
Abstract
Introduction
High-dose catecholamines can impair hypoxic pulmonary vasoconstriction and increase shunt fraction. We aimed to determine if Angiotensin II (Ang-2) is associated with improved PaO2/FiO2 and SpO2/FiO2 in patients in shock.
Methods
Adult patients at four tertiary care centers and one community hospital in the United States who received Ang-2 from July 2018-September 2020 were included in this retrospective, observational cohort study. PaO2, SpO2, and FiO2 were measured at 13 timepoints during the 48-h before and after Ang-2 initiation. Piecewise linear mixed models of PaO2/FiO2 and SpO2/FiO2 were created to evaluate hourly changes in oxygenation after Ang-2 initiation. The difference in the proportion of patients with PaO2/FiO2 ≤ 300 mm Hg at the time of Ang-2 initiation and 48 h after was also examined.
Results
The study included 254 patients. In the 48 h prior to Ang-2 initiation, oxygenation was significantly declining (hourly PaO2/FiO2 change −4.7 mm Hg/hr, 95% CI − 6.0 to −3.5, p < .001; hourly SpO2/FiO2 change −3.1/hr, 95% CI−3.7 to −2.4, p < .001). Ang-2 treatment was associated with significant improvements in PaO2/FiO2 and SpO2/FiO2 in the 48-h after initiation (hourly PaO2/FiO2 change +1.5 mm Hg/hr, 95% CI 0.5-2.5, p = .003; hourly SpO2/FiO2 change +0.9/hr, 95% CI 0.5-1.2, p < .001). The difference in the hourly change in oxygenation before and after Ang-2 initiation was also significant (pinteraction < 0.001 for both PaO2/FiO2 and SpO2/FiO2). This improvement was associated with significantly fewer patients having a PaO2/FiO2 ≤ 300 mm Hg at 48 h compared to baseline (mean difference −14.9%, 95% CI −25.3% to −4.6%, p = .011). Subgroup analysis found that patients with either a baseline PaO2/FiO2 ≤ 300 mm Hg or a norepinephrine-equivalent dose requirement >0.2 µg/kg/min had the greatest associations with oxygenation improvement.
Conclusions
Ang-2 is associated with improved PaO2/FiO2 and SpO2/FiO2. The mechanisms for this improvement are not entirely clear but may be due to catecholamine-sparing effect or may also be related to improved ventilation-perfusion matching, intrapulmonary shunt, or oxygen delivery.
Keywords
Introduction
The treatment of shock relies on vasopressors when non-pharmacologic interventions are unable to maintain adequate mean arterial pressure (MAP). 1 Distributive shock is the most common type of shock, accounting for nearly two-thirds of all cases in the intensive care unit (ICU). 2 In distributive shock, norepinephrine is often utilized as the first-line agent, followed by either vasopressin or epinephrine when other interventions are unsuccessful in maintaining an adequate MAP. 3 Their mechanism for vasoconstriction is through binding of α1 receptors (norepinephrine and epinephrine) or V1a receptors (vasopressin) on vascular smooth muscle. 4 Although exogenous catecholamines and vasopressin are often able to increase blood pressure, their use is associated with mesenteric ischemia, necrosis, and cardiac arrhythmias at high doses.5–7 Moreover, their use may be associated with worse oxygenation by altering lung perfusion, which leads to intrapulmonary shunt and ventilation/perfusion (V/Q) mismatch.8–12 Even elevated endogenous catecholamines, as in the case of central nervous system injury and pheochromocytoma, have been associated with adverse events such as pulmonary edema, impaired gas exchange, and cardiomyopathy.10,12,13
Angiotensin II (Ang-2) is a non-catecholamine vasopressor that exerts its vasoconstrictive properties through agonism of angiotensin type I (AT1) receptors. 4 In the Angiotensin II for the Treatment of High-Output Shock 3 (ATHOS-3) trial, Ang-2 was shown to increase MAP more frequently (69.9% Ang-2 vs 23.4% control, p < .001), while decreasing background norepinephrine-equivalent dose (NED). 14 Several other studies have found similar hemodynamic benefits and NED reduction when Ang-2 is utilized to treat shock.15–17
Data from small studies suggest that Ang-2 may also be associated with improved oxygenation.18,19 One study of 16 patients infected with the novel coronavirus 2019 (COVID-19) in Italy examined the association of Ang-2 with the partial pressure of oxygen (PaO2), fraction of inspired oxygen (FiO2), peripheral capillary oxygen saturation (SpO2), and positive end-expiratory pressure (PEEP). 18 Patients treated with Ang-2 had significant improvements in PEEP, FiO2, and SpO2/FiO2. 18 Another study of 29 COVID-19 patients in New York found that Ang-2 was associated with an improvement in hypercapnia and reduction of PEEP when compared to controls. 19 Despite these associations with improved gas exchange, neither study was able to find improvements in the PaO2/FiO2 ratio, possibly because of the relatively small sample sizes.
Given previous studies that showed an association of Ang-2 with improved respiratory parameters in COVID-19 patients, we aimed to see if these findings are applicable to the non-COVID-19 population. Our primary objective was to evaluate the association of Ang-2 with improved PaO2/FiO2 and SpO2/FiO2 ratios. We hypothesized that patients would have a significant hourly increase in these parameters in the 48 h after the administration of Ang-2. As a secondary endpoint, we evaluated the NED during this timeframe, and hypothesized that there would be a significant hourly decrease in NED after Ang-2 administration.
Methods
Patients
The Angiotensin II Research to Evaluate the Multi Institutional Use in Shock and Oxygenation (ARTEMIS O2) study utilized data from non-COVID-19 patients abstracted from electronic health records from multiple medical centers. The study was deemed to be exempt from institutional review board (IRB) review by the George Washington University.
Two hundred fifty-four patients were included from four academic tertiary care centers and one community hospital in the United States: George Washington University, Northeast Georgia Health System, Mayo Clinic, University of Mississippi, and St. Joseph Mercy Ann Arbor Hospital. Consecutive adult patients admitted between July 2018 and September 2020 who were administered angiotensin II for the treatment of shock were eligible for inclusion. Shock was defined as the receipt of any vasopressor for the maintenance of a mean arterial pressure (MAP) ≥ 65 mm Hg. Patients under 18 years old and those with a diagnosis of COVID-19 were excluded from the study. Demographics, comorbidities, illness severity scores, vasopressor dose, respiratory parameters, cumulative fluid balance, and outcomes were collected for all patients. Respiratory parameters such as PaO2, SpO2, and FiO2 were recorded relative to the time of Ang-2 administration at hours −48, −36, −24, −18, −12, −6, 0, 0.5, 1, 3, 6, 24, and 48, where hour 0 represented the time of Ang-2 administration. Other data such as ventilator mode, tidal volume, and PEEP were collected immediately after intubation. The NED was calculated based on previous studies. 14
Outcomes
The primary outcome of this study was the hourly change in PaO2/FiO2 during the 48 h before and after Ang-2 administration. The secondary outcome was the hourly change in SpO2/FiO2 during this timeframe. Additional exploratory outcomes included the hourly change in NED, as well as the difference in the proportion of patients with PaO2/FiO2 ≤ 300 mm Hg at the time of Ang-2 initiation and at 48 h after initiation.
Statistical Analysis
Statistical analysis was performed with SPSS Statistics 27 (IBM Corporation, Somers, NY) and R 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria) utilizing the “lme4” and “nlme” packages.20,21 Continuous variables are reported as the median value and interquartile range (IQR), and categorical variables are reported as number and percentage.
For the analysis of the primary and secondary outcomes, piecewise linear mixed models were created, one with PaO2/FiO2 as the dependent variable, and another with SpO2/FiO2 as the dependent variable. The breakpoint of each model was the time of Ang-2 initiation (hour = 0), and the time relative to the initiation of Ang-2 was entered as a fixed effect. Because multiple PaO2/FiO2 and SpO2/FiO2 values were obtained for each patient, each observation was nested within patients to account for within-patient correlations. A first-order autoregressive structure was utilized to account for the decreasing correlation of measurements with lengthening time between each measurement. Sensitivity analyses were performed whereby the duration of vasopressors prior to Ang-2 administration, the duration of Ang-2 therapy, and in-hospital mortality were included as variables in order to assess whether varying time lengths prior to Ang-2 initiation, varying duration of exposure to Ang-2, or early death could confound the primary and secondary outcomes. Lastly, we also assessed the effects of survivor bias by performing additional sensitivity analyses on piecewise linear mixed models analyses in only those who expired in the first 48 h and in only in those who survived the first 48 h of Ang-2 administration. Finally, the difference in the proportion of patients with a PaO2/FiO2 ≤ 300 mm Hg at the time of Ang-2 initiation and at 48 h after initiation was analyzed with a Wald test with continuity correction. 22 Differences in cumulative fluid balance at study time points were assessed with the Wilcoxon signed rank test.
Results
The study included 254 patients. Median age was 62 (IQR 50-70) years, and 61.0% of patients were male (Table 1). Use of home angiotensin converting enzyme inhibitors (ACE-I) and angiotensin receptor blockers (ARBs) occurred in 20.5% and 11.0% of patients, respectively. Other relevant home medications that may have increased the risk of vasoplegia were examined including milrinone (0.8%), amiodarone (3.9%), calcium channel blockers (19.7%), and beta blockers (23.6%). The etiology of shock as documented in the medical record was most commonly septic distributive (65.0%), followed by cardiogenic (22.4%), non-septic distributive (12.2%), and hypovolemic (7.1%). With a median Acute Physiology and Chronic Health Evaluation II (APACHE II) score of 23 (IQR 17-28), predicted mortality in our cohort was high. 23 Actual in-hospital mortality was 65.4%.
Patient Characteristics.
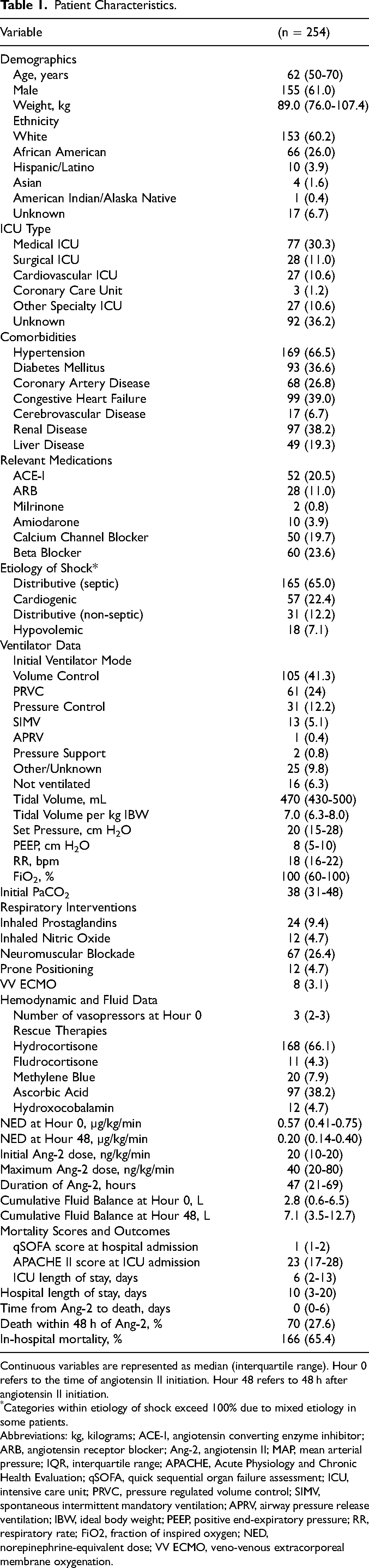
Continuous variables are represented as median (interquartile range). Hour 0 refers to the time of angiotensin II initiation. Hour 48 refers to 48 h after angiotensin II initiation.
*Categories within etiology of shock exceed 100% due to mixed etiology in some patients.
Abbreviations: kg, kilograms; ACE-I, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; Ang-2, angiotensin II; MAP, mean arterial pressure; IQR, interquartile range; APACHE, Acute Physiology and Chronic Health Evaluation; qSOFA, quick sequential organ failure assessment; ICU, intensive care unit; PRVC, pressure regulated volume control; SIMV, spontaneous intermittent mandatory ventilation; APRV, airway pressure release ventilation; IBW, ideal body weight; PEEP, positive end-expiratory pressure; RR, respiratory rate; FiO2, fraction of inspired oxygen; NED, norepinephrine-equivalent dose; VV ECMO, veno-venous extracorporeal membrane oxygenation.
Prior to Ang-2 treatment, 238 (93.7%) of patients were endotracheally intubated, and the remaining 16 (6.3%) required non-invasive therapy such as high-flow nasal cannula, continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPap). Other respiratory co-therapies included inhaled prostaglandins (9.4%) or nitric oxide (4.7%), neuromuscular paralysis (26.4%), prone positioning (4.7%), and venovenous ECMO (3.1%). For those patients who were intubated, patients received these interventions a median of 0 days (IQR 0-1) after endotracheal intubation. Patients were receiving a median of 3 vasopressors (IQR 2-3) at a NED of 0.57 µg/kg/min (IQR 0.41-0.75). Adjunctive treatments for shock most commonly included hydrocortisone (66.1%), followed by ascorbic acid (38.2%), methylene blue (7.9%), hydroxocobalamin (4.7%), and fludrocortisone (4.3%).
At 48 h prior to Ang-2 initiation, the median PaO2/FiO2 was 410 mm Hg and decreased to 146 at the time of Ang-2 treatment (Table 2). Similarly, 48 h prior to treatment with Ang-2, the median SpO2/FiO2 was 325, and decreased to 140 at the time of Ang-2 initiation. The piecewise linear mixed models incorporated measurements of each parameter at each timepoint and found significant decreases in the median PaO2/FiO2 (hourly change −4.7 mm Hg/hr, 95% CI −6.0 to −3.5, p < .001) and SpO2/FiO2 (hourly change −3.1/hr, 95% CI −3.7 to −2.4, p < .001) in the 48 h preceding Ang-2 initiation (Figure 1, Table 3).
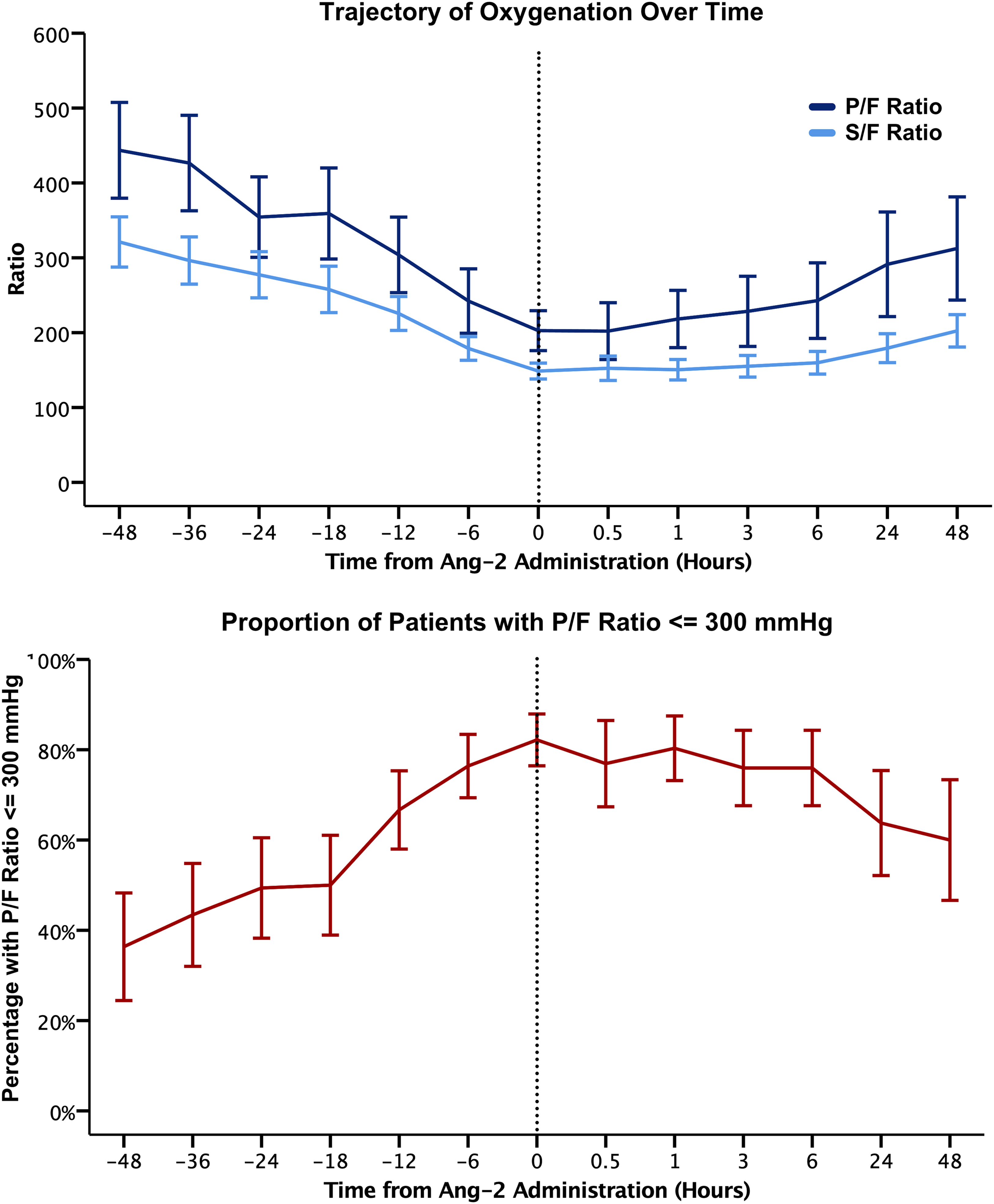
Trajectory of oxygenation over time. Mean PaO2/FiO2, SpO2/FiO2, and percentage of patients with PaO2/FiO2 ≤ 300 are depicted at each time point. Time is recorded relative to the time of Ang-2 administration. Error bars show the 95% confidence interval at each time point. The decline in oxygenation stopped at the time Ang-2 was administered and then improved significantly for both PaO2/FiO2 and SpO2/FiO2 (p < .001 for both).
Respiratory Parameters Before and After Angiotensin II Administration.
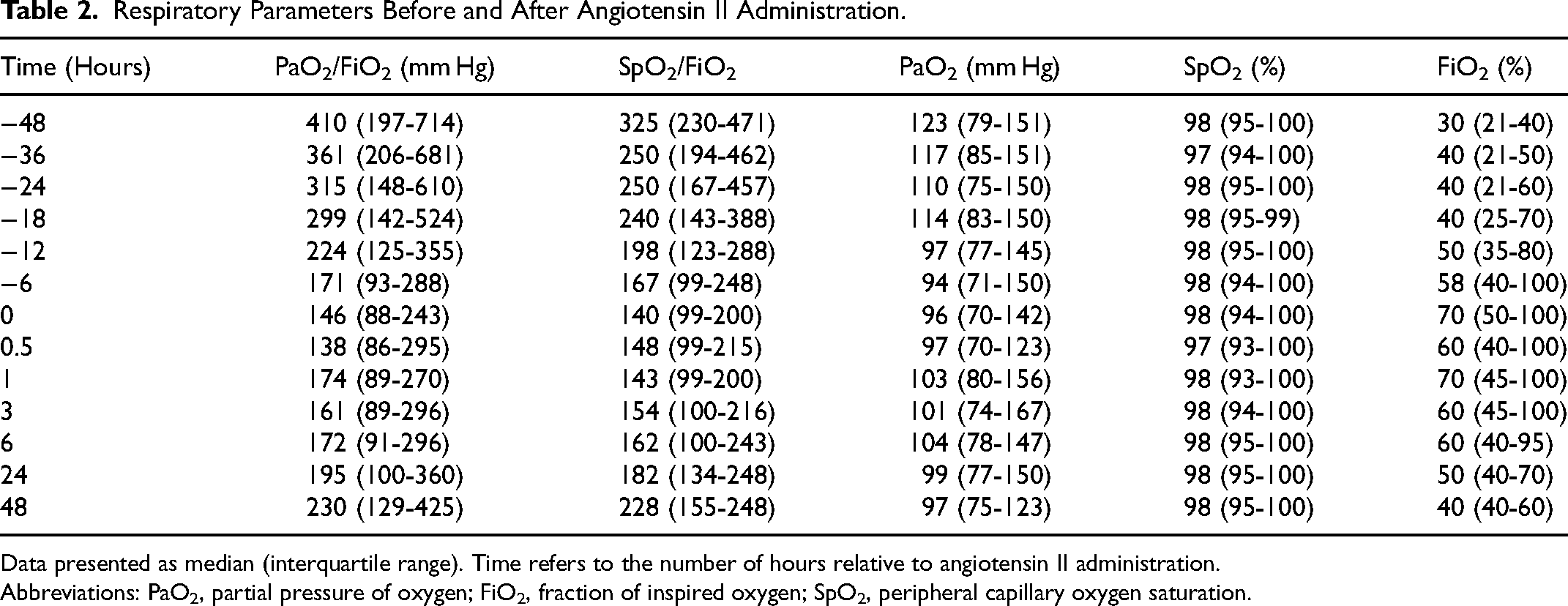
Data presented as median (interquartile range). Time refers to the number of hours relative to angiotensin II administration.
Abbreviations: PaO2, partial pressure of oxygen; FiO2, fraction of inspired oxygen; SpO2, peripheral capillary oxygen saturation.
Piecewise Linear Mixed Model of Respiratory and Hemodynamic Parameters.
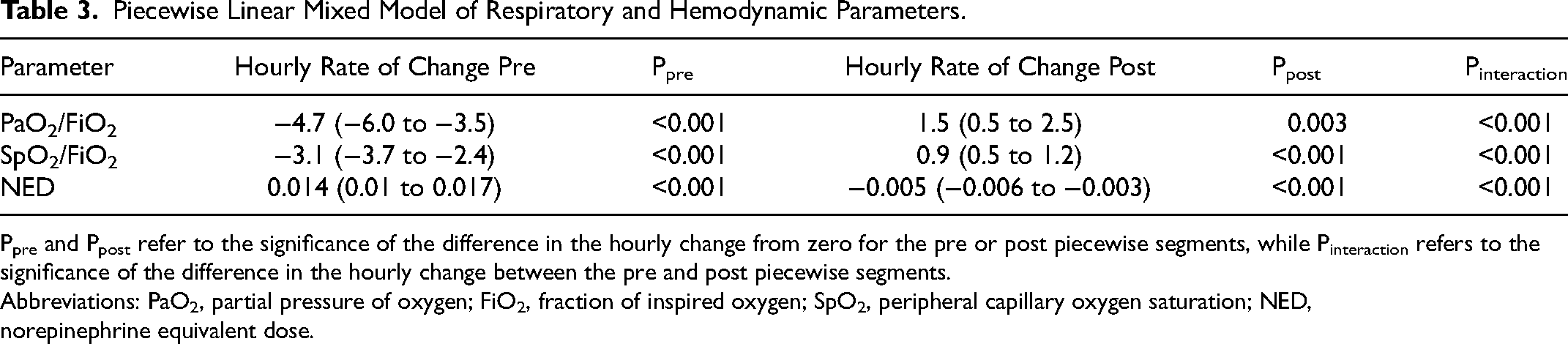
Ppre and Ppost refer to the significance of the difference in the hourly change from zero for the pre or post piecewise segments, while Pinteraction refers to the significance of the difference in the hourly change between the pre and post piecewise segments.
Abbreviations: PaO2, partial pressure of oxygen; FiO2, fraction of inspired oxygen; SpO2, peripheral capillary oxygen saturation; NED, norepinephrine equivalent dose.
Forty-eight hours after treatment with Ang-2, PaO2/FiO2 increased from 146 at baseline to 230 mm Hg. Similarly, the SpO2/FiO2 increased from 140 to 228. The rate of change in cumulative fluid balance was not significantly different between these time points (0.94 mL/kg/h pre-administration vs 0.91 mL/kg/h post-administration, pinteraction = 0.88). The piecewise linear mixed model of the post-administration timepoints found that the incremental hourly improvements in PaO2/FiO2 (change +1.5 mm Hg/hr, 95% CI 0.5-2.5, p = .003) and SpO2/FiO2 (change +0.9/hr, 95% CI 0.5–1.2, p < .001) were statistically significant. The slopes of the pre and post-administration regression lines were compared, and there was a significant difference in the hourly change of both PaO2/FiO2 and SpO2/FiO2 after Ang-2 treatment was initiated (pinteraction < 0.001 for both). This indicates that prior to Ang-2 treatment, both PaO2/FiO2 and SpO2/FiO2 were worsening, however, the trajectory reversed and significantly improved after Ang-2 was started. This improvement in oxygenation was also associated with a significantly lower proportion of patients having a PaO2/FiO2 ≤ 300 mm Hg compared to the time period before Ang-2 administration (mean difference −14.9%, 95% CI −25.3% to −4.6%, p = .011) (Figure 1). 24
Similar piecewise analysis was performed to evaluate the hourly changes in the NED during the pre- and post-Ang-2 administration timeframes. The NED was a median of 0.17 µg/kg/min (IQR 0.06–0.33) 48 h prior to Ang-2 administration and increased to 0.57 µg/kg/min (IQR 0.41–0.75) at the time Ang-2 was started (Figure 2). Forty-eight hours after Ang-2 treatment, the NED decreased to 0.20 µg/kg/min (IQR 0.14-0.40). In the piecewise analysis, the hourly increase in NED before Ang-2 initiation (hourly change + 0.014 µg/kg/min, 95% CI 0.01–0.017, p < .001), hourly decrease in NED after initiation (hourly change −0.005 µg/kg/min, 95% CI −0.006 to −0.003, p < .001), and the change in slope (pinteraction < 0.001) during these timeframes were statistically significant. Taken together, the hemodynamic data indicate that there was a significantly improved trajectory in NED after Ang-2 treatment was initiated.
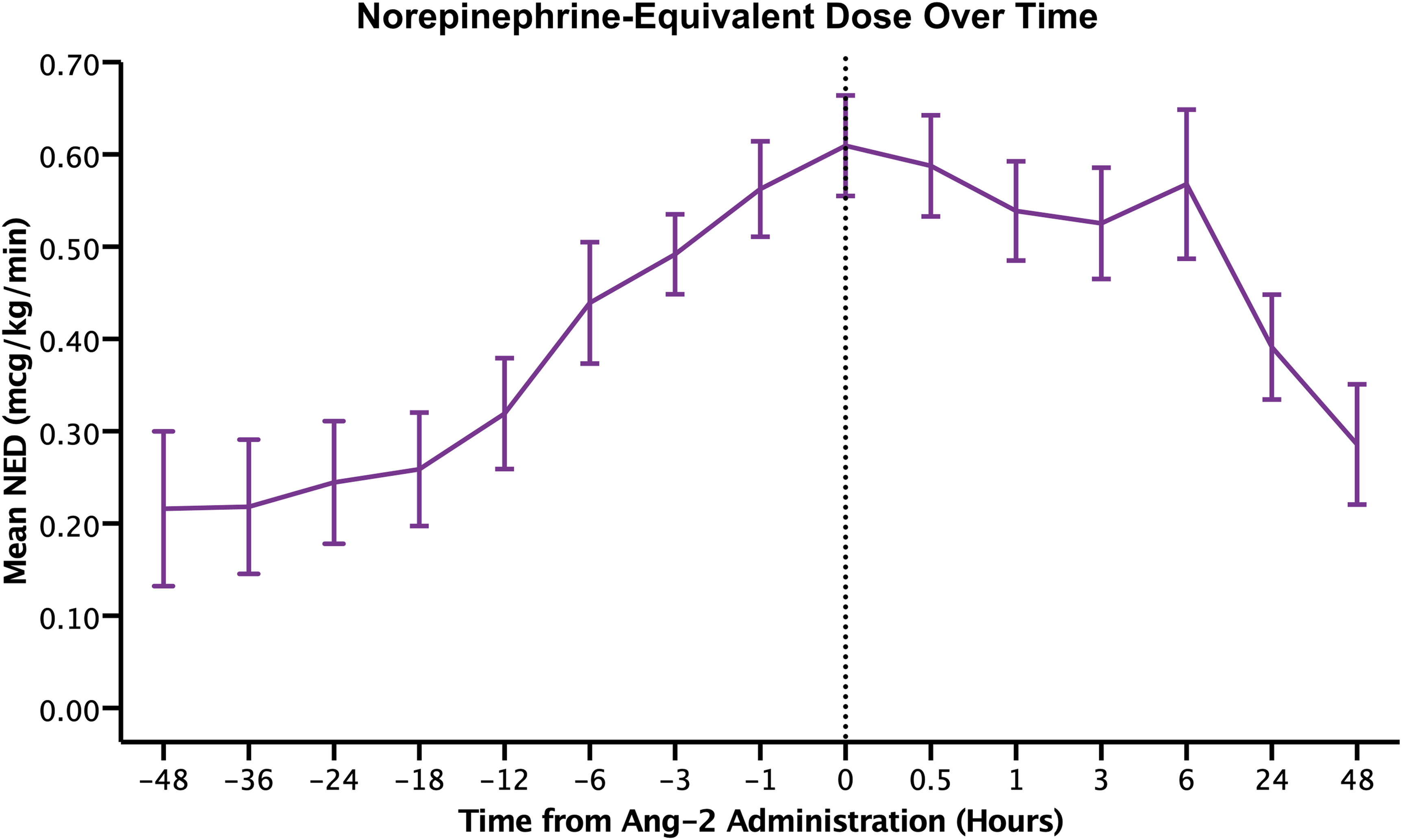
Norepinephrine-equivalent dose requirement over time. Mean NEDs at each time point are depicted. Time is recorded relative to the time of Ang-2 administration.
Subgroup Analysis
To help guide future studies, we performed a subgroup analysis of the primary outcome and stratified patients by level of oxygenation and NED at the time of Ang-2 administration. In patients with a baseline PaO2/FiO2 ≤ 300 mm Hg, there was a significant hourly improvement in PaO2/FiO2 (−6.0 mm Hg/h pre-administration versus + 1.3 mm Hg/h post-administration, pinteraction < 0.001), whereas in patients with a baseline PaO2/FiO2 > 300 mm Hg, this was not significantly different (−0.49 mm Hg/h pre-administration versus + 1.71 mm Hg/h post-administration, pinteraction = 0.34).
Similarly, patients were stratified by NED requirement at the time of Ang-2 administration, and in those with high NED requirements (>0.2 µg/kg/min), there was a significant hourly improvement in PaO2/FiO2, whereas, in those with low NED requirements at baseline, this improvement was not statistically significant. Specifically, in the subset of patients with a NED ≤0.2 µg/kg/min at the time of Ang-2 administration, the change in PaO2/FiO2 was not significant (−7.6 mm Hg/hr pre versus + 0.99 mm Hg/hr post, pinteraction = 0.48). However, the PaO2/FiO2 ratios in the subgroups of patients with a baseline NED of 0.21–0.40 µg/kg/min (−4.3 mm Hg/hr pre versus + 0.04 mm Hg/hr post, pinteraction = 0.002), NED 0.41–0.60 µg/kg/min (−5.6 mm Hg/hr pre versus + 1.6 mm Hg/hr post, pinteraction < 0.001), and NED >0.60 µg/kg/min (−5.4 mm Hg/hr pre versus + 1.9 mm Hg/hr post, pinteraction < 0.001), were associated with significant improvements in oxygenation.
Sensitivity Analysis
In the first sensitivity analysis, the duration of vasopressors prior to Ang-2 administration, the duration of Ang-2 therapy, and in-hospital mortality were added as independent variables to the models to assess their impact on the primary outcome. Consistent with the original models, there remained significant hourly worsening of the median PaO2/FiO2 (−5.4 mm Hg/h, 95% CI −6.9 to −4.0, p < .001), SpO2/FiO2 (−3.5/h, 95% CI −4.1 to −2.8, p < .001), and NED (hourly change 0.020 µg/kg/min, 95% CI 0.016–0.024, p < .001) in the 48 h preceding Ang-2 initiation. After Ang-2 initiation, there were significant hourly improvements in the median PaO2/FiO2 (1.5 mm Hg/hr, 95% CI 0.6-2.5, p = .002), SpO2/FiO2 (0.5 mm Hg/hr, 95% CI 0.2–0.8, p < .001), and NED (hourly change −0.006 µg/kg/min, 95% CI −0.007 to −0.004, p < .001). The differences in the pre- and post-administration hourly change for all three variables remained statistically significant (pinteraction < 0.001 for all).
In the first 48-h following Ang-2 initiation, 70 patients (27.6%) expired (Table 1). A second sensitivity analysis was performed to assess for any potential impact of this early death on the trajectory of PaO2/FiO2 and SpO2/FiO2. The models were separately computed for those surviving the first 48 h and for those expiring within the first 48 h. In the population who survived the first 48 h of Ang-2 therapy, there was significant worsening of oxygenation prior to Ang-2 and significant improvement in oxygenation after Ang-2 administration (PaO2/FiO2 hourly change pre −5.9 mm Hg/hr, 95% CI −7.4 to −4.4, p < .001; post + 1.6 mm Hg/hr, 95% CI 0.6-2.6, p = .001; difference in hourly change pinteraction < 0.001; SpO2/FiO2 hourly change pre −4.0/h, 95% CI −4.7 to −3.3, p < .001; post + 0.5/h, 95% CI 0.2–0.8, p = .001; difference in hourly change pinteraction < 0.001). Similarly, when examining only the population who expired in the first 48 h of Ang-2 therapy, there were also statistically significant improvements in oxygenation before and after Ang-2 therapy (PaO2/FiO2 hourly change pre −4.7 mm Hg/h, 95% CI −6.0 to −3.5, p < .001; post + 1.5 mm Hg/hr, 95% CI 0.5–2.5, p = .003; difference in hourly change pinteraction < 0.001; SpO2/FiO2 hourly change pre −3.0/h, 95% CI −3.7 to −2.4, p < .001; post + 0.5/h, 95% CI 0.3–0.8, p < .001; difference in hourly change pinteraction < 0.001).
Discussion
Multiple studies have demonstrated that Ang-2 treatment is associated with improved hemodynamics in distributive shock and improved outcomes in certain subgroups, such as in high-renin shock and in AKI requiring renal replacement therapy.14–17,25,26 Our hypothesis-generating pilot study is the largest examining the association between Ang-2 treatment and improved oxygenation in critically ill patients and the first performed in the non-COVID-19 population. One case series of 16 COVID-19 positive patients in Italy found that there was a significant improvement in oxygenation during the 48-h timeframe after Ang-2 treatment. 18 Specifically, SpO2/FiO2 increased from 140.7 to 193.8, FiO2 improved from 70% to 40%, and PEEP decreased from 14 to 11 cmH2O. The hourly improvement in these parameters was statistically significant, but the hourly improvement in PaO2/FiO2 was not. 18
In a propensity-matched study of 29 COVID-19 patients in New York, patients receiving Ang-2 had a significant reduction in PEEP, whereas those in the control group did not (PEEP difference −1.8 cm/H2O/day, pinteraction = 0.004). 19 In addition, after adjustment for minute ventilation, hypercapnia was also improved in the Ang-2 group compared to controls at 48 h (mean change −7.2 mm Hg/day, pinteraction = 0.01) and at 7 days (mean change −2.0 mm Hg, pinteraction = 0.009). All of these improvements occurred in the context of significantly decreased vasopressor requirements in the Ang-2 group over this time frame. 19 When examining the daily improvement in PaO2/FiO2, this difference was again not significant (difference 26.7 mm Hg/day, pinteraction = 0.13). However, with only 29 patients in the study, it was likely not adequately powered to detect this difference. 19
In our cohort, oxygenation was significantly worsening prior to Ang-2 treatment, but was associated with significant improvements after Ang-2 was initiated. This occurred in conjunction with a reduction in the NED requirement. The oxygenation improvement occurred rapidly and was observed in as little as 1 h after Ang-2 treatment was initiated. This rapidity is consistent with the kinetic profile and rapid onset of Ang-2. Patients were not observed to have a significant difference in the rate of change in cumulative fluid balance before and after Ang-2 initiation, making these findings unlikely to be the result of changes in fluid balance.
Intrapulmonary Shunt
The mechanisms that explain our study's findings are not entirely clear and could be the result of improved intrapulmonary shunt, V/Q matching, or oxygen delivery. In contrast to catecholamines, which act on α and β receptors, Ang-2 acts on angiotensin type I (AT1) receptors and is an effective catecholamine-sparing agent. 4 High levels of catecholamines have been implicated in causing pulmonary edema and intrapulmonary shunt.10–12 The pulmonary vasculature contains abundant α and β receptors, and sympathetic overactivation by catecholamines can directly agonize these receptors and increase pro-inflammatory cytokines such as interleukins and tumor necrosis factor-α. 27 Both of these mechanisms compromise the pulmonary endothelium, increase pulmonary venule permeability, and allow for the rapid development of pulmonary edema.11,28 In neurogenic pulmonary edema (NPE), excess sympathetic activity plays a central role in the disease. 29 In rodent and canines, central nervous system (CNS) injury have led to hypoxemia and increased pulmonary vascular resistance, but these were prevented when an alpha antagonist such as phentolamine or phenoxybenzamine were administered prior to injury.30,31 In CNS-injured monkeys, sympathetic denervation also prevented pulmonary edema from occurring. 32
One case report describes severe pulmonary edema in a patient with plasma catecholamine and urine metanephrine levels 2–20 times normal limits. 10 Catecholamine blockade with phentolamine resulted in improvement in FiO2 and PEEP within hours. 14 When phentolamine was abruptly discontinued, the patient's oxygenation rapidly deteriorated, and when it was restarted, the gas exchange quickly improved. Another case report describes pheochromocytoma, pulmonary edema, and hypotension in a patient with plasma norepinephrine and epinephrine levels 4–8 times the normal limit. 13 Exogenous norepinephrine infusion reproduced the radiologic findings and hypoxemia, which resolved when the norepinephrine infusion was stopped. Additional hypoxemic crises were associated with elevated plasma catecholamine levels and resolved with the administration of phentolamine. 13
These data indicate that catecholamines may have a critical role in the formation of pulmonary edema. Excess adrenergic stimulation from endogenously produced catecholamines result in worsening oxygenation and intrapulmonary shunt, and high doses of exogenous catecholamines may impair oxygenation through a similar mechanism. 13 Our subgroup analysis demonstrating improvements in oxygenation in those on high-dose vasopressors, but not low-dose vasopressors, is consistent with this theory. However, because this study utilized within-patients comparisons instead of between-patients comparisons to an Ang-2 naïve population, whether similar effects might be observed with other non-catecholamines such as vasopressin, remains unclear.
V/Q Mismatch
Another possible explanation for our findings is through improved V/Q matching from a reduction in catecholamine and vasopressin doses. Because of its β2 properties, epinephrine has been shown to decrease hypoxic pulmonary vasoconstriction (HPV) at low doses. 8 However, at high doses, it may increase vasoconstriction in well-oxygenated alveoli, which increases V/Q mismatch. 8 In a study of 16 patients receiving norepinephrine for ARDS, patients failed to have an increase in P/F ratio with the addition of nitric oxide (NO). 9 This suggests that norepinephrine may impair HPV as a non-selective vasoconstrictor by acting on both the extra-pulmonary and intra-pulmonary vasculature. In addition, vasopressin causes pulmonary vasodilation at low doses, which attenuates HPV and also leads to increased V/Q mismatch. 33 In animal studies, the data on the relationship between Ang-2 and HPV is mixed, and some have found enhanced HPV, while others have found no effect.34–37 In humans, renin-angiotensin-aldosterone (RAAS) antagonists such as ACE-Is and ARBs have been found to inhibit HPV.38,39 Conversely, although it may be possible that RASS agonists may have opposite effects on HPV, this is speculative and warrants further investigation.
Oxygen Delivery
Increased oxygen delivery from improved cardiac output could also account for our findings. In animal studies, Ang-2 has been shown to increase cardiac output, heart rate, and stroke volume. 40 In humans, the role of Ang-2 is not clear, as there are no studies that directly measure its effect on cardiac output. When examining RAAS antagonists such as ACE-Is, the data is mixed – cardiac output is not changed in patients with normal ventricular function, but is improved in those with congestive heart failure. 41 The catecholamine-sparing properties of Ang-2 may also play a role in improving oxygen delivery. Excessive sympathetic stimulation by catecholamines can lead to impaired diastolic function, myocardial stunning, and myocardial ischemia. 42 Vasopressin has been shown in multiple studies to decrease cardiac output in septic shock.43–46 Additional studies examining the effect of Ang-2 on cardiac output and oxygen delivery are certainly warranted to elucidate whether this is a plausible mechanism for our findings.
Limitations
There are several limitations to our study. It is retrospective and observational, and the ability to completely control for confounding variables is limited. Thus, our results may not be generalizable to other groups of critically ill patients. Although this is one of the largest studies examining Ang-2, our study only included 254 patients and is subject to bias from the limited sample size. As this was a multi-center study, each center had different protocols and thresholds for Ang-2 initiation, which may confound our results. Additionally, because Ang-2 tends to be applied in settings of refractory shock, high severity of illness, with imminent likelihood of death, our study may be prone to a survivor bias. Because of this, we performed sensitivity analyses to account for both survival after 48 h and early death within the first 48 h of Ang-2 therapy and found that the changes in oxygenation indexes and NED remained significant. Our study did not have a group of Ang-2 naïve patients to make between-patients comparisons. Instead, comparisons were performed within-patients where the timeframe prior to Ang-2 therapy was utilized as the control, and this is a limitation of our study. It is possible that the respiratory parameters could have improved over time from other factors unrelated to Ang-2 therapy. Furthermore, whether these results are due to mechanisms unique to Ang-2, related to catecholamine-sparing, or due to other non-catecholamine vasopressors such as vasopressin, are unknown because of the lack of an Ang-2 naïve arm to make between-patients comparison. Nevertheless, our study, in combination with prior studies published by other investigators, provides evidence that Ang-2 therapy may be associated with improved respiratory parameters in patients with shock.18,19 This is a hypothesis-generating pilot study, that can guide future investigations on the relationships between catecholamines, ventilation-perfusion matching, and Ang-2 in patients with shock.
Conclusion
In this multi-center study of 254 patients, PaO2/FiO2, SpO2/FiO2, and NED significantly worsened in the 48-h period prior to Ang-2 initiation. Treatment with Ang-2 was associated with a reduction in NED and a significant improvement in oxygenation. This corresponded with a decrease in the percentage of patients with a PaO2/FiO2 ≤ 300 compared to baseline. The subgroups with impaired oxygenation (PaO2/FiO2 ≤ 300) or high vasopressor requirements at baseline (NED > 0.2 µg/kg/min) had the greatest recovery in oxygenation. Improved intrapulmonary shunt, V/Q mismatch, or oxygen delivery may account for these findings. It is unclear whether or not these findings can be explained by the reduction in NED alone, rather than by an effect of the Ang-2 or simply a non-catecholamine vasopressor effect that could be afforded by other agents such as vasopressin. Future mechanistic studies should examine how Ang-2 and catecholamines may alter oxygenation in critically ill patients and include well-designed comparisons to Ang-2 naïve patients.
Supplemental Material
sj-docx-1-jic-10.1177_08850666231174870 - Supplemental material for Trajectory of PaO2/FiO2 Ratio in Shock After Angiotensin II
Supplemental material, sj-docx-1-jic-10.1177_08850666231174870 for Trajectory of PaO2/FiO2 Ratio in Shock After Angiotensin II by Patrick M. Wieruszewski, PharmD, Patrick J. Coleman, MD, MPH, Maj, MC, Andrea R. Levine, MD, Danielle Davison, MD, Nathan J. Smischney, MD, MSc, Shravan Kethireddy, MD, Yanglin Guo, MD, Jason Hecht, PharmD, Michael A. Mazzeffi, MD, and Jonathan H. Chow, MD in Journal of Intensive Care Medicine
Footnotes
Acknowledgements
The authors would like to thank Mark Meersman, Drew Dalton, Ivy Benjenk, PhD, and Richard Amdur, PhD for their assistance in obtaining and analyzing the data for this study.
Authorship Statement
Conception and design of the study: Wieruszewski, Coleman, Davison, Mazzeffi, Chow
Acquisition of data: Smischney, Wieruszewski, Yamane, Kethireddy, Levine, Park, Guo, Hecht, Benjenk, Cain, Chaffay, Merren, Gerdes, Boswell, Cruz, Danielson, Azzo, Chisti, Haridasa, Chow
Analysis and interpretation of data: Coleman, Wieruszewski, Davison, Mazzeffi, Chow
Drafted or provided critical revisions: Coleman, Davison, Smischney, Wieruszewski, Yamane, Kethireddy, Levine, Park, Guo, Hecht, Cain, Chaffay, Merren, Gerdes, Boswell, Cruz, Danielson, Azzo, Chisti, Haridasa, Mazzeffi, Chow
Provided final approval of manuscript: Coleman, Davison, Smischney, Wieruszewski, Yamane, Kethireddy, Levine, Park, Guo, Hecht, Cain, Chaffay, Merren, Gerdes, Boswell, Cruz, Danielson, Azzo, Chisti, Haridasa, Mazzeffi, Chow
Ethics Approval
The study was deemed to be exempt by George Washington University Institutional Review Board (IRB).
Consent to Participate
The requirement for written informed consent was waived by the IRB.
Consent for Publication
The requirement for written informed consent was waived by the IRB.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SK and JHC have served on the Speaker's Bureau for La Jolla Pharmaceutical Company. PMW has previously served on a scientific advisory board for La Jolla Pharmaceutical Company. La Jolla Pharmaceutical Company was not involved in any aspect of the conduct of this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.