
Abstract
Keywords
Introduction
Severe accidental hypothermia (AH), defined as an involuntary decline in core temperature to <28 °C, 1 accounts for an average of over 1300 deaths per year in the United States (US).2,3 Extracorporeal Cardiopulmonary Resuscitation (E-CPR) use is associated with improved outcomes, 4 and is recommended in current guidelines.1,5,6
Prior publications reporting the success of E-CPR for cardiac arrest due to AH have described cannulation techniques performed primarily by cardiovascular surgeons7–12 with a neurologically intact survival ranging from 26.5% 9 to up to 90% 13 at established centers. To our knowledge, none of the studies was performed in the United States using intensivist physicians (IPs) as cannulating proceduralists.
In 2017, we created an intensivist led extracorporeal life support (ECLS) team using IPs as cannulators for both veno-venous (V-V) and V-A ECLS. E-CPR is part of our ECLS program, and IPs respond to all cardiac arrests arriving in the Emergency Department (ED). We aimed to evaluate the use of E-CPR for patients undergoing out-of-hospital cardiac arrest (OHCA) due to AH in the United States at a center with IPs as cannulators.
Methods
Setting
This study was conducted at the University of New Mexico Hospital, a 550-bed academic hospital located in Albuquerque, New Mexico that is a level 1 trauma center, an accredited stroke center, and an Extracorporeal Life Support Organization (ELSO) center of excellence. It is the tertiary care center for the state of New Mexico. Albuquerque has an altitude of approximately 5000 feet (1524 meters) and is located in a high desert climate. While average daytime temperature in January is 47 °F (8 °C), nighttime temperatures rapidly drop to an average of 26 °F (−3 °C). 14
In 2017, we created an adult ECLS program using intensivists as both the primary managers of patients requiring ECLS and the cannulators for both (V-A) and (V-V) ECLS. E-CPR plays a central role in this program. IPs respond to all cardiac arrests arriving to the ED during the daytime, and are available within 30 minutes at night. If a patient does not have return of spontaneous circulation within 15 minutes and meets pre-specified inclusion criteria, 15 the patient is cannulated for V-A ECLS per protocol. At our center, E-CPR is also the standard therapy for patients with cardiac arrest and a core temperature less than 32 °C as long as the potassium level is less than 12 mmol/L. V-A cannulation is achieved percutaneously using a bifemoral configuration, with a 25- or 27-french multistage drainage cannula (Maquet, jostra Mezinitechnik AG, Hirrlingen, Germany) in the common femoral vein and a 15- to 17-french single-stage return cannula in the common femoral artery. When possible, cannulation using a bilateral approach is performed. A unilateral approach may be used in complex cases. ECLS flow is commenced following cannula placement using a RotaFlow® (Maquet, Jostra Mezinitechnik, AG, Hirringen, Germany) or CardioHelp® (Maquet, Jostra Mezinitechnik, AG, Hirringten, Germany) pump system with a Quadrox-iD® oxygenator (Maquet, Jostra Mezinitechnik, AG, Hirringen, Germany). Patients receive 5000–7500 units of heparin at the time of cannulation. When necessary, lower extremity ischemia is treated with a reperfusion cannula placed by a vascular surgeon.
Once on ECLS, patients are rewarmed quickly until defibrillation into sinus rhythm, which is attempted once at every 2 °C rise in temperature, can be achieved. Patients are then rewarmed slowly (∼0.25 °C per hour) to a goal temperature of 36 °C and maintained at that temperature for forty-eight hours, unless the patient has immediate return of neurologic function. Patients are assessed daily for liberation from ECLS. Decisions regarding weaning and decannulation are made by the attending intensivist. Decannulation from V-A ECLS is typically performed in the operating room by a vascular surgeon.
Population and Data Collection
This retrospective study was approved by the University of New Mexico Institutional Review Board and informed consent was waived. We reviewed all patients treated with V-A ECLS between January 1, 2017 and November 1, 2021 and identified all patients placed on ECLS for hypothermic cardiac arrest. We reviewed the electronic medical record and collected the following data: age, sex, cause of hypothermia, initial core temperature, initial cardiac rhythm, time from arrest to cannulation, time from arrival in the ED to cannulation, initial serum lactate level, initial serum potassium level, initial serum pH, Hypothermia Outcome Prediction after ECLS (HOPE) score, duration of ECLS, hospital length of stay, mortality, and Cerebral Performance Category (CPC) score at discharge.
Results
Nine patients were identified with OHCA due to AH as the indication for initiation of V-A ECLS. The patient characteristics and initial biological data are presented in Table 1.
Patient Characteristics and Initial Biological Data.
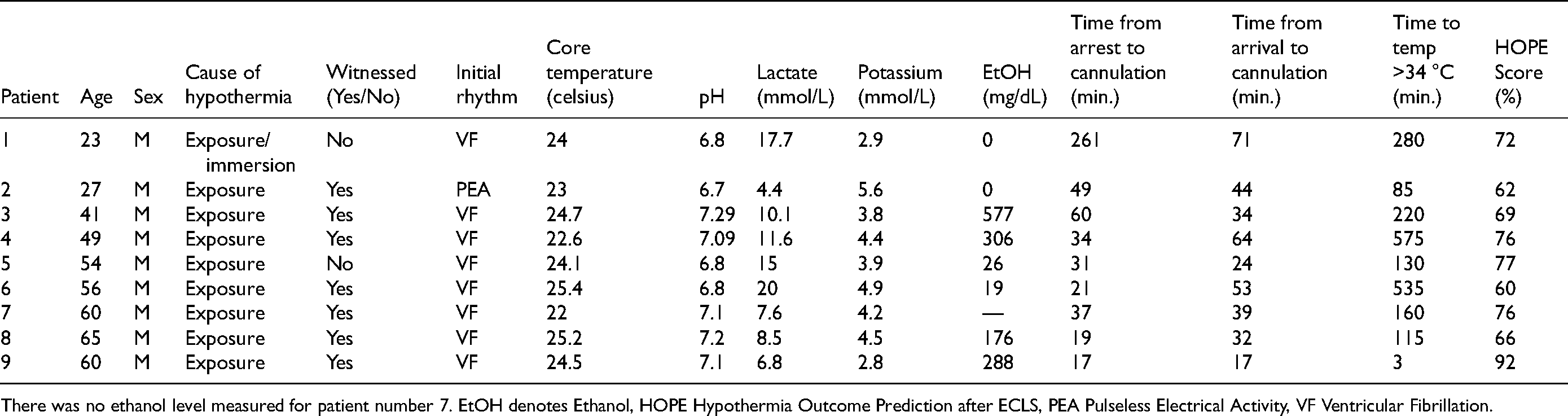
There was no ethanol level measured for patient number 7. EtOH denotes Ethanol, HOPE Hypothermia Outcome Prediction after ECLS, PEA Pulseless Electrical Activity, VF Ventricular Fibrillation.
The average age was 48 years old. All patients were male. All arrests involved exposure in a cold weather environment with one patient having a simultaneous water immersion event. Seven arrests (78%) were witnessed. All patients were in active cardiac arrest during cannulation for V-A ECLS. Three patients developed cardiac arrest in the field, two arrested during ground transport, and four patients had cardiac arrest shortly after arrival in the ED. For the six patients who developed cardiac arrest prior to arrival, the mean time from cardiac arrest to arrival in the ED was 55.5 min (range 5 to 180 min). The mean time from cardiac arrest to initiation of ECLS was 58 min (range 17 to 251 min). For the four patients that arrested after arrival, the mean time from ED arrival to the initiation of ECLS was 42 min. The mean initial core temperature was 23.8 degrees Celsius (range 22-24.4 degrees Celsius). The initial rhythm was ventricular fibrillation (VF) in 8 patients and pulseless electrical activity (PEA) in one. Four patients had a blood alcohol content above 80 mg/dL, the legal limit for impaired driving in the state of New Mexico. The mean initial pH was 6.98 and the mean lactate was 11.3 mmol/dL (range 4.4-17.7 mmol/dL). The mean HOPE 7 score survival predictability was 72.2% (range 60-92%).
Patient outcomes are presented in Table 2. The mean duration of ECLS was 39.1 h (range 2-109). The mean hospital length of stay was 10.2 days (range 1.3 to 20.7). Five patients were discharged home, 2 patients were discharged to an acute rehabilitation facility, 1 patient was transferred to a skilled nursing facility, and 1 patient was transferred to a Veteran's Administration hospital. All nine patients had a CPC score of 1 or 2 at the time of discharge or transfer.
Patient Outcomes.
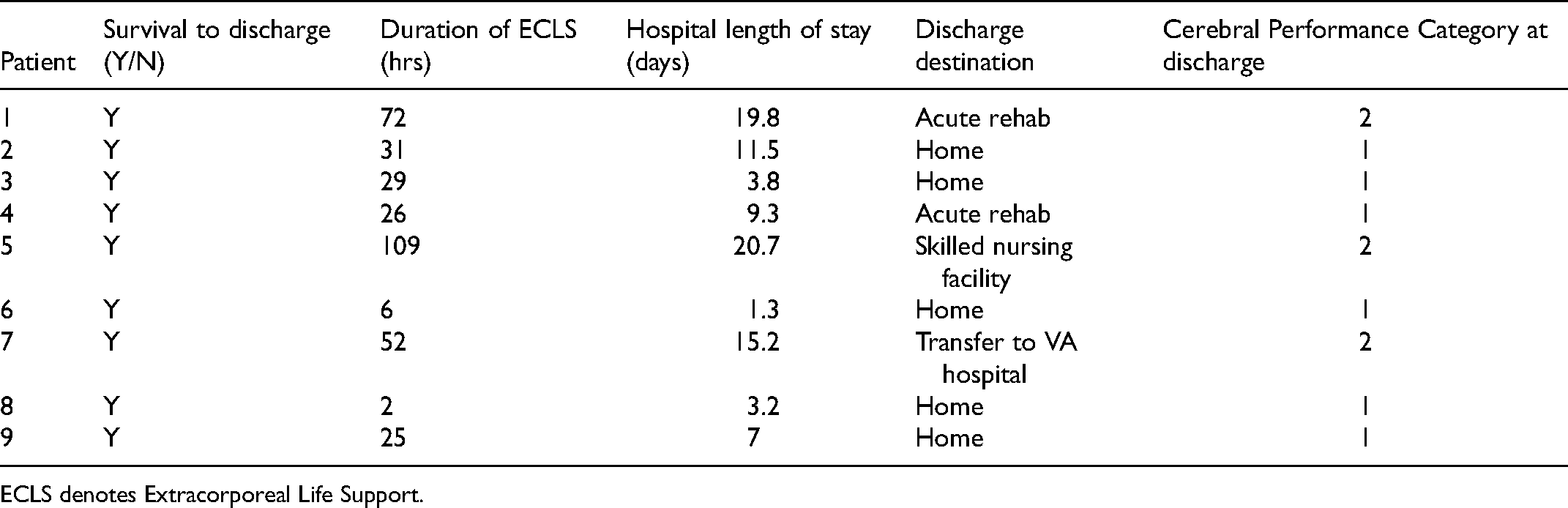
ECLS denotes Extracorporeal Life Support.
Discussion
We present nine consecutive patients over a 4-year period that presented with cardiac arrest due to AH treated with ECLS who survived with a favorable neurological outcome. To our knowledge, this is the largest report of consecutive patients with cardiac arrest due to AH with a 100% favorable neurological outcome. This occurred despite prolonged downtimes, relatively advanced age, and markedly elevated lactate levels, all of which would be associated with poor survival in other forms of cardiac arrest 16 and E-CPR. 17
In an analysis performed by Pasquier et al, 7 the average duration of CPR prior to cannulation was 106 min in survivors and 120 min in nonsurvivors, a statistically significant difference. The average time from arrest to cannulation in their study was 120 min, with an overall survival rate of 37%. In our series, one patient was transferred to two facilities while undergoing CPR prior to ECLS cannulation and therefore had a CPR duration of 251 min. If that patient is excluded, the average time from cardiac arrest to cannulation was 34 min. This was enabled by the availability of an IP for cannulator at all times as part of our hospital's E-CPR program, which likely contributed to the high survival rate seen in this case series.
It should be noted, however, that three of the patients were cannulated after a duration of CPR longer than the sixty minutes recommended by the ELSO 15 and all survived with a favorable neurologic outcome. This is consistent with prior data7,9 indicating that duration of CPR, though inversely correlated with survival, is not prohibitive, and in our study one patient survived with a favorable outcome after nearly four hours of CPR. In fact, neurologically intact survival after cardiac arrest from AH after over six hours of CPR has been reported. 18 Potassium levels have been shown to be informative in determining whether or not resuscitation should continue in cardiac arrest due to AH. 7 In this case series, all patients had normal or nearly normal potassium levels and none had potassium levels above 12 mmol/L, a criteria for withholding ECLS for cardiac arrest due to AH at our center. 1 The HOPE score, an established prediction model for survival in hypothermic cardiac arrest, 7 predicted a high likelihood of survival in the patients in this series.
Mean duration of ECLS support in our patients was 39.1 h (1.6 days), which is shorter than the 78 h (3.25 days) reported in other survivors of E-CPR. 19 Further, the mean hospital length of stay was 10.3 days, which is substantially lower than the hospital length of stay seen in other studies involving E-CPR for OHCA. 20 This is likely due to the more immediate reversibility of hypothermia as a cause of cardiac arrest, as well as the relative lack of need for interventions other than rewarming.
The state of New Mexico is a high-desert environment that often sees temperatures well above freezing during the day, even in mid-winter. At night the temperature rapidly drops, often well below freezing. This creates an environment where people may be comfortable outside during the day but rapidly develop hypothermia at night, leading to a relatively high frequency of cardiac arrests due to AH. In similar geographic regions, a readily available, rapidly deployable E-CPR program may be useful.
At our center, employing IPs as cannulators enabled the development of a rapidly deployable E-CPR program. The use of IPs for cannulation has been shown to be safe and effective21,22 and there were no cannulation complications in this series. Using IPs as cannulators may decrease response time due to the lack of competing operating room obligations. Our IPs are also the primary managers of patients on ECLS and manage the patients from time of admission to discharge. This may contribute to the high survival seen in this series.
Limitations
This is a single-center case series with no control group, so it is impossible to determine whether standard rewarming would generate similar outcomes, although the outcomes in our case series are superior to those reported in cohorts without E-CPR. 23 The cohort in this study was also entirely male, all were found outdoors, and a majority had an elevated blood alcohol level. Hence, this group does not represent the wide variety of patients that are known to present with hypothermic arrest, such as victims of avalanche or prolonged immersion. Further, though the patients in our cohort did not have clinically apparent neurological deficits at discharge, we were not able to perform long-term follow-up or neuroimaging to evaluate for milder forms of cognitive impairment. However, prior evidence suggests minimal cognitive impairment in this patient population. 11
Conclusion
We present the largest reported case series of consecutive patients with cardiac arrest due to AH who all survived with a favorable neurologic outcome after being treated with an intensivist-led E-CPR system. Larger cohort studies are needed to further elucidate the effect this E-CPR system may have on survival in OHCA due to AH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.