
Abstract
Introduction
Many patients who pass a spontaneous awakening trial (SAT) and spontaneous breathing trial (SBT) do not undergo extubation that day. We aimed to identify predictors of extubation on the day of passing an SBT and to develop prediction models for extubation among mechanically ventilated patients.
Methods
In a cohort of mechanically ventilated patients who had passed an SBT in a single, academic medical intensive care unit (ICU) from 2018 to 2019, we developed a logistic regression model for identifying predictors of extubation.
Results
Of 745 patients in our study, 77% were extubated the day they passed a SBT. Independent predictors of extubation included higher Richmond Agitation Sedation Scale (RASS) (−2 compared to −4: odds ratio (OR) 1.83, 95% confidence interval (CI) 1.56 to 2.14), receipt of sedation on the day prior (OR 2.12, 95% CI 1.63 to 2.74), absence of diagnosis of sepsis or septic shock (OR 0.77, 95% CI 0.59 to 1), absence of neurological illness (OR 0.59, 95% CI 0.37 to 0.96), indication for intubation of altered mental status, seizure, or agitation (OR 1.67, 95% CI 1.05 to 2.65), and absence of hemodynamic instability or cardiac arrest (OR 0.67, 95% CI 0.47 to 0.95).
Conclusion and Relevance
Patients on mechanical ventilation were more likely to be extubated on the day they passed an SBT if they had higher RASS scores, received sedation the day prior, or did not have diagnosis of sepsis, neurological illness, or hemodynamic instability. Future research should attempt to identify and address modifiable risk factors for failure to extubate after passing an SBT.
Keywords
Background
Over 5 million Americans are admitted annually to an intensive care unit (ICU) due to critical illness with approximately 39% of those patients receiving mechanical ventilation during their ICU stay.1,2 Spontaneous awakening trials (SATs) and spontaneous breathing trials (SBTs) have been found to decrease the duration of invasive mechanical ventilation and decrease 1-year mortality.3,4 The decision to extubate patients on mechanical ventilation, however, is complex. Patients who fail extubation have been found to have longer durations of mechanical ventilation, increased likeliness of requiring tracheostomy, prolonged length of stay, increased cost, and mortality. 5
While the majority of patients who pass an SAT and SBT are extubated within 24 h, clinicians defer extubation in a significant minority of patients based on a perceived risk of extubation failure. While risk factors for extubation failure have been extensively evaluated, few studies have identified what variables contribute to a clinician's decision to defer extubation for a patient who has passed an SAT and SBT.
The aims of this study were (1) to evaluate the proportion of patients who are not extubated on the calendar day on which they pass an SAT and SBT and (2) to evaluate the patient factors associated with the decision to delay extubation.
Methods
Study Design and Population
We conducted an observational analysis of prospectively collected data for adults receiving invasive mechanical ventilation in the 35-bed medical ICU at the Vanderbilt University Medical Center in Nashville, Tennessee between July 1, 2018 and June 30, 2021. All data used in the current analysis were collected as part of an ongoing study of oxygen targets during invasive mechanical ventilation, 6 and the results of which will be published separately. The current secondary analysis of de-identified data was approved as exempt nonhuman subjects research by the Institutional Review Board at the Vanderbilt University Medical Center. The cohort for this analysis included all patients who received invasive mechanical ventilation in the study ICU during the study period except those who were prisoners, those who were pregnant, those who were extubated the same day of intubation, and those who received chronic invasive mechanical ventilation at their place of residence prior to ICU admission.
Demographic data, primary diagnoses, and baseline characteristics for patients were collected manually by study personnel. 6 Multiple acute illnesses and indications for intubation were allowed. Pharmacy personnel collected daily information on SATs and SBTs using a structured data collection process that captured for all patients daily: (1) whether the patient passed the SAT safety screen, (2) whether the patient passed the SAT, (3) whether the patient passed the SBT safety screen, and (4) whether the patient passed the SBT. Successful passing of an SAT trial consisted of pausing sedative and analgesic continuous infusions, while allowing intermittent bolus dosing of analgesics for pain as needed. Only the first extubation was considered for each patient encounter.
Statistical Analysis
Continuous variables were summarized as median with interquartile range (IQR). Categorical variables were summarized as a number with percentage (n, %). Chi-square and Wilcoxon rank-sum tests were utilized for univariate comparison.
The primary analysis focused on days on which a patient passed both the SAT and SBT. A multivariable logistic regression was fit to evaluate the relationship between patient variables and the outcome of extubation. Each day a patient passed both the SAT and SBT were included and analyzed independently. Candidate covariables were selected a priori based on clinical experience and prior research on causes of extubation failure. Nonlinearity was allowed for continuous variables using restricted cubic splines with 3 to 5 knots. Performance of the logistic regression model was evaluated by comparing predicted probabilities of extubation with observed probabilities using a bias-corrected concordance statistic to determine the extent of over- or under predicting probability of extubation. The predictive accuracy of the model was quantified using Harrell's concordance index (C-index), 7 which correlates to the area under the receiver operating characteristic curve and values range from 0.5, indicating no predictive discrimination, to 1.0, indicating a perfect separation of patients with different outcomes.8,9 The results were described by number and proportion or median and IQR for dichotomous and continuous variables. Statistical analysis and graphics were conducted using R Version 3.3.2. A significance level of .05 was used for all analyses.
Results
Among patients who received invasive mechanical ventilation in the study ICU between July 1, 2018 and June 30, 2019, 745 patients with 775 unique ICU admissions were eligible and were included in the current analysis. Baseline characteristics are shown in Table 1. Patients had a median age of 58 years (IQR: 45-68), and 37% of patients had comorbidities, including COPD (19%), heart failure with reduced ejection fraction (4%), coronary artery disease (19%), and end-stage renal disease on renal replacement therapy (6%). The most common indication for mechanical ventilation was altered mental status (59%), followed by hypoxic respiratory failure (36%) and hypercarbic hypoxemic respiratory failure (17%). Of the total 745 patients in the study cohort, a total of 171 patients (23%) of patients were not extubated on a day on which they passed an SAT and SBT.
Baseline Characteristics.
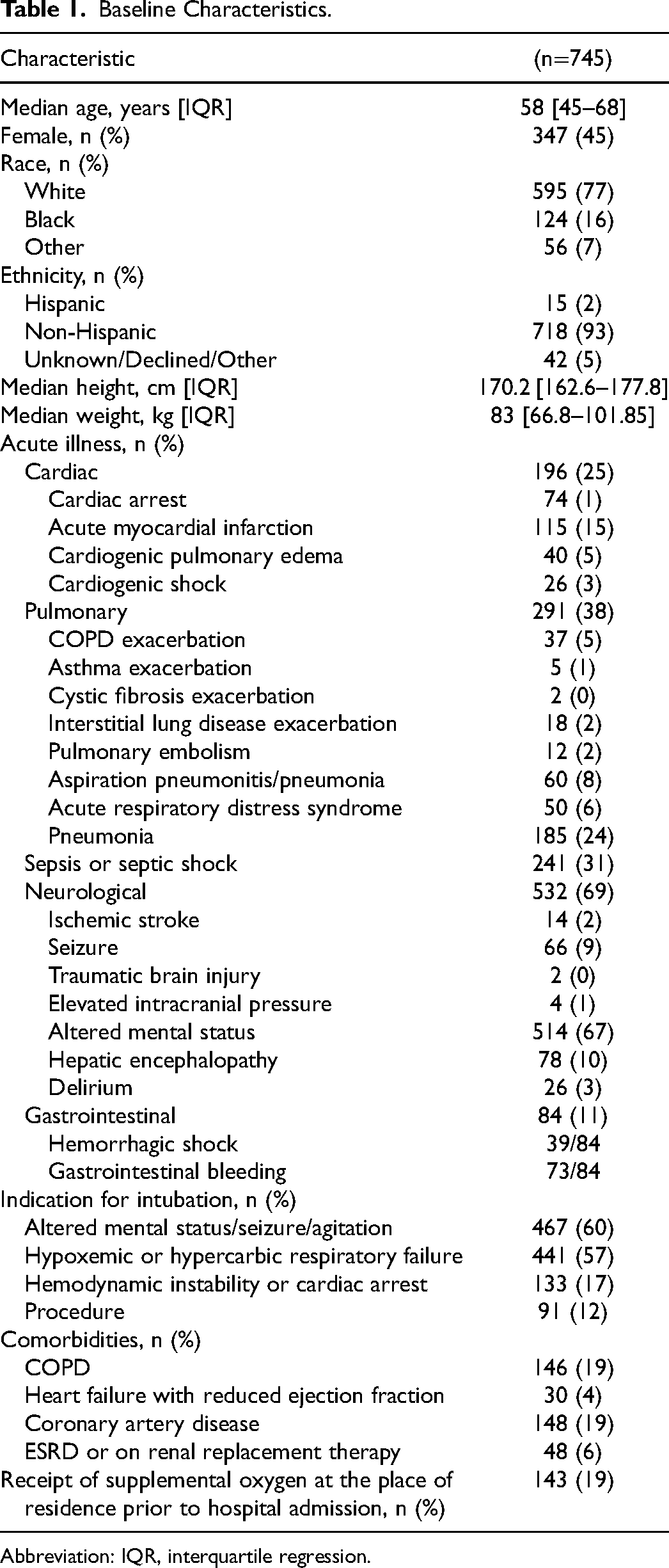
Abbreviation: IQR, interquartile regression.
Logistic Regression Modeling for Risk Factor Identification
Results of the logistic regression model evaluating variables associated with extubation on a day in which the patient passed an SAT and SBT are summarized in Table 2. Continuous variable effects are summarized by comparing 75th to 25th percentiles due to nonlinearity. Variables independently associated with extubation included Richmond Agitation Sedation Scale (RASS) (−2 compared to −4; odds ratio (OR), 1.83; 95% confidence interval (CI) 1.56 to 2.14) (Figure 1), the receipt of sedation on the prior day (OR, 2.12; 95% CI 1.63 to 2.74), sepsis or septic shock (OR 0.77, 95% CI 0.59 to 1), neurological illness (OR 0.59, 95% CI 0.37 to 0.96), and altered mental status, seizure, or agitation (OR 1.67, 95% CI 1.05 to 2.65), hypoxemic or hypercarbic respiratory failure (OR 0.58, 95% CI 0.43 to 0.78), or hemodynamic instability or cardiac arrest as the indication of intubation (OR 0.67, 95% CI 0.47 to 0.95).
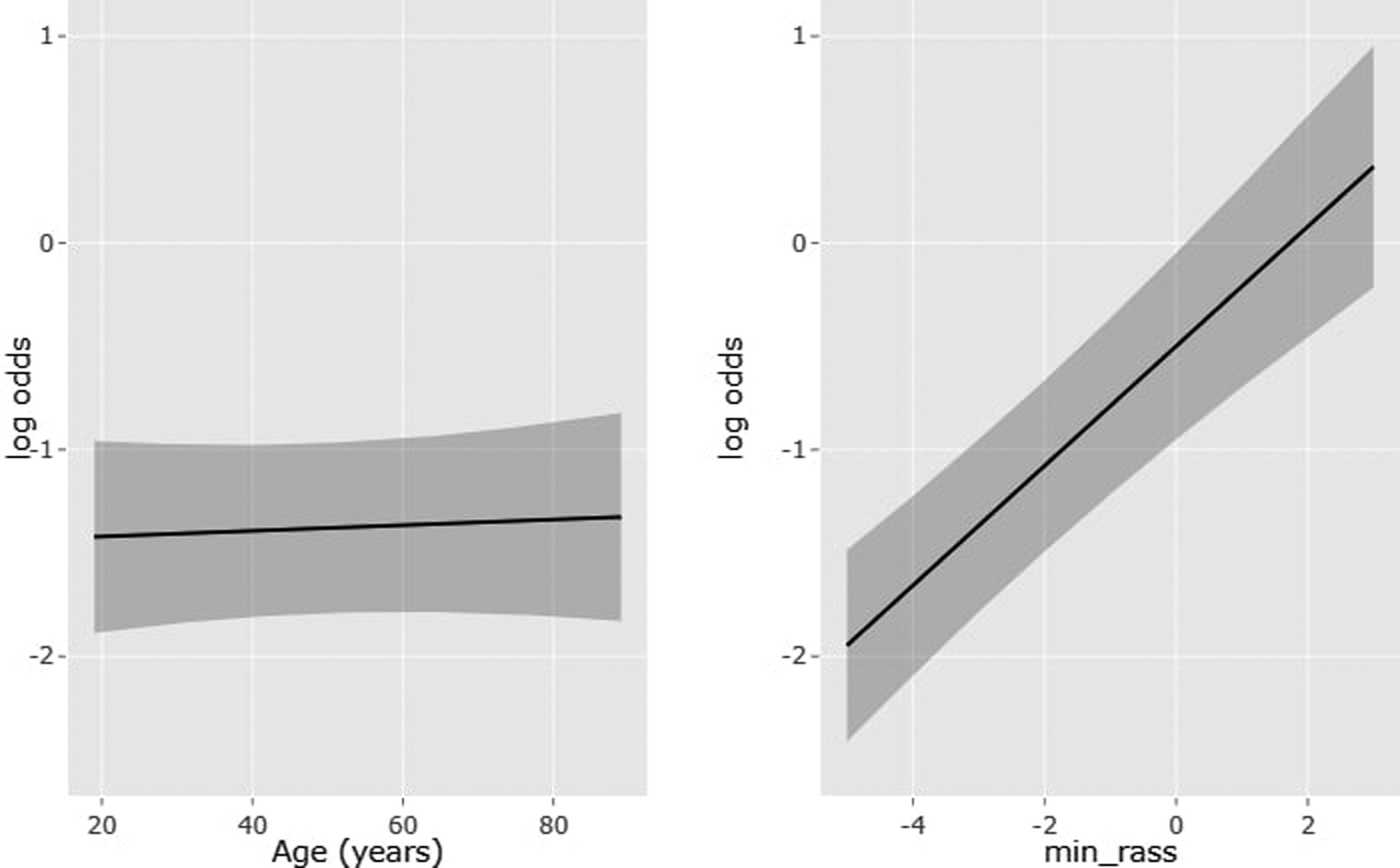
Logistic odds for the variation in risk factors.
Multivariable Logistic Regression.
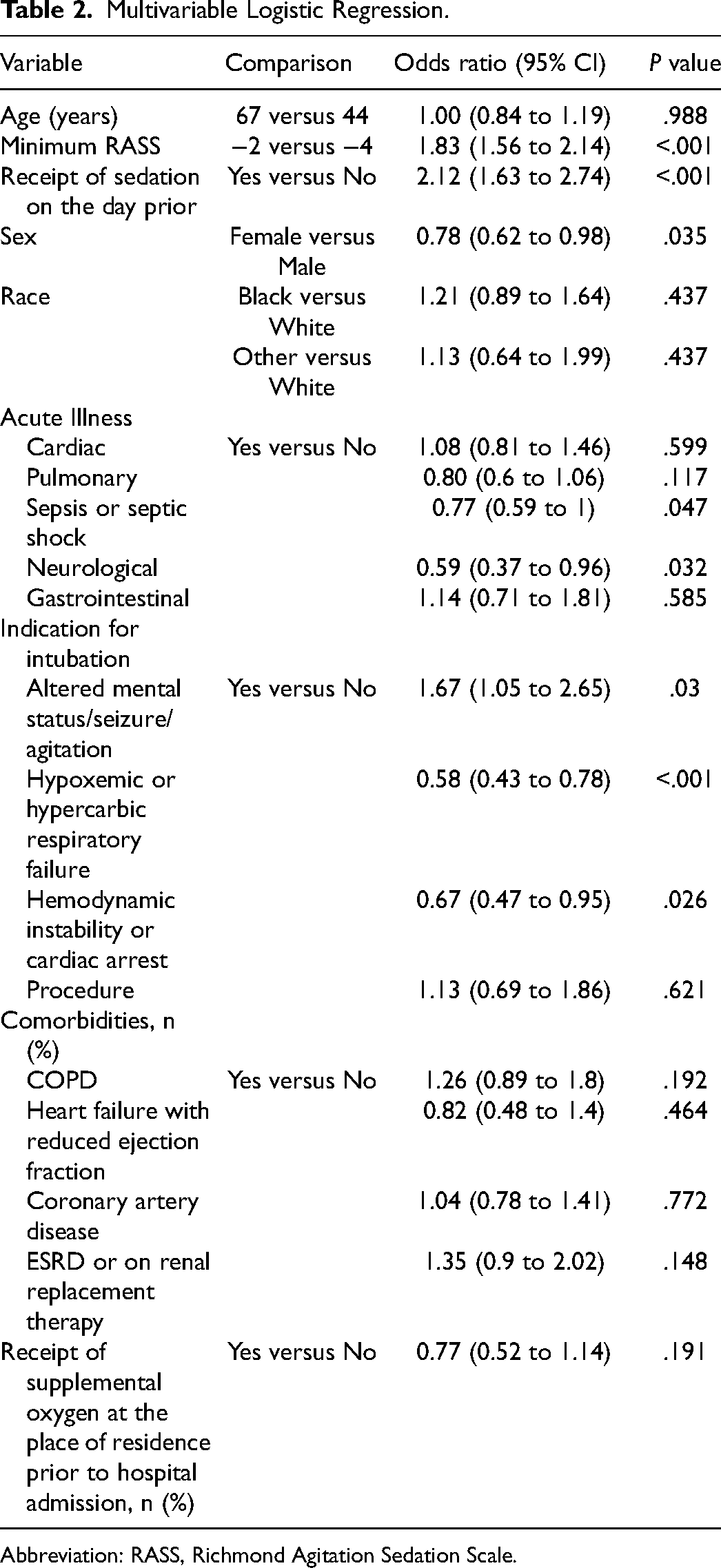
Abbreviation: RASS, Richmond Agitation Sedation Scale.
The C-index of the model was 0.681. Figure 2 shows a calibration plot comparing the predicted probability of extubation to actual probabilities. The mean absolute error was 0.009, with a 0.9 quantile of absolute error of 0.014.
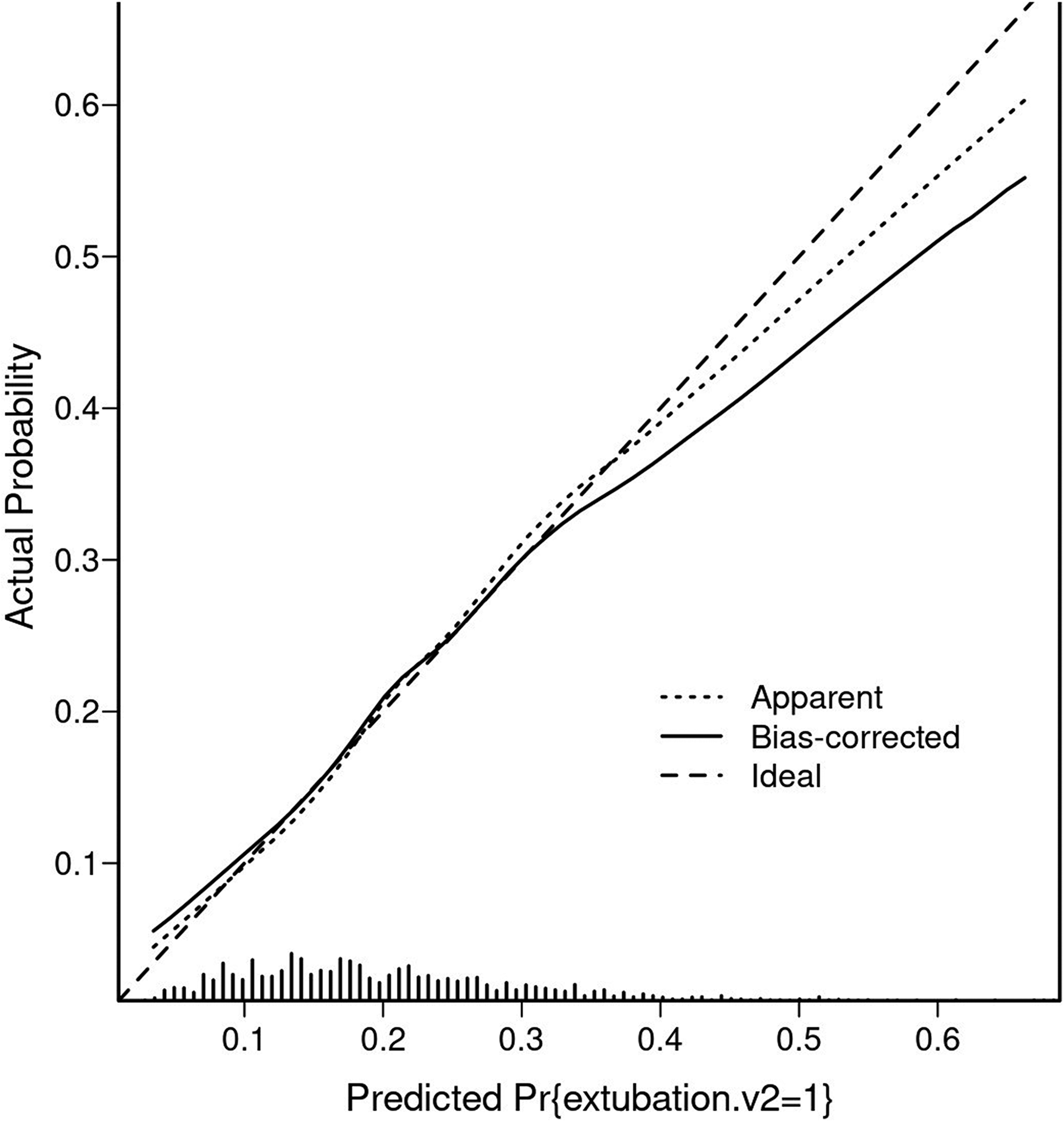
Bootstrapped calibration for the multiple regression model predicting extubation.
Discussion
Our results demonstrate that patients on mechanical ventilation were more likely to be extubated on the day they passed an SBT if they had higher RASS scores, had received sedation the day prior, and did not have diagnosis of sepsis, neurological illness, or hemodynamic instability.
Mechanical ventilation is a life-saving therapy for critically ill patients, but mechanical ventilation also increases the risk of lung injury, pneumonia, and laryngeal injury.10,11 Prior research has shown that SATs and SBTs reduce the duration of mechanical ventilation and improve outcomes for mechanically ventilated patients. 4 It is surprising, therefore, that nearly a quarter of patients who pass an SAT and SBT are not extubated on the day they pass these tests.
While SBTs have been shown to reliably identify patients who are likely to tolerate extubation from the perspective of pulmonary mechanics, it does not directly assess other factors that may be important in extubation failure, including the level of patient's cognition, ability to engage in commands, strength of cough, or ability to clear secretions following extubation. Our finding that patients with higher RASS scores were more likely to be extubated may be related to the fact that patients with low RASS scores are unable to follow commands and handle secretions. Additionally, our results found that patients receiving sedation the day prior to extubation were more likely to be extubated. This finding could suggest that some patients receiving mechanical ventilation but not receiving sedation have reasons beyond pulmonary mechanics for ongoing intubation (eg, impaired neurological function, planned procedure, or upper airway obstruction). Further, this study evaluated sedation in a dichotomous fashion and did not account for medication dosage and duration, which limits the ability to evaluate potential harms from high-dose sedative administration. Our study found no significant association between increasing age and extubation. Additionally, our study found no difference in duration of time between patients passing an SAT and SBT between those who were extubated versus those who were not extubated, nor was there a difference between the time of day the SAT or SBT occurred in those who were extubated versus those who were not extubated.
Prior studies evaluating the causes of failure following extubation have identified multiple risk factors including impaired neurological status, excessive secretions, and increasing age.12,13,14,15,16 Our study suggests that clinicians may incorporate these variables into their decision-making at the time of extubation, as neurologic status and RASS level were also associated with the probability of extubation among those who passed an SAT and SBT. Notably, age was not associated with the probability of extubation despite being associated with extubation failure in many prior studies, which may represent the clinician understanding that while elderly patients are at high risk of failure, their risk of failure will not improve by delaying extubation.17,18,19
Our study has several strengths including a novel research question and a large sample size. The diversity in indications for mechanical ventilation and comorbidities improves generalizability. Our study also has limitations. It was limited to a single site and the variables available for analysis were limited to those collected during the original study. Limited information was available on the dose of sedative medications and non-pulmonary reasons for ongoing intubation (eg, upper airway obstruction, planned procedure). Additionally, patients receiving dexmedetomidine were not analyzed separately. As dexmedetomidine could be used as a bridge to extubation, this raises the risk of confounding for our findings that sedation exposure increased the probability of extubation.
Conclusions
Nearly one quarter of patients who pass an SAT and SBT are not extubated on the day they pass. Higher RASS scores, receipt of sedation on the day prior, and absence of sepsis, neurological illness, or hemodynamic instability are associated with an increased probability of extubation after passing an SAT and SBT. Future research is required to focus on identifying and addressing modifiable risk factors for failure to extubate after passing an SBT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vanderbilt Institute for Clinical and Translational Research (grant number VR54187).