
Abstract
Background
Cardiopulmonary Resuscitation (CPR) causes significant injuries and increased cost among transiently resuscitated patients that do not survive their hospitalizations. Descriptive studies show zero and near-zero percent survival for CPR recipients with high Apache II scores. Despite these factors, no controlled studies exist in CPR to guide patient selection for CPR candidacy. Our objective was therefore to perform a controlled study in CPR to inform recommendations for CPR candidacy. We hypothesize that the protective effects of CPR decrease as illness severity increases, and that Full-Code status provides no survival benefit over Do-Not-Resuscitate (DNR) status for patients with the highest predicted mortality by Apache IV score.
Methods
We performed propensity-score matched survival analyses between Full-Code and DNR patients after stratifying by predicted mortality quartiles using Apache IV scores. Primary outcomes were mortality hazard ratios. Secondary outcomes were Median Survival Differences, ICU LOS, and tracheostomy rates.
Results
Among 17,710 propensity-score matched ICU encounters, DNR status was associated with greater mortality in the first through third predicted mortality quartiles. There was no difference in survival outcomes in the fourth quartile (HR 0.99, p = .96). There was a stepwise decrease in the mortality hazard ratio for DNR patients as quartiles increased.
Conclusion
Full-Code status provides no survival benefit over DNR status in individuals with greater than 75% predicted mortality by Apache IV score. There is a stepwise decrease in survival benefit for Full-Code patients as predicted mortality increases. We propose that it is reasonable to consider a very high predicted mortality by Apache IV score a contraindication to CPR given the lack of survival benefit seen in these patients. Larger studies with similar methods should be performed to reinforce or refute these findings.
Introduction
In-hospital cardiopulmonary resuscitation (CPR) causes significant injuries 1 and increased cost among those who are transiently resuscitated but do not survive their hospitalization. 2 Observational studies report zero, or close to zero percent survival for CPR recipients with high Apache II scores3–5 and futile resuscitations may adversely affect providers’ mental health.6–8 We define futile resuscitations as those that have an extremely low likelihood of survival, 9 do not accomplish patients’ broader goals 10 and are performed against the best judgment of the healthcare team because of patient or family demands. 11 Therefore, universally offering CPR to those who desire it pits non-maleficence against patient autonomy. There may also be health economics and triage issues if resource utilization increases for patients with no probability of survival.
Despite these factors, contraindications are nonexistent for in-hospital, futile CPR. Physicians are not required to offer interventions that cannot reasonably be expected to yield the intended clinical benefit or achieve agreed-on goals for care. 12 There are no controlled studies in CPR futility that we are aware of, so higher-level evidence is lacking to clarify if or when CPR should be contraindicated. There is only one study we are aware of that used data from Full-Code patients to predict survival outcomes in Do-Not-Resuscitate (DNR) patients, but this was to measure excess mortality attributable to being assigned a DNR status at the time of admission and was not designed to measure effectiveness of Full-Code resuscitation. Their hypothesis was based on the idea that DNR patients receive overall less intense care, making DNR status itself an independent risk factor for mortality regardless of cardiac arrest. 13
If CPR has a survival benefit, then full-code patients should have a survival advantage over DNR patients on matched levels of illness severity. To our knowledge, no study directly compares survival differences between DNR and Full-Code patients in the ICU after stratifying by predicted mortality.
Materials and Methods
We performed a propensity score matched comparison of survival between Full-Code and DNR patients, stratified by quartiles of predicted mortality by APACHE IV scores. We hypothesize that the protective effects of CPR decrease as illness severity increases, and that Full-Code status provides no survival benefit for patients with the highest predicted mortality. Primary outcomes were mortality hazard ratios comparing DNR and Full-Code patients within quartiles. Secondary outcomes were Median Survival Differences, ICU LOS, and tracheostomy rates. ICU LOS and tracheostomy rates were chosen as a surrogate for measuring cost.
Data
ICU admissions since the time of adoption of our EMR (10/1/2017 to 10/1/2021) from five hospitals with 144 ICU beds were captured. Our health systems’ capabilities include Level 1 trauma, stroke and STEMI care, transplant surgery, burn care, and general medical/surgical intensive care needs.
Children less than 18 years of age, pregnant patients, or patients under state custody were excluded.
Classifying Patients with Multiple Hospitalizations and ICU Admissions
The Apache score was the highest Apache Score in the first 24 h of ICU admission. The Apache score from the first ICU admission was taken for patients with multiple ICU admissions during one hospitalization. The same strategy was used in developing the Apache IV score. 14 For patients with 30-day hospital readmissions that included ICU admissions in both hospitalizations, data were abstracted from the hospitalization containing a death or the highest Apache IV score. ICU LOS was total ICU days during a hospitalization.
Classifying Code Status
An algorithm classified code status in our data because many patients change their status during a hospitalization. The following examples highlight why utilizing intention-to-treat or per-protocol analysis for crossover patients would likely introduce systemic bias:
Patients admitted without prior directives, incapacitated, and without designated healthcare agents are presumed Full-Code. Many patients become DNR after an agent is identified or they establish their own directives. Many patients with prior directives for DNR are assigned a Full-Code status for 24 hours after an operation due to institutional policy mandating reconsideration of perioperative code status. Many Full-Code patients that receive CPR are made DNR only when futility becomes apparent. Full-Code to DNR: These patients were classified as DNR because the intention for CPR was stopped before there was an indication for such. Presumed Full-Code patients or those with prior directives frequently become DNR based on goals of care conversations when admitted for critical illness. DNR to Full-Code: These patients were classified as a CPR patient because the intention to perform CPR was established before there was a need for such. Patients presenting in extremis may be admitted as a DNR patient by the families. When the patient’s condition improves, families or patients may change the status to Full-Code. This likely represents a rare event.
Therefore, any patient that received in-hospital CPR was classified as Full-Code. Anyone who died and never received in-Hospital CPR was classified as DNR. For everyone else, code statuses at the time of ICU admission and discharge or death were used to identify crossover. For crossover patients that did not receive CPR:
Apache IV Stratification and Propensity Score Matching
The final data were stratified into predicted mortality quartiles based on Apache IV scores (i.e. 0% to 25% predicted mortality, >25% to 50% predicted mortality, etc.). Within quartiles, patients were matched on propensity scores derived from logistic regression. Covariate selection was performed using the recommended 15 and evidenced based 16 practice for selecting covariates for propensity scoring; that is, covariates were associated with the exposure (Code Status) and outcome (ICU mortality), or the outcome alone. These were identified through a literature search for factors associated with Code Status or CPR and survival outcomes. These were age, gender, marital status, primary language, race/ethnicity, Charleson Comorbidity Index, the presence of metastatic malignancy, and admission diagnosis category (cardiovascular vs. non-cardiovascular). Admission diagnosis was from ICD-10 codes for medical admissions and CPT codes for surgical admissions. Matching was performed using nearest neighbor, variable ratio matching (maximum 2:1), with replacement and a 0.2 caliper. Weights were derived for encounters based on matching. Covariate balance was checked with Standardized Mean Differences <0.1. 17
Statistical Analysis
Hazard ratios for Mortality differences between DNR and Full-Code patients within quartiles were calculated using Cox Regression and survival curves were produced. Data was censored four weeks after the last date of enrollment. Median survival differences were calculated using the log rank statistic. Our alpha-level was 0.1 to decrease the risk of a type II error. Such an error risks falsely concluding that Full-Code resuscitation is futile.
R studio version 1.4 (https://www.rstudio.com/products/rstudio/), and IBM SPSS Statistics (IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) were used. The IRB for Human Subjects Research approved this research (ID H00022391_1).
Results
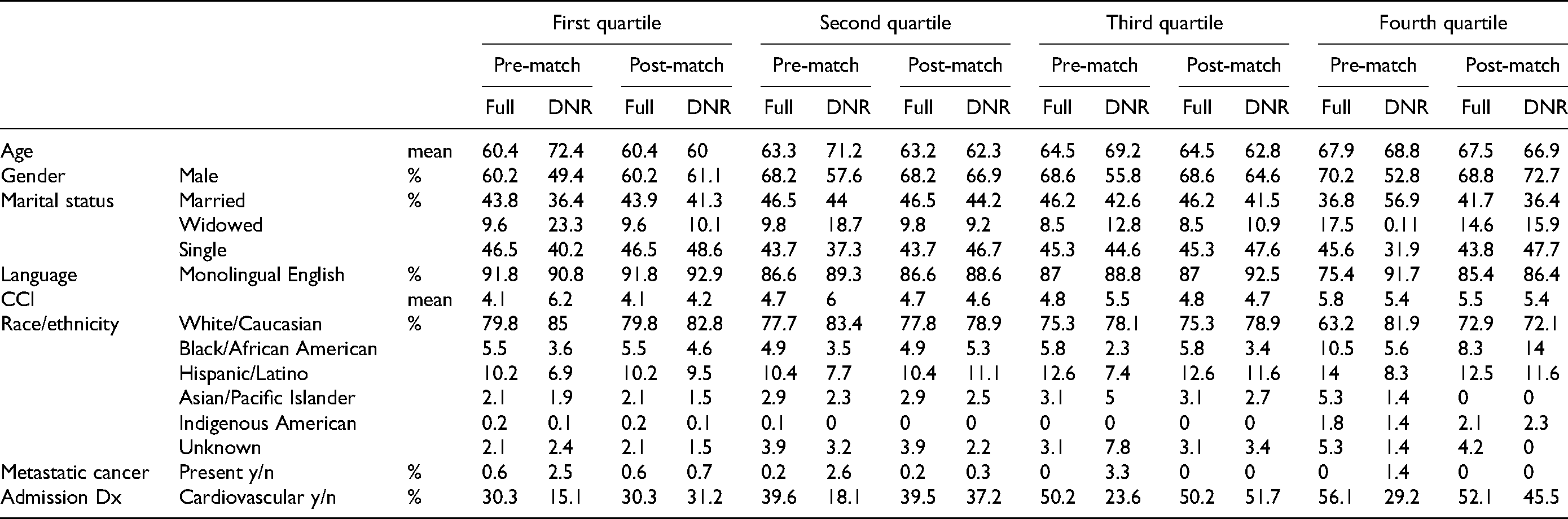
There were 29,597 unique encounters after exclusion criteria, and 20,376 had sufficient data for Apache IV Scores. After propensity score matching, 17,710 encounters remained for analysis (87%). All covariates were balanced after matching. Table 1 shows pre- and post-match covariate balance across all quartiles. The total observed mortality in matched data was equitable to that predicted by Apache IV scores (23.2%, 50.4%, 65.2%, and 85.9% mortality for the first, second, third, and fourth quartiles, respectively). Median time to censorship was 760 days.
Pre- and Post-match Covariate Balance Across Quartiles. All Post-match Variables were Balanced (Standardized Mean Differences <0.1).
Primary Outcomes
DNR status was associated with greater hazards for mortality in the first through third predicted mortality quartiles, but there was no difference in the fourth quartile (HR 0.99, p = .96). There was a stepwise decrease in hazard ratios for mortality between DNR and Full Code patients as quartiles increased. This suggests a decreasing survival benefit for Full Code patients as illness severity increases, which we expected based on our hypothesis. Table 2 shows summary statistics for primary and secondary outcomes, respectively. Figure 1 shows survival curves. Figure 2 shows the trend for decreasing survival difference across quartiles; as the predicted mortality quartile increases, the hazard ratio 95% confidence interval approaches and then crosses one at the fourth quartile. This means that there is no significant difference between survival outcomes for Full Code and DNR patients in the fourth quartile.
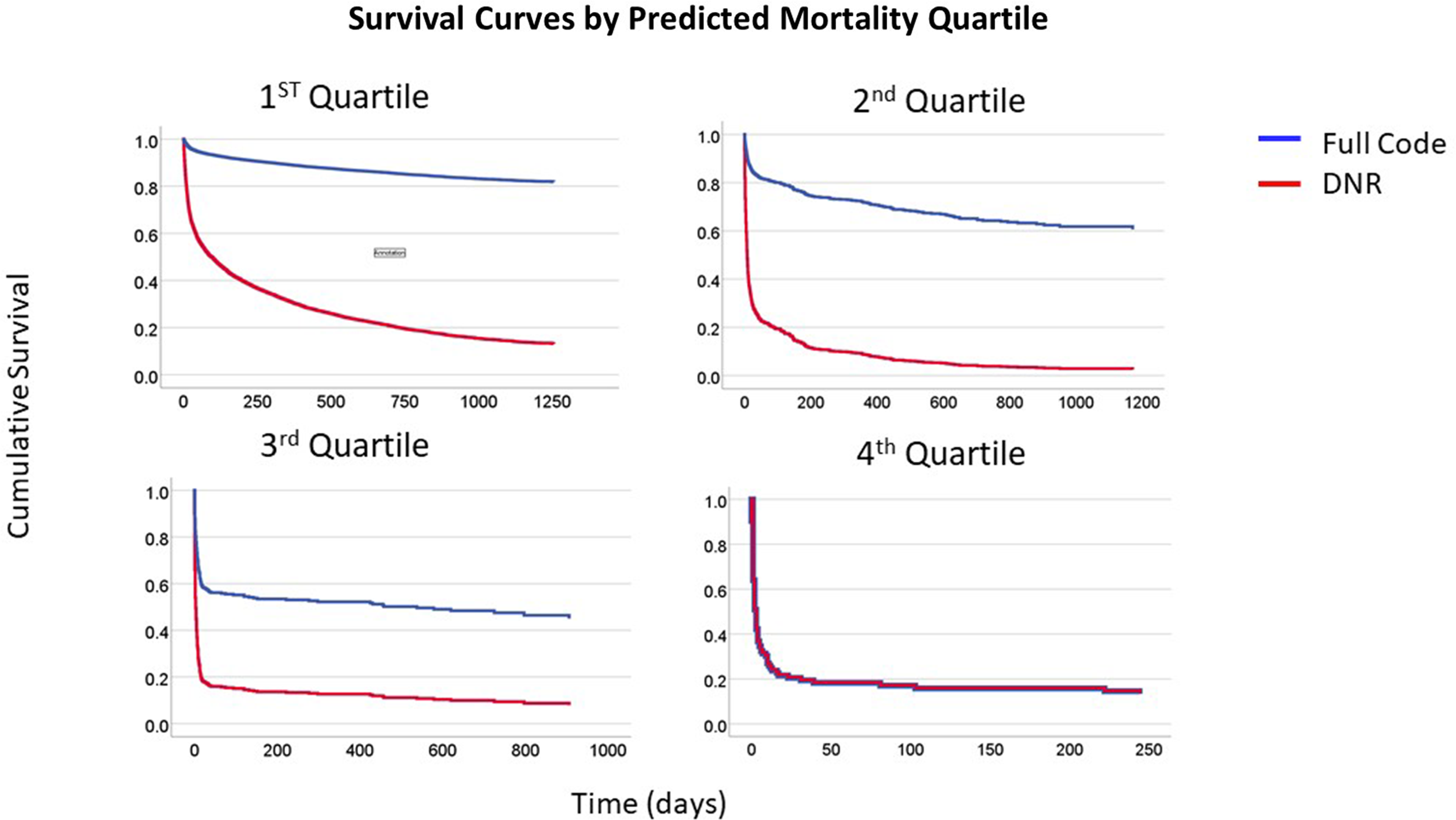
Survival curves, DNR vs. full code status by predicted mortality quartile.
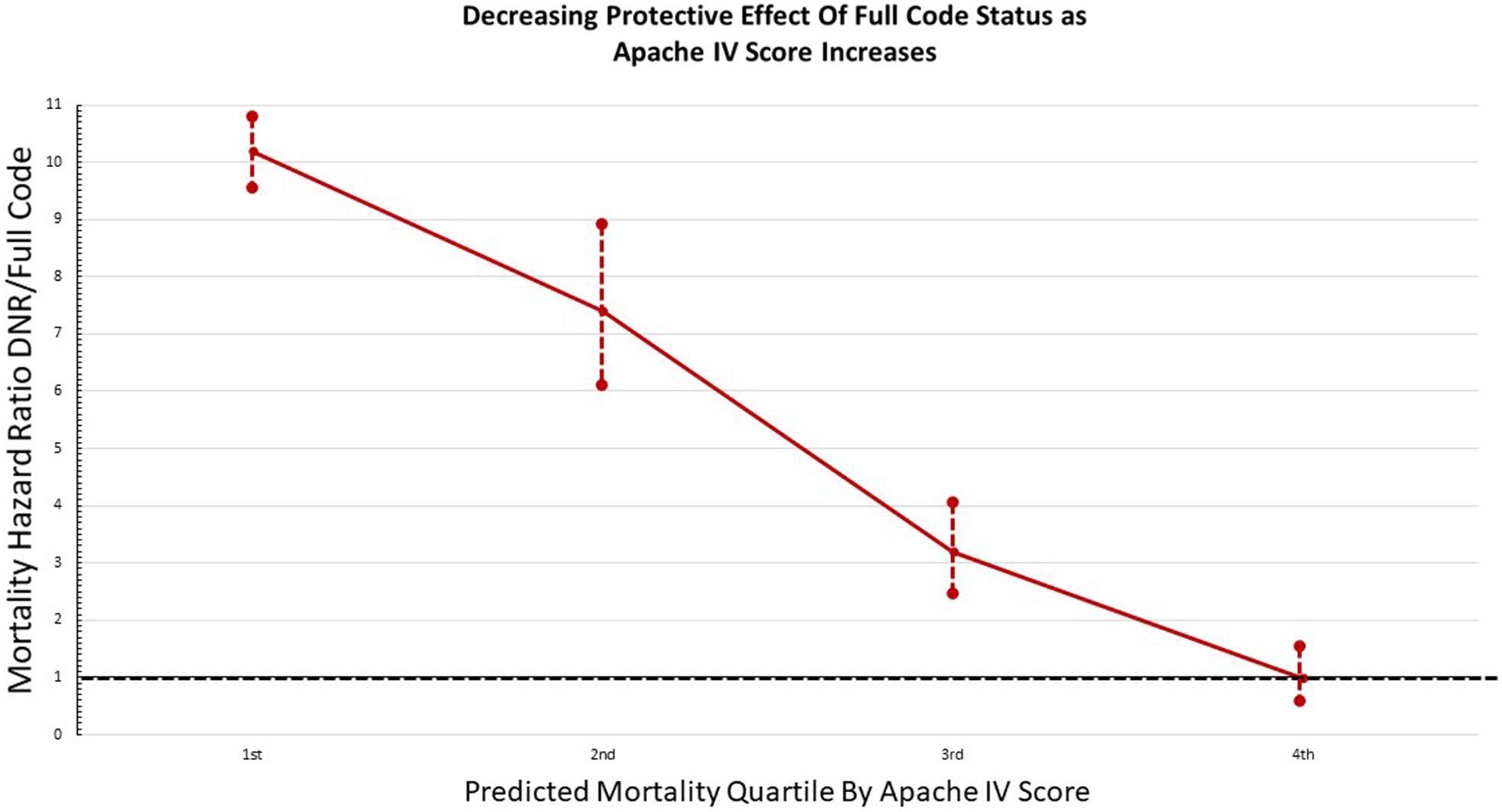
There is a stepwise decrease in mortality hazard ratio (DNR/full code) as predicted mortality quartile increases. This demonstrates the decreasing survival benefit of Full Code status as illness severity increases. When the 95% Confidence Interval crosses 1, there is no statistically significant difference in survival outcomes between groups, as seen in the fourth quartile.
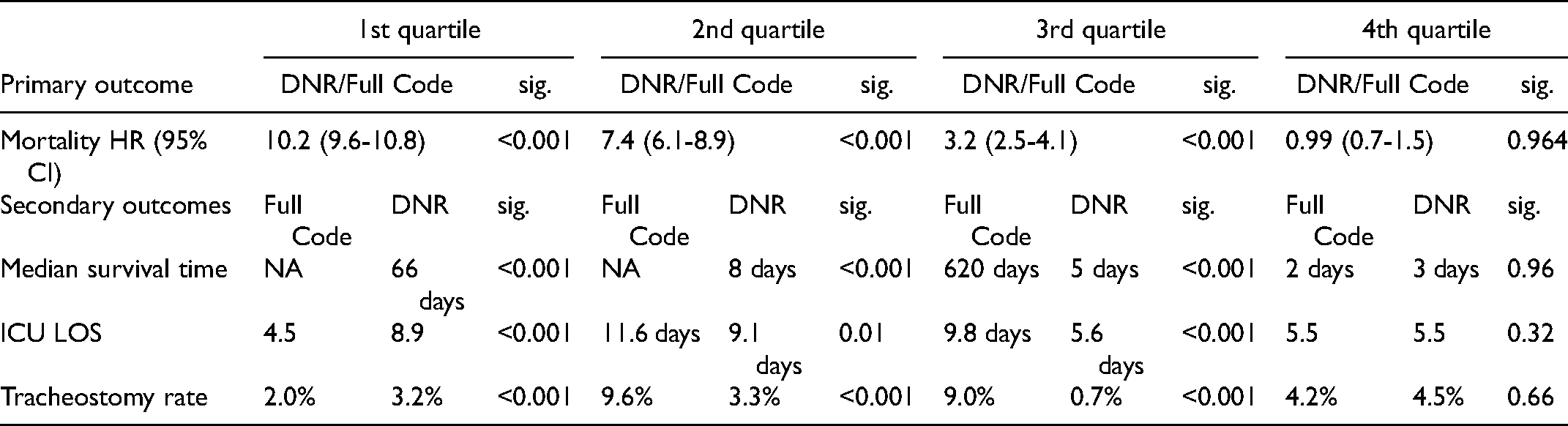
Primary and Secondary Outcomes. Quartiles 1–4 are Predicted Mortality Quartiles by Apache IV Score (ie 0% to 25% Predicted Mortality, >25% to 50% Predicted Mortality, etc).
Secondary Outcomes
Median survival times were significantly greater for Full-Code patients in the first through third quartiles, but not significantly different in the fourth quartile. For the first two quartiles, Full-Code patients’ mortality did not cross the 50th percentile so median survival time could not be calculated for these groups. ICU LOS was longer for Full-Code patients in the second and third quartiles (11.6 vs. 9.1 days, p = .01 and 9.8 vs. 5.6 days, p < .001). ICU LOS was similar between Full-Code and DNR patients in the fourth quartile (5.5 vs. 5.5 days, p = .32). Tracheostomy rates showed a similar trend.
Discussion
We hypothesized that Full-Code status provides no survival benefit over DNR status among patients with high predicted mortality in the ICU, and our data supports this assertion. We also identified a stepwise decrease in survival benefit for Full-Code patients when compared to DNR patients as illness severity increases, which suggests a possible ceiling effect of Full-Code resuscitation for improving survival.
These outcomes are in line with observational studies of CPR recipients that found zero or near-zero percent survival among high Apache Score patients.3–5 We build on these studies by including a matched control group to generate survival differences between Full-Code and DNR patients. Absent the ability to randomize patients to CPR or no CPR when cardiac arrest occurs, we feel this represents a conservative and valid approach for analyzing the effect of CPR in a controlled manner. These outcomes may not be specific for defining with great granularity an Apache Score beyond which Full-Code status should not be allocated. These findings should be validated with larger data sets across greater time frames. Nonetheless, we identified a concerning trend worthy of discussion and further inquiry.
Second, like Fuchs et al identified, being assigned a DNR status at the time of admission is an independent risk factor for mortality, possibly due to less intense treatment given to DNR patients based on the status alone. It is unclear if this is due to providers offering less care overall or a package of treatment limitations chosen by the patient or family. 13 While likely not captured in our matching algorithm, this bias strengthens our findings because, despite likely receiving more intense treatment overall, Full-Code patients still had no difference in mortality when compared to DNR patients in the fourth quartile. Fuchs et al found a 60.7% 1-year crude mortality rate for all DNR patients in their study. Given the high long term mortality rates in even the lowest risk group in our data (first quartile), we performed a post-hoc analysis to compare our crude mortality rate of DNR patients with that of Fuchs et al. We identified a rate of 78.0% for all DNR patients with a median follow up time of 760 days. While this morality rate is 18% higher than what Fuchs et al, identified, our timeframe is more than twice as long. This suggests that our data is in line with the findings of Fuchs et al.
Some clinicians perform “slow codes” in futile patients. These are resuscitations carried out slowly or by omitting the most aggressive measures, with the intention that the patient will expire. 18 This practice cannot be justified within the confines of modern ethics. It is, by definition, a morbid, resource-intensive resuscitation with no goal of survival by those performing it. Our outcomes suggest that patients with a high risk for mortality may not be CPR candidates. Should further research confirm these findings, it might obviate the need for the ethical contortions forced on clinicians when being asked to run futile codes.
Futility of Full Code resuscitation in certain patient groups does not mean futility of other interventions. Any intervention, where indicated, should be made in accordance with the mutually agreed upon goals of care established among providers and patients. We suggest that code status be viewed as a consent for a procedure, not an implication for goals of care.
We also expected higher LOS in the fourth quartile because prior studies showed increase cost among CPR recipients who transiently survived. 2 However, ICU LOS and tracheostomy rates were higher for Full-Code patients only where Full-Code status had a survival benefit (second and third quartiles) but were the same where there was no survival difference (fourth quartile). Lack of an increase in LOS implies less of an economic impact of CPR in futile patients than we hypothesized. This makes sense because we found no survival benefit for Full-Code status at 24 hours in the fourth quartile. Therefore, no increased LOS in this group should be seen. Second, ICU LOS was longer for DNR patients in the first quartile. One explanation may be that these patients are generally more frail or ill than their Full-Code counterparts, even after matching. If that is the case, this might further strengthen our findings, because despite being presumably stronger and healthier than their matched DNR counterparts based on this observation, there was still no survival difference seen in the fourth quartile.
Data is lacking on whether patients that die while receiving CPR perceive the morbidity of resuscitation. Nonetheless, providers are not obligated to administer futile care, 12 and doing so at the expense of limited resources and provider mental health may be costly. Narrowing the indications for emergent, end-of-life resuscitation based on outcomes and patient dignity has precedence, such as in surgical resuscitative thoracotomy. 19 Therefore, we ask, as others have, “… why is the act of ‘cutting’ viewed differently from the act of intubating and ventilating, or compressing and shocking? The bodily integrity of the patient is violated in both”. 20 Our outcomes do not support the use of CPR in ICU patients that have greater than 75% predicted mortality by Apache IV score.
Limitations
Frequent changes in code status makes group allocation difficult. We used an algorithm based on logic and clinical experience because we felt intention-to-treat or per-protocol analysis would introduce systemic bias. Our DNR groups had poor long-term survival, even in the first quartile (36.8% at six months), which would be expected for appropriately classified DNR patients. This finding is also in line with prior study, as discussed above. However, our classification is imperfect due to its retrospective nature and may introduce bias in ways we are unaware of.
The reasons for assigning DNR status in the first quartile may differ systematically from those in the fourth quartile. We identified that survival differences decrease as predicted mortality increases in a stepwise manner. This limitation may confound that linear association and weaken its strength.
We did not abstract data on if patients received non-invasive positive pressure ventilation (NIPPV), which may be an important caveat when calculating the Apache-IV score. The variation in types of NIPPV, how long it was administered, and the indications present challenges in abstraction and incorporation into this sort of analysis. For example, some patients have orders for home CPAP, and the level of FiO2 is variable by mode. This may represent a limitation of our study.
Lastly, DNR status is an independent risk factor for mortality. 13 This bias is likely embedded in our outcomes and exaggerates absolute survival differences between DNR and Full-Code patients. Therefore, any inaccuracy introduced by this bias may imply that our outcomes are conservative and strengthen our outcomes.
Conclusion
Our study showed that Full-Code status provides no survival benefit over DNR status for patients with a predicted mortality greater than 75% by Apache IV score. We suggest that it is reasonable to consider making a very high predicted mortality by Apache IV score a contraindication to CPR. Patient dignity at the end of life means recognizing the limits of our medical abilities, such as the futility of Full-Code resuscitation demonstrated in patients with a very high predicted mortality by Apache IV score. Confirmatory studies with similar methods and larger datasets may better delineate a cutoff beyond which CPR should not be offered.
Footnotes
Acknowledgments
The Authors would like to acknowledge the following individuals for their encouragement, advice, and assistance: Drs. Bruce Barton, Clark Murray, Ricardo J. Bello, Eric Finnesgard, Jonson Yee, Jon Dorfman, and Mark Maxfield.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.