
Abstract
Objective
To study coronary interventions and mortality among patients with ST-elevated myocardial infarction (STEMI) who were admitted with septic shock.
Methods
Data from the national emergency department sample (NEDS) that constitutes 20% sample of hospital-owned emergency departments in the United States was analyzed for the septic shock related visits from 2016 to 2018. Septic shock was defined by the ICD codes.
Results
Out of 1 375 507 adult septic shock patients, 521 300 had a primary diagnosis of septic shock (mean age 67.41±15.67 years, 51.1% females) in the national emergency database for the years 2016 to 2018. Of these patients, 2768 (0.53%) had STEMI recorded during the hospitalization. Mortality rates for STEMI patients were higher than patients without STEMI (52.3% vs 23.5%). Mortality rates improved with PCI among STEMI patients (43.8% vs 56.2%). Coronary angiography was performed among 16% of patients of which percutaneous coronary intervention (PCI) rates were 7.7% among patients with STEMI septic shock. PCI numerically improved mortality, however, had no significant difference than patients without PCI on multivariate logistic regression and univariate logistic regression post coarsened exact matching of baseline characteristics among STEMI patients. Among the predictors, STEMI was a significant predictor of mortality in septic shock patients (OR 2.87, 95% CI 2.37-3.49; P<.001). Age, peripheral vascular disease, were predominant predictors of mortality in STEMI with septic shock subgroup (P <.001). Pneumonia was the predominant underlying infection among STEMI (36.4%) and without STEMI group (29.5%).
Conclusion
STEMI complicating septic shock worsens mortality. PCI and coronary angiography numerically improved mortality, however, had no significant difference from patients without PCI. More research will be needed to improve mortality in such a critically ill subgroup of patients.
Introduction
Sepsis is a major health care burden in the United States and yearly 1.7 million hospitalizations are reported secondary to sepsis.1,2 A significant number of such patients have severe sepsis and septic shock which represent approximately 2% of hospitalizations of which half are admitted to intensive care units.3,4 Septic shock has been reported with a high mortality rate of up to 38%. 5 Patients with septic shock having multiorgan failure are predisposed to complications including ST-elevated myocardial infarction (STEMI) which can worsen the survival outcomes. STEMI has been reported with a mortality rate of up to 12.8% in the general population. 6 Myocardial dysfunction during septic shock has been reported to worsen the mortality outcomes.7–9
To our knowledge, there are no previous studies are available which have evaluated outcomes of patients with a STEMI and septic shock. Few cases have reported STEMI complicating septic shock with resultant emergent coronary angiography and intervention as per requirement.10–12
Data regarding the trend, outcomes, and predictors of mortality in patients with septic shock with and without STEMI could provide information for improving health care approaches and policymaking for these patients. Currently, very limited knowledge is available regarding STEMI outcomes in patients with septic shock. Therefore, we aimed to examine the predictors, and mortality outcomes of septic shock patients with STEMI for the years 2016 to 2018 in the national emergency department sample database.
Methods
Study Population and Design
We performed an observational retrospective cohort study of patients that had septic shock and were diagnosed with STEMI during the hospitalization for the years 2016 to 2018 in the National Emergency Department Sample (NEDS) database. The NEDS constitutes an approximately 20% sample of hospital-owned emergency departments in the United States. 13 Using a stratified, random sampling design, a sample of hospital-owned emergency departments from the United States participating in both the State Inpatient Databases (SID) and the State Emergency Department Databases (SEDD) was selected, and 100% of the emergency department visits from the selected hospital-owned ED were retained. Hospitals were included in the NEDS sample based on geographic region (northeast, mid-west, west, or south), location (urban or rural), teaching status (teaching or non-teaching), ownership (public, private not for-profit, private for profit), and Trauma Center Designation. A total of 950 EDs are included in NEDS. From each selected ED, all visits were included, which amounted to more than 33 million unweighted visits each year. Patients with age < 18 years were excluded at the time of data extraction from the NEDS database. The study was exempt from institutional review board evaluation as it was based on the national emergency database, however, it was performed according to the ethical criteria set up by Healthcare Cost and Utilization Project (HCUP). 13
Study Definitions
Septic shock was defined with the International Classification of Diseases, Tenth Edition, (ICD-10) code “R65.21.” Only patients with a primary diagnosis of septic shock were included in the study. We excluded patients younger than 18 years, and patients with missing data. Based on this exclusion we identified 521 300 adult septic shock which included 2768 (0.53%) patients who had STEMI during the hospitalization. We generated STEMI using ICD-10 codes “I21.01,” “I21.02,” “I21.09,” “I21.11,” “I21.19,” “I21.21,” “I2129,” “I21.3,” “I22.8,” and “I22.0.”
Patient and Hospital Characteristics
Baseline patient demographic characteristics (age, sex, and insurance payer) were extracted. Diagnostic codes were used to identify the comorbidities of hypertension, diabetes mellitus, obesity, congestive heart failure, smoking, hyperlipidemia, prior myocardial infarction, prior PCI, prior coronary artery bypass grafting, cerebrovascular disease, peripheral vascular disease (PVD), chronic obstructive pulmonary disease (COPD), malignancy, chronic kidney disease, atrial fibrillation using ICD-10 codes. Elixhauser comorbidity index codes were also used to extract the comorbidities. 14 We extracted the rates of coronary procedures among patients with and without STEMI septic shock. Cardiovascular interventions were defined by ICD-10 procedural classification system (PCS) codes and current procedure terminology codes (CPT) codes. The interventions included coronary angiography and percutaneous coronary intervention. We extracted major types of infections associated with each group which included pneumonia, urosepsis (urogenital infections), osteomyelitis, cellulitis, infective endocarditis using ICD-10 codes.
Outcomes
The primary outcome of our study was mortality from STEMI and septic shock. We evaluated the effects of coronary interventions on mortality among STEMI septic shock patients. We evaluated the underlying infections associated with STEMI and without STEMI septic shock patients.
Statistical Methods
Categorical variables were expressed as weighted values along with percentages while continuous variables were expressed as mean ± standard deviation if the variable was normally distributed otherwise as median with 25th and 75th percentiles. Descriptive statistics were performed for demographics and comorbidities which were stratified by STEMI and without STEMI septic shock. We used survey statistics to calculate Pearson's chi-square test for categorical variables and t-test for the continuous variables. We calculated the proportion of PCI and coronary angiography performed among the STEMI and patients without STEMI septic shock. We then computed the odds ratio (OR) with 95% confidence interval (CI) for the association of STEMI with mortality in multivariable-adjusted logistic regression model1 adjusted for age, hypertension, diabetes mellitus, hyperlipidemia, obesity, liver dysfunction, prior-myocardial infarction, sex, smoking, congestive heart failure, peripheral vascular disease (PVD), chronic obstructive pulmonary disease (COPD), renal failure, atrial fibrillation, teaching hospital, urban location of the hospital, and insurance status. We also calculated OR and 95% CI in a multivariate logistic regression adjusted for model2 which included model1, and sequential addition of PCI and coronary angiography. To overcome the confounding effects of baseline characteristics we did coarsened exact matching for the model1 variables to evaluate effects of coronary angiography and PCI on mortality among STEMI septic shock patients (Supplemental Digital Content—Table 1). 15 We also performed sensitivity analysis by excluding patients who had a short length of hospital stay to avoid confounding effects from early death shortly after admission.
Subgroup analyses of mortality were performed for STEMI patients in whom coronary procedures were performed. We also evaluated the underlying infection associated with STEMI and without STEMI septic shock patients. The proportions were compared using Pearson's chi-square test.
We calculate the median length of hospital stay for patients among the STEMI subgroup who had coronary angiography. All analyses were weighted analyses. Statistical analysis was performed using STATA version 16.1 (College Station, Texas). All P values were 2 sided, with a significance threshold of P < .05.
Results
A total of 1 375 507 adult septic shock patients were recorded in the national emergency database for the years 2016 to 2018. Out of these patients, 521 300 (mean age 67.41 ± 15.67 years, 51.1% females) had a primary diagnosis of septic shock recorded during the hospitalization. Of these 2768 (0.53%) had STEMI recorded during the hospitalization (Figure 1). Baseline characteristics of the patients with a diagnosis of septic shock with and without STEMI are given in Table 1. STEMI patients were more likely to be elderly and males. STEMI patients had a higher prevalence of prior myocardial infarction, prior history of PCI, history of stroke, liver diseases, and congestive heart failure compared to without STEMI septic shock patients. Pneumonia was the most common infection among STEMI (36.4%) and without STEMI (29.5%) septic shock patients (Figure 2). STEMI patients had higher number of coronary angiographies (n = 441, 16%) than patients without STEMI septic shock (n = 4975, 0.96%). Higher number of percutaneous coronary interventions were done in STEMI septic shock patients (n = 213, 7.71%) than in patients without STEMI septic shock (n = 1054, 0.2%). Medicare was the primary payor for STEMI and without STEMI septic shock patients. A significant number of patients had a disposition to hospice among STEMI septic shock (51.4%) and without STEMI septic shock (20.5%) among the alive discharges.
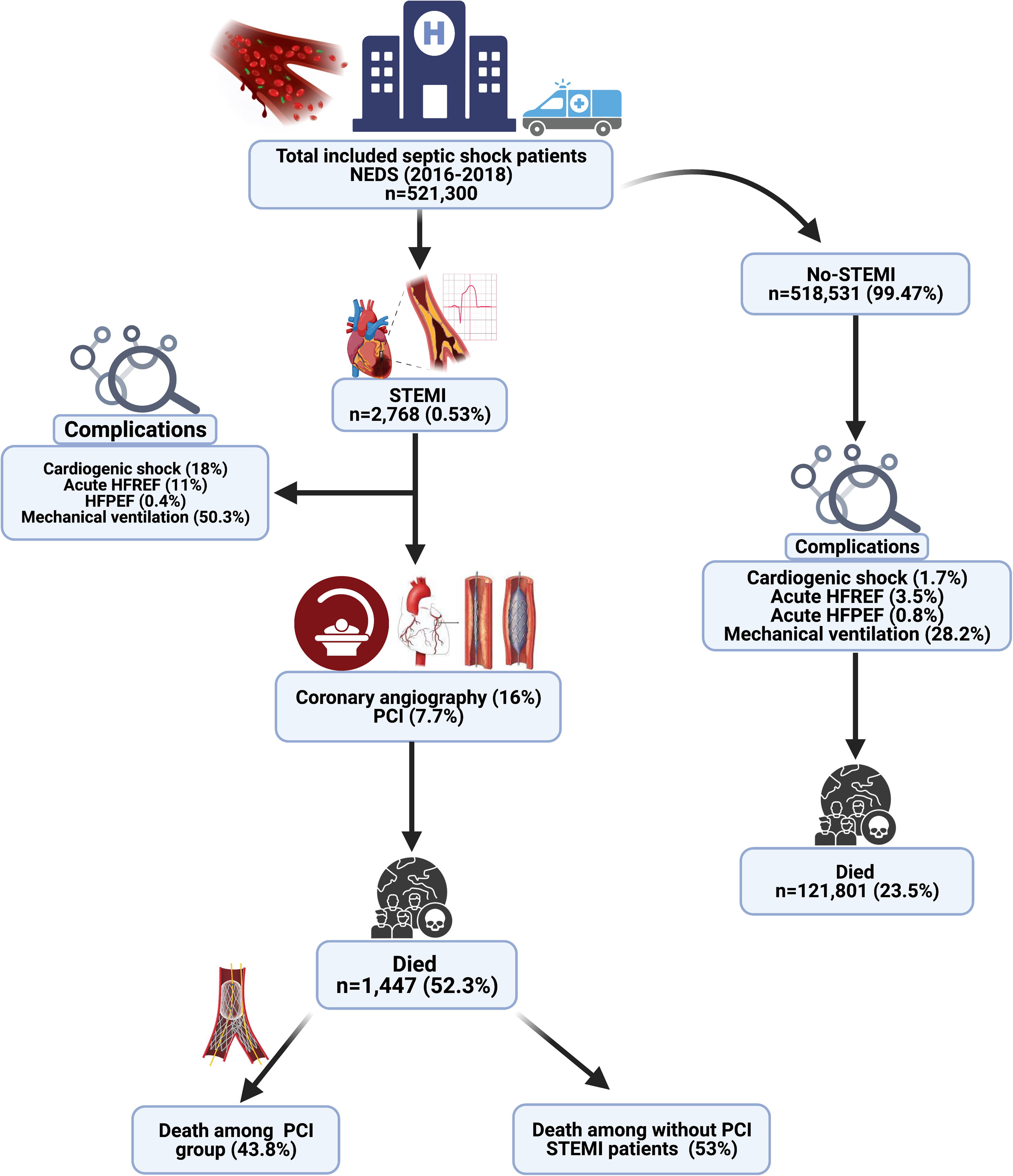
Graphic abstract (created with biorender.com).
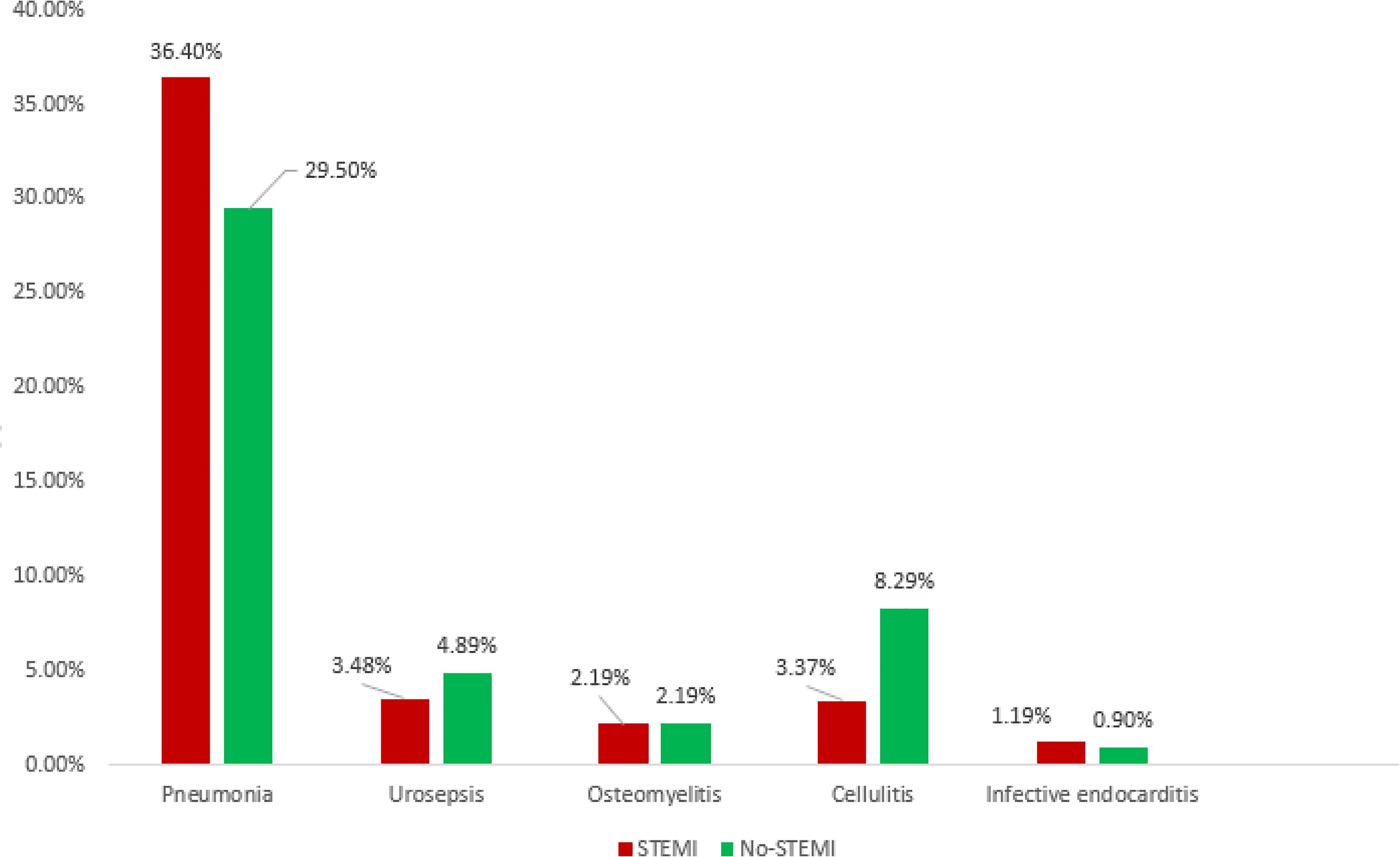
Prevalence of major infections associated with STEMI and without STEMI septic shock. Pneumonia was the predominant infection associated with STEMI and without STEMI. STEMI, ST-elevation myocardial infarction.
Baseline Characteristics of STEMI and Without STEMI Septic Shock Patient Population.
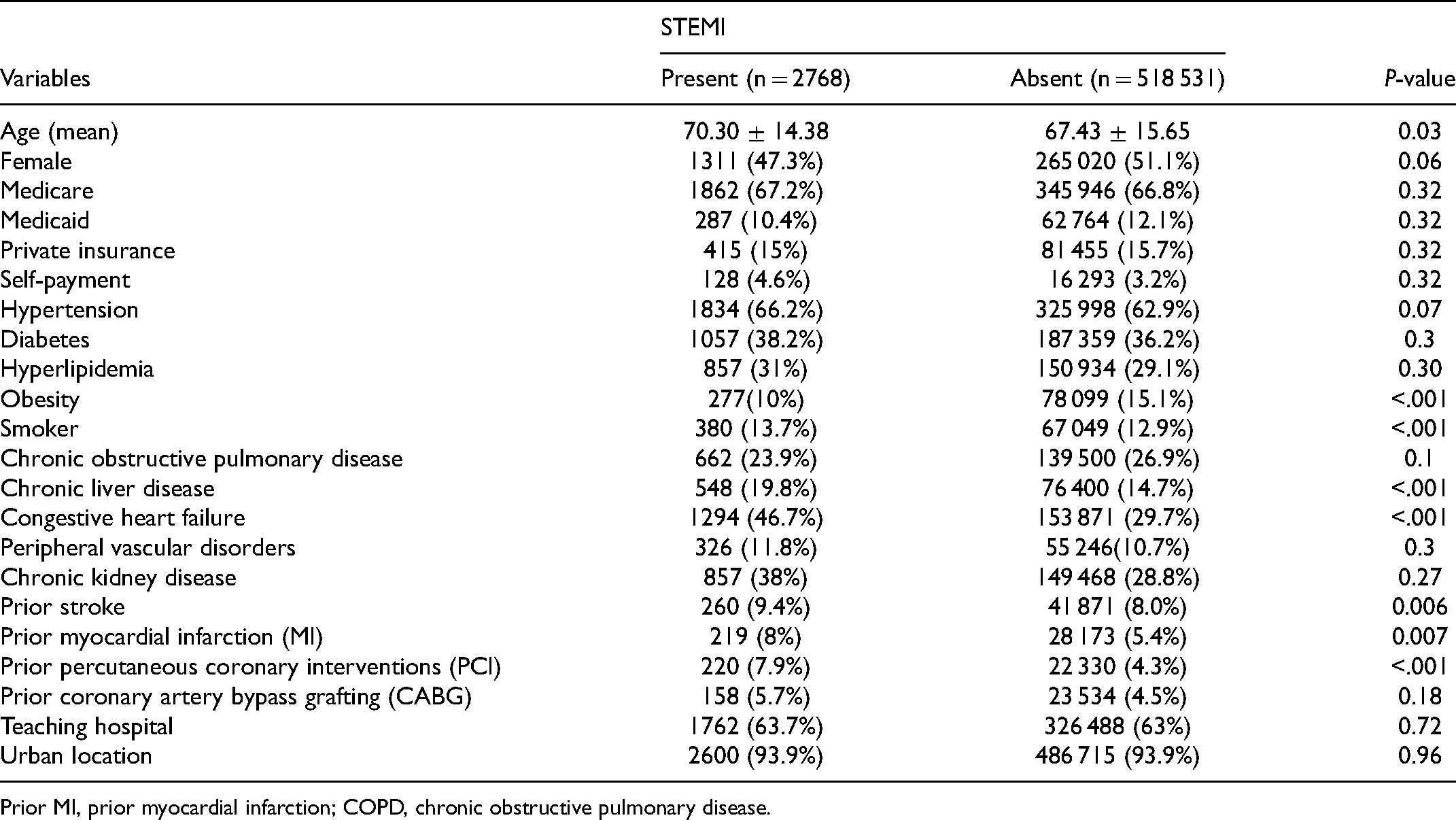
Prior MI, prior myocardial infarction; COPD, chronic obstructive pulmonary disease.
Mortality Outcomes
Out of 2 768 patients who had STEMI, 1447 (52.3%) died, and out of 518 531 patients without STEMI, 121 801 (23.5%) died during the hospitalization. In a multivariable logistic regression model adjusted for model1 STEMI was strongly associated with mortality among septic shock patients (OR 2.87, 95% CI 2.37-3.49; P < .001). Mortality rates numerically improved with PCI among STEMI patients (43.8% vs 56.2%) (Supplemental Digital Content—Table 2). However, in a multivariate logistic regression adjusted for model2 for mortality among STEMI septic shock patients, cardiac procedures had no significant association with mortality (PCI: OR 0.69, 95% CI 0.38, 1.24; P = .21) and coronary angiography: OR 0.64, 95% CI 0.41, 1.02; P = .06) among STEMI septic shock patients. After coarsened exact matching for model1, on univariate logistic regression results were consistent and coronary procedures had no significant association with mortality among STEMI septic shock patients. On sensitivity analysis after excluding patients with a hospital stay of fewer than 48 h, to exclude patients who died within 48 h of admission to hospital, PCI and coronary angiography had no association with mortality among STEMI septic shock patients.
Complications
Cardiogenic shock was observed in higher proportion of STEMI septic shock (n = 495, 18%) than patients without STEMI septic shock (n = 8901, 1.7%). A total of 12 (0.4%) among STEMI septic shock versus 4503 (0.8%) among without STEMI septic shock had acute heart failure with preserved ejection fraction and 304 (11%) among STEMI septic shock versus 18 262 (3.5%) without STEMI septic shock patients had acute heart failure with reduced ejection failure during the hospitalization. Patients with STEMI septic shock had higher rates of dialysis requiring acute kidney injury, 93 (3.3%), than patients without STEMI septic shock (11 188 (2%). Among STEMI septic shock patients 1393 (50.3%) needed mechanical ventilation as compared to 146 347 (28.2%) without STEMI septic shock.
Predictors of Mortality in STEMI and Septic Shock
In multivariable-adjusted logistic regression model1 analyzing mortality in STEMI septic shock population, age, peripheral vascular disease, were strongly associated with mortality among STEMI in septic shock patients (Figure 3).
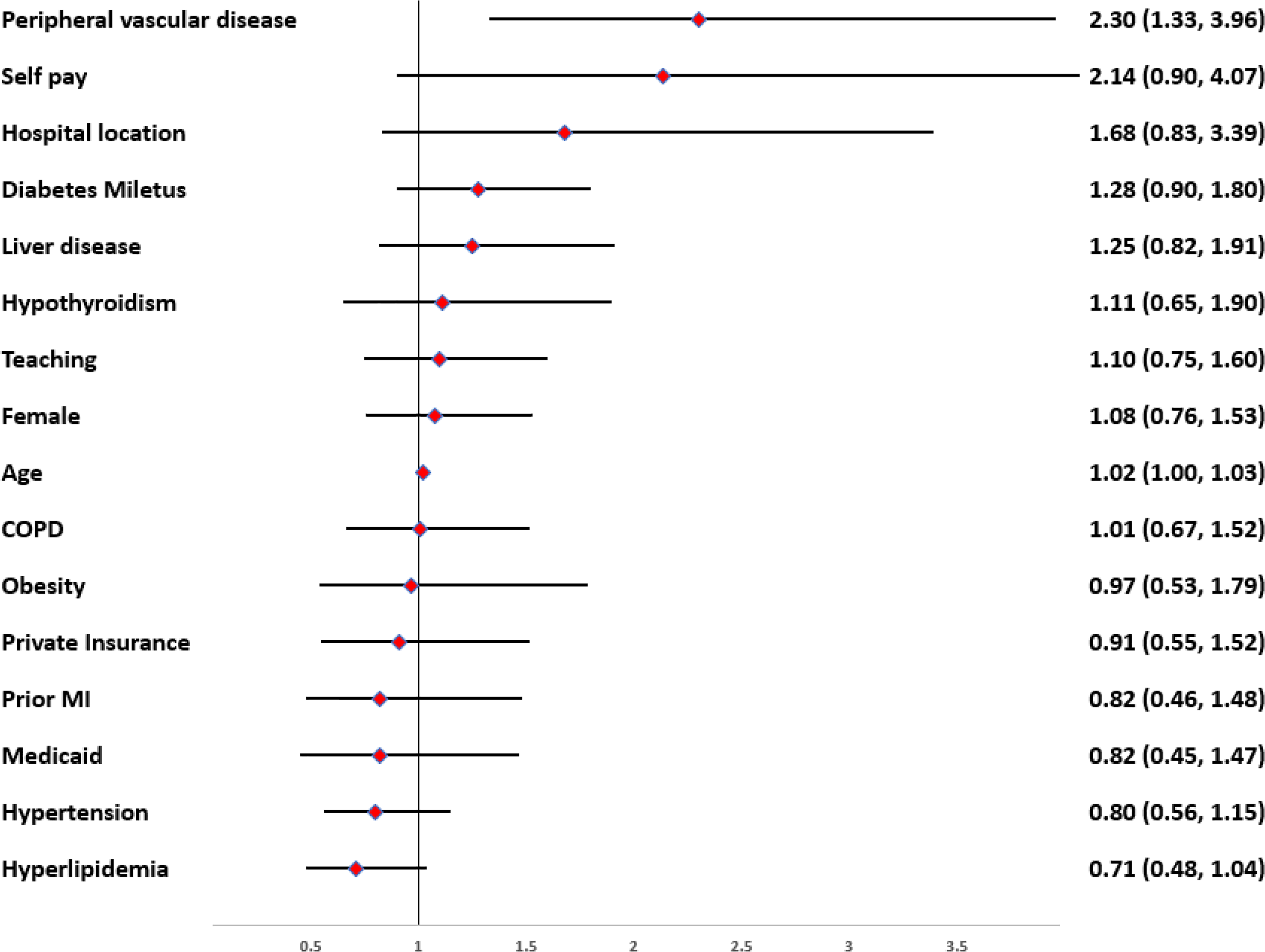
Predictors of mortality from STEMI in septic shock patients. Odds ratio and 95% confidence interval. COPD, chronic obstructive pulmonary disease; Prior MI, prior myocardial infarction.
Length of Hospital Stay
We also calculated the median length of stay for patients who had coronary angiography among the STEMI subgroup. Patients who had coronary angiography among STEMI patients had a median length of stay of 9 days (interquartile 3, 15) versus 4 days (interquartile 1, 10) who did not have coronary angiography among STEMI patients. Patients who died and did not have angiography among the STEMI subgroup had a median length of hospital stay of 2 days (interquartile 1, 4).
Discussions
To our knowledge, this is the first study evaluating outcomes of STEMI in patients primarily hospitalized for septic shock and the effects of coronary interventions on mortality among STEMI patients. Patients with septic shock associated with STEMI were predominantly males with a high comorbidity pattern. STEMI was strongly associated with mortality and higher mortality was observed among patients with STEMI (53.2%) than patients without STEMI among the septic shock population (25.2%). Alive STEMI septic shock discharges had a higher proportion of coronary interventions than the patients who died during the hospitalization among the STEMI septic shock patients. STEMI patients undergoing PCI had numerically lower mortality, however, there was no significant difference than patients who did not undergo PCI. Most of the STEMI patients who died without having coronary procedures had a median length of hospital stay of 2 days. Age and peripheral vascular disease were among the predominant predictors associated with mortality in patients with STEMI septic shock. Pneumonia was the predominant infection type association with and without STEMI septic shock patients. A high proportion of patients went to hospice among septic shock patients with higher numbers among patients with STEMI.
Previous studies have reported high mortality rates for patients with septic shock. A meta-analysis of 72 studies reported mortality rates for the septic shock of 38%. 5 However, the mortality rates were better than reported in the decade before 2010, 40% to 80%. 16 On the contrary we observed a better overall mortality rate of 29.8% for the whole cohort of septic shock patients. Mortality for patients admitted with a primary diagnosis of septic shock was 23.6%. For patients where the septic shock was complicated with STEMI, mortality was much higher, 52.3%. The higher mortality could be multifactorial. Cardiac myocardial dysfunction has been reported to worsen mortality outcomes in septic shock and septic shock can precipitate acute coronary events.7, 8 One in every 5 patients of STEMI septic shock also were coded as having cardiogenic shock, in our study. This group of patients had higher mortality rates (56.4%) than patients without associated cardiogenic shock (51.4%) in the STEMI subgroup. The higher rates of cardiogenic shock would be another reason for worsening mortality results. A prospective study of 7865 STEMI patients, with a 13% cardiogenic shock patient population, reported high mortality of 37% for patients with STEMI and cardiogenic shock. 17
Higher rates of coronary procedures were performed in STEMI septic shock patients; however, the rates were not as has as the national standards for STEMI patients. A Report from the National Cardiovascular Data Registry, 2011 reported rates of 87.9% PCI in patients with STEMI. 18 We observed a PCI rate of only 7.7% in our STEMI septic shock patients with coronary angiography rates of 16%. The low rates of coronary interventions in the subgroup of patients can be multifactorial. Patients among the STEMI subgroup who died without angiography had a median length of stay of 2 days. The earlier death could be one of the reasons for the low rates of coronary procedures among this subgroup of STEMI patients. Another reason could be secondary to being high risk procedures in already critically ill patients, as has been reported previously. 19 There was a numerical improvement in mortality with PCI among STEMI patients, however, there was no significant difference than patients who did not have PCI on multivariate logistic regression and univariate logistic regression post coarsening exact matching of the baseline characteristics. Sensitivity analysis was performed by excluding patients with less than 48 h of hospital stay and coronary procedures had no significant association with mortality. To our knowledge, there are no previous studies that have evaluated coronary interventions among patients with STEMI complicating septic shock. More randomized trials will be needed to evaluate the effects of early PCI in STEMI septic shock patients.
Interestingly pneumonia was the predominant infection recorded for STEMI and patients without STEMI. A prospective study of 3588 patients with severe sepsis reported a higher incidence of pneumonia with associated high mortality rates. 20 Higher proportion of patients with STEMI septic shock had infective endocarditis than patients without STEMI. Patients with infective endocarditis are at a higher risk of developing septic emboli into the coronary artery and hence can present as STEMI. 21
We evaluated predictors associated with mortality among STEMI with septic shock. We observed elderly patients with the peripheral arterial disease were more likely to die among the subgroup of patients with STEMI septic shock. Previous studies have reported the presence of peripheral arterial disease as an independent predictor of acute myocardial infarction and mortality among patients with acute myocardial infarction.22,23
Most of the surviving patients with septic shock had a disposition to nursing/skilled care. Significant rates of disposition to hospice were observed among the STEMI septic shock patients.
Study Limitations
Our study has several limitations. First, this is a retrospective, observational study, and inference regarding causation should be made with caution as controlling for comorbidities is challenging. Also, we relied on reported ICD-10 codes to identify diagnoses to perform our analysis. The national emergency database is an administrative database that could be subject to inaccurate over-coding and underreporting of some comorbid diagnoses. There is also an absence of important information related to patients’ physical examination, medications, and laboratory results. Thus, baseline severity scoring systems of septic shock such as qSOFA, APACHE II, SAPS could not be evaluated in these patient population. We could not evaluate the time to coronary interventions or use of fibrinolytic therapy. We could not evaluate if the early death was secondary to delay in coronary interventions or early death was the reason for not performing coronary interventions. We could not evaluate time to death post STEMI event. We could not evaluate the echocardiography procedures done in these patients. Also, we could not evaluate single or multiple vessel coronary artery involvement. However, NEDS and the codes used in this study have been applied in multiple clinical studies and can be considered a highly reliable database, and giving the large cohort analyzed this minimizes the study limitation.
Conclusions
STEMI may be one of the associated complications among patients admitted for septic shock. The mortality rates among STEMI septic shock were higher than the septic shock patients without STEMI. Higher complication rates including cardiogenic shock, ventilator requirement, and acute kidney injury requiring dialysis were associated with such a critically ill subgroup of patients. Despite some numerical improvement in mortality, PCI and coronary angiography had no significant difference from patients who had no PCI. Patients who did not have coronary procedures died earlier during the hospital stay. Randomized clinical trials will be needed to evaluate the impact of early coronary procedures in this subgroup of patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.