
Abstract
Introduction
Advances in critical care have resulted in an increasing number of post-intensive care unit (post-ICU) survivors.1–6 The coronavirus disease-19 (COVID-19) pandemic has only amplified these numbers.7,8 Given the improvements in ICU-related mortality, increasing attention is being paid to long-term outcomes following critical illness. Many studies have now demonstrated common problems following critical illness, including physical dysfunction, cognitive impairment, and neuropsychiatric disorders including anxiety, depression, and PTSD.9–13 In order to recognize the common problems experienced by survivors of critical illness, a stakeholders’ meeting in 2012 coined the term “post-intensive care syndrome,” or PICS. 14 Other problems have been noted, including but not limited to chronic pain, fatigue, loss of appetite, weight loss, swallowing dysfunction, impaired voice, nutritional deficiencies, a decrease in bone mineral density, hair loss, peripheral neuropathies. Similar to the post-ICU patients themselves, families and caregivers may also be affected by stress, anxiety, depression and PTSD, now termed PICS-family (PICS-F). In addition to the morbidity included in the syndromes of PICS and PICS-F, survivors of critical illness have high rates of healthcare utilization and costs including urgent care visits, emergency department visits, and re-hospitalization, in addition to high rates of mortality.15–21
Despite the very high risk of post-critical illness morbidity and mortality, there is not a routine mechanism or care pathway for survivors of critical illness.22,23 Some specialized centers have created post-ICU clinics (also termed ICU recovery clinics), but these are only available to a small minority of patients.24–26 Rather, the majority of these patients are released from the hospital into the care of their primary care providers (PCPs). Oftentimes, these providers are unaware of the hospitalization, the care the patient received while in the hospital, follow-up testing needed, and/or common sequelae seen due to recent critical illness. This has resulted in disorganized and fragmented healthcare delivery in patients with complex needs.27–29 With this disjointed care model involving multiple clinicians (ie intensivists, hospitalists, PCPs, specialists), there is concern that post-ICU care is not optimal for patients. We sought to assess primary care physicians’ current practice after critical illness, the barriers to care for these patients, and their knowledge of common issues/complications following critical illness, as well as to evaluate ways to improve care for survivors of critical illness. We hypothesize that barriers exist in providing optimal transitional care in the post-ICU period.
Materials and Methods
We designed a survey that was administered on paper or electronically to randomly selected primary care physicians in North Carolina. The study sample was identified using a publicly available list of licensed providers from the North Carolina Medical Board (NCMB) currently practicing in an outpatient setting. Those who were excluded from the study included trainees, advanced practice providers (APPs, ie nurse practitioners and physicians’ assistants), retired physicians, and hospitalists. A random 5% sample was taken, leaving 220 primary care physicians. Note that primary care providers (PCPs) is a term inclusive of primary care physicians and primary care advanced practice providers (APPs; comprised of nurse practitioners (NPs) and physician assistants (PAs)); we only surveyed primary care physicians in this study. The project was approved by the Wake Forest Baptist Medical Center Board (IRB00040688) and was given a waiver of written (signed) consent.
Survey Instrument
A survey was developed to assess the following domains: provider demographics, current practice characteristics, potential barriers to providing care, knowledge of common issues/complications following critical illness, and interest in changing care models for survivors of critical illness. For the purposes of this survey, we defined critical illness as an acute life-threatening condition associated with a risk of organ dysfunction, long-term morbidity, and mortality for which patients are often admitted to an ICU. We also defined PICS as a collection of physical dysfunction, cognitive impairment, and mental health problems among patients who survive a critical illness, and emphasized that PICS included physical deconditioning and disability, dyssomnia, deficits in memory, anxiety, PTSD, and depression.9–13 Respondents were asked to consider patients with severe infection requiring mechanical ventilation or vasopressors as examples of the main drivers of critical illness and we noted that, for this survey, we were not interested in critical illness seen in the post-operative setting. Content experts in critical care, post-ICU care, primary care, and survey methodology reviewed the comprehensiveness, clarity, and face validity of the questions. The survey was then piloted in 12 individuals to assess administrative ease, comprehensibility, flow of questions, and time required to complete the survey. The final paper survey consisted of a 4-page questionnaire with 29 questions which took 5-10 minutes to complete. The electronic version of the survey was identical and contained in REDCap.
Survey Procedure
The questionnaire was first mailed in October 2016, along with a cover letter and pre-stamped return envelope. The cover letter included instructions on how to access an online version of the survey should the respondent prefer this method over returning the paper version of the survey. Subjects who did not respond were mailed a follow-up survey package on 2 subsequent occasions at 3 months and 6 months with a $1 cash incentive. Surveys were accepted until April 2018.
Statistical Analyses
Descriptive statistics were presented as counts and percentages, with means (SD) or medians (interquartile range, IQR) as appropriate. Bivariable analyses of familiarity with PICS, familiarity with PICS-F, whether respondents thought more education would be helpful, whether respondents thought a list of commonly encountered problems would be helpful, and whether respondents thought a special transitional clinic might be helpful were performed to evaluate possible associations with demographic factors and current practice factors. Multivariable logistic regression was used to evaluate these associations while adjusting for other potential factors. Pre-selected variables (based on hypotheses about demographics and practice patterns) were included in the multivariable analysis if their bivariable association had a P-value ≤ .2. Collinearity was assessed using pairwise correlation coefficients between demographics and current practice patterns. Stata version 12.1 (StataCorp, College Station, TX) was used for all analyses. Significant differences between groups are reported at the level of .05.
Results
Respondent Demographics
Of the 220 surveys mailed; 196 total surveys were successfully delivered (Figure 1). Eighty responses were received, 77 of these had complete data (39% effective response rate). Respondents had a median age of 53 (Interquartile Range (IQR) 46-61), 66% were male, and 75% were Caucasian. Sixty-four percent were family medicine physicians; the remainder were internal medicine. Most had been in practice for more than 10 years. Full demographics are in Table 1.
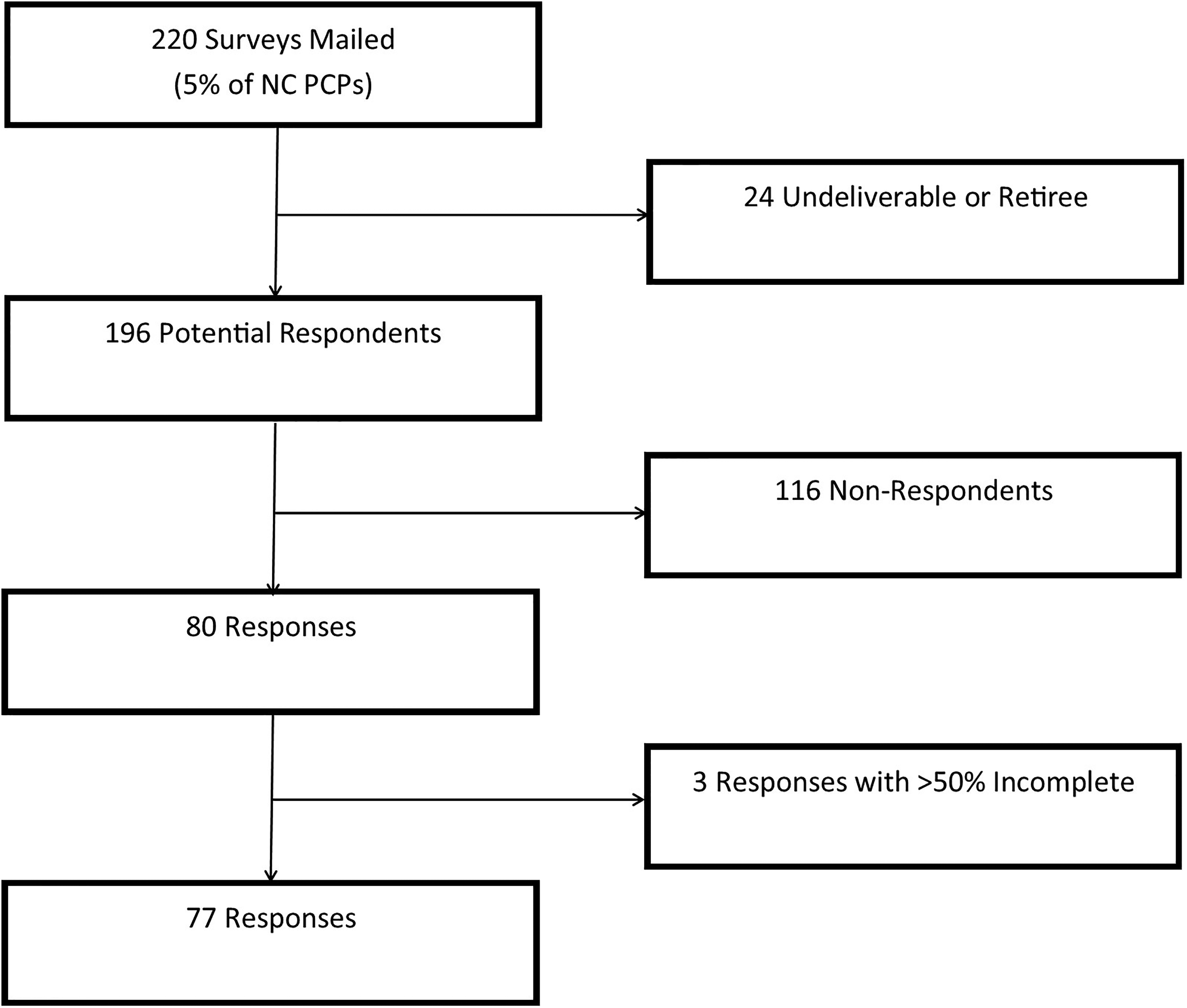
Flow diagram of surveys.
Demographics of the Primary Care Physician Survey Respondents.
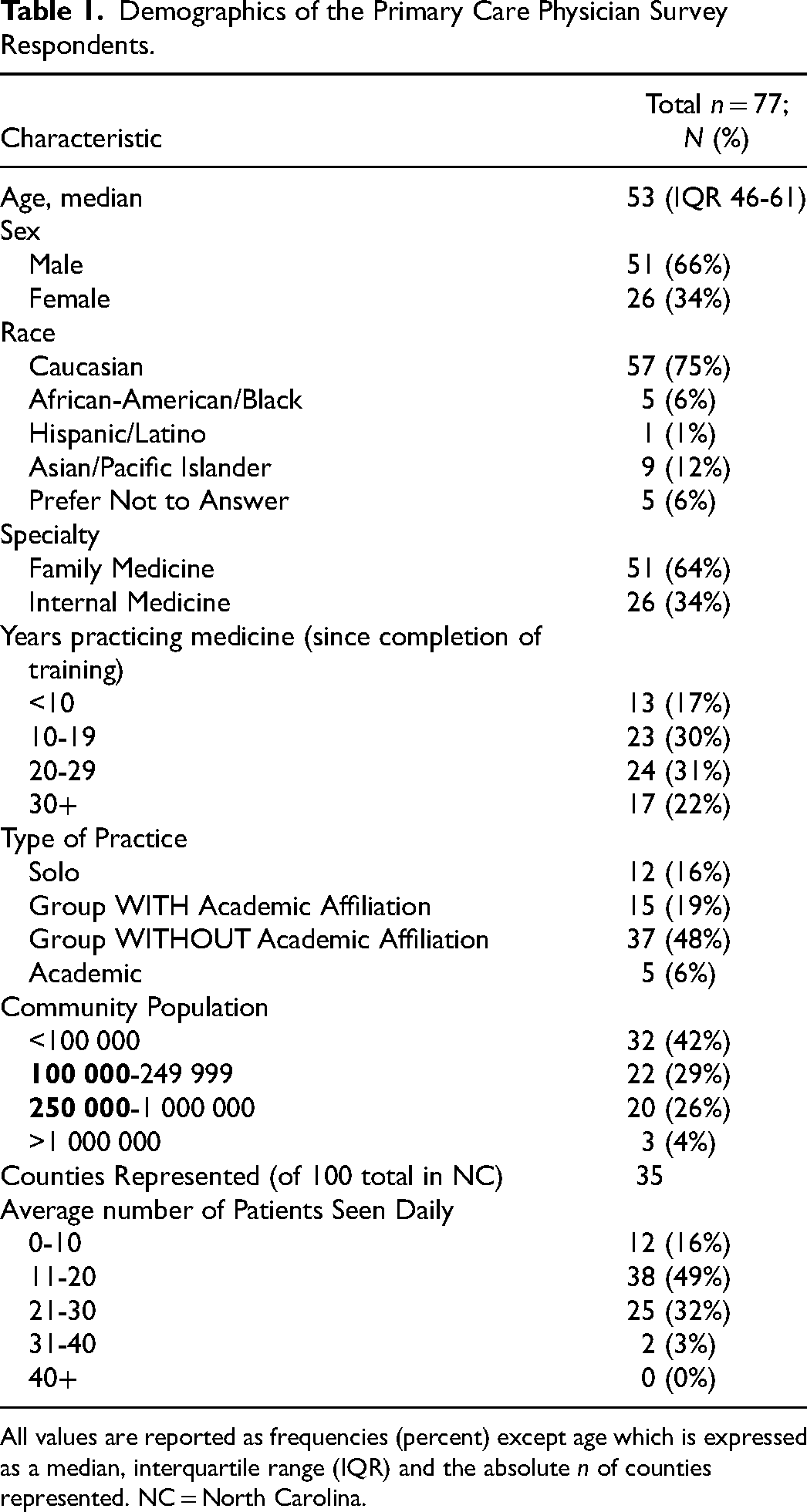
All values are reported as frequencies (percent) except age which is expressed as a median, interquartile range (IQR) and the absolute n of counties represented. NC = North Carolina.
Current Practice Patterns and Potential Barriers to Care
Current practice of primary care physicians is reported in Table 2. Physicians reported seeing approximately 1 or 2 post-critical illness patients per month (21%) or fewer (56%). They spent a median of 30 (interquartile range 30-40) minutes with survivors of critical illness. Sixty-seven percent of primary care physicians did not have a formal or methodical way of assessing survivors of critical illness. End of life issues, including advanced directives and/or limitations to life-sustaining therapies were common topics in these visits (8% always, 36% often, 43% sometimes). Patients were most likely to be referred to physical therapy and occupational therapy.
Current Practice in Post-Critical Illness Patients.
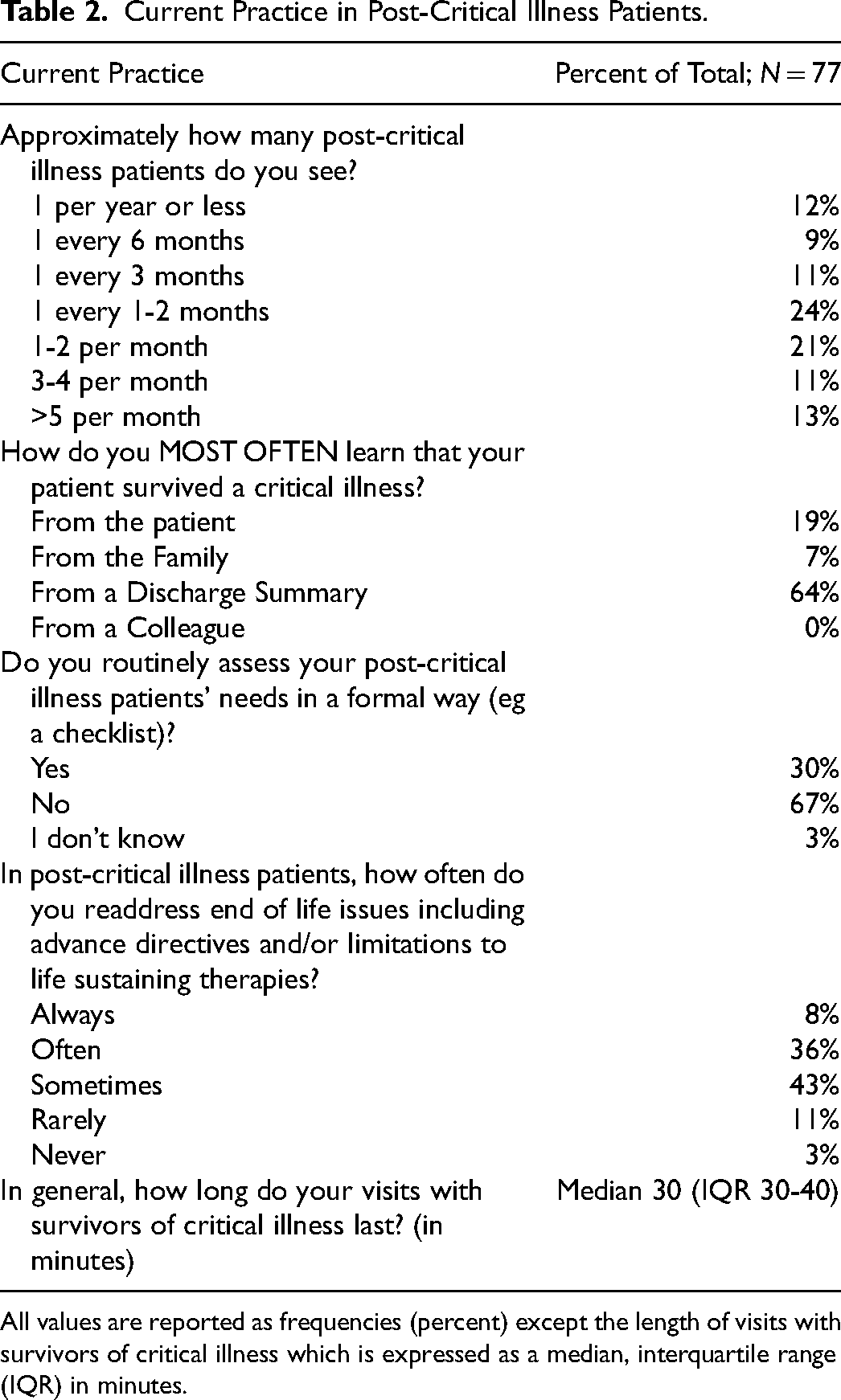
All values are reported as frequencies (percent) except the length of visits with survivors of critical illness which is expressed as a median, interquartile range (IQR) in minutes.
We then surveyed primary care physician respondents about potential barriers to care (Table 3). Only 34% of respondents also noted that they “often” or “always” had enough time to spend with survivors of critical illness during their hospital follow-up appointment; 27% reported “rarely” or “never” having enough time. Seventy-two percent of respondents noted “often” or “always” having an up to date list of medications for their post-critical illness patients; similarly, 71% of respondents noted that they “often” or “always” had a discharge summary regarding the patient's hospital course. Of primary care physician respondents, 22% reported that they “rarely” and 4% that they “never” had a list of test results that were pending for the patient at the time of hospital discharge.
Potential Barriers to Care.
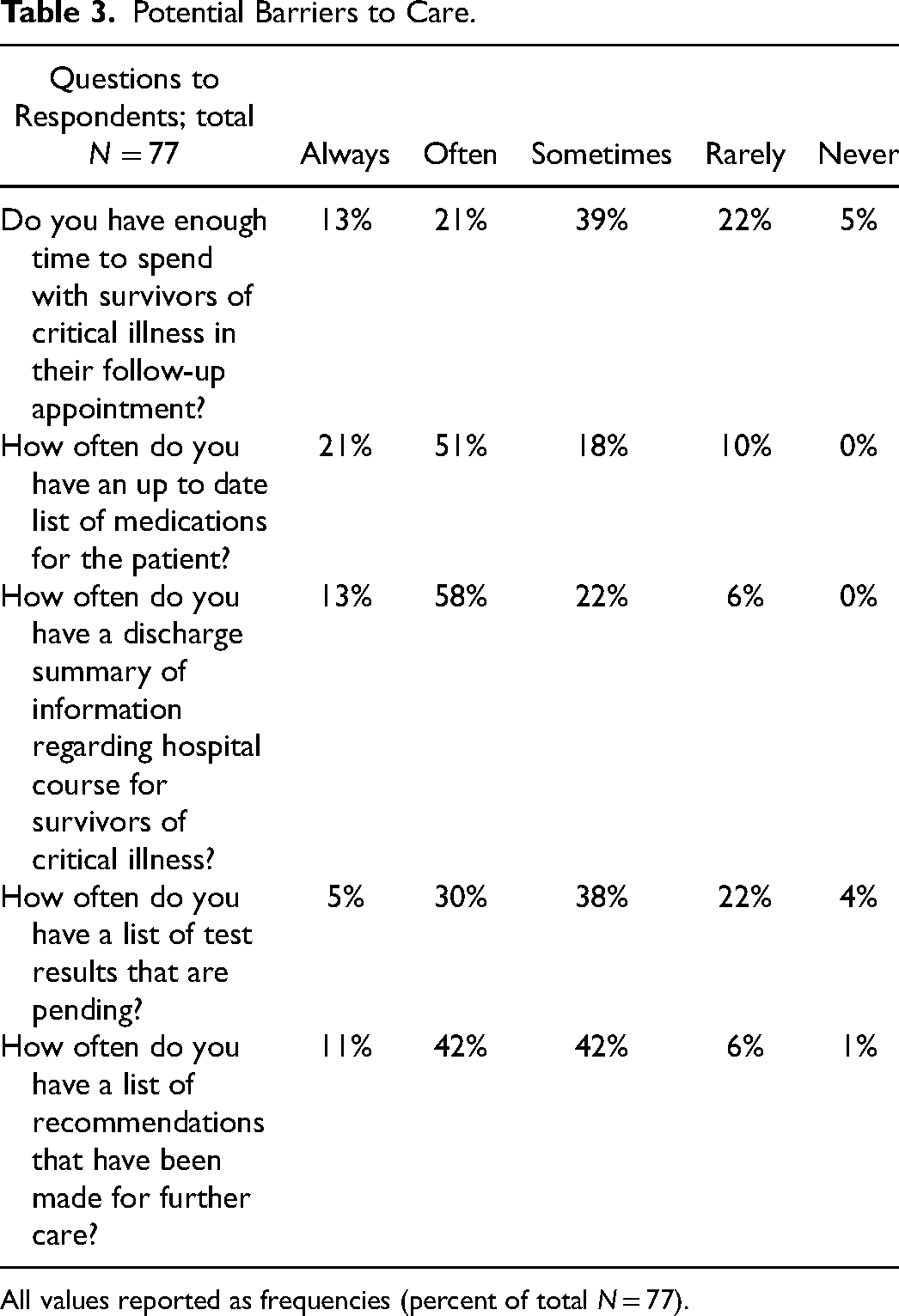
All values reported as frequencies (percent of total N = 77).
Other barriers commonly noted include concerns about coordination of care, with a particular emphasis on lack of personal communication between hospital-based providers and primary care providers as well as discharge summaries (lack of adequacy of them, inconsistency of them from particular institutions, and no receipt of them from skilled nursing facilities or rehab centers); lack of resources, including prescription coverage, home care, transportation, and family support; and lack of timely access to subspecialists. Two examples of excerpts from respondents are below. Respondent 24: “Both Hospital X and Hospital Y now use electronic medical records which are absolutely awful. The dictated discharge summary of yesteryear was way better at relaying pertinent information. Today I rarely see a discharge summary, but rather a clinical care document that mostly consists of ‘copy and paste’ results several pages long with little information I need to know. I might find 1 or 2 useful sentences in 8 or 10 pages of ‘fluff.’ It should be an embarrassment to the institution.”
Respondent 59: “Those caring for my patients in hospital don't know the patient, their family, or me, and they don't often care about my long term relationship. That plays out in ways that are disadvantageous to good care.”
Knowledge of Common Issues/Complications After Critical Illness
We also assessed knowledge of common issues/complications following critical illness. Sixty-five percent of primary care physician respondents reported that they were not familiar with the term PICS and 81% reported that they were not familiar with the term PICS-F. Despite a lack of awareness of terminology regarding PICS and PICS-F, many respondents listed elements of PICS and PICs-F when asked about what they “perceive as the top 5 common problems/medical complaints for patients following critical illness.” This included 36% of respondents who reported trouble with physical function, 27% who reported concerns for neuropsychiatric impairments (anxiety, depression, PTSD), 10% who reported concerns about cognitive impairment, and 14% who reported concerns about family support, family stress, and financial issues (PICS-F).
Potential Changes in Care Models for Survivors of Critical Illness
The majority of primary care physician respondents thought more education regarding PICS and PICS-F would be helpful (84%). Ninety-one percent of respondents thought a list of commonly encountered problems in the post-critical illness population would be helpful. The utility of a specialized transitional clinic (eg post-ICU clinic or ICU Recovery Clinic) was endorsed by 57% of respondents; 26% were not sure about the utility of such a clinic and 17% did not think such a clinic would be helpful. Most (62%) primary care physician respondents noted being comfortable caring for their patients after critical illness, but a substantive 27% did not. Respondents overall (75%) felt like they were aware of common problems encountered following critical illness and 88% reported that they felt like they knew when to refer post-ICU patients to specialists. Only 19% thought patients and their families were educated about common problems encountered in survivors of critical illness.
Bivariable and Multivariable Analyses
In bivariable analysis (Table 4), familiarity with PICS and PICS-F may be more common in physicians who had been in practice longer (P = .06 for PICS; P = .08 for PICS-F). Also, non-academic physicians reported more familiarity with PICS (43% vs 20%, P = .01) and PICS-F (21% vs 2%, P = .03) than academic physicians. In multivariable analysis, the only significant association was that non-academic physicians reported familiarity with PICS (OR 0.25 (0.08-0.73, P = .01). No other factors were significant in bivariable or multivariable analysis for familiarity with PICS or PICS-F. Similarly, in analyses looking at associations between a desire for more education, interest in a list of common problems encountered in the post-critical illness population, and interest in a specialized transitional clinic, we did not find any associations with any demographic information collected. There was a strong association between a desire for more education (84%) and interest in a list of common problems encountered in the post-critical illness population (91%), P < .001.
Bivariable and Multivariable Analyses for Familiarity with PICS and PICS-F and Demographic and Current Practice Factors.
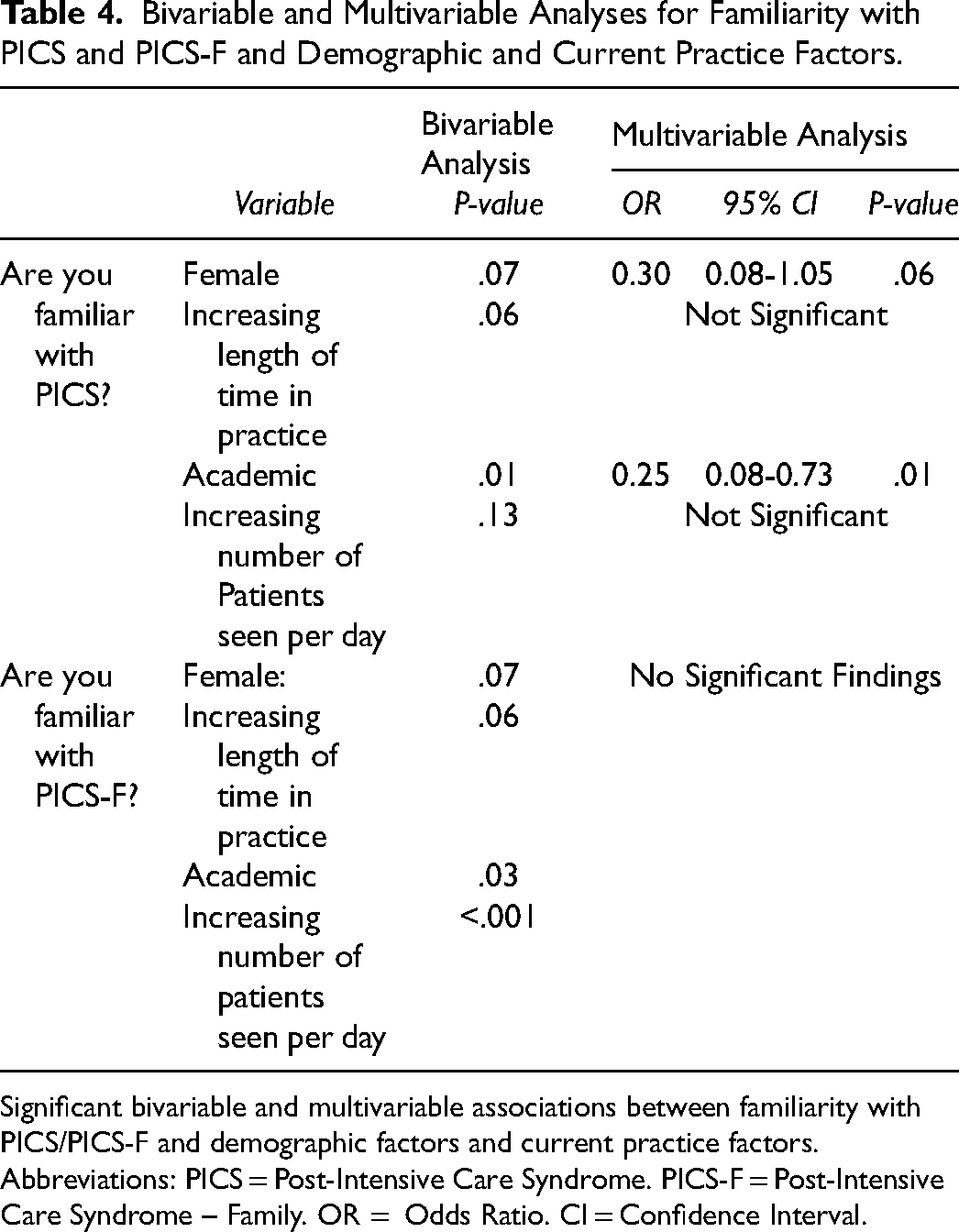
Significant bivariable and multivariable associations between familiarity with PICS/PICS-F and demographic factors and current practice factors. Abbreviations: PICS = Post-Intensive Care Syndrome. PICS-F = Post-Intensive Care Syndrome – Family. OR = Odds Ratio. CI = Confidence Interval.
Discussion
To our knowledge, this is the first study to describe primary care physician practice in regards to care following critical illness and knowledge of common complications following critical illness. We found that the majority of respondents reported feeling comfortable caring for patients after a critical illness and also felt that they were aware of common problems encountered after critical illness. However, they reported a low exposure to these patients. Similarly, only a minority described a systematic approach to evaluating post-critically ill patients. Barriers to care were present, and each domain (time during appointment, availability of an up-to-date list of medications, access to the discharge summary, list of pending test results, list of further care recommendations) assessed represents a possible opportunity to improve patient care. Finally, primary care physicians acknowledge that they have had less focused education in regards to ICU survivorship, and were highly receptive to it. About half thought a specialized transitional clinic would be helpful. Taken together, these data demonstrate that there is significant opportunity to improve the care of post-critically ill patients.
This study demonstrates that future care models should incorporate a multifaceted approach to improve the care of survivors after critical illness. First, we as critical care clinicians, need to better educate patients about recovery after critical illness including PICS and PICS-F. Various methods to do this include discussion with patients/families by the ICU team 30 and the hospitalist team, patient handouts and informational brochures,31,32 accurate media coverage,33,34 and reputable websites and videos to which we can refer patients/families.35–38 We also need to better understand what our patients take away from conversations when we, as critical care providers, do discuss issues about care and recovery after the ICU with them. We also need to learn when and how it is best to discuss issues around recovery with patients and their families. Work in similar areas has shown that physicians and patients/families may have discordant perceptions of the same discussion, which may be important to further study in regards to discussions with patients and families about PICS and PICS-F, and recovery after critical illness.39–41
Second, practitioners need to be equipped with tools to help them care for these complex patients. Education of all care providers including hospitalists, critical care providers, and primary care providers is essential.42–44 Additionally, communication between hospital-based care providers and primary care practitioners needs to be improved, as noted by our respondents and in other studies.45,46 This may include direct communication (phone calls, messages via email or through an electronic medical record) with the PCP at ICU admission and discharge. In addition, discharge summaries could be improved with a more complete description of life-support interventions needed and duration of them, reasons for treatment and code status decisions, complications of treatments, and discharge gaps.47,48 A list of common problems encountered after critical illness may be beneficial as well. 6 Further understanding of the needs of primary care physicians in regards to knowledge gaps and opportunities in the area of ICU survivorship, in the setting of their time constraints and competing interests will be needed too. Additionally, support from the hospital, health system or insurance may be complementary to care provided by primary care providers, but this is not yet clear.49,50
Finally, post-ICU clinics may have a significant role in the care of post-critically ill patients.29,51,52 Post-ICU clinics have become increasingly present, especially since the start of the coronavirus pandemic, but are still not common.26,53 These clinics allow critical care physicians to learn about post-critically patients and their recovery process; they also allow critical care practitioners to reevaluate processes and quality improvement initiatives in the ICU. 54 They may provide an opportunity for positive (and negative) feedback about particular patients to be given to the entire ICU team. Post-ICU clinics may have higher volumes of post-critically ill patients compared to individual PCPs, and so may be better suited for advancing the field of ICU survivorship. 26 Finally, post-ICU clinics may also be cost-saving; 55 other studies are examining the role for telehealth management of these patients (NCT03926533, NCT04576065, NCT03671447). Future work to overcome common barriers (including implementation and attendance) to post-ICU clinics is needed as well. 56
Strengths of this study include the rigor of the survey methodology, including the random distribution of the survey to North Carolina primary care physicians, and the novelty of the study. Limitations of our study include our sample size and response rate. Notably though, our response rate of 39% is in line with other surveys of physicians (where effective response rates are often reported to be 33%-52%).57–60 Additionally, the demographics of our respondents were similar to that of all primary care physicians across the state of North Carolina. Sixty-six percent of our respondents were male, with a median age of 53, and 64% were family physicians; this is in line with published data showing primary care physicians in NC overall are 63% male, with a median age of 50, and 58% are family physicians. 61 Another limitation was the fact that we did not survey Advanced Practice Providers (Nurse Practitioners and Physician Assistants), who also provide primary care to patients. We were also limited in our ability to further evaluate associations between respondent demographics and current practices with familiarity with PICS and PICS-F, a desire for more education, interest in a list of common problems encountered in the post-critical illness population, and interest in a specialized transitional clinic due to sample size. Finally, we asked clinicians to generalize their practices toward a heterogeneous population, which may be a difficult task. It is also important to note that our study was completed prior to the current coronavirus pandemic; it is possible that more primary care physicians are now more aware of PICS/PICS-F given the well-recognized concerns about the post-acute sequelae of COVID-19.
Conclusions
In sum, significant gaps and barriers exist to providing optimal post-ICU care. Post-ICU clinics are one way to improve care for these post-critically ill patients, but the reach of critical illness survivorship care must also include PCPs, patients, and their families. PCPs can be better equipped to care for survivors of critical illness through better communication with in-hospital physicians, education regarding common issues seen post-critical illness, provision of sufficient time to see these complex patients, and tools to assess patients systematically. Similarly, patients and families must be routinely educated about PICS/PICS-F. Through better collaboration, education, and engagement, care of post-ICU patients can be improved.
Footnotes
Acknowledgements
The authors would like to thank all the survey respondents for their participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RNB was supported in part by a grant from the Wake Forest Claude D. Pepper Older Americans Independence Center (P30-AG21332) and the Wake Forest University School of Medicine, Department of Internal Medicine. The authors gratefully acknowledge use of the services and facilities of the Wake Forest CTSI, funded by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR001420.