
Abstract
Introduction
The COVID-19 disease spread rapidly to all other countries after being detected in China in 2019, and the World Health Organization declared COVID-19 pandemics.1,2 Although it was initially thought that this disease was no different from other diseases such as SARS and influenza in terms of mortality, hospitalization, and death, 3 with increasing evidence and over time, it was shown that in addition to various health, economic and social consequences it also has many psychological effects on human societies.4,5 As of July 22, 2022, this pandemic has affected about 551 million people and killed 6.5 million people worldwide. 6 In Iran, until Jun 22, 2022, six waves of epidemics have been repeated. About 7.5 million cases of COVID-19 disease have been tested positive for PCR, and with 141 300 deaths reported, the death rate from the disease is 1.88 per 100 000 general population. 7 These numbers can vary depending on the disease's underestimation and lack of testing. Based on the estimated excess death related to COVID-19, the actual death will be twice as many as reported in Iran. 8
Although interventions such as vaccination have been able to reduce the incidence of death and COVID-19 worldwide, the long-term problems with COVID have added to the concerns of human societies.9,10 Evidence suggests that COVID-19 has long-term consequences for the heart, brain, and other organs. 11 Globally, about 53.2 million major depressive disorder cases have been reported due to the COVID-19 pandemic, and the pooled prevalence is 3152.9 cases per 100 000 population. As a result, the side effects of COVID-19 can be serious and manifest themselves in the long run. 12 The risk of cardiovascular disorders in people with COVID-19 is significantly higher than in those without the disease. 13 It is estimated that the countries will face many challenges with long-COVID in the next years. As a result, it is possible to reduce the long-term and short-term effects of COVID-19 infection by performing evidence-based interventions, identifying the relevant, effective factors, and finally preventing infection, death, and hospitalization. 14
From the beginning of the COVID-19 pandemic, countries have adopted different policies and interventions to reduce the burden of COVID-19 in terms of death, hospitalization, and even social, psychological, and economic effects. 15 Some countries, such as China, have followed the zero- COVID-19 approach, 16 while others have imposed restrictions, mass vaccinations, contact tracing, and other non-pharmacological interventions. 17 Although social and public interventions in countries reduce the adverse effects of COVID-19, recognizing the risk factors associated with COVID-19 severity and death in communities can help the health system identify high-risk groups and implement appropriate risk-reduction interventions.18,19 In Iran, several social and non-pharmacological interventions have been performed to reduce the COVID-19 adverse effects, but recognizing the factors associated with the incidence of death and severity can provide comprehensive information on high-risk and low-risk groups. To our knowledge, separate studies have shown the relationship between some factors, but systematically, related risk factors have not been studied. Current meta-analysis studies have also been conducted with limited articles in the past, and the findings of newer meta-analyses can help to show better the clinical, epidemiological, and diagnostic aspects of this disease. This study aims to investigate the risk factors associated with severity and death from COVID-19 through a systematic review and meta-analysis of the published documents in Iran.
Materials and Methods
Setting
This study is in line with the recommendations outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 20 We have investigated the risk factors associated with severity and death from COVID-19 in Iran from the beginning of the COVID-19 epidemic to March 20, 2022.
Search Strategy
A systematic searching was performed based on all articles indexed in Scopus, Embase, Web of Science (WOS), PubMed, and Google Scholar in English and Scientific Information Database (SID) and IRANDOC indexes using the keywords “(“Iran”[Mesh Terms] OR “Iran”[All Fields]) AND (“COVID-19”[Title/Abstract] OR “Corona”[Title/Abstract] OR “2019 novel coronavirus”[Title/Abstract] OR “severe acute respiratory syndrome coronavirus 2”[Title/Abstract] OR “corona virus disease 2019”[Title/Abstract] OR “SARS-COV-2”[Title/Abstract] OR “Coronavirus”[Title/Abstract]) OR “COVID”[Mesh]) AND (“infection”[Title/Abstract] OR “incidence”[Title/Abstract] OR “morbidity”[Title/Abstract] OR “sick*”[Title/Abstract] OR “death”[Title/Abstract] OR “mortality”[Title/Abstract] OR “fatal*”[Title/Abstract] OR “severity”[Title/Abstract] OR “ICU”[Title/Abstract] OR “hospital*”[Title/Abstract] OR “Dying”[Title/Abstract] OR “intensit*”[Title/Abstract]) AND (“related factor*”[All Fields] OR “factor associated”[All Fields] OR “associated factor”[All Fields] OR “risk factor”[All Fields] OR “factor*”[All Fields] OR “factor related”"[All Fields]).”
Inclusion Criteria
All studies were included by identifying observational studies conducted in Iran. Other review studies, case studies, and laboratory studies that did not meet the inclusion criteria were excluded. Two researchers evaluated the search results independently. We also did snowballing with searching the references of the included articles to explode our search strategy. Based on COVID-19 Treatment Guidelines Panel and Coronavirus Disease 2019 (COVID-19) Treatment Guidelines, 21 severity disease due to COVID-19 mentioned in studies was defined: “Individuals who have SpO2 < 94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) < 300 mm Hg, a respiratory rate >30 breaths/min, or lung infiltrates >50% and Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.” Disease severity in our study was defined as a form of the disease that requires hospitalization, oxygen therapy, and/or mechanical ventilation in ICU or Hospital. 22 Cardiovascular diseases were defined to any cardiovascular disorder related to the heart and blood vessels. 23 Cerebrovascular disease was included all disorders in which an area of the brain is temporarily or permanently affected by ischemia or hemorrhage, and one or more blood vessels of the brain are involved in the pathological process. 24 chronic liver disease was determined” Chronic liver disease (CLD) is a progressive deterioration of liver functions for more than six months, which includes synthesis of clotting factors, other proteins, detoxification of harmful products of metabolism, and excretion of bile.” 25 ARDS also was defined “as syndrome of inflammation and increased permeability” leading to acute onset of bilateral infiltrates on chest radiograph with PaO2/FiO2 ≤ 200 that cannot be explained by left heart dysfunction.” 26 Any study that introduced these conditions as inclusion criteria were included.
Selection Process
Two independent researchers initially screened the search strategy results based on abstracts and titles. Then the full texts of related articles were evaluated based on inclusion and exclusion criteria. A third researcher reviewed studies in which individuals did not reach a decision. Finally, observational studies that reported death and severity-related factors related to COVID-19 were included in the meta-analysis.
Data Collection Process
Two researchers also independently extracted the required data from the studies. The third researcher reviewed the list of articles and extracted the data to ensure that there were no duplicate articles and resolved disputes over the study's inclusion.
Assessment of Methodological Quality, Risk of Bias, and Publication Bias
We used the Newcastle Ottawa Scale for cohort, evidence-based, and cross-sectional studies to assess quality. According to these checklists, studies can be divided into three groups (good, acceptable, and poor quality). 27
Statistical Approach
The “metan” command performed a random-effects meta-analysis in STATA. Forest plots were used for a graphical description of the results. We used HRs and ORs reported for the association between risk factors and COVID-19 severity and death to calculate ln HRs, ln ORs, and their standard errors (SE). Finally, publication bias was assessed by the Egger test. The data were analyzed using Stata version 11.0. Pooled estimates in meta-analyses were estimated with a 95% confidence interval. P-values were considered significant at the level of < .05.
Results
Search Results and Quality Assessment
After deleting duplicates, we identified 2463 studies from four databases and then screened articles by title and full text according to the study's objectives. Finally, 69 studies were included in the meta-analysis (Figure 1), of which 62 studies had assessed risk factors for death from COVID28–89); 13 studies determined risk factors for severity ((41,50,53–55,65,90–96), out of which six studies reported both outcomes ((35, 44, 47–49, 59)). Out of 69 studies, 33 were cohort studies, eight were case-control studies, and 28 were cross-sectional studies. The mean sample size was 2742 (Range: 35–40 957) (Table 1).
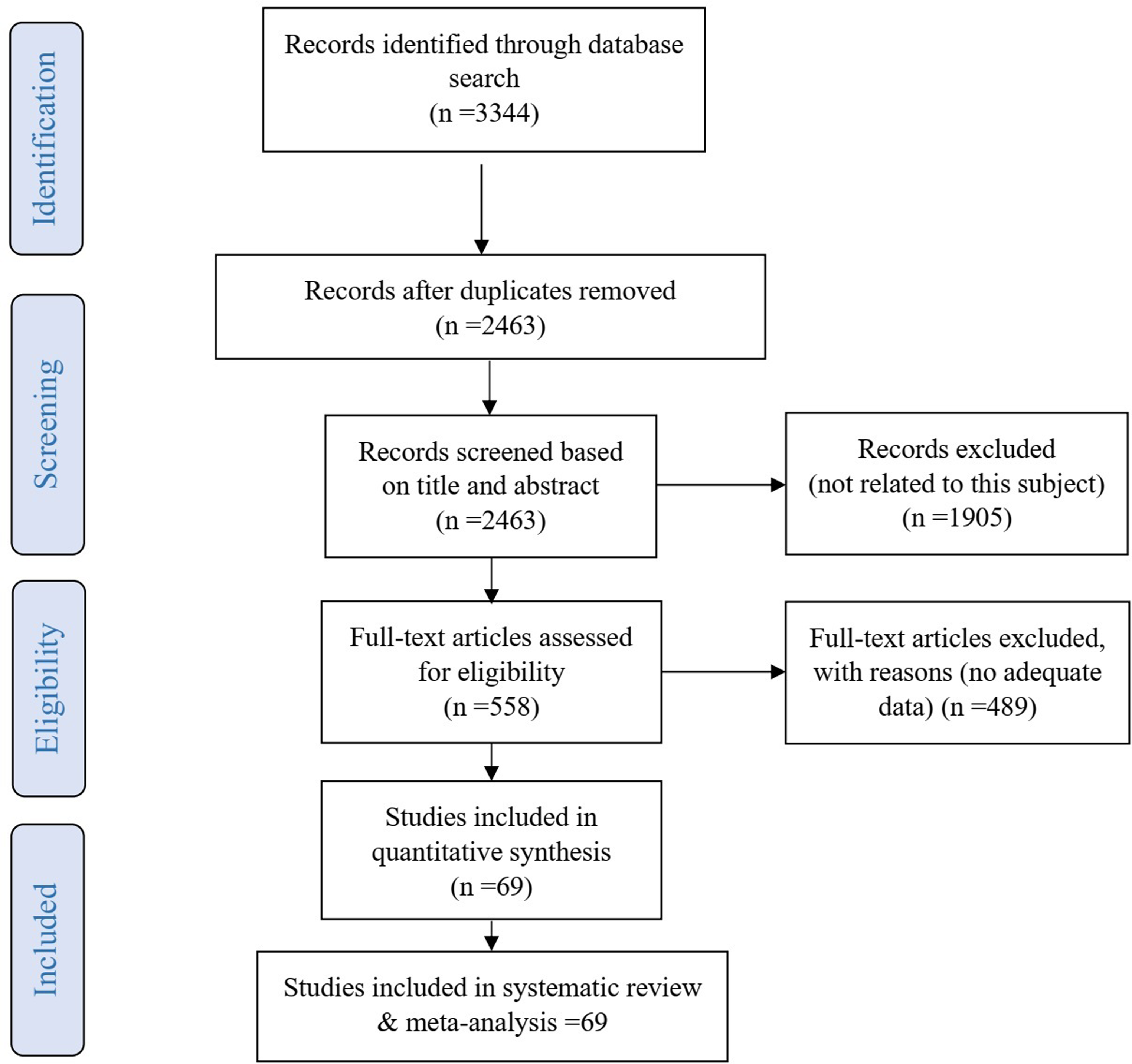
Flow diagram of the study selection process.
Characteristics of Included Studies and Quality of Assessment.
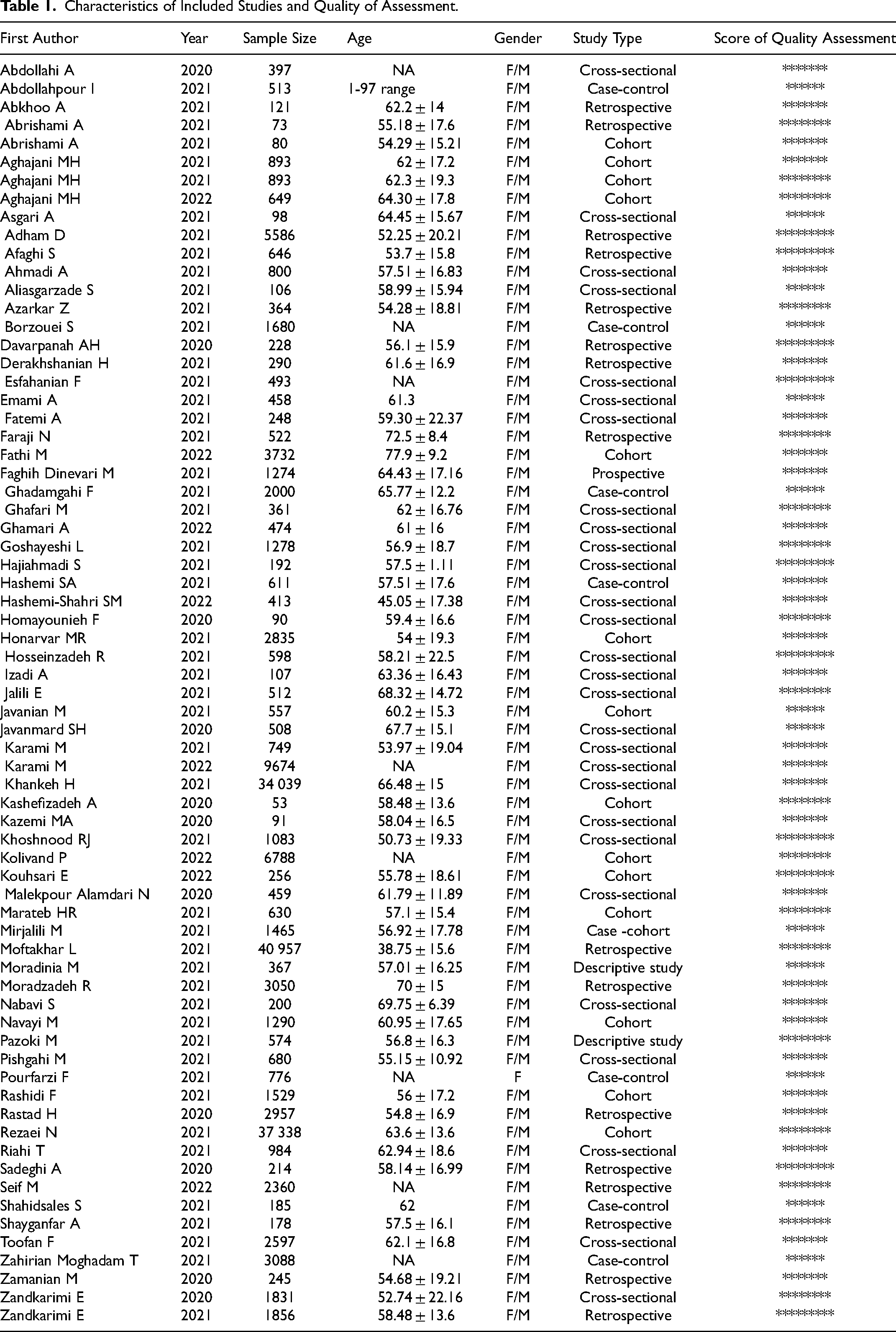
When we assess the quality of included studies, the Newcastle Ottawa scale showed that 10 studies (14.49%) scored 9, 18 studies (26.09%) scored 8, and 27 studies (39.13%) scored 7, and 14 studies (20.29%) scored six points. Therefore, all studies scored above five and had high quality (Table 1).
Demographic Characteristics and Risk of Death from COVID-19
In a meta-analysis, 35 studies examined the effect of age on Death from COVID-19, and 35 effect sizes were obtained. The meta-analysis results showed a significant association between older age and Death from COVID-19, and the pooled OR and HR were 1.04 (95% CI = 1.03 to 1.06) and 1.03 (95% CI = 1.02 to 1.04) for each one-year increase in age respectively. Twenty-seven studies assessed the risk of Death from COVID-19 for gender and showed that the male gender significantly affects death, and the pooled OR was 1.21 (95% CI =1.05 to 1.38) (Table 2 and Figure 2).
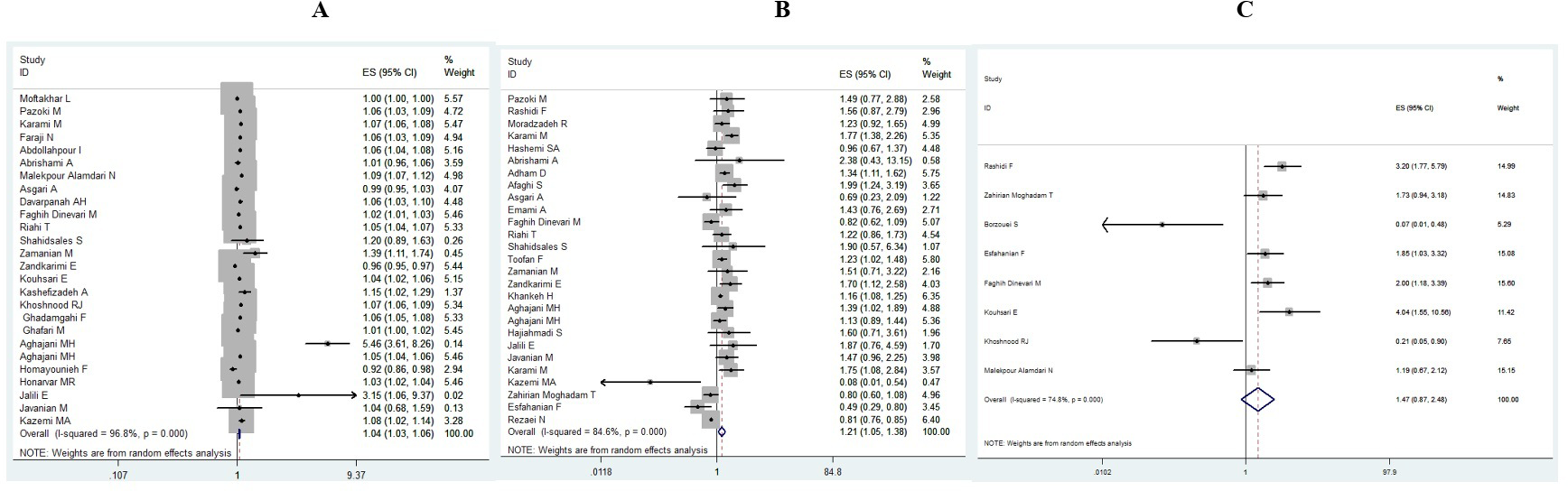
Meta-analysis to assess the risk of death for (A) age (B) sex, male. (C) Smoking.
Association of Demographic, Clinical Characteristics and Laboratory Parameters with Death in Patients with COVID-19.
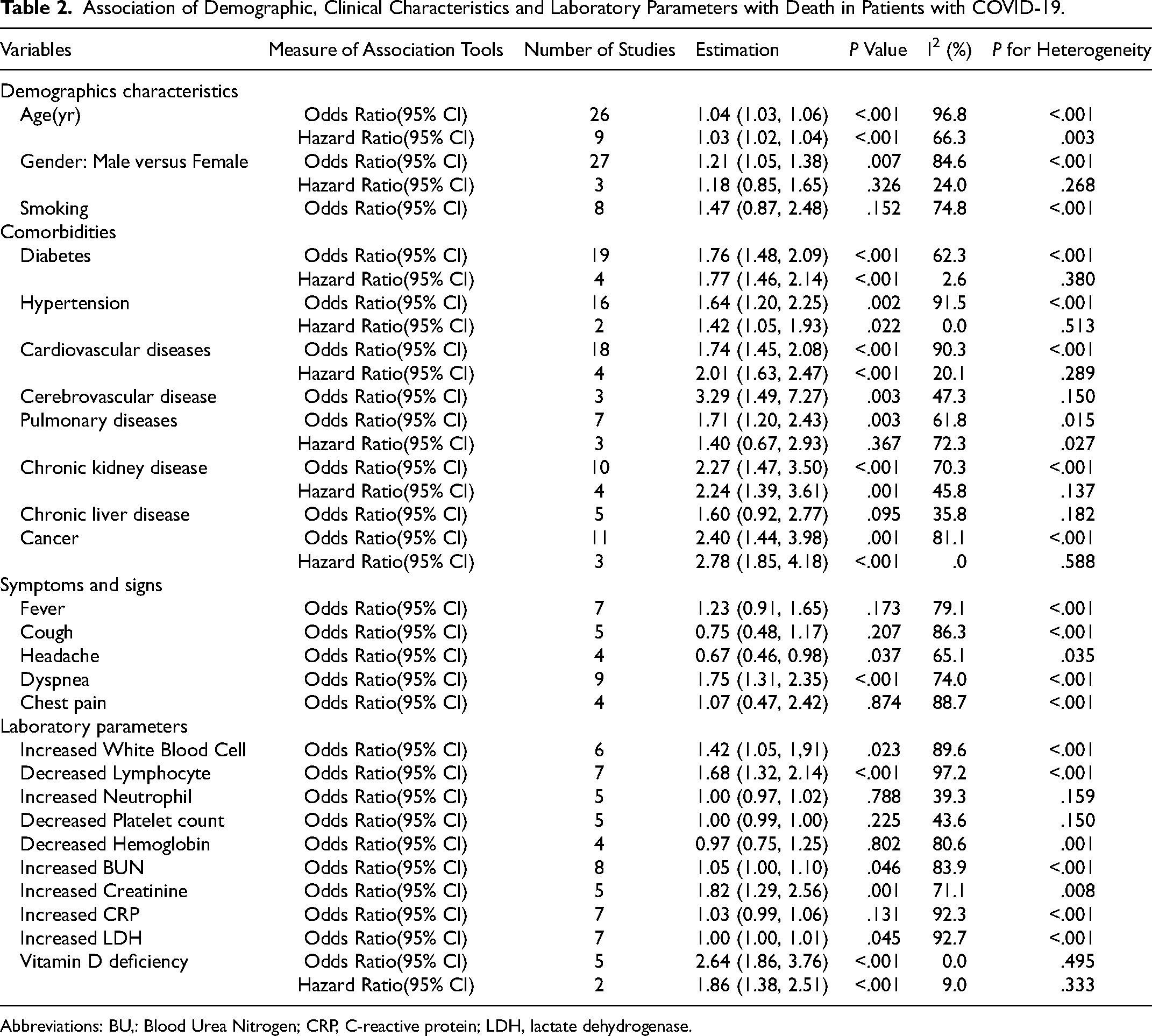
Abbreviations: BU,: Blood Urea Nitrogen; CRP, C-reactive protein; LDH, lactate dehydrogenase.
Comorbidities and Risk of Death from COVID-19
Twenty-three studies evaluated the association between diabetes and Death from COVID-19 and showed a significant association between diabetes and coronaviruses mortality (pOR = 1.76; 95%CI = 1.48 to 2.09; pHR = 1.77; 95%CI = 1.46 to 2.14). In addition, we found a significant positive association between hypertension (pOR = 1.64; 95% CI = 1.20, 2.25; pHR = 1.42; 95% CI 1.05 to 1.93), cardiovascular disease (CVD) (pOR = 1.74; 95% CI = 1.45 to 2.08; pHR = 2.01; 95% CI = 1.63 to 2.47), cerebrovascular disease (pOR = 3.29; 95% CI = 1.49 to 7.27), pulmonary diseases (pOR = 1.71; 95% CI = 1.20 to 2.43), chronic kidney disease (CKD) (pOR = 2.27; 95% CI = 1.47 to 3.50; pHR = 2.24; 95% CI = 1.39 to 3.61), cancer (pOR = 2.40; 95% CI = 1.44 to 3.98; pHR = 2.78; 95% CI = 1.85 to 4.18), and Death from COVID-19 (Table 2 and Figure 3).
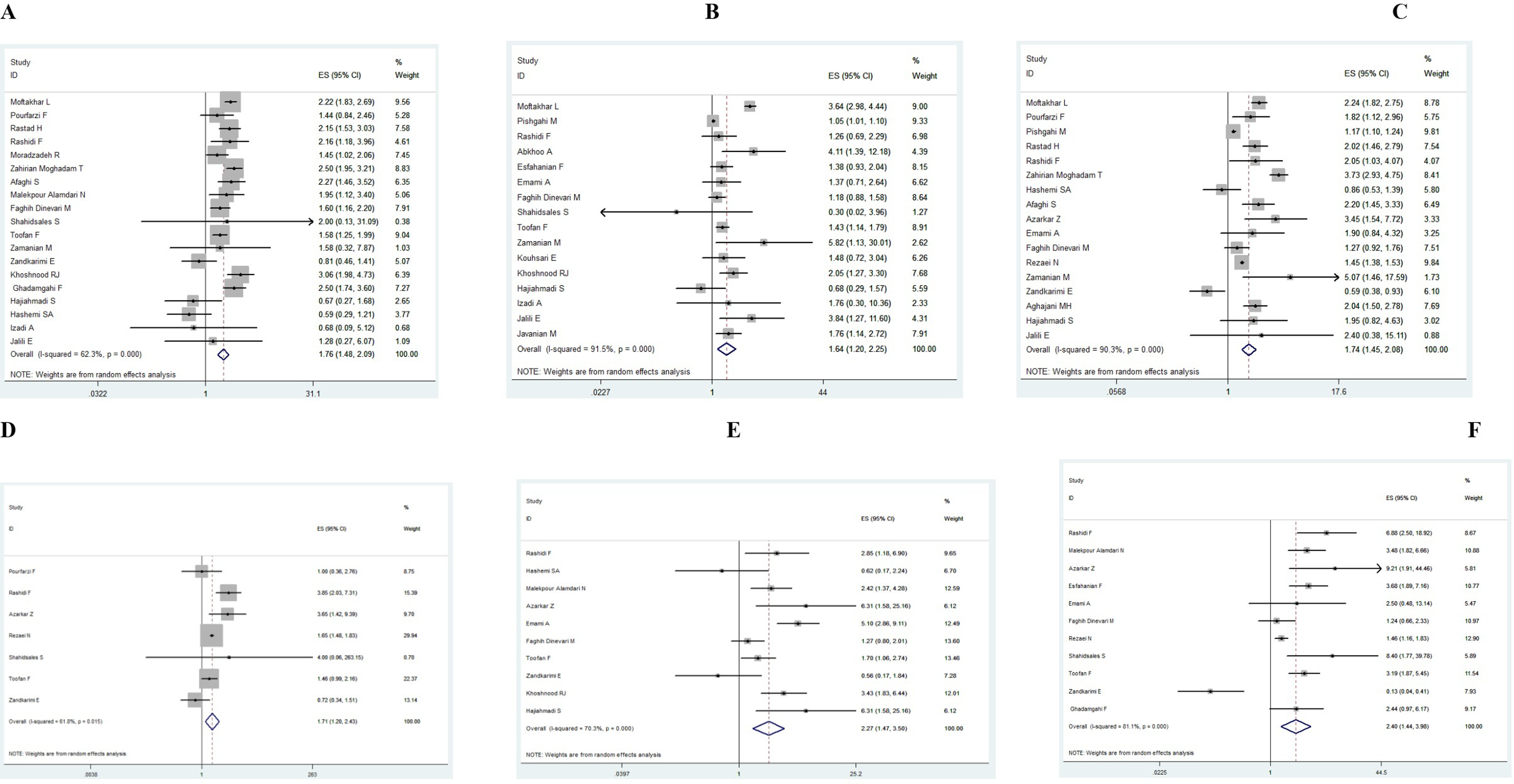
Meta-analysis to assess the risk of mortality for (A) diabetes (B) hypertension. (C) Cardiovascular disease. (E) Chronic kidney disease. (F) Cancer.
Symptoms and Risk of Death from COVID-19
Death from COVID-19 risk was significantly associated with a negative direction with Headache (pOR = 0.67; 95%CI = 0.46 to 0.98). In addition, the combined nine effect sizes from 9 studies showed a significant association between Dyspnea and Death from COVID-19 (pOR = 1.75; 95%CI = 1.31 to 2.35) (Table 2).
Laboratory Parameters and Risk of Death from COVID-19
Six studies have investigated the effect of the increased WBC on Death from COVID-19. The results showed a significant association between increased WBC and coronaviruses mortality (pOR = 1.42; 95%CI = 1.05 to 1.91). In addition, we found a significant association between decreased Lymphocyte (pOR = 1.68; 95% CI 1.32, 2.14), increased blood urea nitrogen (BUN) (pOR = 1.05; 95% CI 1.00 to 1.10), increased creatinine (pOR = 1.82; 95% CI 1.29 to 2.56), vitamin D deficiency (pOR = 2.64; 95% CI = 1.86 to 3.76; pHR = 1.86; 95% CI = 1.38 to 2.51), and Death from COVID-19 (Table 2).
Disease Severity-Related Risk Factors
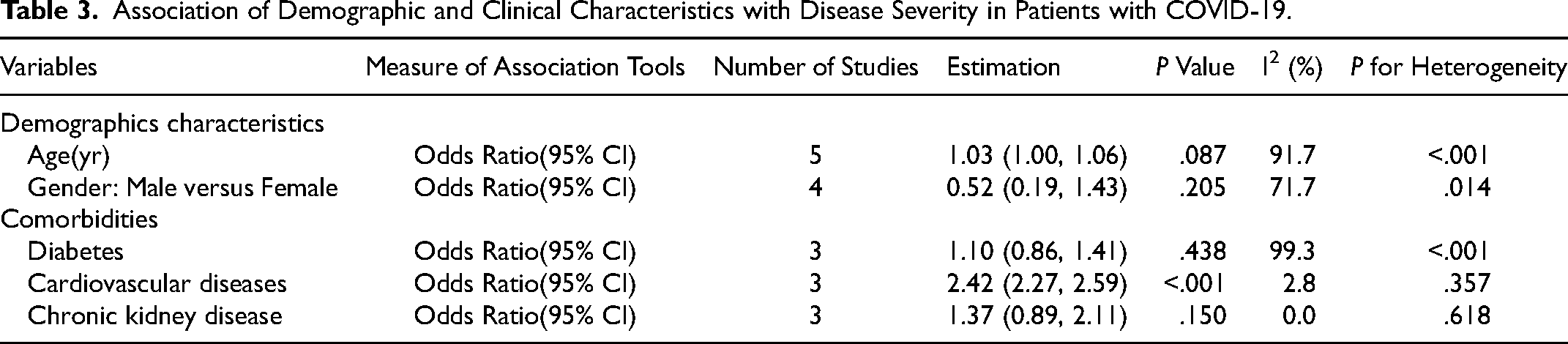
In a meta-analysis of 18 effect sizes, demographic and clinical features were obtained from 13 studies. The results of the meta-analysis showed that there was only a significant relationship between CVD and disease severity (pOR = 2.42; 95% CI = 2.27 to 2.59) (Table 3).
Association of Demographic and Clinical Characteristics with Disease Severity in Patients with COVID-19.
Publication Bias
Based on the results of the Egger's test (age: P = .087, gender: P = .070, smoking: P = .216, diabetes: P = .221, hypertension: P = .589, CVD: P = .284, CVA: P = .602, pulmonary diseases: P = .881, CKD: P = .210, chronic liver disease: P = .624, cancer: P = .938, fever: P = .230, cough: P = .327, dyspnea: P = .667, chest pain: P = .174, headache: P = 1.000, WBC: P = .142, lymphocyte: P = .573, neutrophil: P = .624, platelet: P = .055, HB: P = .498, BUN: P = .621, creatinine: P = 1.000, CRP: P = .573, LDH: P = .176, vitamin D: P = .142), there was no evidence of publication bias among articles assessing risk factors for Death from COVID-19. In addition, there was no evidence of publication bias among articles assessing disease severity risk factors (age: P = .624, gender: P = .065, diabetes: P = .117, CVD: P = .602, CKD: P = .602).
Meta-Regression Analysis
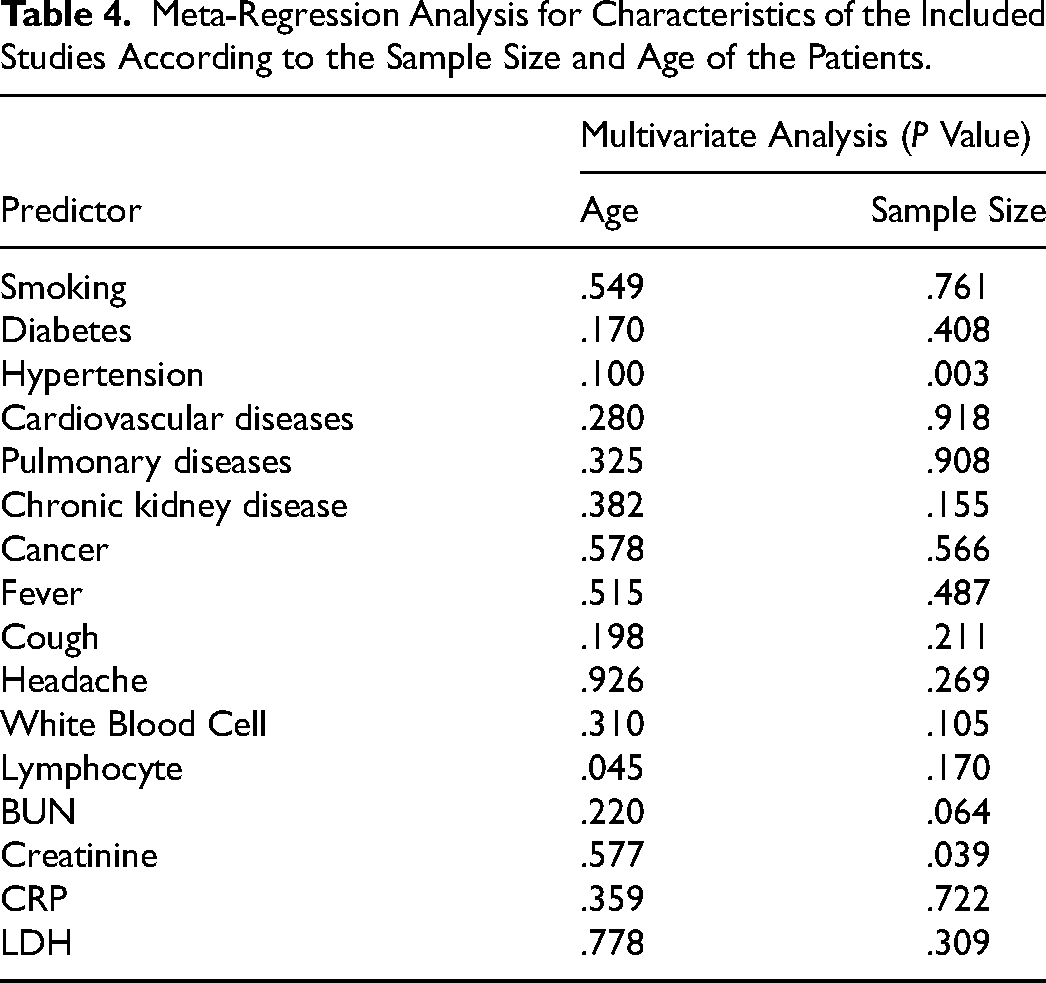
Meta-regression showed that the sample size is an important source of heterogeneity when examining the potential predictive effect of hypertension (Original I2 = 91.5, I2 residual = 64.8, P = .002) and creatinine (Original I2 = 71.7, I2 residual = 0.0, P = .039). Also, the mean age of patients is an important source of heterogeneity when examining the potential predictive effect of lymphocyte (Original I2 = 97.2, I2 residual = 77.7, P = .045) (Table 4).
Meta-Regression Analysis for Characteristics of the Included Studies According to the Sample Size and Age of the Patients.
Discussion
This study aimed to assess risk factors associated with COVID-19 severity and death in Iran. Based on this meta-analysis study, some factors related to the dimensions of the COVID-19 disease have been mentioned in the studies conducted in Iran.
Our study showed a significant association between diabetes and hypertension with death from COVID-19. Some studies similar to our results showed that diabetes and hypertension are important factors in COVID-19 mortality. A systematic review showed that diabetic ketoacidosis (DKA) in COVID-19 patients portends a poor prognosis with a mortality rate approaching 50%. Differentiating isolated DKA from combined DKA/HHS (hyperglycemic hyperosmolar syndrome) is essential as the latter represents nearly one-fifth of the DKA cases and tends to have higher mortality than DKA alone. 97 Another study suggests that diabetes and hypertension were associated with higher COVID-19 mortality, contributing to nearly 30% of death from COVID-19 s. 98 A meta-analysis study showed that COVID-19 severity and death were associated with Diabetes Mellitus, ARDS, and disease progression in patients with COVID-19. The association was weaker in the older and hypertensive patients. 99 According to the latest national study, it has been shown that diabetes, cardiovascular disease, CKD, and hypertension, as diseases with significant prevalence, have a great impact on increasing the burden of diseases in Iran. 100 It seems that one of the reasons for the high mortality rate due to COVID-19 in Iran, in some periods, has been related to the high incidence of COVID-19 in populations with chronic disease and the elderly population. In line with the findings of our study, Mirjalili et al. 101 showed that diabetes, hypertension, CKD, and cardiovascular disease in people with COVID-19 increased mortality and severity by about 55%. Other studies also showed that these diseases positively affect Death from COVID-19.102–104 Although the World Health Organization has emphasized that the elderly and people with chronic diseases are at risk of death from COVID-19, 105 the importance of this problem is not addressed in the management strategies of this epidemic. The present study showed a significant association between older age and Death from COVID-19, similar to some research done in Iran.106,107 In addition, the Iranian elderly mostly have chronic diseases such as diabetes, cardiovascular and hypertension, which were immunized in the first step of nationwide vaccination; the clinical and treatment interventions performed were uniform for all populations, and more specialized services for the elderly and underlying patients could prevent death. Previous studies showed that elderly people usually experience a decrease in their immune system ability,108,109 and the coexistence of aging and chronic diseases can play a vital role in increasing the death from COVID-19. 110 In the clinical management of elderly patients, medical staff should consider the higher mortality risk and make more critical decisions in this age group to prevent more deaths. Our results showed that men have higher mortality due to COVID-19 than women, and other similar studies have also demonstrated this relationship.111–113 It can be said that the X chromosome in women seems to reduce susceptibility to infection, and sex hormones play a role in innate and adaptive immunity. 114 Besides, men maybe are at a greater risk of getting COVID-19 infection due to being more active in society, working in places with others, and not paying more attention to self-care than women, which ultimately leads to an increase in mortality.
Regarding symptoms, the present study showed that headache has an inverse relationship with death from COVID-19. Previous studies have also investigated this issue. In line with this study, other studies also showed a better prognosis for patients with headaches.115–117 Some studies have shown that having a headache is associated with decreased inflammatory biomarkers, such as C-reactive protein (CRP) and lower and more stable levels of interleukin-6 (IL-6) during hospitalization.118,119 A study investigating headache phenotypes related to covid-19 showed that tension headaches are related to decreased levels of CRP and procalcitonin. 120 However, there is still no clear epidemiological and clinical knowledge about the relationship between headache and higher death from COVID-19, and more studies can help find this relationship in patients with different clinical, laboratory, and diagnostic characteristics. Various studies have seen dyspnea as a symptom associated with higher death from COVID-19.121,122 These findings were also observed in our study. A systematic review study has shown that considering the dyspnea symptom is even more important than fever in terms of diagnosis and prognosis, 123 and identifying this symptom can be important before making clinical decisions.
Blood markers in COVID-19 patients can be important in clinical and treatment planning. Some studies consider the status of such markers for diagnostic evaluation, survival, and prognosis of patients.124,125 We observed a significant association between increased WBC, decreased lymphocyte, increased BUN, increased creatinine, vitamin D deficiency, and death from COVID-19. In line with our results, Henry et al. 126 showed in their meta-analysis study that WBC as an increasing marker in patients with the acute condition of COVID-19 could be considered a good marker for predicting their prognosis. Lan et al. 127 also showed that people with a shorter survival from COVID-19 infection had a decrease in lymphocytes, and the odds of mortality in patients with low blood lymphocytes were nine times higher than in those with high lymphocytes. Similar studies also showed a relationship between death from COVID-19 and vitamin D deficiency.128–130 In countries such as Iran, which are facing the limitation of testing for the diagnosis of COVID-19 and the patients ignore their disease, blood markers can be an important indicator to consider the patients’ clinical profile to educate and adhere to the treatment.
Regarding the limitations of this study, some factors could not be included in the final analysis due to the lack of sufficient studies to measure its effects, and increasing the number of similar studies in the future may change the results of related meta-analyses. The lack of sufficient access to national data in Iran to conduct more valid epidemiological studies is one of the limitations of all studies. However, for the first time, this study has simultaneously shown the effects of some factors related to the severity and death-related COVID-19 in Iran. There is a heterogeneity among studies included the meta-analysis in terms of the place (ICU, wards or emergency rooms) where the studies were conducted. It may influence the results of laboratory parameters, as the clinical condition of ICU patients is more severe than patients in wards.
Conclusion
Our study showed some factors related to severity and death associated with COVID-19 in Iran. Clinical decisions are usually chosen by knowing the factors affecting prognosis, severity, and death. Since this study showed the effect of some blood markers, co-morbidities, headache and dyspnea, aging, and male gender, the diagnostic value of these factors can be used for medical teams and therapeutic and clinical decisions.
Footnotes
Author Contributions
Conceptualization: KA, SSHN. Search strategy searching: AM, NT. Formal analysis: SSG, SSHN. Methodology: AM, KE, SSHN. Project administration: SSHN, AM. Visualization: NI, FS, YM. Writing–original draft: AS, SF, RF. Searching team: ER, SSG, KFB, ZB, AM.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethics Statement
The Ethical Committee of Shahid Beheshti University of Medical Sciences approved this study with ID: IR.BMSU.REC.1399.095.