
Abstract
Introduction
The pathophysiology of acute nausea and vomiting (N/V) is not fully understood, but known to be partially mediated by antagonism of chemoreceptors in the gastrointestinal tract such as 5-hydroxytryptamine 3 (5-HT3), neurokinin 1, dopamine, acetylcholine and substance P.1,2 Medications targeting these chemoreceptors have become a mainstay of anti-emetic therapy, including: ondansetron – a 5HT3 with strong evidence for preventing post-operative and chemotherapy-induced N/V, metoclopramide – a dopamine and 5-HT4 receptor antagonist that increases GI motility, and prochlorperazine – a dopamine antagonist with anticholinergic effects.1,3 In the predictable circumstances of chemotherapy and surgery where nausea and vomiting are expected, there are clear guidelines and treatment algorithms.4,5 However, outside of these circumstances, the most frequently used anti-emetic classes have displayed similar effectiveness and there is little consensus as to which agent should be used.6,7
Anti-emetics have displayed similar effectiveness outside of specific circumstances such as surgical prophylaxis or chemotherapy, and it has been recommended that anti-emetics be chosen based on individual patient safety characteristics. 8 Clinicians must consider a patients’ age, comorbidities, pregnancy status, and acute illness when deciding on an anti-emetic regimen to avoid predictable adverse effects of QT-prolongation associated with 5-HT3 antagonist use, and anticholinergic or extrapyramidal effects with dopamine antagonists.9,10 The safety concerns that must be considered become increasingly complicated in patients experiencing critical illness, where pharmacologic therapies with ondansetron or prochlorperazine are common to prevent dehydration and aspiration as a result of vomiting. 11 However, a recent pharmacoepidemiologic study has identified an association between ondansetron use and a decrease in the risk for acute kidney injury (AKI). 12 5-HT3 antagonists have also been found to be nephroprotective in animal models. 13 Anti-emetics are generally metabolized through conjugation and hepatic routes, and it is important to further explore the role they play on renal function since anti-emetics are often administered despite compromised renal function because of their relative safety.14-16
AKI is a rapid increase in serum creatinine or decrease in urine output that is associated with kidney damage and dysfunction. 17 AKI occurs in roughly 10 to 15% of all hospital admissions, but upward of 50% in patients admitted to the ICU.18,19 Patients experiencing low-grade AKI in the ICU have 68% increased odds of mortality compared to those without AKI, but patients with the highest-grade AKI have an almost 7-fold increase in the odds of mortality. 19 AKI also substantially increases hospitalization costs, with patients experiencing AKI incurring roughly $1800 higher hospitalization costs, which can increase to $11,000 if dialysis is needed. 20
The goal of our study was to determine the association between ondansetron and AKI. In order to control for indication bias, we compared this association to that of other anti-emetics, prochlorperazine and metoclopramide when used in an intensive care setting. To the best of our knowledge, there has been no real-world studies that have examined the risk of AKI following anti-emetic use in an intensive care population. Using a cohort of intensive care patient encounters, we employed a propensity-matched analysis of AKI occurrence following ICU admission in order to determine the association between anti-emetic usage and the subsequent risk of AKI, 90-day mortality, and time to AKI.
Methods
International Review Board Approval
This study utilized de-identified health information, and was deemed exempt for consent by the University of Pittsburgh Institutional Review Board.
Study Design
The study design used was a retrospective cohort analysis conducted in accordance with the STROBE guidelines for reporting in observational research. 21
Data Source
We used the High-Density Intensive Care-15 database (HiDenIC-15), which includes data from patients admitted to intensive care units across 12 facilities in western Pennsylvania between October 2008 – December 2014.
Study Population
Our source population consisted of the first ICU encounter for each patient within HiDenIC-15 with at least one recorded serum creatinine lab result. Patients were excluded if they were under the age of 18. In order to balance the baseline risk of AKI upon ICU admission, patients were also excluded if they had a history of extra-corporeal membrane oxygenation use, a history of immunosuppression, a history of end-stage renal disease, a previous solid organ transplant, or experienced AKI prior to or within the first 24 h following ICU admission. We used patient-level data for the remaining 93,242 patient encounters for the analysis.
Exposure Definition
Ondansetron use was defined as the administration of any form of ondansetron within the first 24 h following ICU admission. 15 Metoclopramide and prochlorperazine were identified as comparators for ondansetron because both of these medications have anti-emetic properties and are available in both an intravenous and oral formulation.14,16 Metoclopramide use and prochlorperazine use were defined using the same criteria as ondansetron. All medication exposures were determined based on the exclusive use of the medication of interest relative to the other two medications. For example, all patients considered to have used ondansetron received at least one dose of ondansetron, and zero doses of both prochlorperazine and metoclopramide during the same time period. The patients not receiving either of these three options were considered as a control group. Patients receiving doses of more than one anti-emetic of interest in the exposure period were excluded from the primary analysis but considered in a sensitivity analysis.
Outcome Definition
Our primary outcome was the occurrence of AKI following ICU admission. AKI was defined using the Kidney Disease, Improving Global Outcomes (KDIGO) 2012 guidelines. 22 To ensure that the kidney outcomes being analyzed were occurring during the exposure period of ondansetron, AKI was evaluated using hours >24 - ≤72 after ICU admission. Secondary outcomes were hours to first AKI, and 90-day mortality (both beginning on hour 24 post-ICU admission).
Covariate Selection
Independent variables included: age, race (white, black, or other), sex, weight, the presence of sepsis, a Charlson comorbidity index, and a history of hypertension. Each patient also had a sequential organ failure assessment score (SOFA), as well as an acute physiology, age, chronic health evaluation (APACHE) score calculated upon admission that were included as control variables.23,24 APACHE and SOFA are risk stratification methods that have been well-established in accurately predicting mortality risk in an ICU setting. 25 We also controlled for baseline serum creatinine using the methods for estimating baseline serum creatinine recommended by the KDIGO 2012 AKI guidelines. 26 Lastly, we identified ICU admissions as occurring by either surgical or medical sources, with surgical admissions defined as the patient having a Current Procedures and Terminology (CPT) code indicating a procedure within 5 days prior to ICU admission, and medical admissions defined as the absence of recent procedure.
Statistical Analysis
We calculated the rate of use for each anti-emetic within the first 24 h of ICU admission, and subsequent rates of occurrence of AKI, hours to first AKI, and 90-day mortality. The primary outcome of AKI between hours >24 - ≤72 was analyzed using propensity score-matched (one-to-one nearest neighbor matching) logistic regression (continuous regression for hours to AKI). Propensity score matching was used to balance the proclivity for an individual patient to receive an anti-emetic agent using the covariates listed above. 27 The secondary outcomes of hours to first AKI and 90-day all-cause mortality were analyzed using Cox proportional hazard models in order to estimate the time-to-event nature of these outcomes. 28 Ninety-day mortality was also analyzed using IPTW-adjusted logistic regression as a binary variable (death vs. alive at 90 days). Results from the propensity-adjusted analyses are presented as average-treatment effect absolute risk differences. Sensitivity analyses were conducted challenging our initial definitions. First, we analyzed different exposure windows; using patients receiving anti-emetics within 6 and 12 h of admission instead of 24 h. Next, we also considered a shorter outcome window of 24 h instead of 48. We also conducted inverse propensity-treatment weighting analyses using the same covariates to check for the robustness of our model, with no substantial change in results. 29 Additionally, an analysis of covariate distribution pre- and post-propensity score weighting displayed sufficient balance. Our definition of a surgical admission was a CPT code indicating a procedure within 5 days prior to ICU admission, but it was noted that surgical admissions were highly predictive of patient survival. Lastly, we expanded our groups to allow for patients receiving more than one anti-emetic, whereas our initial analysis excluded these patients and analyzed only patients exclusively using one anti-emetic (Table 1).
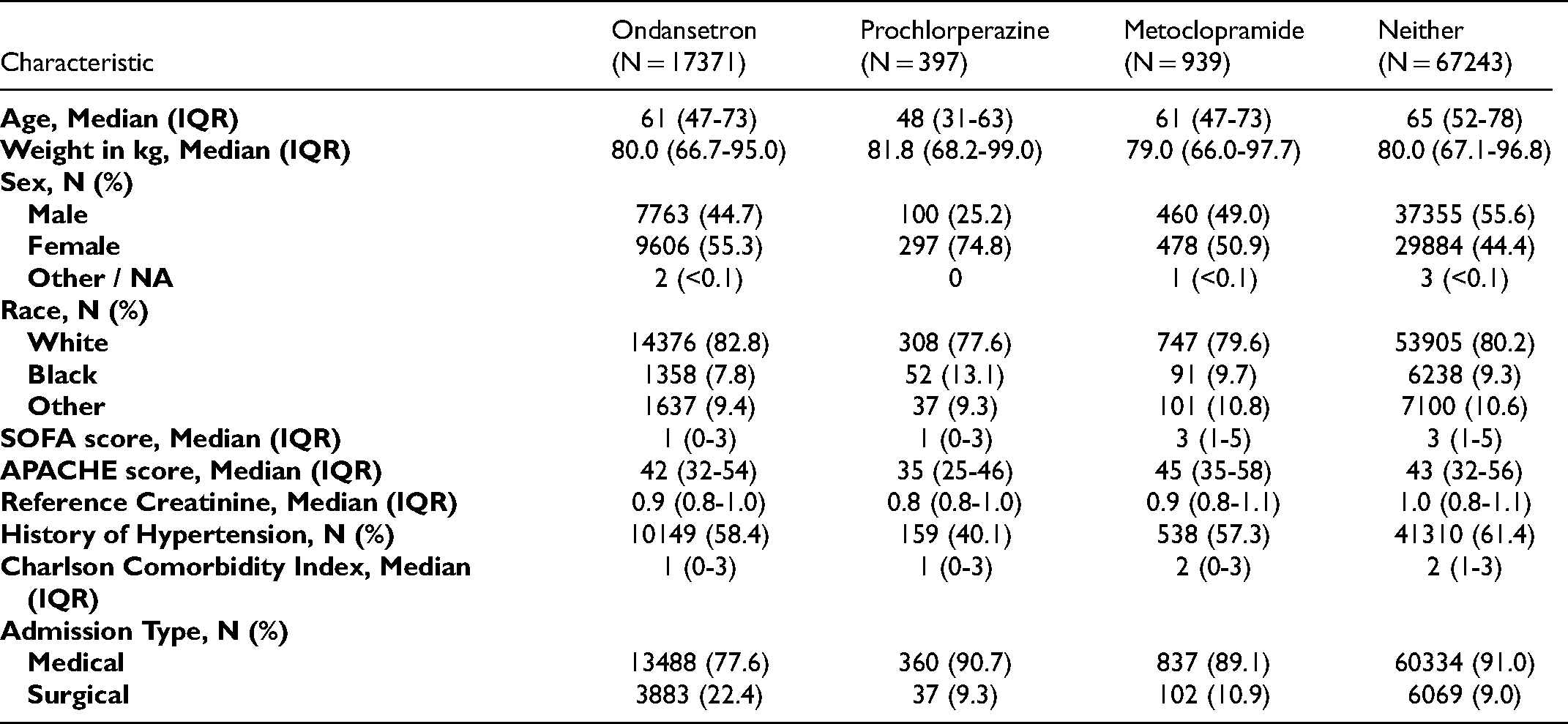
Cohort Demographics and Characteristics.
Results
After applying the exclusion criteria, there were 85,950 patients eligible for analysis (Figure 1). Of these admissions, we identified that 17,371 patients (20.21%) in which at least one dose of ondansetron was administered. Prochlorperazine and metoclopramide were used far less often—397 (0.46%) and 939 (1.09%) patients respectively. The remaining 67,243 (78.4%) were not exposed to any of these medications. Patients receiving and not receiving these medications had similar demographics and comorbidities, with some notable exceptions of patients using prochlorperazine being generally younger, more likely to be female, and generally healthier than other medication groups (lower average SOFA and APACHE scores, lower history of hypertension). There was also an apparent trend toward the use of ondansetron in surgical patients, with roughly 24% of patients receiving ondansetron having a recent surgery prior to ICU admission.
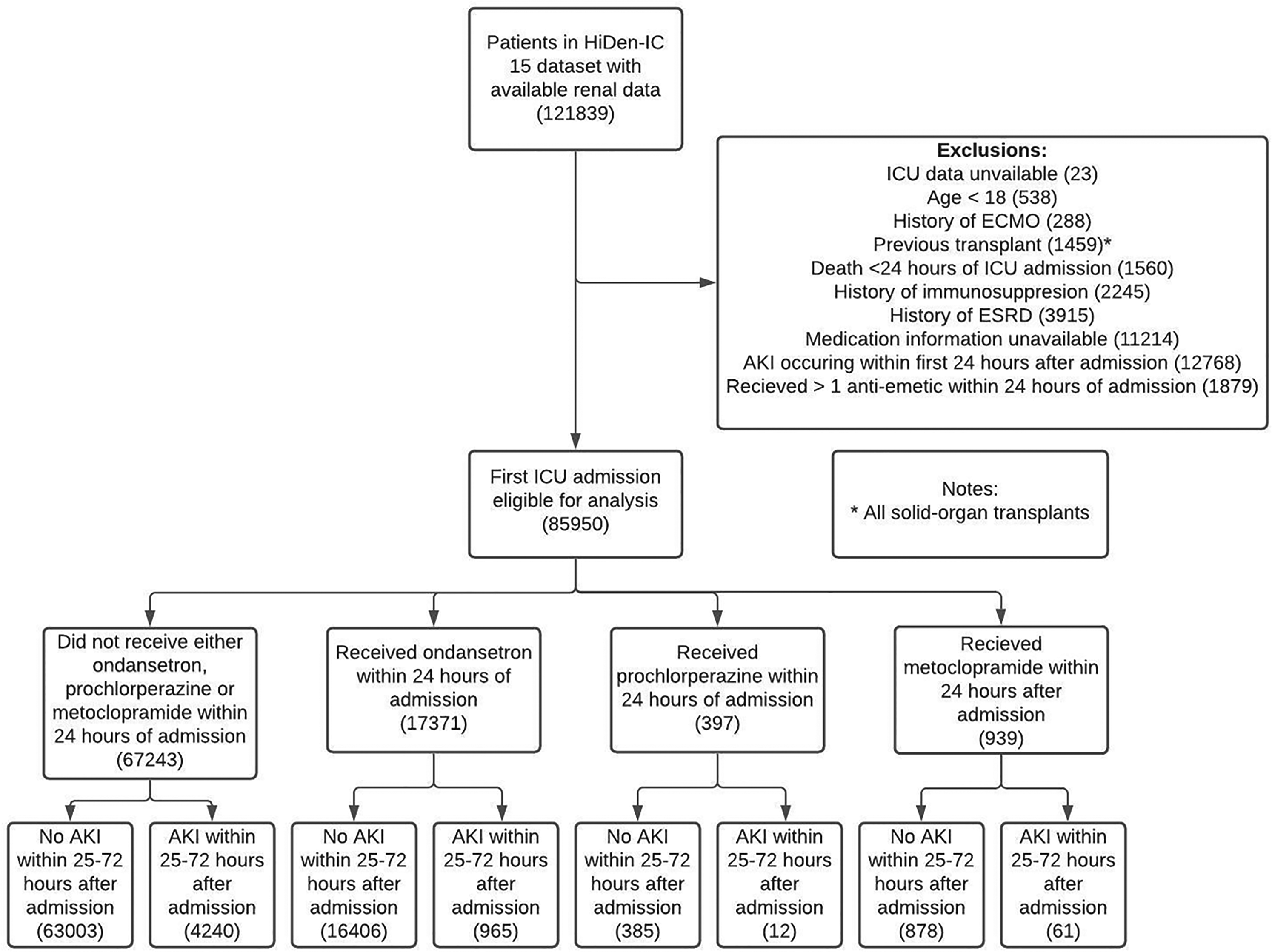
Cohort selection process and exclusion criteria.
The overall rate of AKI occurring hours 25 to 72 after admission was low across all medication groups, but was particularly low among patients receiving prochlorperazine (Table 2). In the propensity-matched regression results, there was no difference in the rate of AKI across each medication group (Table 3). The use of ondansetron (% Difference: 0.36; 95% CI −0.18-0.90), prochlorperazine (−2.37; −5.16 to 0.43), or metoclopramide (0.76; −1.37-2.90) did not significantly affect the rate of AKI. There were significant, but inconsistent differences seen in the rate of stage 2 to 3 AKI occurring, with the use of ondansetron being associated with an increased risk (0.58; 0.20-0.96), and prochlorperazine being associated with a decreased risk (−1.67; −2.23 – −1.08). There were differences seen in 90-day mortality in patients receiving ondansetron. Ondansetron use was associated with a significant decrease in 90-day mortality (−5.48; −6.17 – −4.79), and was seen consistently in both patients experiencing AKI (−7.47; −11.29 – −3.64) and not experiencing AKI (−5.64; −6.32 – −5.00). No significant differences were seen in 90-day mortality in patients receiving prochlorperazine or metoclopramide, regardless of AKI status. The reduction in mortality associated with ondansetron remained significant when considering the potential for unmeasured confounding (Supplemental Table 2). There were no significant differences seen in the average hours to AKI in the weighted analysis. Notably, the prochlorperazine group could not be analyzed for the outcomes of mortality with AKI or hours to AKI because of an overall small number of patients experiencing AKI within this group (12 patients total).
Unadjusted Outcome Results.
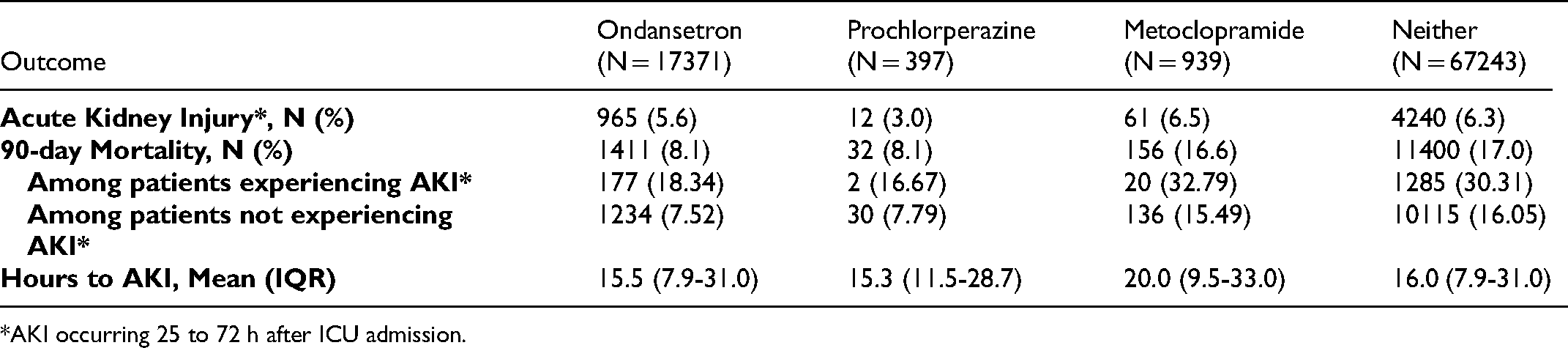
*AKI occurring 25 to 72 h after ICU admission.
Propensity-Matched Outcome Results.
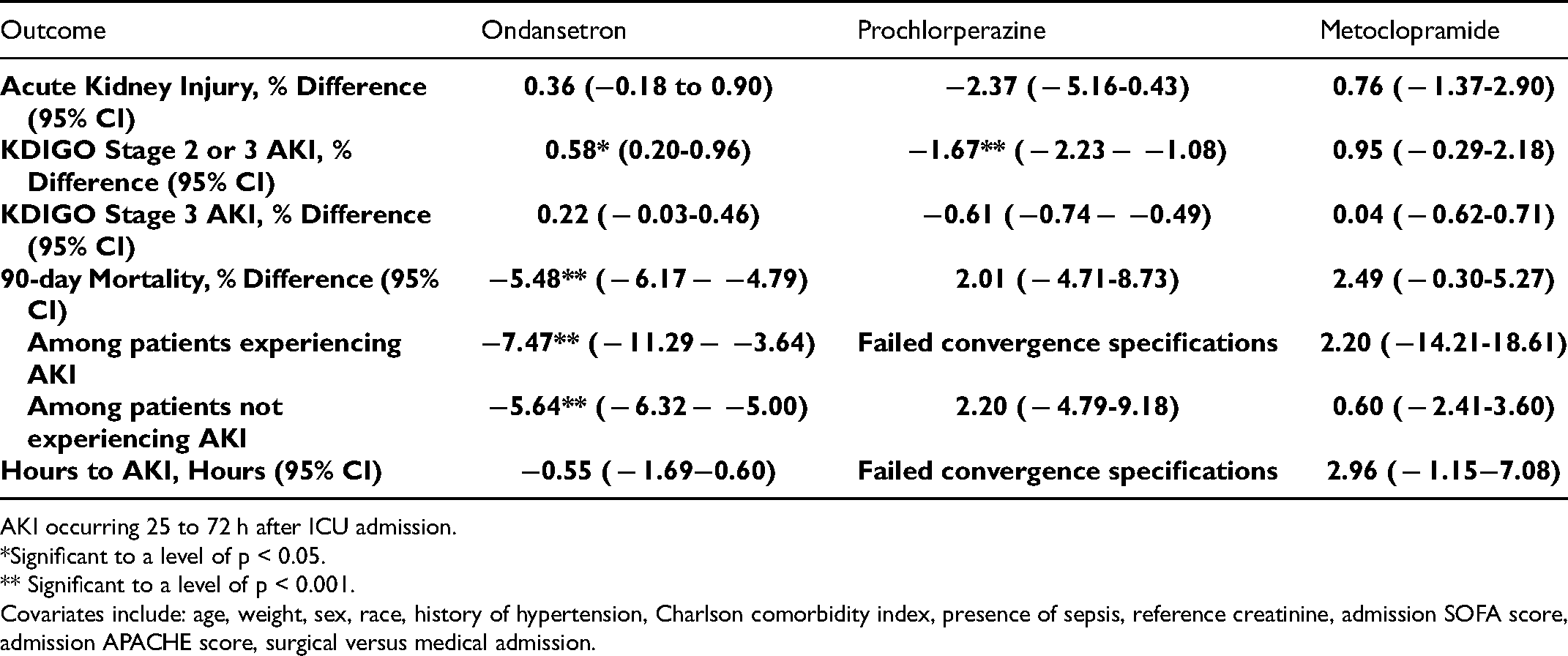
AKI occurring 25 to 72 h after ICU admission.
*Significant to a level of p < 0.05.
** Significant to a level of p < 0.001.
Covariates include: age, weight, sex, race, history of hypertension, Charlson comorbidity index, presence of sepsis, reference creatinine, admission SOFA score, admission APACHE score, surgical versus medical admission.
The results of the Cox Proportional hazard models for 90-day mortality are similar. Ondansetron use (Hazard Ratio 0.649; CI 0.614-0.687) was associated with a clear decrease in 90-day mortality, whereas the use of metoclopramide (1.05; 0.900-1.234) or prochlorperazine (0.897; 0.634-1.27) were not (Figure 2). These results remained consistent regardless of AKI status, with the receipt of ondansetron consistently being associated with decreases in 90-day mortality both in patients experiencing AKI (0.746; 0.636-0.875) and not experiencing AKI (0.637; 0.600-0.677). The results were also similar in a sensitivity analysis of 90-day, in-hospital mortality (Supplemental Figure 1). When stratified by stage of AKI experienced, there was no significant decrease in mortality in either medication use group in patients experiencing stage 2 or higher or stage 3 AKI alone, but metoclopramide use was associated with a significant increase mortality in stage 3 AKI (2.28; 1.01-5.19).
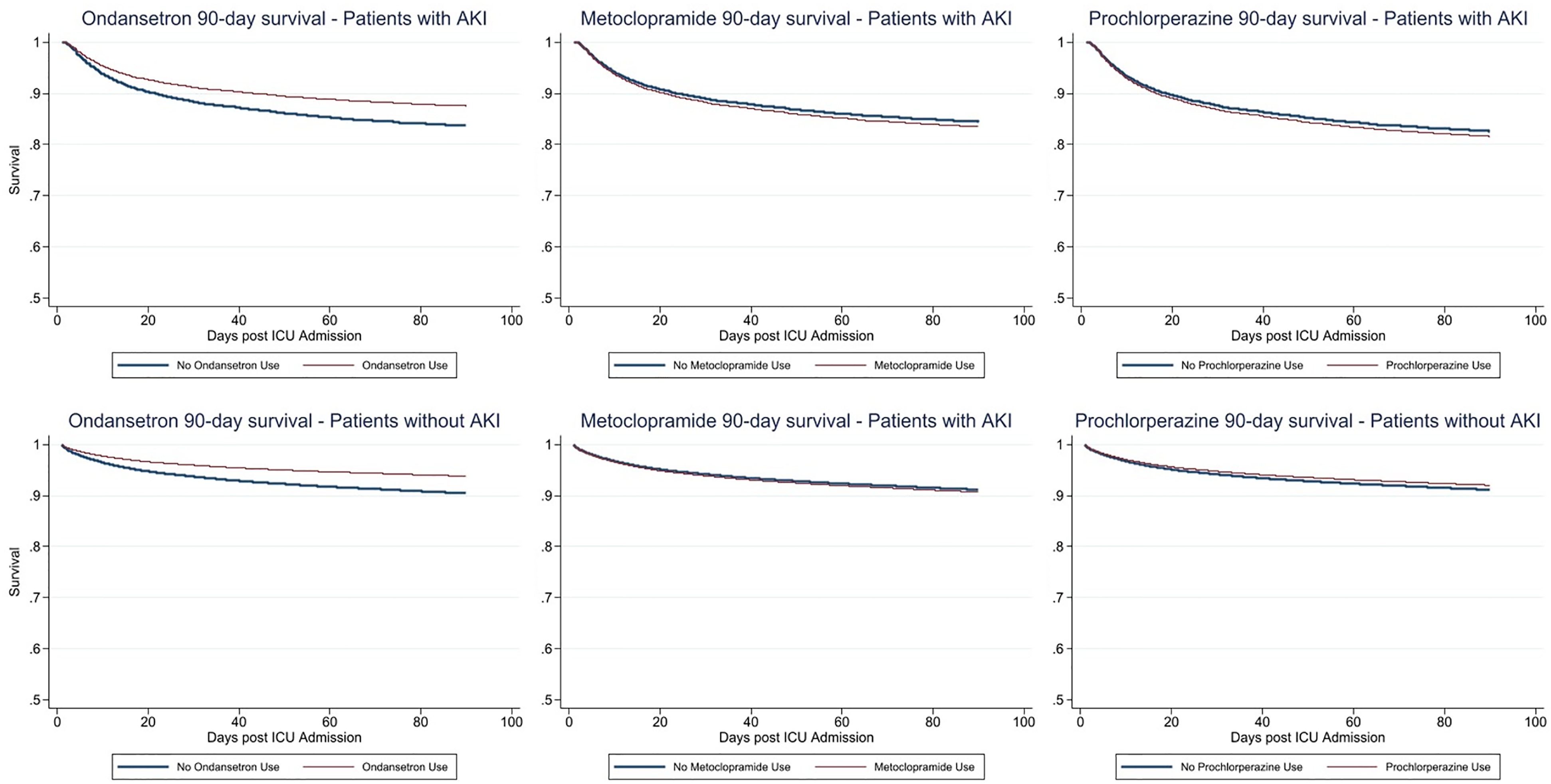
90-day survival function generated from Cox proportional hazard models of patients using each anti-emetic. Ondansetron difference significant to p < 0.001 level. Covariates include: age, weight, sex, race, history of hypertension, Charlson comorbidity index, presence of sepsis, reference creatinine, admission SOFA score, admission APACHE score, surgical versus medical admission.
Discussion
To the best of our knowledge, this is the first large, retrospective cohort study analyzing kidney-related outcomes of anti-emetic usage in an ICU population. The overall results of our propensity-matched analysis show no significant differences in the association of AKI in patients receiving either ondansetron, prochlorperazine, or metoclopramide in an ICU setting. There were statistically significant associations in sub-group analyses; with ondansetron use showing very small increased rates of KDIGO stage 2 or 3 AKI, and prochlorperazine decreasing this risk. However, these associations are inconsistent with the primary results findings and are of uncertain clinical significance. There was also no difference between anti-emetic groups in the time to first AKI following ICU admission. Interestingly, in a secondary outcome analysis of 90-day mortality following ICU admission, ondansetron use was associated with highly significant decreases in all-cause mortality, which was not seen in either the prochlorperazine or metoclopramide use groups. The decrease in 90-day mortality occurred independent of AKI occurrence within the time window analyzed, and does not appear to be related to an effect on kidney function.
Our results contrast the previous findings that ondansetron use is potentially associated with an increased risk of AKI. 30 There is a lack of literature describing real-world kidney-related outcomes following anti-emetic use, and our study is the first to include a comparison of these outcomes when using three of the most commonly used anti-emetics in intensive care. The mechanism through which anti-emetics may modulate renal function are poorly described. Human kidney cells possess 5-HT3 receptors, the target receptor of ondansetron, and animal studies have revealed that administration of 5-HT3 antagonists can exhibit beneficial anti-inflammatory properties.31,32 However, the extent to which anti-emetic medications act systemically to a degree required to contribute to renal function is unknown, and requires further studies to isolate this effect.
Our results show a significant decrease in all-cause 90-day mortality following ondansetron use in critically-ill patients. It was expected that anti-emetic use might be highly associated with an ICU admission secondary to surgery, but the benefit seen with reduced mortality remained significant after controlling for surgical/medical admission status. The reduction in mortality was independent of AKI status or the severity of AKI occurrence, indicating that any potential benefit ondansetron may be providing in mortality reduction is not the result of a decrease in AKI risk or severity. Disease severity was controlled for by using SOFA and APACHE scores, but it is possible there remains residual confounding associated with receiving ondansetron and reduced disease severity that may be affecting this result. Our results are subject to residual confounding due to its observational design, but the reduction in mortality associated with ondansetron use remained robust when considering E-values for unmeasured confounding. An potential unmeasured confounder would require an estimated OR of 2.5 or greater in order to explain the measured effect of ondansetron on mortality reduction. 33 The potential for ondansetron to reduce all-cause mortality should be examined through clinical trials or further real-world evidence studies in order to determine the role that 5-HT3 has in mortality reduction and disease severity.
A limitation of our analysis is the difficulty in clearly defining the temporality of anti-emetic administration and the development of AKI. We used variable definitions that included strict time frames for exposures and outcomes to maximize the likelihood that the anti-emetics received would be exerting their effects within the outcome window, but it is possible that some off-target effects were being captured. These strict definitions also caused some low sample sizes, particularly with prochlorperazine, which failed model specification requirements in some sub-group analyses due to an overall low number of patients experiencing AKI within this group. We restricted our population to patients who exclusively used one anti-emetic during the exposure period, whereas patients may receive multiple anti-emetics in actual practice. A sensitivity analysis including patients receiving more than one anti-emetic did not change the results appreciably (Supplemental Table 2). In the interest of ensuring our definition of a surgical admission was robust, we expanded this definition to include a period of within 10 days of ICU admission. The number of surgical patients within the ondansetron group increased by only 52 patients, with no appreciable change in results. Finally, we attempted to balance AKI risk using disease severity scores and baseline serum creatinine values, but there may be residual confounding such as the receipt of concomitant nephrotoxins that were not captured. However, we calculated E-values to estimate the effect of this unmeasured confounding which provide context for the extent amount of unmeasured confounding required to explain our results (Supplemental Table 1).
Conclusions
Ondansetron, prochlorperazine, or metoclopramide were utilized by roughly 22% patients in the ICU, with ondansetron comprising over 90% of use. There was no difference in AKI risk, or time to first AKI following the use of either anti-emetic. This is in contrast to pharmacoepidemiologic findings suggesting a possible link between ondansetron and AKI. Patients who used ondansetron had significantly reduced 90-day mortality following ICU admission, but the apparent benefit in survival was not influenced by the occurrence of AKI. The potential for ondansetron to reduce mortality should be further analyzed using clinical trials.
Supplemental Material
sj-docx-1-jicm-10.1177_08850666211073582 - Supplemental material for Kidney and Mortality Outcomes Associated with Ondansetron in Critically Ill Patients
Supplemental material, sj-docx-1-jicm-10.1177_08850666211073582 for Kidney and Mortality Outcomes Associated with Ondansetron in Critically Ill Patients by Matthew Gray, Priyanka Priyanka, Sandra Kane-Gill, Lirong Wang and John A. Kellum in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-2-jicm-10.1177_08850666211073582 - Supplemental material for Kidney and Mortality Outcomes Associated with Ondansetron in Critically Ill Patients
Supplemental material, sj-docx-2-jicm-10.1177_08850666211073582 for Kidney and Mortality Outcomes Associated with Ondansetron in Critically Ill Patients by Matthew Gray, Priyanka Priyanka, Sandra Kane-Gill, Lirong Wang and John A. Kellum in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-3-jicm-10.1177_08850666211073582 - Supplemental material for Kidney and Mortality Outcomes Associated with Ondansetron in Critically Ill Patients
Supplemental material, sj-docx-3-jicm-10.1177_08850666211073582 for Kidney and Mortality Outcomes Associated with Ondansetron in Critically Ill Patients by Matthew Gray, Priyanka Priyanka, Sandra Kane-Gill, Lirong Wang and John A. Kellum in Journal of Intensive Care Medicine
Footnotes
Funding
No funding was provided for this project.
Conflicts of Interest
Drs. Wang, and Kellum are listed on a provisional patent application filed by the University of Pittsburgh for the use of 5-HT3-targeting drugs for treatment of AKI.
Availability of Data and Materials
The data for this project was procured and processed through a data user agreement with University of Pittsburgh and University of Pittsburg Medical center (UPMC), and restricted to be shared with outside sources.
Author Contributions
MG – Concept development, statistical analysis, manuscript preparation; PP – Statistical analysis, manuscript review; LW – Concept development, manuscript review; SKG – Concept development, manuscript review; JAK – Concept development, subject matter expert, manuscript review
Ethics Approval
Approved as exempt by IRB
Consent to Participate
Not applicable
Consent for Publication
Not applicable
Prior Presentation
A poster abstract of this article was presented at the International Conference on Pharmacoepidemiology and Therapeutic Risk Management Virtual 2021 Meeting entitled: “Association of Ondansetron Use and Subsequent Acute Kidney Injury in Critical Care”
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Xxxxxxx.Drs. Wang, and Kellum are listed on a provisional patent application filed by the University of Pittsburgh for the use of 5-HT3-targeting drugs for treatment of AKI.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.