
Abstract
High-risk pulmonary embolism (PE) also known as massive PE carries a high rate of morbidity and mortality. The incidence of high-risk PE continues to increase, yet the outcomes of high-risk PE continue to remain poor. Patients with high-risk PE are often critically ill, with complex underlying physiology, and treatment for the high-risk PE patient almost always requires care and management from an intensivist. Treatment options for high-risk PE continue to evolve rapidly with multiple options for definitive reperfusion therapy and supportive care. A thorough understanding of the physiology, risk stratification, treatment, and support options for the high-risk PE patient is necessary for all intensivists in order to improve outcomes. This article aims to provide a review from an intensivist's perspective highlighting the physiological consequences, risk stratification, and treatment options for these patients as well as providing a proposed algorithm to the risk stratification and acute management of high-risk PE.
Introduction
Acute pulmonary embolism (PE) continues to be a leading cause of mortality. It estimated to be the third leading cause of cardiovascular mortality in the United States (US). 1 High-risk, also known as massive, PE represents the most severe form of PE, carrying a high rate of morbidity and mortality even with treatment. 2 There is a wide variation in the presentation of the high-risk PE patient, and its recognition and urgent treatment is important. By definition, high-risk PE patients are hemodynamically unstable and often require care in an intensive care unit. An understanding of treatment options for high-risk PE is paramount for intensivists given the complex physiology that is encountered in high-risk PE. The use of systemic thrombolysis (ST) is often discussed as the first-line treatment strategy for high-risk PE, but there has been an increase in alternative treatment strategies including catheter and surgical embolectomy and mechanical circulatory support (MCS) options that an intensivist should be aware of. This review will outline the current treatment options for the high-risk PE patient, address risk stratification, review supportive care options including anticoagulation and right ventricle support, and provide an algorithm to assist in the management of the high-risk PE patient. Although high-risk PE can affect all ages and populations, this review will focus primarily on the adult population. The management of unique PE populations such as PE in the pediatric patient, pregnancy, or acute on chronic thromboembolic disease is beyond the scope of the current review and as such is not covered in the current review.
Definition/Incidence/Mortality
High-risk PE also known as massive PE is defined as patients who exhibit hemodynamic instability in the setting of an acute PE. The European Society of Cardiology defines this as 1 or more of the following: (i) cardiac arrest, (ii) systolic blood pressure (SBP) of < 90 mmHg with end-organ hypoperfusion or need of vasopressors to maintain SBP > 90 mmHg, and (iii) persistent SBP < 90 mmHg or a drop in SBP of ≥ 40 mmHg lasting for 15 min without an alternative etiology. 3 The current definition of high-risk PE encompasses a broad spectrum of phenotypes from a relatively stable hemodynamic and clinical presentation, to either shock with stable, low-dose vasopressor requirements, escalating multi-vasopressor shock, shock requiring MCS, catastrophic presentations with cardiac arrest, or sudden cardiac death. The incidence of high-risk PE is estimated to be between 3% and 12% depending on the studied cohort.4,5 The exact incidence is likely higher given that the most severe form of high-risk PE is cardiac arrest or sudden cardiac death, and the etiology of death in non-survivors may not always be evaluated or known unless an autopsy is performed. 6 Mortality from high-risk PE remains high despite established recommended treatment with ST and anticoagulation with an estimate for all-cause mortality to be 40%. 7 Those with high-risk PE who require mechanical ventilation (MV) may have a mortality rate approaching 80% and those who suffer a cardiopulmonary arrest have mortality rates ranging from 65% to 95%.8,9 Novel approaches in treatment for high-risk PE including the use of percutaneous embolectomy, surgical embolectomy, and MCS may improve mortality and outcomes in this patient population.5,10
Diagnosis of High-Risk PE
Acute PE is most often diagnosed by computed topography pulmonary angiogram (CTPA) or ventilation perfusion (V/Q) scan. CTPA has the advantage of providing rapid diagnosis of PE or an alternative diagnosis. CTPA also allows for the assessment of cardiac and other vascular structures and helps identify the presence of right ventricular (RV) dysfunction. Certain CTPA findings have also been associated with poor outcomes in PE patients, for example, an increased RV to left ventricle (LV) ratios of > 1.5 with reflux of contrast is associated with adverse outcomes, while a decrease in left atrial volume is associated with increased mortality.11,12 Some patients may be too unstable for definitive imaging with CTPA or VQ to diagnose PE. Transthoracic echocardiography (TTE) and/or transesophageal echocardiography (TEE) may be able to visualize the proximal pulmonary arteries and identify PE to make a formal diagnosis. In scenarios where the proximal arteries cannot be visualized or there is a high clinical suspicion despite no thrombi visualized by TTE/TEE, point-of-care ultrasound may aid in determining the likelihood of the diagnosis if the presence of deep vein thrombosis, right-heart thrombi (RHT), or acute RV dysfunction is identified on ultrasound.13,14
Pathophysiologic Consequences of High-Risk PE
Under normal physiology, the RV contracts against a low resistance, high compliance, pulmonary vascular bed. Additionally, the RV is morphologically and structurally different compared to the LV which accounts for their differing adaptive response to increasing preload and afterload. 15 The more muscular LV, with its circumferentially arrayed fibers, is able to withstand sudden increases in afterload, but is less adaptive to increases in preload. On the other hand, the RV is able to accommodate large increases in venous return that is typical of the physiological response to exercise. This is likely because the normal RV is able to retain its shape rather than stretch, allowing it to adapt to increasing preload. The highly compliant RV is also able to function normally for decades in pathogenic states of increased preload, such as that seen in left to right intracardiac shunt defects. 16 However, in scenarios of acute increases in RV afterload such as that encountered in acute PE, the RV falters (Figure 1).
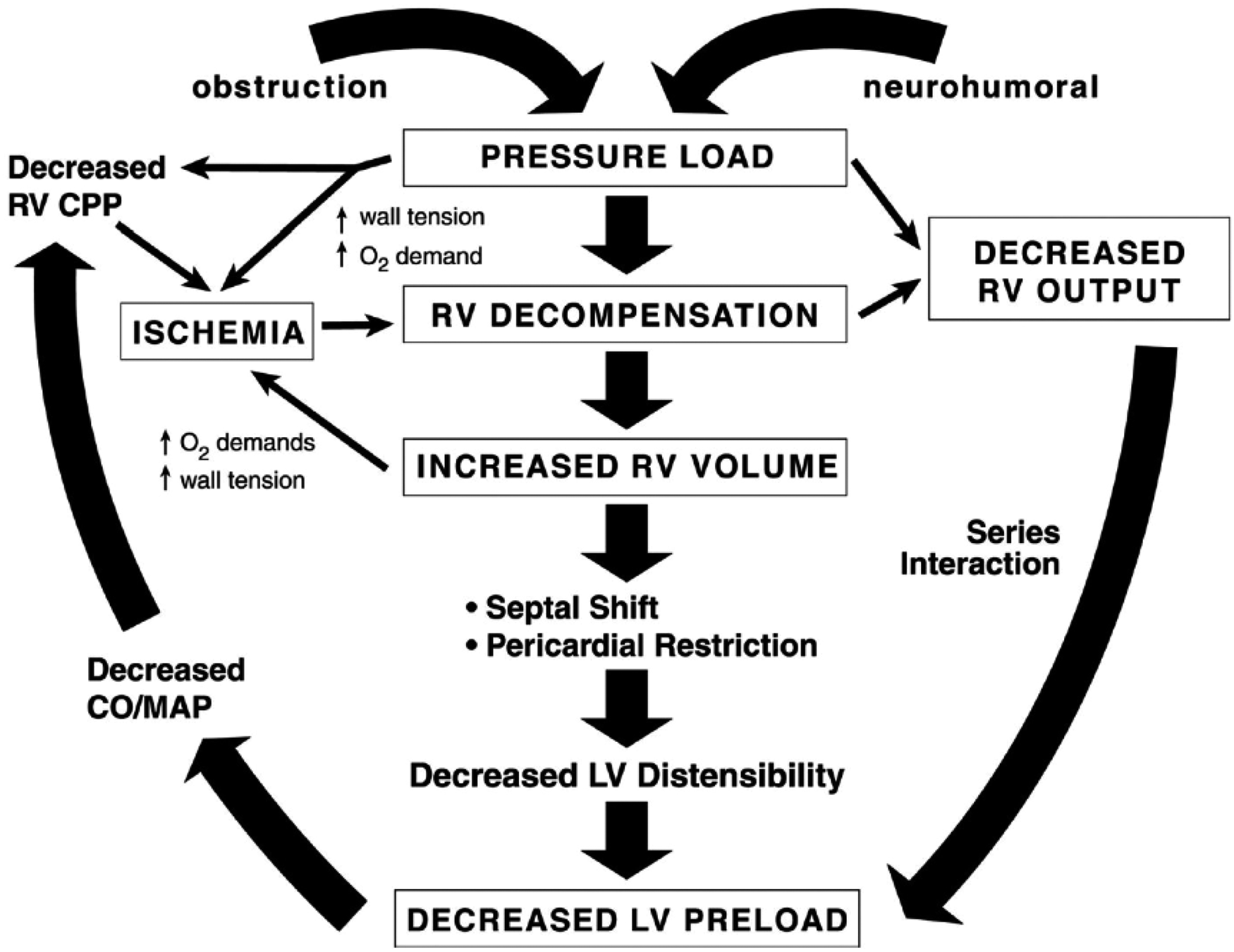
Right ventricle spiral of death.
The initial response of the RV to the sudden increase in afterload is to increase its contractile reserve to match the increasing afterload. This adaptation is initially achieved through an increase in sympathetic output. The matching of RV contractility (termed end-systolic elastance, Ees) and its afterload (termed arterial elastance, Ea) describes RV-PA coupling, and its preservation allows for optimal RV functioning at minimal energy cost.17–20 However, when the RV is no longer able to augment its contractile force in the face of increasing afterload, the RV dilates and shifts to rely on heterometric or volumetric adaptation (ie, the Frank–Starling mechanism) to sustain its flow output in response to increasing metabolic demand. 15 With worsening RV function, the decreasing RV stroke volume leads to a compensatory increase in the heart rate, which in turn further increases its afterload. 21 The resulting increase in Ea with failure to mount a corresponding increase in Ees leads to RV-PA uncoupling.22,23 These (mal)adaptive RV responses also result in a serial and parallel impact on LV function and subsequent circulatory collapse, if left untreated. First, the diminished RV stroke volume results in reduced antegrade filling of the LV (ie, serial RV–LV interaction). Next, as the RV progressively dilates, the interventricular septum shifts toward the LV results in further underfilling of the LV (ie, parallel RV–LV interaction). The reduced LV output along with increasing RV free wall tension reduces the mean systemic arterial pressure and consequently the coronary artery to RV perfusion gradient, resulting in RV ischemia and infarction. Eventually, myocardial oxygen demand exceeds supply and RV contractility further declines resulting in RV-PA uncoupling, RV failure, and further reduction in systemic arterial pressure.24,25 Sustained reductions in systemic blood pressure and shock can be late manifestations of PE as other markers of RV dysfunction may be evident earlier on imaging (CTPA and TTE) such as increased RV volume, reduced RV contractility, and demand ischemia in the form of elevated cardiac biomarkers such as troponin levels. Echocardiography may play a crucial role in determining the severity of RV dysfunction by assessing functional parameters such as tricuspid annular plane systolic excursion (TAPSE), tricuspid annular systolic velocity (S′), right ventricular systolic pressure (RVSP), TAPSE/RVSP, and velocity time integrals of both the RV and LV, which have prognostic implications for patients diagnosed with acute PE.23,26–28
In addition to circulatory failure observed in high-risk PE, disruptions in pulmonary physiology also occur due to abnormal alveolar VQ ratios contributing to abnormal gas exchange. A major pathophysiologic consequence of acute PE is an increased alveolar dead space. This occurs because lung units continue to be ventilated in spite of diminished or absent perfusion. Complete vascular obstruction by a PE causes an increase in absolute dead space. In contrast, incomplete obstruction of a pulmonary artery (ie, increased ventilation relative to perfusion) increases physiologic dead space by increasing ratios of ventilation relative to blood of involved lung units. These effects may impair the efficient elimination of carbon dioxide by the lung. Although an acute PE may impair carbon dioxide elimination, hypercapnia with resulting respiratory acidosis rarely accompanies acute PE. This presumably reflects the fact that compensatory hyperventilation eliminates carbon dioxide in all but the most extensive PE. Patients with high-risk PE are at risk for hypercapnia due to the potential extensive clot burden and due to the inability to effectively clear carbon dioxide to compensate for their underlying shock and concomitant metabolic acidosis. In cases with a sufficient degree of vascular obstruction to produce hypercapnia, the hemodynamic sequelae of acute RV failure typically prove fatal. 29 In some patients, there may be evidence of intracardiac shunting via right to left communication such as a patent foramen ovale, leading to worsening hypoxemia. Furthermore, reduced cardiac output can lead to reduced mixed venous oxygen due to reduced pulmonary blood flow which can further worsen the hypoxemia by presenting the pulmonary capillary with lower oxygen. 30
Risk Stratification
There is currently no agreed upon risk stratification for patients identified with high-risk PE. As noted above, the diagnosis of high-risk PE is defined as hemodynamic instability which has a wide spectrum of presentations. Given the wide variation in presentation, there is a need to further sub-classify high-risk PE patients to match urgency and intensity of treatment to the severity of the disease, similar to intermediate-risk PE which is further subclassified to intermediate-high and intermediate-low. 3 A patient on a low-dose, stable, single vasopressor with minimal evidence of organ dysfunction will be treated differently compared to a patient in a peri-arrest or active cardiopulmonary arrest secondary to PE, although both would be classified as high-risk PE. Carroll et al proposed a further subclassification of high-risk PE to include stable high-risk and catastrophic high-risk PE. 5 There may be a role to further subclassify high-risk PE into 3 categories to include stable, unstable, and catastrophic to better capture the wide variation in presentation (Table 1). In addition to severity of shock, other poor prognostic signs include advanced comorbid conditions, need for intubation, degree of organ injury, prior cardiac arrest, and concomitant RHT, all of which may be associated with increased rates of mortality.8,9
Subclassification of High-Risk PE.
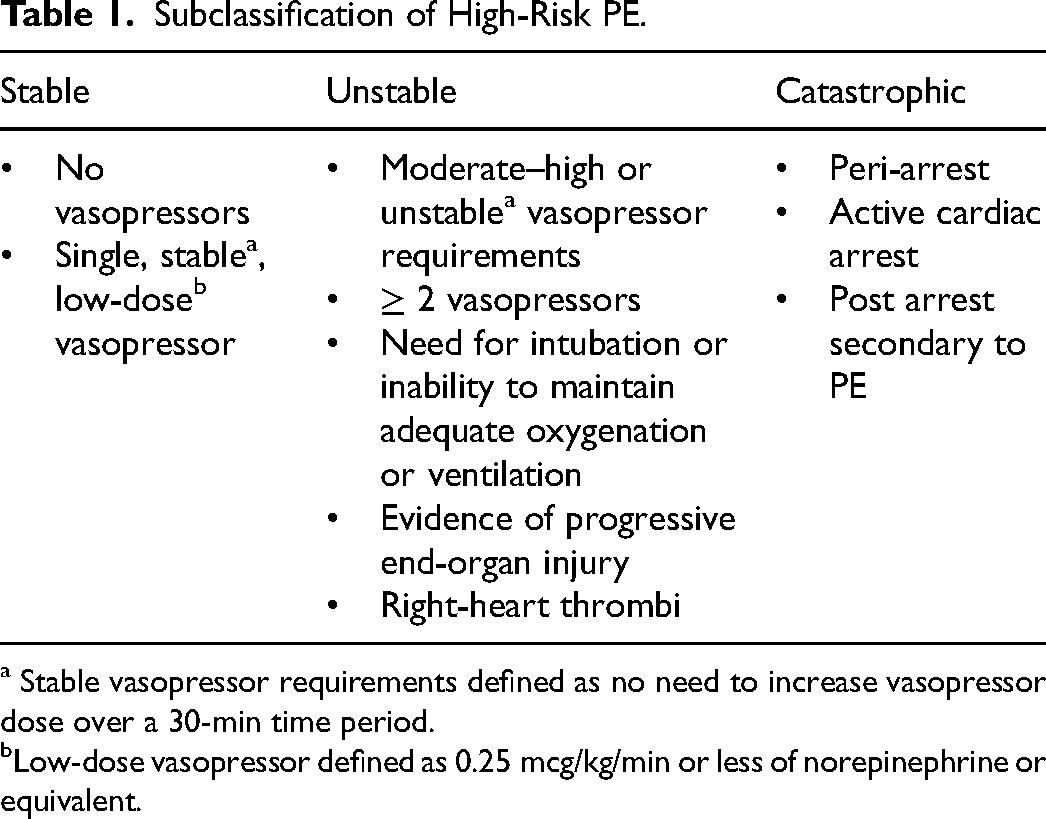
Stable vasopressor requirements defined as no need to increase vasopressor dose over a 30-min time period.
Low-dose vasopressor defined as 0.25 mcg/kg/min or less of norepinephrine or equivalent.
Treatment Considerations
Treatment of high-risk PE is a medical emergency and is focused on immediate reperfusion therapy to alleviate the pulmonary obstruction and anticoagulation, supporting the RV, preventing additional increases in PVR, and maintaining systemic perfusion and oxygen delivery. An outline of treatment based on severity of high-risk PE can be found in Figure 2.
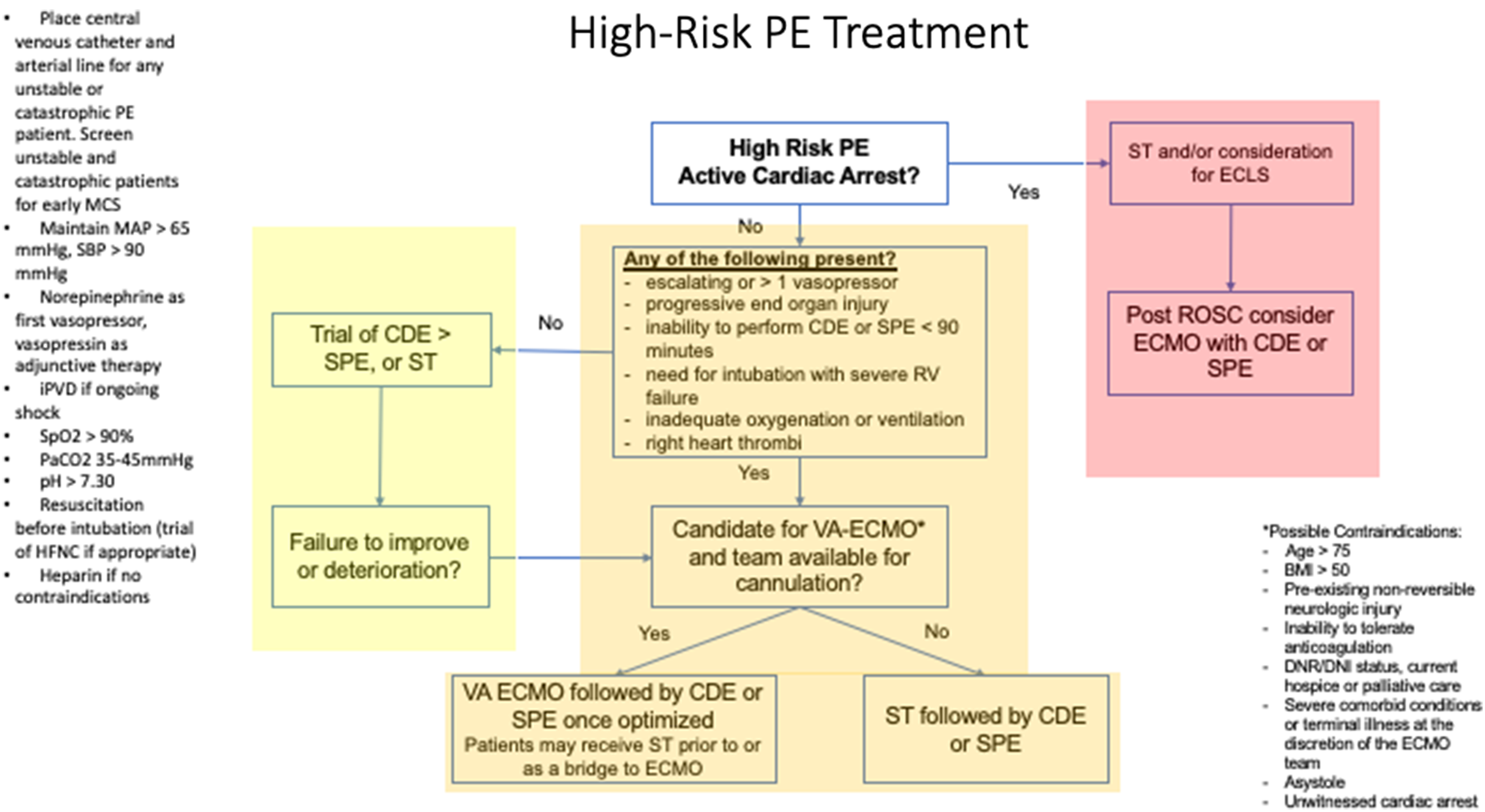
Proposed algorithm for the treatment of high-risk pulmonary embolism (PE).
Reperfusion Therapy
The goal of reperfusion therapy is to remove or reduce the thrombi from PE that is leading to the obstructive shock. Reducing the degree of pulmonary vascular obstruction will lead to reductions in RV afterload and improve RV stroke volume and LV preload. Options for reperfusion therapy include ST, catheter-directed thrombolysis (CDT), catheter-directed embolectomy (CDE), surgical pulmonary embolectomy (SPE), and MCS such as veno-arterial extracorporeal membrane oxygenation (VA-ECMO). Unlike acute coronary syndrome and acute ischemic stroke, there are no time metrics for reperfusion therapy, but it is assumed that delays in treatment are associated with worst outcomes. At the time of this review, ST is the current first-line recommended therapy for those without contraindications who present with high-risk PE. 3
Systemic Thrombolytics (ST)
ST is an appealing treatment option as it is readily available, easy to administer, and does not require specialized equipment or personnel to administer. The optimal agent for ST, dose, and timing of administration is not known, but there are recommended regimens that are often followed (Table 2). 3 Common agents include alteplase and tenecteplase. Alteplase is currently approved by the US Food and Drug Administration for PE; however, tenecteplase is not. The 2 agents differ on dosing and administration and have different pharmacokinetics. Tenecteplase has a higher fibrin specificity and longer half-life compared to alteplase leading to reduced bleeding events, and this also permits it to be administered a bolus dose rather than a continuous infusion.31,32 Tenecteplase has weight-based dosing considerations, whereas there are no weight-based alterations to alteplase. There is a growing interest in the use of tenecteplase for PE in the US given its increasing use for treatment of acute ischemic stroke, potential reduction in bleeding events, faster administration, and ideal weight-based dosing administration. The most significant complication of ST is the risk of major and potentially life-threatening bleeding. Complications may be higher in the high-risk PE patient given the increased likelihood for concomitant multiorgan failure and coagulopathy, which can alter the normal pharmacokinetics of ST. There are a large number of relative and absolute contraindications to ST, and up to 40% of patients may have a relative or absolute contraindication to ST, limiting its use (Table 2).33,34 There is also a concern that ST may not be effective against sub-acute or chronic thrombi. Given the limitations of ST, there is a growing interest in alternative treatment strategies to ST monotherapy for the treatment of high-risk PE. Alternative treatment strategies include rapid percutaneous or surgical treatment options with concomitant MCS.5,10 There are currently no randomized controlled trials looking at which type of reperfusion therapy, the timing of reperfusion therapy, or what combination of reperfusion therapies is superior for the management of the high-risk PE patient. Percutaneous treatment strategies for acute PE continue to evolve and currently present itself with a number of different device options available.
Systemic Thrombolytic Regimens and Contraindications to Systemic Thrombolytics.
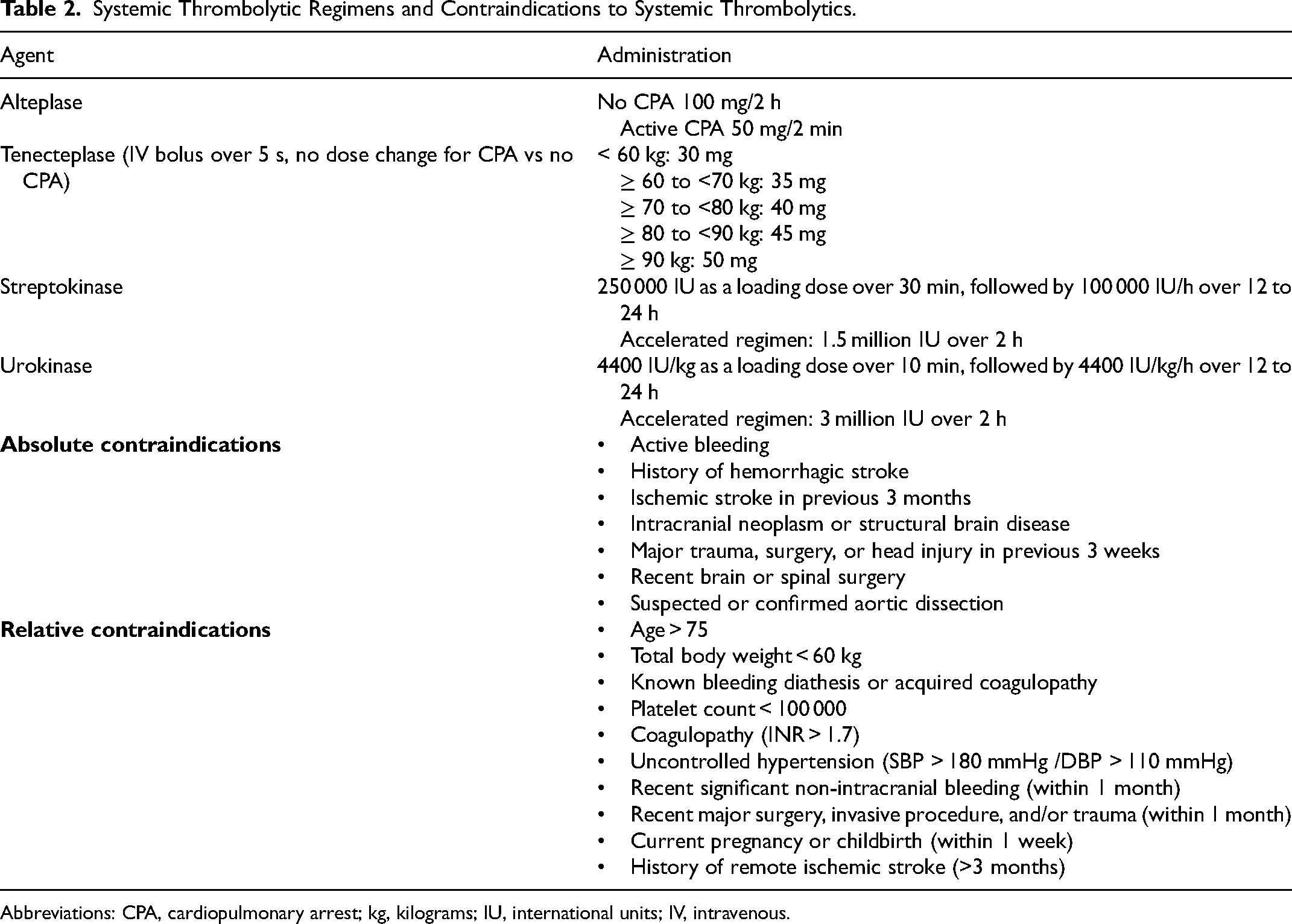
Abbreviations: CPA, cardiopulmonary arrest; kg, kilograms; IU, international units; IV, intravenous.
Percutaneous and Surgical Treatment Strategies
The 2 main percutaneous treatment strategies include CDE and CDT. Both CDE and CDT can be performed under local or moderate/conscious sedation and do not require general anesthesia unless indicated for another reason such as concomitant respiratory failure or cardiac arrest.
CDT is performed by the initial placement of small-bore catheters into the pulmonary arteries followed by the administration of low-dose continuous thrombolytics directly into the pulmonary circulation. The overall dose of thrombolytics is lower compared to suggested ST regimens; however, the duration of infusion is longer. There are different treatment protocols for CDT including the dose of alteplase which can vary between 8 and 24 mg for a duration of 4 to 24 h. 35 CDT can be combined with ultrasound assistance (USCDT) to enhance the effect of thrombolysis. 36 CDT has been shown to reduce pulmonary pressures and improve RV/LV ratios; however, this effect may not occur for some time depending on the intensity and length of the infusion protocol. For high-risk PE patients who are unstable, there is a need for rapid improvement in RV function than what CDT may offer. In addition, although the total dose of thrombolysis in USCDT is reduced compared to CDT, there is still a risk of bleeding. 35 Patients receiving CDT should be monitored for access site injuries such as hematoma, dissection and pseudoaneurysm, injury to the pulmonary vasculature, and systemic bleeding and coagulopathy in the setting of thrombolytic therapy. Each institution has their own protocols regarding the dose intensity and duration of CDT and the choice of anticoagulation regimen during and after the procedure. Commonly, a low-dose heparin infusion is continued during the procedure, followed by transition to full-dose anticoagulation post procedure (typically with heparin) prior to transitioning to long-term anticoagulation.
Modern CDE is performed by navigating a large-bore catheter device into the proximal pulmonary vasculature to aspirate encountered thrombi. CDE has mainly been studied for intermediate-risk PE; however, multiple single-center experiences describing its use in high-risk PE have been associated with improved outcomes compared to historical cohorts. The benefits of CDE include its rapid removal of thrombi compared to CDT or ST and complete avoidance of thrombolysis, and it also allows for reinfusion of aspirated blood to minimize procedural-related total blood volume loss. CDE does require large-bore access which may be associated with vascular access site injury; however, data from the FlowTriever Pulmonary Embolectomy Clinical Study (FLARE) and FlowTriever All-Comer Registry for Patient Safety and Hemodynamics (FLASH) studies as well as single-center experience with CDE demonstrated minimal vascular access site, bleeding complications, or pulmonary vascular injury.33,37–39 Due to its large-bore catheter size, most CDE procedures require administration of anticoagulation during the procedure itself, often using point-of-care labs to target an activated clotting time (ACT) of 200 s. Post-operative patients are usually maintained on therapeutic anticoagulation with heparin prior to transitioning to long-term anticoagulation. The recently completed FlowTriever for Acute Massive PE Trial (FLAME, Clinical Trials NCT04795167) was a prospective, multicenter, non-randomized, parallel, observation study that assessed the use of FlowTriever (a form of CDE) compared to other non-FlowTriever therapies for the treatment of high-risk PE. The trial was stopped early after a pre-specified interim analysis revealed a significant reduction in the primary composite outcome (all-cause mortality, bail-out to alternative treatment, bleeding, or clinical deterioration) in favor of treatment with FlowTriever. The full publication of this trial is still in process, but the preliminary data seems to support that a rapid percutaneous approach for high-risk PE may be feasible with improved outcomes compared to other alternative reperfusion therapies.
SPE is performed while a patient is on cardiopulmonary bypass, under general anesthesia, and is performed with induced cardiac arrest and aortic cross-clamping. 10 SPE has historically been reserved for patients who have failed other reperfusion therapies, have RHT, or have contraindications to certain therapies (eg, high bleed risk with ST). With the advancement of surgical techniques and perioperative practices, mortality with SPE has improved compared to historical SPE data. 10 Although SPE is invasive, it allows for immediate removal of proximal thrombi and is associated with improvement in RV function. 10 Limitations to SPE include the need for an experienced surgical team and for general anesthesia, and it is more invasive compared to CDE. Complications of SPE include bleeding complications, failure to wean from bypass, cardiac tamponade, pulmonary artery, injury and sternal wound infection. 40
MCS should be considered in patients with high-risk PE, especially for those who remain unstable despite the use of vasopressors. 41 MCS options consists of VA-ECMO or right ventricular assist devices (RVAD) with the goal to support cardiac output to physiologic or near-physiologic levels. VA-ECMO is typically achieved through peripheral cannulation of the femoral vein and artery. A pump is used to pull blood from the venous circulation through the inflow cannula, subsequently passed through an oxygenator, and returned to the patient through an outflow cannula via the femoral artery. Although other configurations for VA-ECMO exist (eg, from the femoral vein to the subclavian artery or centrally via the aorta), the relative ease of access via the femoral artery and vein makes it the preferred choice in high acuity clinical scenarios. 42 VA-ECMO allows for bypass of the pathologic abnormality (ie, thrombi in the pulmonary artery). VA-ECMO monotherapy with anticoagulation may provide sufficient RV support and treatment of the PE. More commonly, VA-ECMO is performed in combination with either CDE or SPE and data supports improved outcomes with a combined approach compared to VA-ECMO monotherapy. 43 VA-ECMO can also be used to stabilize patients prior to performing CDE or SPE, allowing for these procedures to be performed in a safe and controlled fashion, and if needed permits the safe transfer of patients to a tertiary or quaternary referral center for further advanced care. 44 Note that venous–venous ECMO does not have a role in the hemodynamically unstable patient but may be considered in patients who have refractory hypoxemia without shock. There are no randomized controlled trials for VA-ECMO and high-risk PE. Most of the data comes from case-series, retrospective data, and meta-analysis with a wide range (45%-95%) of reported survival, with an average ECMO run time of 4 to 6 days.45,46 Alternatively, a percutaneous RVAD can be considered to augment RV function. These devices augment cardiac output by drawing blood from the IVC and delivering it to the pulmonary artery. Several systems, including the Impella RP and the TandemHeart Protek Duo, exist today.47,48 However, there are several drawbacks to the use of an RVAD over VA-ECMO. First, because RV function is augmented via flow through the pulmonary vessels, RV afterload is increased. Second, RVADs are typically placed under fluoroscopy, limiting their use in high acuity scenarios. Finally, there is less data and typically less clinical experience in their use, in comparison to VA-ECMO. 10
Patients on ECMO require additional monitoring by an intensivist compared to patients not requiring ECMO. The ECMO circuit should be inspected thoroughly on a routine basis. Care should be given to the appearance of the circuit, and any loose connections and kinks must be resolved immediately. Deposition of fibrin strands in the cannulae or fibrin clots in the oxygenator should be noted, as a sign of inadequate anticoagulation or as a sign of prolonged duration of ECMO support. The pump flow rate, pump RPM, and transmembrane pressure gradient (ΔP) along with the arterial and venous side pressures should be noted. Pump flow rates should always rest above 2 L/min, although most adults who have not had meaningful recovery of native cardiac output will require closer to 3.5 to 5 L/min of flow. Arterial and venous pressures should be noted, as high negative pressures on the venous side increase the likelihood of unstable flow, hemodynamic instability, and air entrainment, whereas high arterial pressures can result in increased rates of hemolysis. The pump RPM, in combination with the measured flow rate, can give the bedside clinician an idea of trends in peripheral vascular resistance. Changes in ΔP above 20 mmHg should be noted, as it can portend pump failure. 49 In patients on peripheral VA-ECMO, it is possible for the patient to become hypoxemic despite appropriate oxygenator and pump function, due to the retrograde nature of VA-ECMO perfusion. This occurs because the patient's native cardiac output relies on the adequate function of native pulmonary gas exchange to oxygenate the blood. When native cardiac output outstrips the capacity for native pulmonary gas exchange, proximal blood can be deoxygenated, while peripheral perfusion is oxygen rich. This phenomenon is referred to as the Harlequin or North–South syndrome and can be identified by monitoring oxygenation at the most proximal takeoff from the aorta (ie, the right upper extremity), via pulse oximetry and serial blood gases. 42 In addition, particular care should be paid to serial neurologic exams for patients on VA-ECMO, as these patients are at high risk of embolic stroke. Patients on ECMO require anticoagulation which is discussed in more detail below.
CDT, CDE, and SPE require a patient to be stable enough to transfer to a procedure room for the planned intervention and stable enough to await appropriate personnel to complete the procedure safely. Some patients will be too unstable for transfer, have continued deterioration while waiting their treatment, or be too unstable to tolerate an advanced procedure safely. In these patients, the decision to proceed with VA-ECMO or ST should be considered to prevent additional hemodynamic compromise from progressive RV failure and to prevent circulatory arrest. VA-ECMO or ST monotherapy may lead to improvement in hemodynamics; for those patients without improvement or evidence of progressive shock, CDE or SPE can still be considered after either initiation of VA-ECMO or post ST. An outline for a possible approach to initiation of VA-ECMO for high-risk PE was published by Carroll et al, where the authors suggest for patients who have catastrophic PE, to proceed with ECMO if it can be initiated within 30 min, followed by evaluation for CDT or SPE. 5 In cases where ECMO cannot be initiated within 30 min, or in centers without ECMO capability, ST should be administered if no contraindications, followed by evaluation for ECMO, CDT, or SPE if there is no clinical or hemodynamic improvement after initial ST. We propose a similar treatment approach based on the high-risk PE subclassification (stable, unstable, or catastrophic) as can be seen in Figure 2.
Some patients may fail to improve or deteriorate during attempts at reperfusion with ST, CDE, or SPE. For these patients, VA-ECMO could be considered as a rescue therapy or as a bridge to an alternative reperfusion strategy, although earlier rather than later initiation of EMCO is associated with better outcomes. 50 Of note, although the risk of bleeding with ECMO cannulation increases post ST, it can still be completed safely, and ST should not be considered a contraindication to VA-ECMO. 46 Bleeding risks may be minimized by using ultrasound-guided cannulation for ECMO and by having the procedure completed by an experienced operator.
Anticoagulation of the High-Risk PE Patient
Anticoagulation is the cornerstone to the management of PE despite risk stratification, and all patients should be started on therapeutic anticoagulation if no contraindications. 51 There is minimal data to support if 1 anticoagulant is superior to another; however, heparin is often the agent of choice for high-risk PE as it allows for reliable monitoring of drug levels, has a short half-life, and can be reversed. 3 The presence of liver and kidney injury, both of which can be consequences of high-risk PE, can alter the pharmacokinetics of low molecular weight heparin (LMWH), direct oral anticoagulants (DOAC), and vitamin K antagonists (VKA), making these agents less attractive. 3 It is also important to be able to monitor the therapeutic effect of the anticoagulant which can be done routinely with heparin using partial thrombin time (PTT), factor Xa levels, or ACT. Other common anticoagulants (DOACs, VKA, and LMWH) may have less reliable measurements of blood levels. Heparin infusions can be easily stopped if additional procedures are required, and if there is a bleeding complication, heparin can be reversed with protamine sulfate. 52 For patients that have received ST, heparin is often resumed once the PTT is less than twice the upper normal limit often without a bolus to reduce bleeding events. 53 Patients requiring MCS also require continuous anticoagulation to prevent thrombosis of the support devices. In addition, MCS may lead to a consumptive thrombocytopenia and platelet levels should be monitored closely and potentially assessed for heparin-induced thrombocytopenia.54,55 For patients on VA-ECMO, bivalirudin may be an alternative first-line anticoagulation strategy as it functions as a direct thrombin inhibitor with a shorter half-life than heparin.56,57 Once patients clinically and hemodynamically improve from the high-risk PE, consideration of transition to alternative anticoagulation such as DOACs should be considered. 58
For patients who cannot tolerate anticoagulation or develop contraindications to anticoagulation, the placement of a retrievable inferior vena cava filter (rIVCF) should be considered. 58 The risks versus benefits of empiric rIVCF for all high-risk PE patients are outside of the scope of this review article.
Supportive Care
In addition to reperfusion and anticoagulation therapy, attention must be paid to the management of concomitant RV failure and supportive care. In some scenarios, despite treatment with reperfusion therapies, patients may continue to exhibit signs of RV failure either from partial recovery of RV function or from having other pre-existing etiologies of pulmonary hypertension (chronic left-sided heart failure and/or chronic lung disease); accordingly, careful attention to the unique physiology of RV failure is required.
Hemodynamics/Blood Pressure Goals
Blood pressure targets for PE are extrapolated from other shock physiologies, and there has been no clear consensus on targeting a specific blood pressure target in the high-risk PE patient. Therefore, the common blood pressure threshold of a mean arterial blood pressure of 65 mmHg and ensuring adequate perfusion for the individualized patient is often followed. It is important to note that hypotension will lead to worsening RV to coronary artery perfusion gradient and further increase demand ischemia of the already strained RV. Unlike the LV, the RV receives coronary perfusion during systole and diastole. 16 RV perfusion pressure is therefore driven by the difference between the systemic systolic and diastolic blood pressures and the RV systolic and diastolic pressures, respectively. Resuscitation should target increasing the systemic mean arterial pressure (MAP) while minimizing increases in RV pressures and central venous pressure (CVP) if possible, to ensure adequate coronary to RV perfusion gradient. 59 Treatment of hypotension is aimed at cautious and often minimal intravenous fluid administration given the risk of further worsening RV pressure and volume overload. 60 Therefore, the early use of vasopressors should be considered to support blood pressure and norepineprhine remains the vasopressor of choice. 60 There is a growing interest in the use of vasopressin for its unique properties to increase the systemic MAP without increasing PVR, but more data is still required before using this as a first-line agent. 61 Epinephrine can be considered as an adjunct to vasopressin because of its ability to provide additional inotropic effects; however, one should be aware of the potential tachycardic response and pro-arrhythmogenic effects with higher doses which can further worsen RV function. 62 Pure inotropes or inodilators such as dobutamine and milrinone may be considered if there is evidence of ongoing RV failure and shock, although these agents may lead to arterial hypotension if used without a vasopressor in addition to being pro-arrhythmogenic. Patients with ongoing clinical deterioration or those with escalating vasopressor or those multiple vasopressor requirements should be considered for possible MCS in the form of VA-ECMO. As detailed above, VA-ECMO can be used to rapidly decompress the RV and support systemic perfusion and oxygenation. The ECMO flow can be adjusted to provide RV support as needed and can be paired with vasopressors and inotropes as needed. Other MCS options may be of future interest for the management of RV failure in the setting of PE such as Impella RP or Protek Duo devices. 10
Given the severity of illness and complexity of these patients, the placement of central venous catheters with CVP monitoring and arterial line placement for systemic BP monitoring should be considered, although the placement of such devices should not delay resuscitation. Resuscitation can be guided by a number of different parameters such as clinical exam (capillary refill, mental status, and urine output), and laboratory data such as serum lactate as well as liver and renal function tests can serve as an assessment for systemic congestion of the RV and a measure of end-organ perfusion. 63 Echocardiographic data can provide insights into both LV and RV function and be used to evaluate for recovery after an intervention such as CDE, SPE, or titration of vasopressors and can be used to rule out other etiologies of shock. For patients with central venous catheters, in addition to CVP, a central venous oxygen saturation (CVO2) may be helpful with the assumption that lower CVO2 values in the setting of high-risk PE may indicate poor RV function. In some patients, especially those on MCS, a pulmonary artery catheter may be of benefit to obtain full hemodynamic assessments. 64
Inhaled pulmonary vasodilators may be considered for patients with high-risk PE who have persistent shock despite initiation of treatment with vasopressors. Inhaled pulmonary vasodilators can help reduce RV afterload and improve RV function by causing pulmonary artery vasodilation. Commonly used agents include inhaled nitric oxide and inhaled epoprostenol. Inhaled pulmonary vasodilators may also improve hypoxemia by improving perfusion to lung units that receive the most ventilation leading to improved VQ matching. Furthermore, by decreasing RV afterload, it allows for increased mixed venous oxygen content delivery to the pulmonary capillaries and helps reduce the intracardiac shunt fraction in patients with right to left intra-cardiac shunts, further improving systemic oxygenation. Although inhaled pulmonary vasodilators have been associated with improvement in oxygenation and RV function, there have been few studies specifically assessing its use in the high-risk PE cohort. It is likely that inhaled pulmonary vasodilators can be used as adjunct for care in high-risk PE patient's refractory to initial treatment or as a bridge to additional treatment strategies. 65
Oxygenation and Ventilation
Maintaining appropriate oxygenation is also important to prevent the hypoxic pulmonary vasoconstriction response which can increase the PVR. An oxygen saturation goal of >90% should be maintained to prevent the hypoxic pulmonary vasoconstriction response. Patients with high-risk PE and severe shock are also at risk for concomitant hypercarbic respiratory failure, and careful attention to ventilation and pH should be monitored. There are no clear pH or carbon dioxide goals for high-risk PE, but given the understanding that hypercapnic acidosis can increase PVR and reduce RV function, severe abnormalities should be avoided. 66 For patients with hypoxemia and hypercapnic acidosis, non-invasive support should be considered, if possible, prior to MV due to the potential deleterious effects of MV. 3 High-flow nasal cannula (HFNC) may be of benefit as it allows a significant higher flow of oxygen compared to conventional nasal cannula which can assist with reducing dead space and improved carbon dioxide clearance. 67 In patients with severe hypoxemia and or hypercapnic acidosis, non-invasive positive pressure ventilation can also be trialed; however, these patients need close monitoring due to the physiological effects of positive pressure ventilation which will be discussed in more detail below. Some patients will require MV for oxygenation and ventilatory support given the severity of their disease. MV carries multiple physiological consequences and is associated with a higher rate of complications in patients with underlying RV failure. 68 Intubation in the critically ill patient is often achieved by rapid sequence intubation (RSI) combining an induction agent and neuromuscular blockade (NMB). The use of RSI and sedation required post-intubation may lead to vasoplegia and loss of underlying sympathetic tone leading to abrupt circulatory collapse. Certain induction agents such as propofol may be associated with more hemodynamic instability and should be avoided. More hemodynamically neutral induction agents such as ketamine or etomidate should be considered instead. 69 Although NMB does not directly cause vasoplegia, its use may be associated with loss of sympathetic drive-in high catecholamine states such as severe shock. Alternatively, topical anesthesia and awake intubation may be considered to avoid the potential hemodynamic consequences of RSI. 70 Agents used for post-intubation sedation should ideally also be hemodynamically neutral.
The peri-intubation and transition to positive pressure ventilation has important physiological consequences. The intubation process itself may exacerbate hypoxemia and hypercarbia with the potential loss of minute ventilation following RSI and the time taken to establish the advanced airway with an endotracheal tube. Intubation should be completed by an experienced operator to maximize attempts at first-pass success and time to endotracheal tube placement to prevent additional hypoxemia and hypercarbia. 71 Positive pressure ventilation leads to increased intra-thoracic pressure translating to both reduced venous return and increased RV afterload. In addition to the placement of the endotracheal tube, appropriate tidal volume, positive end expiatory pressure (PEEP), and airway pressures need to be selected and closely monitored. Insufficient tidal volumes may lead to worsening atelectasis leading to alveolar hypoxia and hypercarbia. On the other hand, excessive tidal volumes can contribute to increased airway pressures, barotrauma, and alveolar distension leading to compression of alveolar vessels and increased PVR. 66 PEEP should be titrated to assist with hypoxemia, but excessive titration should be avoided, as excessive PEEP can contribute to increased intra-thoracic pressures which in turn can decrease RV preload and increase RV afterload. Targeting an oxygen saturation of 90% or greater and normocapnia and preventing severe acidosis (pH < 7.30) while maintaining a plateau pressure of <30 mmHg and using safe tidal volumes 6 to 8 cc/kg of ideal body weight can prevent further RV decompensation. 3
Although there are risks involved with positive pressure ventilation and MV, if indicated, the procedure should not be delayed as the risks of ongoing hypoxemia and hypercapnic acidosis outweigh the risks of MV. Several steps can be taken to minimize the risks of MV including using hemodynamically neutral induction agents; having adequate vasopressors initiated prior to intubation; initiating inhaled pulmonary vasodilators during the peri-intubation period; using continuous capnography to rapidly confirm endotracheal tube placement; avoiding hypoxemia with appropriate pre- and peri-intubation oxygenation; avoidance of large tidal volumes, PEEP, and airway pressures; and consideration for awake intubation. Given the high association of circulatory collapse in patients with shock secondary to acute RV failure, an arterial line and definitive intravenous access for vasopressors should be considered. In centers that have the capability for VA-ECMO, pre-intubation ECMO or obtaining appropriate arterial and venous access for rapid ECMO initiation can be considered prior to intubation.
Cardiac Arrest
Patients with high-risk PE may deteriorate and have a cardiac arrest event or present as a cardiac arrest event. For patients with suspected or confirmed high-risk PE who are suffering a cardiac arrest, adjunctive therapy to advanced cardiac life support should be considered. ST for PE-related cardiac arrest has been associated with improved return of spontaneous circulation (ROSC) and survival. 72 Patients who do not have absolute contraindications should receive ST as early as possible in attempt to ROSC. High-quality chest compressions with minimal interruptions should be performed to help circulate the ST, and the duration of resuscitation post ST administration varies from at least 15 min to 90 min to ensure adequate circulation of the ST agent. 73 Patients should be assessed for extracorporeal cardiopulmonary resuscitation (ECPR) if available as this adjunct has been shown to improve outcomes in PE-related cardiac arrest. 74 As mentioned above, prior use of ST is not a contraindication to ECMO or ECPR. Appropriate post-arrest management should be undertaken to help improve neurological outcomes post arrest. Targeted temperature control is a common practice post arrest. Of note, ST is not a contraindication to targeted temperature management.
Given the high mortality rate of high-risk PE, along with the complexity of the disease with the need for advanced treatments and monitoring (CDE, SPE, and ECMO), patients with high-risk PE should be transferred to an experienced center that has the ability to offer these advanced treatments. 75 Even patients who have already received ST should be considered for transfer as some patients will fail to improve with ST monotherapy and may be considered for additional advanced therapies. The treatment of high-risk PE patients transcends multiple specialties, and therefore, multidisciplinary discussion is important to optimize care for such patients. PE response teams (PERTs) if available should be involved in such a patients care. PERTs and hospitals that have a higher volume of PE cases are associated with improved outcomes for these patients.76–78
Right-Heart Thrombi
RHT is estimated to be present in 2% to 5% of all PE cases with greater incidence in patients who have more severe PE on presentation and has been associated with a higher risk of mortality than those without RHT.14,79 RHT is a broad term that encompasses either immobile or mobile thrombi in any part of the right atrium (RA), RV, or in the proximal inferior vena cava (IVC). 14 Treatment of the high-risk PE patient with underlying RHT is considered a medical emergency as RHT have the potential to embolize into the pulmonary circulation leading to further increases in PVR and hemodynamic collapse and/or lead to a paradoxical embolism if there is an underlying right to left shunt present. Treatment should be aimed at supporting the underlying hemodynamics, addressing the RHT to prevent additional acute PE, and alleviating the pulmonary thrombi burden to reduce RV afterload. 14 Similar to high-risk PE without RHT, patients with high-risk PE and RHT can be considered for a combination of ST, CDE, surgical approaches, and VA-ECMO depending on the resources and expertise available at the treatment center. 14 ST may be used as the initial therapy to treat both the RHT and PE for those who are unstable or at centers without access to CDE or surgical therapies. Patients who receive ST should be re-evaluated for adjunctive therapy with CDE, SPE, or VA-ECMO for those who have persistent RHT or evidence of persistent shock following initial ST. 14 If available, CDE allows for a minimally invasive approach for simultaneous treatment of both RHT and PE. 14 Careful attention is required to not embolize the RHT while navigating CDE devices near the RHT. The use of intracardiac echocardiography or TEE can assist in preventing this complication. Surgical embolectomy combined with SPE can be used to treat both RHT and PE but is the most invasive approach and requires general anesthesia and an experienced surgical team. Surgical therapy may be best suited for patients who have a large amount of RHT, RHT trapped across a right to left shunt, RHT associated with intracardiac devices, or concern for underlying cardiac tumors. 14 Similar for treatment of high-risk PE without RHT, VA-ECMO monotherapy with anticoagulation or VA-ECMO performed with either CDE or SPE can be used for patients with high-risk PE with RHT. 14 One should pay careful attention to possible thrombosis of the venous cannula or ECMO circuit which may occur if the venous cannula drains the RHT.
Proposed Algorithm for High-Risk PE
We propose that patients who are diagnosed with high-risk PE should be immediately sub-classified into 1 of 3 categories corresponding to increasing severity: stable, unstable, or catastrophic (Table 1). Stable patients are those who are not requiring vasopressors or those who are on a single, stable, low-dose vasopressor (0.25 mcg/kg/min of norepinephrine or equivalent). Unstable patients are defined as those who require more than 1 vasopressor, continuous escalation of a single vasopressor (ie, cannot achieve a stable infusion for > 30 min), need for intubation or those with evidence of worsening perfusion or symptoms (depressed mental status, increasing lactate, recurrent syncope, etc) or evidence of RHT. Catastrophic patients are those who are in a near, active, or post cardiac arrest. Sub-classifying high-risk patients allows one to better match the intensity of treatment to the severity of presenting disease (Figure 2). Patients with stable disease could be evaluated for rapid CDE (if available and can be performed in a reasonable amount of time [< 90 min]) as an alternative to ST. If CDE is not available, ST should be considered if there are no contraindications. Patients with unstable disease should be screened for VA-ECMO as a bridge to either CDE or SPE. If VA-ECMO cannot be completed rapidly (< 30 min), patients should receive ST if there are no contraindications. These patients should also be re-evaluated for possible ECMO, CDE, or SPE if there has been no clinical improvement. For catastrophic PE patients, treatment with ST +/− ECPR if available should be considered with additional evaluation for adjunctive CDE or SPE depending on clinical stability. Given the risk of deterioration, need for vasopressors, and potential advanced therapies, unstable and catastrophic PE categories should be considered for early definitive access and hemodynamic monitoring with central venous catheter and arterial line placement. Patients being considered for VA-ECMO should have arterial line placement in the right upper extremity, if possible, to better assess for oxygenation and the potential development of North–South syndrome. For all high-risk PE categories, target a MAP > 65 mmHg and ensure adequate end-organ perfusion, early initiation of vasopressors, and evaluation for MCS if unable to achieve this. All high-risk PE patients should have an oxygen saturation > 90% and normocapnia and target a pH > 7.30. If MV is required, taking precautionary steps as noted above is important to prevent additional deterioration during the peri-intubation period. Patients should be considered for transfer to a hospital that has experience with MCS, CDE, and SPE.
Conclusions and Future Considerations
Although high-risk PE continues to carry a high mortality rate, there is considerable effort to improve outcomes for these patients. Emerging therapeutic options such as early CDE, SPE, and MCS with or without ST may help improve high-risk PE outcomes. Regardless of which reperfusion or combination of reperfusion therapy that is performed, excellent critical care medicine regarding resuscitation, ventilation, oxygenation, and sedation can help assist RV recovery, mitigate multi-organ dysfunction, and improve outcomes in high-risk PE patients. Transfer to advanced centers, multidisciplinary discussion, and utilization of PERTs may also improve care for these patients. Additional studies are needed to help determine the optimal therapy or combination of therapies, optimal time to reperfusion therapy, and additional risk stratification to help match the intensity of treatment to the corresponding disease severity in high-risk PE. With such advancements, the future outcomes for high-risk PE appear promising.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.