
Abstract
Introduction
Parents of children in the pediatric intensive care unit (PICU) experience substantial stress; a parent's perception of their child's illness severity, more than objective measures, predicts psychological outcomes. No tools exist to assess parents’ real-time experiences. This pilot study evaluated the feasibility and acceptability of a text-based tool to measure parental experience.
Methods
Inclusion criteria included PICU stay >48 h, physician approval, smartphone access, and English-speaking caregiver. Eligible parents received a text-based baseline survey and surveys every other day while hospitalized regarding their mood/experiences and optional open-ended questions regarding stressors. They received post-discharge follow-up surveys at 1 week and 1, 3, and 6 months. Follow-up surveys assessed mood and symptoms of depression, anxiety, and post-traumatic stress. Interviews and surveys about the interface were conducted 1 week and 3 months following discharge. Feasibility was assessed by descriptive statistics (eg, response rates), and acceptability was assessed by descriptive statistics (survey results) and thematic analyses of interviews.
Results
Of 20 enrolled participants, the first 5 were excluded due to technical issues. Of the 15 included, results demonstrated feasibility and acceptability. Most participants (86%) completed all surveys during the PICU stay and continued to complete surveys at a high rate: 79%–94% 3 months post-discharge. All participants agreed that the system was easy to use and were satisfied with the system at discharge, and 91% remained satisfied 3 months post-discharge. Additionally, 76% reported comfort, and 69% reported benefit. From the interviews, participants lauded the system's convenience and applicability of content. Some proposed changes to improve ergonomics. Many suggested this interface could help teams better support families.
Conclusions
A text-based interface for measuring experience in the PICU is feasible and acceptable to parents. Further research can explore how this could identify parents most at risk of adverse psychological sequelae and lead to earlier supportive interventions.
Keywords
Introduction
Children and families treated in the pediatric intensive care unit (PICU) are exposed to stressful experiences.1-4 For many parents, these experiences endure past their child's hospitalization and result in substantial psychological morbidity. Multiple studies suggest that a parent's perception of their child's illness, more than illness severity, impacts psychological outcomes.5-8 Currently, there are no tools to assess parents’ subjective experiences and perceptions in, or near, real time. Such a tool could improve our ability to identify and respond to distress, better supporting parents through the challenges of having a critically ill child. This pilot study explores whether a text messaging platform is a feasible and acceptable way to understand the development of distress and psychological morbidity among parents of PICU patients.
The distress impacting parents of PICU patients is substantial and enduring. In a review by Nelson and Gold, up to 21% of parents with critically ill children met diagnostic criteria for post-traumatic stress disorder (PTSD), and 84% reported symptoms of PTSD after discharge. 9 However, not every parent who undergoes acute stress during their child's hospitalization has lasting psychological sequelae. 10 Multiple studies suggest that one's post-traumatic trajectory is highly influenced by an individual's subjective appraisal of real-time events.6,10,11
The PICU environment makes it difficult to assess a parent's experience and their likelihood of long-term sequelae. Mental health resources are finite, and providers often rely on severity of illness to allocate these resources.12-14 However, illness severity is less predictive than a parent's experiences: fear that one's child might die is more predictive of PTSD than the child's severity of illness.6,7,10,11,15 Moreover, individuals manifest distress differently. Less conspicuous distress may be masked by the high medical and psychosocial acuity in the PICU. Further, parents are heavily taxed while attending to their critically ill child and may not have the bandwidth to participate in interviews or other research procedures. Perhaps for this reason, few studies exist which ask parents to complete surveys during their child's PICU stay, and we did not encounter any studies which asked parents to complete surveys on a repeated measures basis while their child was in the PICU. Even in the acute care setting, recruiting parents for research while one's child is hospitalized presents a challenge for researchers. 16 In a study of parents’ post-traumatic stress symptom trajectories performed in Australia, out of 311 eligible families who were approached, parents from 122 families completed at least 3 of the 4 surveys (39.2%), and only 1 of these time points was during the child's inpatient stay. 17 Surveys were presented in paper—either in person or by mail—and participants included parents of patients in acute care and in the PICU. It stands to reason that recruitment and retention of participants could be more challenging in a higher acuity setting such as the PICU and especially difficult when multiple surveys are performed at multiple time points across a PICU stay.
Text messaging is becoming a convenient and accepted way to communicate with patients and families during and after healthcare encounters.18-22 It is convenient and may bypass some limitations of retrospective methods, such as recall bias. Research from other settings supports its potential convenience to parents23-25 and its potential to help parents feel more supported by their child's medical teams. 26 However, parents’ experiences in the PICU differ meaningfully from those of parents in the community. Parents of PICU patients consistently report substantial psychosocial stressors while their child is hospitalized.7,8,27-30 And while research can present opportunities, parents also report that it can present burdens by asking potential participants for their time amid this already busy and chaotic experience. 31 Moreover, the burdens are likely not equally distributed across a population. Families from minoritized populations and/or of low incomes are disproportionately burdened and therefore often consent for research at lower rates. 32 For these reasons, it is important to determine the feasibility and acceptability of this data collection method specifically within the PICU environment.
At present, there are no tools to assess parents’ subjective experiences and perceptions in, or near, real time. As stated, such a tool would allow providers to identify parents with high levels of distress and respond earlier in its course. This pilot study seeks to ascertain the feasibility (defined by response rates) and acceptability (by parental survey responses and interviews) of a text message–based interface to measure the real-time experiences of PICU patients’ parents. If feasible and acceptable, this may allow for earlier identification of parental stress and perhaps of those most at risk of further psychological sequelae. This could, in turn, allow for earlier allocation of resources to those most in need to reduce psychological morbidity in those most at risk.
Materials and Methods
Positionality
The research team was comprised of physicians (critical care, palliative care, and complex care), psychologists, psychology graduate students, a nurse practitioner, and a research associate across 2 institutions and was comprised of a wide variety of backgrounds and experiences. Individual positionality statements are available in Appendix A.
Study Design
This is a prospective, observational study designed to determine the feasibility and acceptability of a text message–based data collection survey, approved by the Institutional Review Board at a participating institution (#1541760).
Study Environment
The study environment is a single PICU in a free-standing children's hospital in a major metropolitan area, with a total of 72 PICU beds divided into cardiac (24) and non-cardiac (48).
Study Participants
Parents of non-cardiac ICU patients with anticipated PICU length of stay (LOS) of at least 48 h from the time of consent were eligible. Exclusion criteria were inability to complete study materials in English, lack of a device with internet access, or lack of permission by the child's PICU attending physician to approach.
Study Procedures
Eligible participants were introduced to the study by a member of the research team. If they agreed to participate, participants were shown a video with instructions for enrollment of their personal device by inputting their preferred name and phone number, as well as preferences for the timing of surveys. They received the initial enrollment survey on a personal device, which they completed with the study team present to answer questions. Text messages were sent via the Qualtrics 33 interface and included links to surveys and mental health resources, as well as a statement that responses were not reviewed during study. Surveys were administered during and post-hospitalization according to the contents and timeline described under “Survey Contents” below.
Participants received a text message 1 week post-discharge with a link to a survey to complete and were called to schedule a virtual interview regarding the acceptability of study procedures. An additional survey and interview were performed at 3 months to glean participants’ perspectives with an emphasis on the post-discharge portions.
Participants received $25 after the completion of the 1-week interview and survey and an additional $50 after survey and interview completion at 3 months post-discharge.
Study Outcome Measures
Primary Outcomes
Feasibility. Feasibility was assessed by assessing survey completion rates among participants, with feasibility defined as a response rate of >70%, which was deemed to be a high goal based on other comparable pilot studies.19,34 Other feasibility measures included the completion percentage of surveys once started and times to complete surveys.
Acceptability. Acceptability of the interface was assessed via a mixed methods approach, with all participants invited to complete an acceptability survey and a semi-structured interview at 1 week and 3 months post-discharge. Acceptability was defined as >70% of respondents endorsing their support of the tool by survey questions and <30% of respondents endorsing the negative items, for example, that the survey was overly intrusive or burdensome. Qualitative themes were analyzed in order to support or refute the acceptability of the tool.
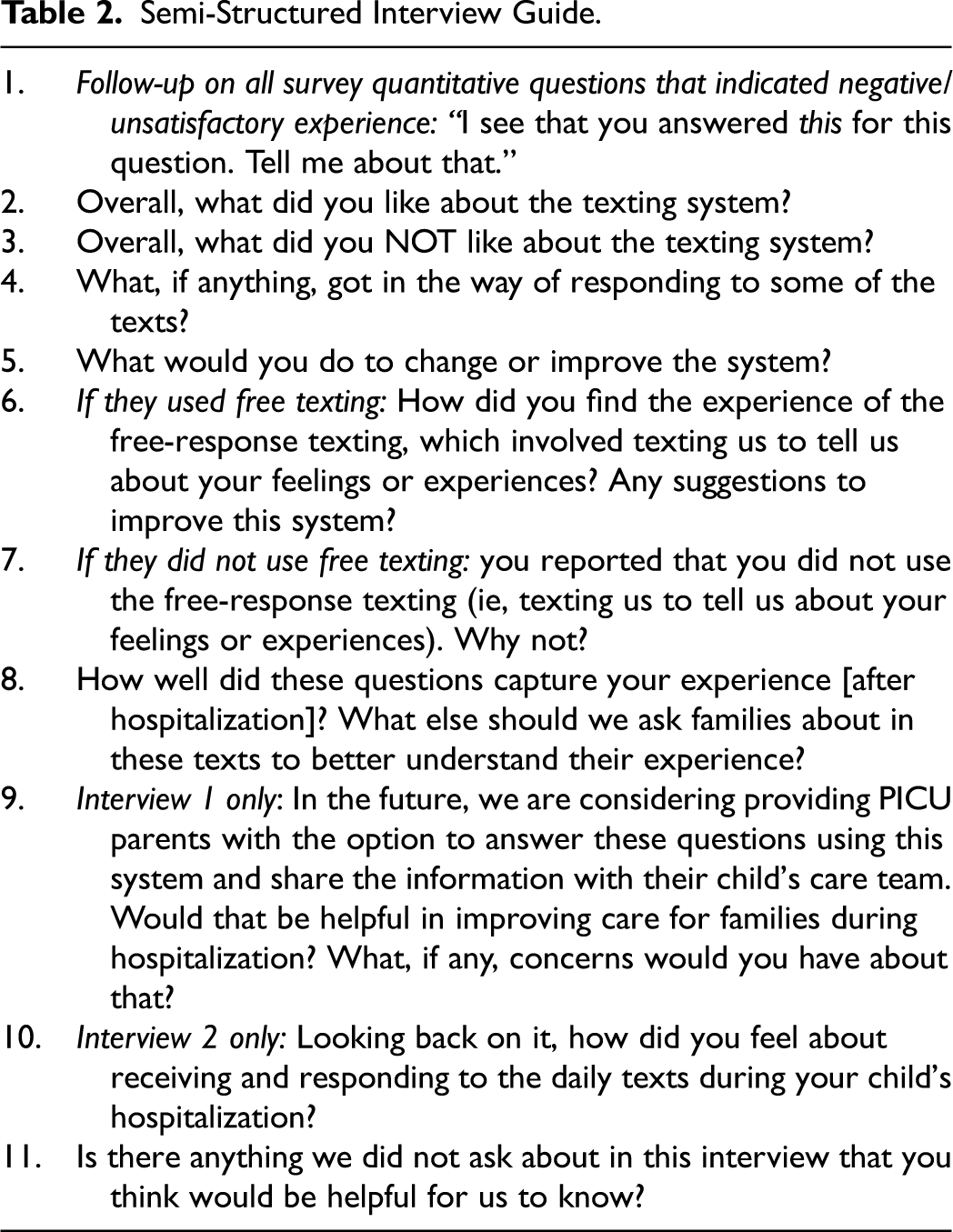
The Likert scale items were adapted from the Telehealth Usability Questionnaire (TUQ), developed by Parmanto and colleagues to assess reliability, validity, acceptability, and practicality of their SMS interface. 35 This interface has previously been used for a telehealth intervention evaluating mood-related symptoms after traumatic brain injury by Dr Juengst and colleagues. 36 For the present study, the general domains of usefulness, ease of use, interface quality, interaction quality, reliability, and satisfaction from the TUQ were utilized; however, the specific questions were modified to the particulars of this specific interface and the specific challenges of the PICU environment. Acceptability survey questions are provided in Table 1. Semi-structured interviews followed an interview guide devised by experts in psychology, critical care, complex care, and online assessment technologies (see Table 2). Participants completed the survey via Qualtrics, 33 then were interviewed to follow up on survey answers and provide more information about their experiences. Interviews were performed via Microsoft Teams, 37 then professionally transcribed with identifiers removed.
Acceptability Survey Results at Day 7 (D7; n = 13) and 3 Months (M3; n = 11) Post-Discharge.
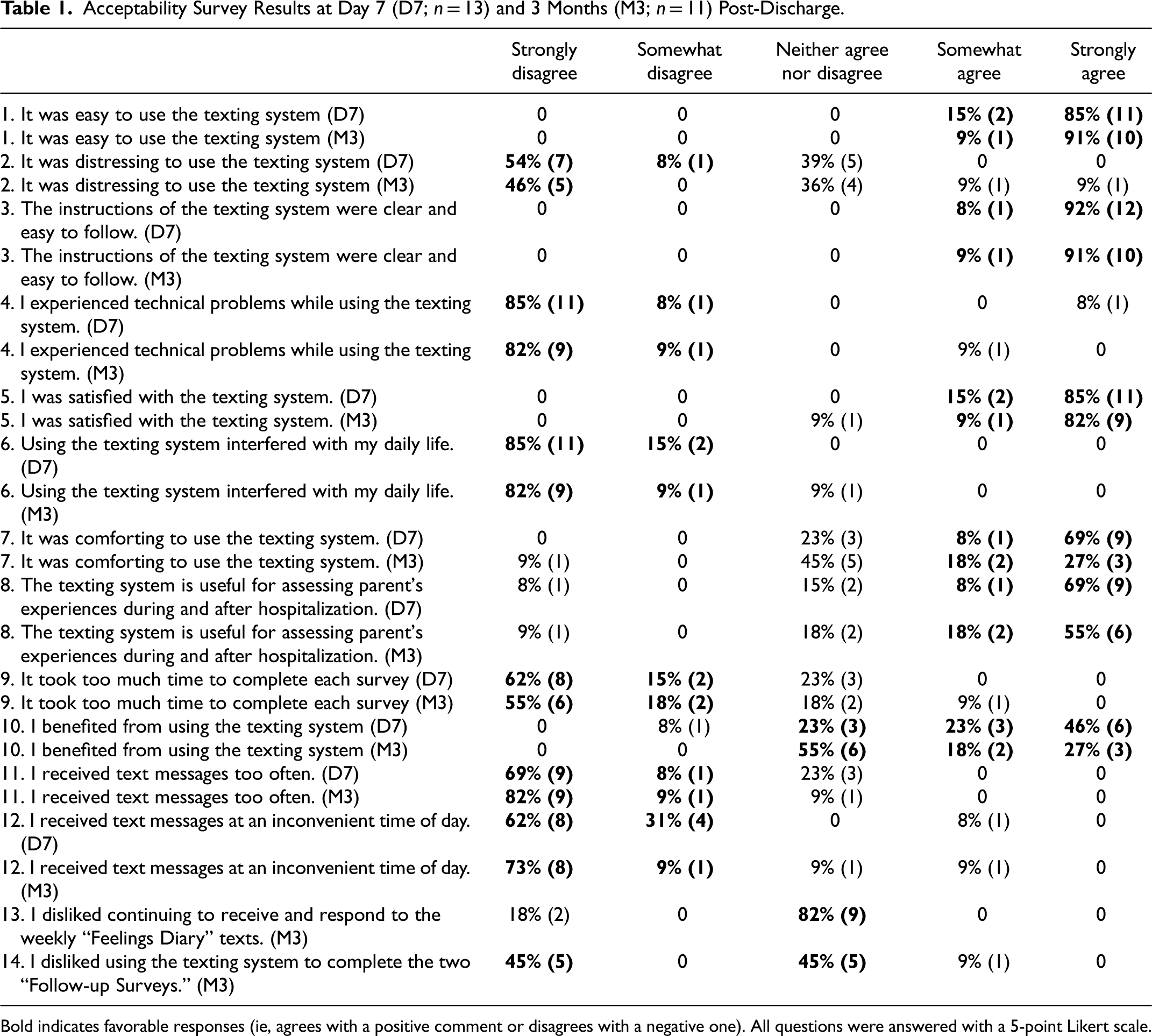
Bold indicates favorable responses (ie, agrees with a positive comment or disagrees with a negative one). All questions were answered with a 5-point Likert scale.
Semi-Structured Interview Guide.
Survey Contents
The content of surveys is described below and in Table 3. These surveys were intended to lay the groundwork for subsequent study of this texting interface; they were not, however, intended to be analyzed in this pilot based on a small sample size.
Contents of Surveys for Each Phase.
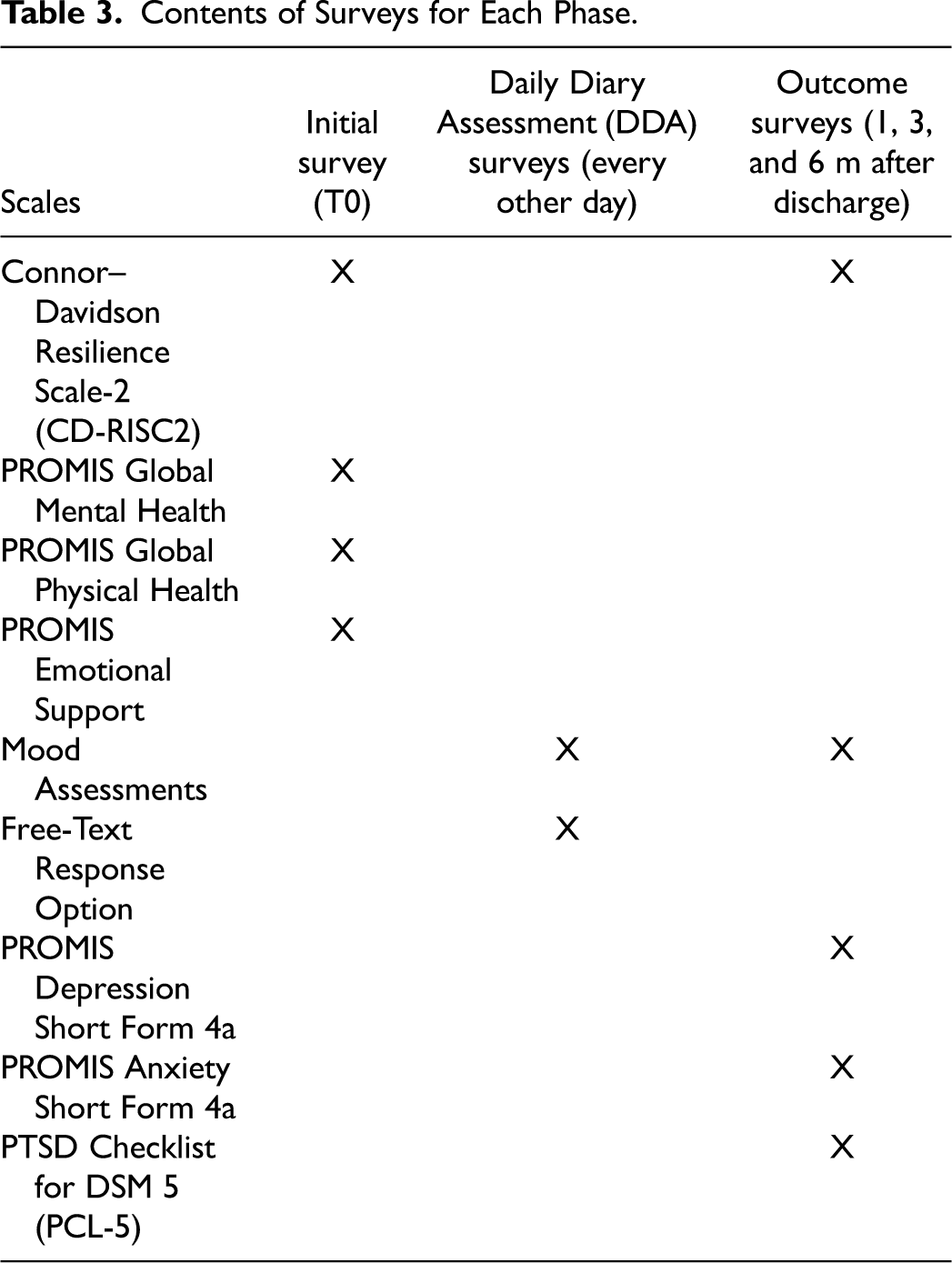
Surveys were selected by the study team, consisting of multiple critical care physicians and psychologists with expertise in both clinical care and research. The surveys were selected to include measures that have known associations with depression, anxiety, and PTSD after PICU stay (mental health, physical health, emotional support, and resilience)7,37,38 and a novel measure to assess participants’ real-time emotional experiences. The latter is based on the established association between parents’ subjective experiences and their risk of experiencing PTSD after medical events.7,10,11
Baseline Survey
The baseline survey was administered to participants at the time of consent. This survey consisted of the following tools: Patient-Reported Outcomes Measurement Information System (PROMIS) Global Mental Health-2, 38 PROMIS Global Physical Health-2, 38 PROMIS Emotional Support 4a, and Connor–Davidson Resilience Scale—2-item version (CD-RISC2). 39 To assure participant confidentiality, neither demographic nor illness-related data were collected on participants nor children. These datapoints were nonessential to the goals of determining feasibility and acceptability of the tool. LOS data was determined from the time of enrollment and collected via participants’ self-report via every-other-day surveys.
Daily Diary Assessments
This survey was issued every other day while hospitalized and for 1 week post-discharge and consisted of mood assessments, an assessment of the child's status, and the opportunity to provide additional information on their experiences and stressors via free text. Mood assessments asked participants to identify with 20 adjectives (10 positive and 10 negative) on a 0–10 scale. With respect to the assessment of a child's status, participants reported their child's disposition (hospital vs discharged). In our sample, discharged patients only went home (vs transfer to another healthcare facility, such as acute rehab or skilled nursing facilities). This allowed participants to be moved into the “post-discharge” cohort without collecting identifying information or accessing medical records.
Outcome Surveys
These surveys, administered at 1, 3, and 6 months post-discharge, consisted of the following tools: mood assessments, CD-RISC2, PROMIS Depression Short Form 4a, PROMIS Anxiety Short Form 4a, and Post-traumatic Stress Disorder Checklist for DSM5 (PCL-5). 40 These outcomes were chosen as they are mental health outcomes which are known to be associated with one's loved one's serious or critical illness.
Data Analysis
Descriptive statistics were utilized to evaluate feasibility (eg, response rates) and acceptability (eg, acceptability, Likert scale survey). As this pilot study was designed with a small sample explicitly to assess feasibility and acceptability, we only analyzed data relevant to the feasibility/acceptability of the interface. Therefore, the content of the mood assessments and outcome surveys was not analyzed.
Responses to the optional open-ended qualitative question were analyzed using modified Delphi coding 41 by constructing themes in a structured, iterative manner. A total of 5 study team members independently reviewed all responses to each question and generated preliminary themes. Themes were discussed and finalized. Each response was then independently coded for the presence or absence of each theme using Microsoft Excel. 42 Codes were compiled and compared across study team members. Items without satisfactory agreement (ie, 80%) were collectively discussed to consensus.
To analyze responses to the qualitative interview questions, transcripts were coded using reflexive thematic analysis. 43 An inductive approach was used given the exploratory nature of the study; 3 investigators reviewed all transcripts to independently generate initial codes until the final codebook was created; 2 investigators then applied a codebook to all transcripts. Disagreements were discussed to 100% consensus. Next, codes were collated and reviewed by 2 investigators to independently identify latent themes (ie, underlying ideas, assumptions, and conceptualizations). Themes were discussed with the third investigator present to resolve disagreements. The first round of interviews was coded using this approach, and then, the codebook from the first round was applied to the second round of interviews. Evaluation of data saturation to determine sample size and quantification of themes are inconsistent with reflexive thematic analysis and therefore were not utilized for this portion of the data.
Results
Participant Data
As discussed in the Methods section, demographic information was largely not collected for this pilot. Median enrolled LOS was 5 days, with interquartile range of 2–6 days. Enrolled LOS ranged between 1 and 60 days in total.
Feasibility of Texting System
Participation Rates
A total of 397 patients were screened, and 41 families were eligible. Of eligible families, 15 were unavailable for the study team approach, 6 declined participation due to time concerns, and 20 families enrolled. The majority who were ineligible had an anticipated LOS less than 48 h or were non-English-speaking. In total, 44 were deemed ineligible by PICU attending physicians due to the child being at end of life, social concerns, and legal guardianship issues. The first 5 enrolled participants experienced technical difficulties related to internet connectivity and text message length limitations, which were subsequently resolved; 4 were excluded from all analyses since they were unable to complete the surveys; 1 was only able to complete the baseline survey, so they were included in baseline analyses but excluded from additional assessments. Another participant voluntarily unenrolled after their first hospital Daily Diary Assessment (DDA) survey; they were therefore included in baseline analyses but excluded from other analyses; 1 participant was excluded at month 6 when the study team became aware their child had died. See Figure 1 for more details.
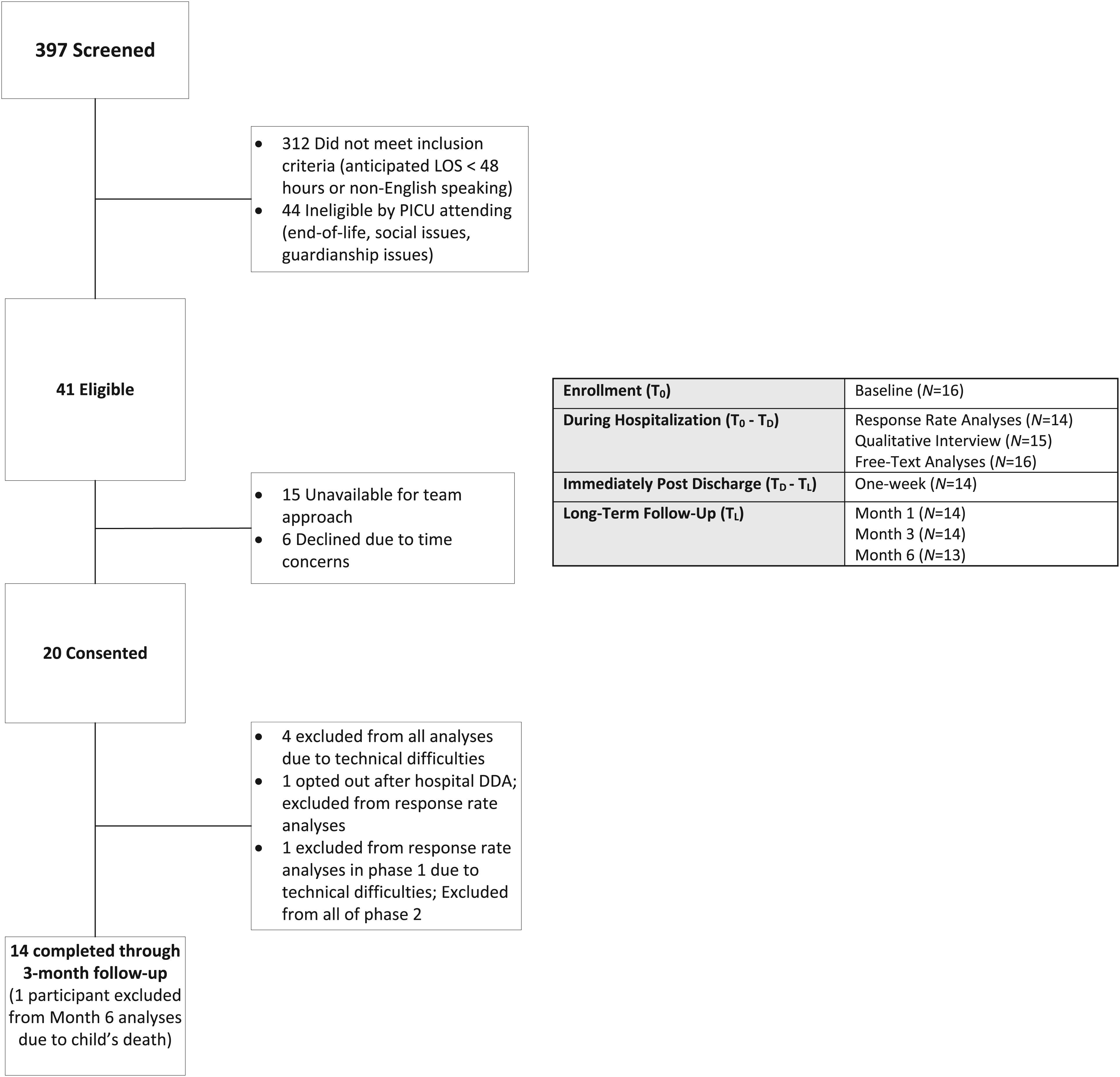
Patient flow through study.
Survey Response Results
All participants completed the baseline study (n = 16). Of participants included in hospital DDA analyses (n = 14), participants were sent an average of 4 surveys during hospitalization (M = 4.2, SD = 7.5; range: 1–30). Most participants (86%) completed all surveys (M = 89, SD = 29). Discharge survey completion rates ranged from 79 to 94% (n = 14), except month 6 completion rate which was 46% (n = 13).
Of surveys that were started, 99.6% were fully completed. After excluding 2 extreme outliers, the average completion time for DDA surveys per participant was 92 s (n = 12, M = 92.1, SD = 40.2, Mdn = 78.9). After removing 3 extreme outliers, the mean completion time for longer surveys (eg, baseline, M1, M3, and M6) per participant was 4.6 min (SD = 2.5′).
Acceptability of Texting System
Likert Scale Survey
Table 1 presents data from Likert scales both during hospitalization and post-discharge. Most participants agreed that the text system was easy to use (100%), the instructions were clear and easy to follow (100%), they were satisfied with the texting system (96%), and it is a useful way to assess experiences during and after hospitalization (75%). Most participants disagreed that they experienced technical problems (92%), it interfered with their daily life (96%), they received text messages too often or at an inconvenient time of day (83%), or it took too much time to complete each survey (75%). Most participants disagreed (54%), or neither agreed nor disagreed (38%) that it was distressing to use the texting system, while 2 participants did find the system distressing. Many participants found the system comforting (77%) and beneficial (69%) during hospitalization, as compared to 45% for each post-discharge. See Table 1 for full data.
Qualitative Interviews
In total, 80% of eligible participants (n = 12) completed the first qualitative interview 1 week after discharge; 60% of eligible participants (n = 8) completed the second qualitative interview 3 months post-discharge. Given that themes were largely consistent across the 2 interviews and almost all (88%) of the participants who completed interview 2 also completed interview 1, results from interview 1 are presented below.
Positives of Texting System. Many participants highlighted positive aspects of the texting system regarding convenience, applicable questions, reminders, and other positives.
All participants described that the texting system was convenient: easy to use and simple, quick to complete, and flexible such that it could be completed at any time, and they enjoyed the texting modality. About half of the participants noted that they felt the questions were applicable and relevant to their experiences: “the questions were straightforward and applicable…and I did have many emotions at 1 time. So yeah. It was spot on” and “I think [the questions] captured [my experience] well.” A couple of participants noted that they appreciated the reminders provided. Several participants provided other relevant answers regarding positives of the system that were coded as other positives, such as the survey prompted reflection and/or was therapeutic.
Areas for Improvement. Participants also responded to questions regarding areas for improvement in the texting system with the following themes emerging: no improvement, improving features, adding features, and improving content.
Almost all participants reported that they would not change anything (no improvement). Few respondents had suggestions to improve features: separating the links spatially, improving the slider, improving reminders, and changing the schedule of messages. A few participants suggested improving content to reduce redundancy and improve the relevance of questions to family circumstances. A few participants described adding features, such as providing support services based on responses.
While 2 participants did endorse finding the system distressing in the post-discharge survey, no additional information was provided during the interview to clarify these responses.
Other Factors to Assess. Participants suggested other factors for investigators to assess to understand their experiences, divided into medical and non-medical factors. Medical factors suggested included child medical factors (eg, severity of illness and medical history) and experiences with the medical team (eg, communication): “what the kid is in the hospital for and the background history of what they’ve gone through” and “if they felt heard by the care team.” Some participants suggested that the survey assess non-medical factors such as the logistical experience of being in the hospital (eg, transportation and finances): “maybe the accommodations and how that is going…are you able to groom yourself? Are you able to stay at the McDonald's house?”
Barriers to Completion. Most participants described that there were no barriers to completing surveys. Some participants stated responsibilities for their child or work occasionally interfered with participation: “Life continued to happen. Between work, school, and taking care of that or like my special needs kids or my other kids.”
Considerations Regarding Sharing Information with Providers. While they were informed that responses during the pilot were not reviewed or shared with their child's care team, participants described potential benefits and concerns if information from the texting system was shared with providers in future iterations.
Benefits. Some participants felt information sharing would offer providers with emotional context regarding how parents are feeling emotionally in order to tailor their care for this family based on that information.
Concerns. Most participants described having no concerns about sharing information with providers. Some participants worried that sharing this information with providers would change care they received including changes in interactions and care for the child and family and/or the provider's response would be inappropriate for the parent's needs.
Feasibility and Acceptability of Open-Ended Qualitative Question
Completion Rate. Overall, participants (n = 14) provided responses to 20% of optional open-ended question prompts. A total of 6 participants (43%) used this option at least once. Of those who used it at least once, most (83%) used this option more than once.
Interview Qualitative Data. Participants described positives of the open-ended question including that it was therapeutic and allowed for elaboration about their experience, and they appreciated that it was optional: “Easy and reflective. It helps to reflect.”
Others noted that they did not respond to the survey due to lack of time, preferring other question types and feeling they had nothing to report.
Optional Open-Ended Qualitative Question Responses
Themes of the optional responses to the open-ended qualitative questions are presented in Appendix B. While they are not salient to the study's primary aims of feasibility and acceptability, they do provide interesting and unique insights into parents’ lived experiences while their child is critically ill.
Discussion
This study demonstrated that use of a text messaging interface to assess parent's experiences throughout their PICU stay and following discharge was feasible and acceptable to participants.
Regarding feasibility, once early technical problems were resolved, most participants completed all requested surveys during PICU stay and continued to do so for 3 months following discharge. Virtually, all surveys were completed once started, and completion time was modest, with a mean of 92 s for the every-other-day surveys, once extreme outliers were removed. These outliers were believed to be participants who left their phone unattended during survey completion. Participants voluntarily provided answers to optional open-ended questions, with 43% of participants electing to use this option in at least 1 instance. Taken together, these data support the feasibility of using a text-based interface to engage families in near–real time, even amid the often chaotic and overwhelming circumstances of a PICU stay. Such a tool therefore could shed light on parents’ lived experiences with their critically ill child and potentially lead to more rapid, responsive interventions. Moreover, these data suggest that families are willing to provide additional contextual information beyond simply answering closed-ended questions.
The use of a near–real-time text-based tool is further supported by acceptability data via surveys and interviews. All participants agreed or strongly agreed that the system was easy to use both during and after PICU stay and that they were satisfied with the system at discharge, with the majority remaining satisfied at month 3 (91%). While the goal of the interface was not to provide a therapeutic intervention, many participants reported benefit: 76% reported the interface to be comforting while their child was hospitalized and 69% that they benefitted from using the system. Both percentages dropped to 45% of participants for the post-discharge texting interface. No participants reported that surveys were too long or that they interfered with their lives during the PICU stay; only 1 participant reported receiving messages at an inconvenient time of day.
Acceptability was further supported by qualitative interviews. Participants appreciated the convenience of the system, the applicability of the questions, and the reminder texts to be helpful. Most participants had no suggestions for the improvement of the system; however, some participants provided constructive feedback. This feedback suggested improvements to both the features/appearance of the system and content. Participants also recommended assessment of other contextual factors, both medical (a child's illness, communication) and non-medical (transportation, financial stress). Logistically, most participants described no barriers to completion but acknowledged that life circumstances occasionally delayed their completion of surveys.
Participants suggested ideas for supporting families. Multiple participants suggested providing support to families based on their responses. Some participants felt that relaying information to medical providers could help providers tailor care to a family based on their experiences. Some noted that such an interface could augment medical communication by providing a venue to ask non-emergent questions. Most participants would feel comfortable sharing their information with medical providers; however, some worried that sharing information might change their child's care in unfavorable ways.
While feedback was overwhelmingly positive, there are important limitations to both the text-based interface and this pilot study. With respect to the interface, the technical issues at initial roll-out warrant consideration for subsequent iterations. In this case, it was fixed by partnering with the local network operators and the survey company. However, this is an important reminder that the technical aspects of such an interface should be thoroughly tested prior to initiation of a study or clinical program such as this, as each hospital will have its own particulars with respect to cellular and wireless internet access. Additionally, 2 participants reported their experiences with the surveys at least somewhat distressing. The follow-up interview was unable to elicit additional details. While this was a minority opinion, further investigation is warranted to understand and mitigate this distress. As this was a feasibility and acceptability study, it had a deliberately small sample size. It should be noted that the acceptability data collected—both via survey questions and interviews—addressed 2 separate but interrelated elements: the acceptability of the interface itself and the acceptability of querying PICU parental experience on a frequent basis more generally. In the case of this study, participants found both elements to be acceptable. However, it is possible that 1 or both elements might not generalize to other settings or different interfaces. Further study in other settings, and with other interfaces, will help to further delineate the most optimal means of data collection regarding parental PICU experiences.
Though qualitative and quantitative data support the notion that this interface was feasible and acceptable, the sample is far too small to make conclusions with respect to participants’ experiences and adverse psychological outcomes. Furthermore, this sample is all drawn from a single PICU, with its own distinct characteristics and demographics. While the interface was feasible and acceptable among this group, that may not generalize to participants from other PICUs. Moreover, we did not collect demographic or clinical information for the purpose of this pilot. Based on this, and our small sample size, we cannot ascertain if there are specific groups for whom this interface and approach are more or less feasible and acceptable—only that, on the whole, it was both feasible and acceptable for this sample. Further, participants in this pilot were all English speakers with their own devices. In the future, efforts should include a diverse group, including non-English speakers and those without cellphones, as these populations likely have unique perspectives and stressors. Subsequent study should capture specific demographic and clinical information to allow for more robust analysis. Given the small sample size, only descriptive statistics were performed. A larger sample would allow for further analysis, including regression modeling, which could elucidate variables which are positively or negatively associated with feasibility, and eventually, to determine associations with parental mental health outcomes. Lastly, as this study was voluntary, it does not capture the experiences of parents who declined to participate. It is possible parents with the highest levels of distress could be over- or under-represented in the study group, which could impact the ability to identify families most at risk.
Conclusions and Future Directions
A text-based interface could be a valuable tool in the armamentarium of researchers and clinicians alike to learn about parents’ experiences with their child's illness while in the PICU and beyond. With feasibility and acceptability established, further research can explore how such an interface may be used for early identification of parents most at risk of adverse psychological sequelae and ultimately for the provision of earlier supportive interventions. Likewise, an interface such as this could be used to assess changes in variables of interest before and after interventions or other PICU events to understand experiences in a more dynamic fashion.
Footnotes
Acknowledgments
The authors would like to acknowledge the input of all members of the Pediatric Collaborative for Resilience and Emotional–Wellness Science (Pediatric CREWS). Specifically, we would like to acknowledge Brynn LiaBraaten, BA; Julia Tager, MS; and Madeline Johnson, BA, for their significant contributions to the analysis of qualitative data elements. Further, we would like to acknowledge the substantial efforts of Sadaf Shad, MD, to the recruitment and instruction of research participants, and of Stacee Lerret, PhD, RN, CPNP-AC/PC, for her insights, guidance, and expertise throughout the research process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, Award Number UL1TR001436, and by the generosity of Froedtert Hospital. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Appendices
Appendix A—Positionality Statements of Authors
Charles Rothschild is an cis-gender, English-speaking white man from Wisconsin who has lived in cities throughout the US. He has traveled extensively throughout Europe, Latin America, Africa, and Asia, and is passionate about the promotion of understanding and equity across cultures. He is a physician who practices Pediatric Critical Care Medicine and Pediatric Palliative Care Medicine. His research centers around collaborative research exploring the factors that contribute to, and help alleviate, distress amongst children with serious illness and their families. Kathryn Balistreri is a white, cisgender woman and clinical psychology graduate student from Milwaukee, WI. She has limited clinical and lived experience in the pediatric ICU, but her research focuses on child and family well-being in the pediatric ICU. These perspectives influenced all stages of the research process, including study design and qualitative interview data collection and analysis. Kathryn Mulligan is a cisgender, white female from El Dorado Hills, California who has lived throughout the United States for training and education. Currently she in her final year of pediatrics residency with plans to pursue training in Pediatric Critical Care and Palliative Care Medicine. Past experiences, both personal and professional, have influenced her perspectives and inform her ongoing research in the PICU. K. Jane Lee is a white, English-speaking, cisgender woman who is a parent to bi-racial children, one of whom has severe neurologic impairment and significant health care needs. She has lived in the Midwest for her entire life. She has a master's degree in Bioethics and has practiced Pediatric Critical Care and Pediatric Complex Care for over 20 years with a diverse patient population. Her academic work has focused on decision-making, resilience, and family wellness. Jeffrey Karst is a cis-gender, English-speaking white male from Wisconsin who grew up in rural Montana, an area with quite limited cultural and ethnic diversity. He is a pediatric psychologist in hematology, oncology, and blood and marrow transplant who works with a socioeconomically and culturally diverse patient population and is appreciative of the willingness of his patients and their families to share more about their cultural experiences and background for the sake of his clinical practice and ongoing education. Miranda Privatt is a cis-gender, white female who grew up and resides in a small suburban town in Southeastern Wisconsin. She has traveled internationally and served cross-cultural populations, including in Mexico and Costa Rica. These experiences have greatly influenced her perspectives. She is a pediatric critical care Clinical Research Coordinator and has a psychology background. Kristin Magner is a cis-gender, white, English-speaking female from Wisconsin who has worked in Pediatric Critical Care as both a nurse and nurse practitioner for her entire career. She has traveled and studied abroad on multiple occasions. Her research focuses on understanding parent and provider perceptions of illness and collaborating with onco-critical care in the management of PICU patients. Han-Joo Lee is an Asian immigrant from South Korea and has resided in the US for approximately 20 years. He is a Professor of Clinical Psychology at the University of Wisconsin-Milwaukee, and has been a member of the Educational Workgroup of the Psychology Departmental Diversity Committee. His research focuses on developing technology-assisted assessment and intervention strategies that can reach out to a wide range of individuals who experience anxiety, trauma, and obsessive-compulsive disorder-related problems. Matthew Scanlon is a white, English-speaking, cisgender male who has spent his life in the Midwest of the U.S. He has worked in the pediatric ICU setting for over two decades, with added experience in patient safety. His direct experiences with patients and families in the PICU setting have both informed and guided his research work. W. Hobart Davies is a cisgender white male psychologist with many years of practice and research experience in various pediatric settings with a wide range of populations. He is an Army brat who has lived throughout the US and in Europe. His research team is focused on exploring new research approaches to amplify the voices of youth and families in pediatric psychology.
Appendix B: Delphi Qualitative category frequencies from PICU parents free-text responses, percentages calculated out of total number of responses (n = 28).
Theme
Illustrative Quote
n (%)
Medical Status of Patient
It is stressful not knowing what our daughter, specific diagnosis is and just stressful that it is a waiting game.
11 (39%)
Negative Emotion
I have been very overwhelmed and physically drained no matter how much sleep I get.
10 (36%)
Faith
Praying everyday & having faith that he will be home soon
7 (25%)
Hospital Challenges
I think being in the hospital this long is getting a little taxing.
4 (14%)
Activity
Keeping busy & talking with family members.
3 (11%)
One Day at a Time
Taking it day by day.
3 (11%)
Hope/Optimism
Her current medical status is very overwhelming, but I am hopeful.
3 (11%)
Hospital Supports
All the nurses and staff were very warm, welcoming, understanding and helpful.
3 (11%)
Enjoyment of Caregiver Role
I just try to enjoy every day I have with him even the bad days.
3 (11%)
Social/Family Supports
What has carried me through is my relationship with my husband.
2 (7%)
Doing Okay
We are good.
2 (7%)