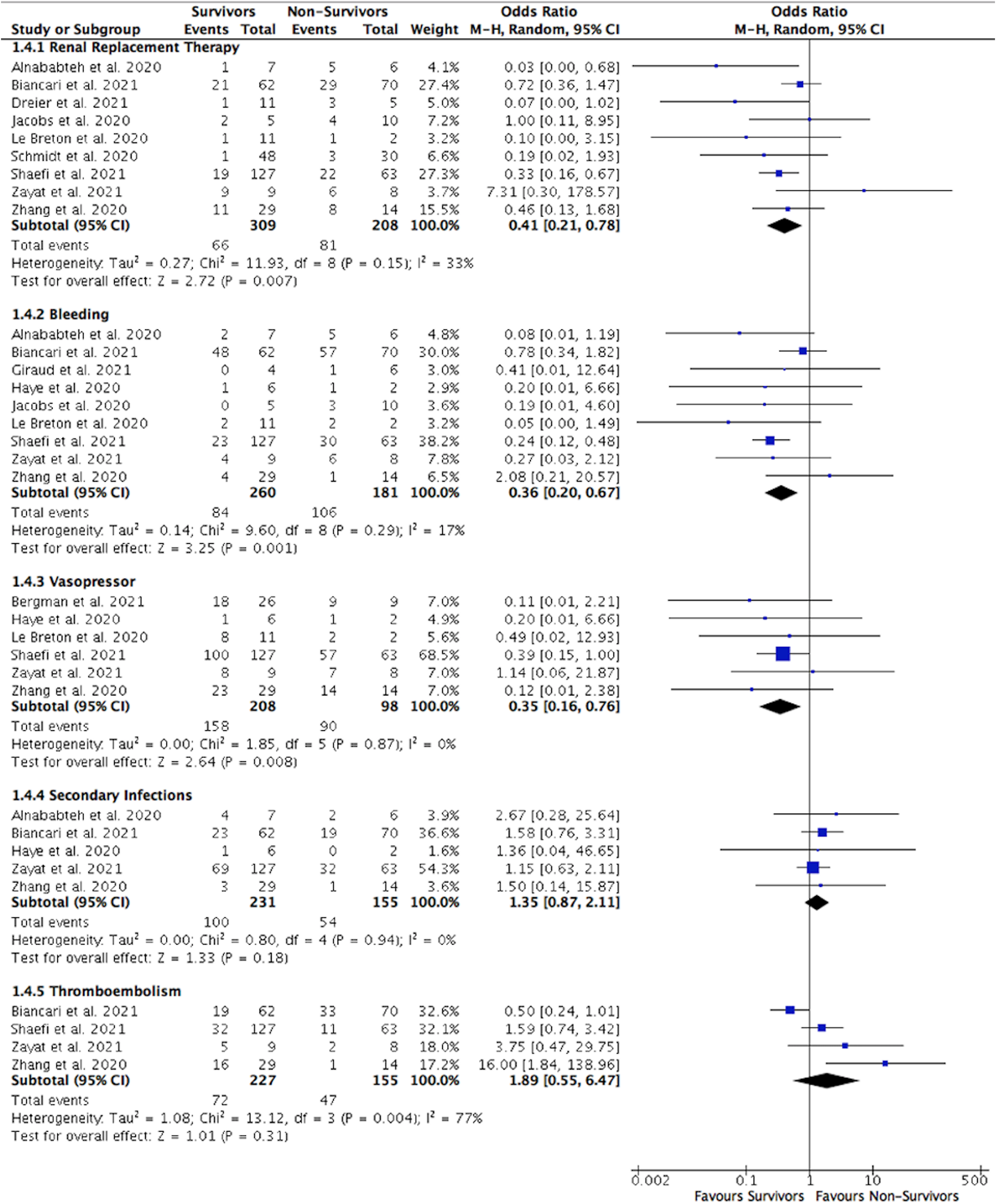
Forrest plot of COVID-19 patients requiring ECMO support divided into survivors versus nonsurvivors. Renal replacement therapy, vasopressor requirement, and complications of bleeding, thromboembolism, and secondary infections were assessed. The odds ratio was calculated by the Mantel-Haenszel method with a random-effects model.
Complications
Three major complications categories were included in the meta-analysis: bleeding, secondary infections, and thromboembolism (Table 1). According to nine studies, the rate of bleeding complications was lower (32% vs 59%; OR 0.36; 95% CI 0.20-0.67;I2 = 17%; P = .001) among COVID-19 survivors requiring ECMO support than nonsurvivors (Figure 5).17–22,25,28,29 Five studies reported that COVID-19 survivors and nonsurvivors requiring ECMO support had comparable (43% vs 35%; OR 1.35; 95% CI 0.87-2.11;I2 = 0%; P = .18) secondary infections rate (Figure 5).18,20,25,28,29 Lastly, the rate of thromboembolism was similar (32% vs 30%; OR 1.89; 95% CI 0.55-6.47;I2 = 77%; P = .31) between survivors and nonsurvivors of COVID-19 requiring ECMO support in four studies (Figure 5).18,22,28,29
Discussion
The right timing and patient selection criteria of escalating care to ECMO support in critically ill COVID-19 patients remain challenging. In the 16 studies involving 706 COVID-19 patients requiring ECMO support, we found an aggregate mortality rate of 40%. Considering the role of ECMO support as a last resort salvage modality in critically ill patients on the verge of death, survival exceeding 50% should be viewed as an encouraging finding. COVID-19 patients requiring ECMO support who died suffered from advanced age, multiple (two and more) comorbidities, and had a more significant requirement of vasopressor and RRT than survivors. COVID-19 survivors and nonsurvivors requiring ECMO support had comparable clinical characteristics of gender and BMI. The duration of MV before ECMO support initiation and the total number of ECMO support days were also similar among these patients. Pre-ECMO pH was lower among nonsurvivors than survivors, but other pre-ECMO respiratory parameters such as PaO2/FiO2 ratio, TV, PEEP, and plateau pressure were no different. Furthermore, a lower rate of bleeding complications was observed in survivors than nonsurvivors requiring ECMO support. However, the rate of thromboembolism and secondary infections was no different.
Advanced age (64 years and older) is a risk factor for poor outcomes among hospitalized COVID-19 patients.32,33 According to the ELSO international multicenter registry, younger non-COVID-19 patients (age 50 and less) receiving ECMO support had a slightly better survival rate (OR: 0.98; 95% CI, 0.974-0.993; P < .001) than older patients. 34 In our meta-analysis, COVID-19 nonsurvivors requiring ECMO support were older (mean 55.15 vs 51.28 years; P < .001) than survivors. The 2017 ELSO guidelines for ECMO support listed advanced age as a relative contraindication, although no specific age cutoff was recommended. 11 The most recent 2020 ELSO guidelines were more specific in defining advanced age as 65 and older. 12 Unsurprisingly, hospitalized COVID-19 patients with multiple comorbidities have a higher mortality rate, as observed in multiple large observational studies.32,33 Similarly, in our meta-analysis, we identified multiple comorbidities as a mortality predictor in the ECMO population. This is consistent with the 2017 and 2020 ELSO guidelines in which disabling neurological diseases, immunodeficiency, malignancy, advanced lung, liver, and kidney diseases were listed as contraindications.11,12
According to a meta-analysis by Peckham et al although men and women were equally likely to be diagnosed with COVID-19 infections, men, in general, had a 3-fold increased risk of requiring ICU admission and a 1.5-fold increased risk of death compared to women. 35 In our meta-analysis, gender was not associated with poor outcomes (OR 0.72; P = .07) among COVID-19 patients requiring ECMO support. Obesity, present in up to 33% of hospitalized COVID-19 patients, has been shown to increase disease severity (OR 3.13; P < .01) and mortality (OR 1.36; P < .01). 36 The 2020 ELSO COVID-19 guidelines recommended against ECMO initiation in COVID-19 patients with BMI above 40 kg/m2. 12 We found no difference in BMI (mean 30.07 kg/m2 vs 30.86 kg/m2, P = .70) between COVID-19 patients survivors and nonsurvivors requiring ECMO support.
Although both the 2017 ELSO and the updated 2020 ELSO COVID-19 guidelines recommended against ECMO support if patients have received MV for more than 7 to 10 days,11,12 many centers do not consider time on ventilation to be a contraindication.37,38 The two largest RCTs assessing critically ill non-COVID-19 patients with refractory hypoxic respiratory failure requiring ECMO (Peek et al and Combes et al) excluded patients receiving MV for more than seven days.39,40 Furthermore, Combes et al observed that patients who received early ECMO support (within three days after onset of ARDS) had a lower death rate (43% vs 65%; P < .05) than those who received late ECMO support. 40 Moreover, large observational studies suggested that the longer the ECMO support duration, the higher the mortality: up to 30% at one week and 60% at one month.34,38 However, our meta-analysis demonstrated that the duration of MV before ECMO support initiation was similar (mean 5.51 vs 6.68 days; P = .12) among survivors and nonsurvivors requiring ECMO support, although the mean duration of MV was less than ten days. The strict adherence to 2017 and 2020 ELSO guidelines may have played a significant role in COVID-19 patient selection for ECMO support.11,12 More research is required to determine the association between the duration of MV before ECMO support initiation and mortality. According to our meta-analysis, the total duration of ECMO support (mean 15.39 vs 16.62 days; P = .51) was no different between COVID-19 survivors and nonsurvivors. Nevertheless, the overall length of ECMO support in our meta-analysis was longer compared to historical data from the H1N1 influenza A (9.6 ± 0.6 days) and MERS (10.5 ± 4.5 days) epidemics despite a lower fatality rate observed in COVID-19 patients. 41 The longer duration of ECMO support among COVID-19 patients could be explained by the advancement in lung-protective ventilation strategy, immunomodulatory therapies, and unique atypical COVID-19 phenotype, in which COVID-19 patients take longer to reach a point of clinical decompensation due to significant gas exchange derangements with relatively preserved lung compliance.42–44
Pre-ECMO respiratory parameters such as pH, PaO2/FiO2 ratio, TV, PEEP, and plateau pressure may help determine outcomes among critically ill patients. Recent large observational studies reported that in critically ill COVID-19 patients, with lower pH and PaO2/FiO2 ratio and higher TV, PEEP, and plateau pressure were associated with greater disease severity and unfavorable outcome.45–47 Both the 2017 ELSO and updated 2020 ELSO COVID-19 guidelines recommended ECMO initiation if either PaO2/FiO2 ratio < 60 to 100, or PaO2/FiO2 ratio <150 and pH < 7.2 with PaCO2 > 80 mm Hg, despite FiO2 of 90% and higher after six hours of optimal lung recruitment attempts involving proning, neuromuscular blockade, PEEP augmentation, and inhaled pulmonary vasodilators.11,12 In our meta-analysis, we found that higher serum pre-ECMO pH was more common (mean 7.33 vs 7.26; P < .001) among COVID-19 survivors requiring ECMO support than nonsurvivors, but PaO2/FiO2 ratio and other ventilatory parameters were not. Although not all ventilatory parameters and partial pressure of arterial carbon dioxide before ECMO support initiation were provided in most studies, we believe COVID-19 nonsurvivors had greater disease severity with refractory respiratory, severe metabolic derangements, and hemodynamic instability based on the higher requirements of RRT and vasopressors.
Many complications (eg, bleeding, thromboembolism, secondary infections) have been described in hospitalized COVID-19 patients. Those increase in frequency among critically ill patients.10,48,49 Furthermore, the incidence of these complications rises while on ECMO support in the setting of prolonged intubation, continuous requirement for anticoagulant infusion, chronic indwelling large-bore ECMO catheters, and prothrombotic environment within the extracorporeal circuit.50,51 A meta-analysis in 2014 demonstrated that significant bleeding was more common among critically ill non-COVID-19 patients receiving ECMO support (OR 11.44; P < .05) than those not receiving ECMO support. 52 However, no difference was observed in secondary infections. A RCT study of critically ill non-COVID-19 patients by Combes et al in 2019 reported that major bleeding events were higher in the ECMO support group than the control group (46% vs 28%; 95% CI 6.0-30.0), but no increase in the risk of secondary infections were observed. 40 An observational study by Hartley et al reported that, although the incidence of thromboembolism was high in 290 critically ill non-COVID-19 patients receiving ECMO support, survival rates were similar among these patients. 53 Two observational studies reported an increased frequency of developing secondary infections among non-COVID-19 ECMO patients with refractory hypoxic respiratory failure requiring prolonged cannulation, but no difference in the length of stay or in-hospital mortality was noted.54,55 According to our meta-analysis, major bleeding was less frequently observed in survivors (OR 0.36; P = .001) than nonsurvivors requiring ECMO support, but thromboembolic and secondary infections complications were similar.
Some common intrinsic pitfalls can affect any meta-analysis, including this one. Heterogeneity of an aggregate cohort is a property indicating dissimilarities between the separate study populations (selection, protocols, local standards). Significant differences can render the conclusions of a meta-analysis questionable. Due to the variability in data collected and reported among the various COVID-19 ECMO studies included, we used a broad definition for comorbidities and assessed those with two and more comorbidities, and complications of bleeding, secondary infections, and thromboembolisms to avoid overlooking important findings from these studies. We statistically evaluated the heterogeneity of the examined outcomes and found no concerning levels across most parameters. Even though the nature of the studies was primarily observational, publication bias is possible. The funnel plot (Supplemental Material Figure 1) demonstrated symmetry using the most common clinical characteristics described among studies indicating a low probability of publication bias. The noncontrolled nature of the intervention may also introduce a selection bias. The results of our study are likely to represent COVID-19 patients receiving VV-ECMO support due to the low number of patients receiving VA-ECMO support which preclude making a distinction between these two groups.
Conclusion
Our meta-analysis findings demonstrated that more than half of COVID-19 patients survived when ECMO support was used as rescue therapy. Further perfecting the technology and protocols will only improve outcomes in the future. Advanced age, multiple comorbidities, lower pre-ECMO pH, the requirement of either RRT or vasopressors are predictive of death. Gender, BMI, the total ECMO support duration and duration of MV to ECMO support initiation, pre-ECMO PaO2/FiO2 ratio, and other ventilatory parameters are not associated with poor outcomes. Bleeding complications were common in nonsurvivors than survivors, but the rate of thromboembolism and secondary infections was similar among COVID-19 patients requiring ECMO support. Our findings align with the ELSO COVID-19 guidelines relating to the contraindications to ECMO support in critically ill patients. Although the duration of MV before ECMO support initiation was similar between survivors and nonsurvivors requiring ECMO support, the mean duration of MV remained less than 10 days. As our knowledge continues to grow during the pandemic with increasing use of ECMO support among critically ill COVID-19 patients, more data will likely become available on those receiving VA-ECMO support. Our meta-analysis results can have significant implications for patient selection and can be a helpful tool in the decision-making on managing critically ill COVID-19 patients with ARDS.
Supplemental Material
sj-docx-1-jic-10.1177_08850666211045632 - Supplemental material for Clinical Characteristics Between Survivors and Nonsurvivors of COVID-19 Patients Requiring Extracorporeal Membrane Oxygenation (ECMO) Support: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jic-10.1177_08850666211045632 for Clinical Characteristics Between Survivors and Nonsurvivors of COVID-19 Patients Requiring Extracorporeal Membrane Oxygenation (ECMO) Support: A Systematic Review and Meta-Analysis by Woon Hean Chong, Biplab K. Saha and Boris I. Medarov in Journal of Intensive Care Medicine
Supplemental Material
sj-tiff-2-jic-10.1177_08850666211045632 - Supplemental material for Clinical Characteristics Between Survivors and Nonsurvivors of COVID-19 Patients Requiring Extracorporeal Membrane Oxygenation (ECMO) Support: A Systematic Review and Meta-Analysis
Supplemental material, sj-tiff-2-jic-10.1177_08850666211045632 for Clinical Characteristics Between Survivors and Nonsurvivors of COVID-19 Patients Requiring Extracorporeal Membrane Oxygenation (ECMO) Support: A Systematic Review and Meta-Analysis by Woon Hean Chong, Biplab K. Saha and Boris I. Medarov in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-3-jic-10.1177_08850666211045632 - Supplemental material for Clinical Characteristics Between Survivors and Nonsurvivors of COVID-19 Patients Requiring Extracorporeal Membrane Oxygenation (ECMO) Support: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-jic-10.1177_08850666211045632 for Clinical Characteristics Between Survivors and Nonsurvivors of COVID-19 Patients Requiring Extracorporeal Membrane Oxygenation (ECMO) Support: A Systematic Review and Meta-Analysis by Woon Hean Chong, Biplab K. Saha and Boris I. Medarov in Journal of Intensive Care Medicine
Footnotes
Author Contributions
WHC contributed to conceptualization, methodology, investigation, data curation, writing—original draft. BKS, contributed to conceptualization, methodology, investigation, data curation, writing—review and editing. BIM, contributed to conceptualization, methodology, investigation, data curation, supervision, project administration, writing—review and editing.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.