
Abstract
Unplanned extubations (UE) frequently occur in critical care units. These events are precipitated by many risk factors and are associated with adverse outcomes for patients. We reviewed the current literature to examine factors related to UE and presented the analysis of 41 articles critical to the topic. Our review has identified specific risk factors that we discuss in this review, such as sedation strategies, physical restraints, endotracheal tube position, and specific nursing care aspects associated with an increased incidence of UE. We recommend interventions to reduce the risk of UE. However, we recommend that bundled rather than a single intervention is likely to yield higher success, given the heterogeneity of factors contributing to increasing the risk of UE.
Keywords
Introduction and Rationale
Unplanned extubations (UE) are a common occurrence in intensive care units. The incidence of UE is best reported as a percentage of intubated patients but better expressed as incidence density while patients are at risk. 1 Therefore, the denominator is presented as days of mechanical ventilation. As such, reported occurrences range from 3% to 16% of intubated patients or 0.1 to 3.6 per 100 days of mechanical ventilation.2–6 UE is classified into deliberate extubations, where patients extubate themselves, or accidental extubation, where patients are extubated during patient care activities. UE, especially the deliberate type, is typically a sequela of many circumstances rather than resulting from a single forerunner and is associated with untoward outcomes such as prolonged duration of mechanical ventilation, prolonged intensive care unit stay, and increased risk of pneumonia.7,8 The complications are especially notable for failed UE events requiring re-intubation. Moreover, there is an increase in mortality among patients with co-morbid conditions. 9 Despite efforts to mitigate risk factors, rates have remained unchanged for the past two decades. The reported rates before the year 2000 ranged from 2.6% to 14%.4,10,11 More recent reports noted a similar but broader variation8,12 ranging from 1% to 22%.3,12–18 Interventions utilizing a multi-disciplinary approach have been implemented to decrease UE, yet only some have successfully improved rates nationally. Due to the complex nature of UEs, preventing these events requires a comprehensive multidisciplinary approach and special attention to risk factors and near-miss events. This review explores the risk factors of UE and strategies to minimize their incidence.
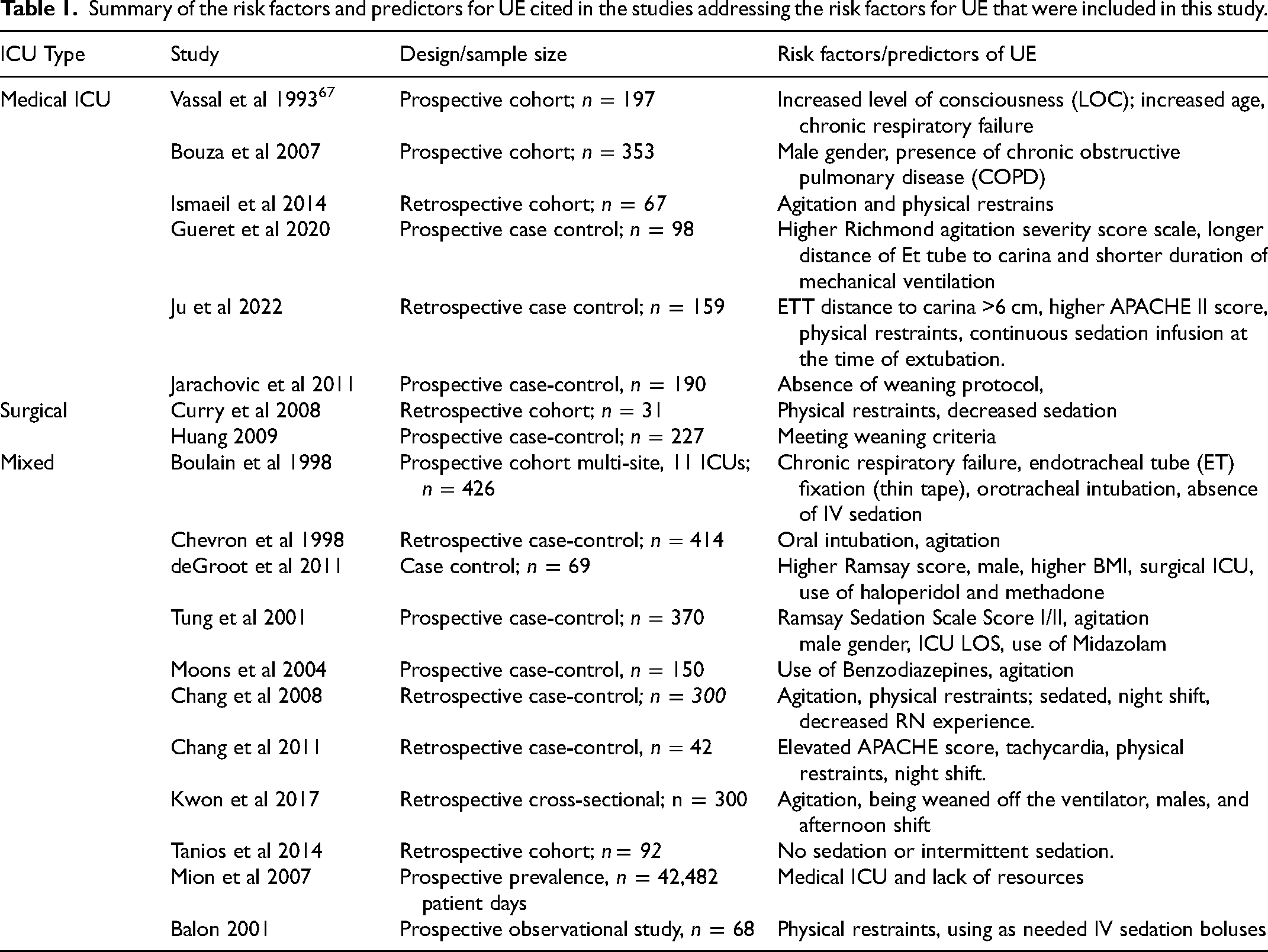
Summary of the risk factors and predictors for UE cited in the studies addressing the risk factors for UE that were included in this study.
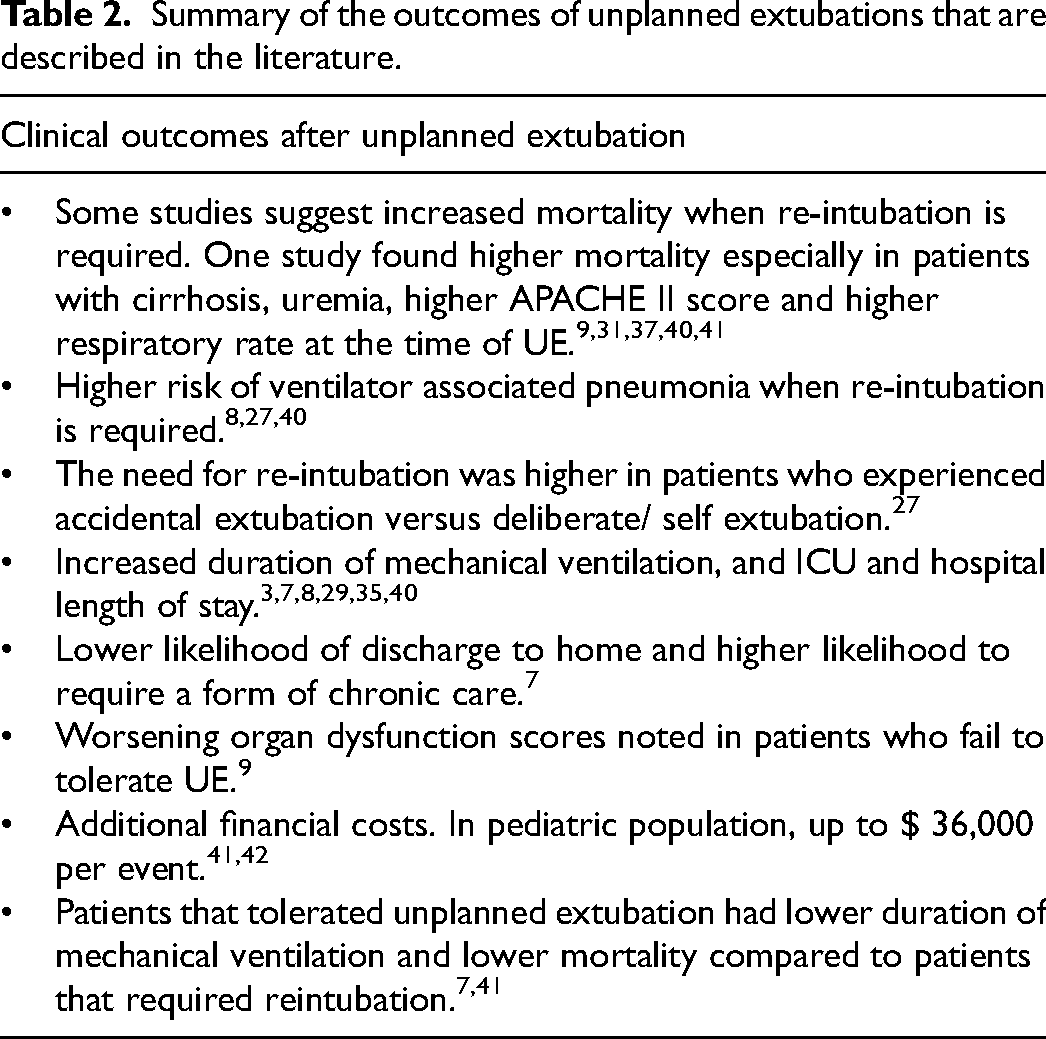
Summary of the outcomes of unplanned extubations that are described in the literature.
Methods
Peer-reviewed publications in the English language published between 1999 and 2021 were included in the search through 2 databases; Google Scholar and PubMed. Seminal articles published before 1999 were included in the review to add context when necessary. A search for articles was conducted using the following keywords: “unplanned extubation,” “unplanned extubation risk factors,” “unplanned extubation outcomes,” “sedation strategy,” and “endotracheal tube.” We included articles based on their relevance to the topic and available text. We excluded studies that were primarily addressing pediatric or neonatal populations. We identified 41 peer-reviewed publications addressing the risk factors and outcomes of UE that we included in this review. We summarized the isk factors for unplanned extubations in Table 1. We also included Table 2, which summaeizes the clinical outcomes of unplanned extubations.
Aim
This literature review aims to identify the significant risk factors for UE cited in the literature recently. We suggest interventions that can reduce the incidence of UE and their associated complications.
Review of the Literature
Risk Factors for Unplanned Extubations
Sedation and Level of Consciousness
Sedation strategy and the level of consciousness significantly impact the risk of UE. Lower sedation level or restlessness has been considered to pose a risk.3,13,19– 23 A retrospective study found that continuous sedation with daily sedation interruptions was associated with a lower rate of UE (1.5 events/ 1000 MV Days) when compared to intermittent sedation (5 events/1000 MV Days) or no sedation (16 events/1000 MV Days). 19 Regarding the choice of sedatives, benzodiazepines have been shown in previous studies to increase the risk of UE.3,20 A likely explanation may be due to the paradoxical effect of benzodiazepines, which are associated with an increased risk of agitation and delirium, contributing to an increased risk of UE. A retrospective study found that mechanically ventilated patients in a surgical critical care unit who experienced UE had a higher Ramsay score (mean Ramsay score, 2.42; SD, 1.06), indicating a lower degree of sedation. 21 Additionally, Various studies have demonstrated an increased risk of re-intubation following UE when patients maintained a higher level of consciousness.3,24–26 Sedation strategies and types of sedatives used may increase the risk of agitation and, subsequently, the risk of UE if not carefully tailored to the patient's needs.
Physical Restraints
Physical restraints are used frequently in critical care units, especially intubated patients, to prevent deliberate extubations or pulling on other tubing and lines. In 2010, a survey of 1976 responders from the American Association for Respiratory Care (AARC), the American Association of Critical Care Nurses (AACN), and the Society of Critical Care Medicine (SCCM) showed that 72% of the respondents perceived the absence of physical restraints as a risk factor for UE. 24 However, using physical restraints does not UE. Several studies have found that patients experiencing UE were more likely to have physical restraints applied during the event than controls.27,28 In a retrospective analysis of 1455 patients receiving mechanical ventilation, researchers compared 100 patients with UE to 200 patients matched and found that using physical restraints was associated with 3.1 times increased risk for UE. 29 No specific reasons for applying physical restraints were reported, and the researchers concluded that better standards are needed when using restraints. The higher risk of UE with using restraints is likely confounded by the presence of delirium, agitation, or inadequate sedation, 30 rather than attributed to agitation from the presence of restraint.
Endotracheal Tube Management
Endotracheal tube (ETT) management and securement play a significant role in UE, precisely the securement depth and proximity to the carina. A case-control study found that a distance from the tip of the carina of more than 59 mm was associated with increased UE risk with an odds ratio of 6. 30 Ju et al. demonstrated an odds ratio for UE of 6.41 when the distance to the carina was greater than 6 cm. Similarly, other studies found that patients with UE had a longer distance from the carina to the ET tube than controls.31,32 Although ET tube placements are generally confirmed by chest X-rays, predicting their positions with subsequent patient care activities is challenging. Head movement has also been associated with changes in the ET tube position and cuff pressure.33,34 Mechanically ventilated and sedated patients in the critical care unit are subject to frequent repositioning, including changes in head position. Therefore, they are at increased risk of ET tube migration and subsequently increased risk for UE.
Nursing Care
Various features of nursing care have been shown to affect the incidence of UE. Yeh et al. reported a 22.5% incidence of UEs in a medical center with 11 ICUs over one year. 12 Only 2.3% of these events occurred with nurses with more than four years of critical care experience. 12 Kwon et al. and Chang et al. found a similar correlation between fewer years of critical care experience and increased risk of UE.13,35 In the former, a retrospective case-control study demonstrated an average critical care experience of 15.3 months in the UE group, while controls who did not experience UE were cared for by nurses with an average critical care experience of 23.7 months. 35 In addition to experience, nurse workload has been linked to an increased incidence of UE. In a multidisciplinary survey of critical care providers, 60% of the responders viewed a nurse-to-patient ratio of 1:3 as a risk factor for UE. Kwon et al. found that in patients with UE, nurses had a higher workload, indicated by a higher WMSCN score. 35 Additionally, a higher incidence of UE was reported during the night shift.13,35–37 A few factors can explain this observation. Night shift nursing staff can be nursing load, experience, or exhaustion and vigilance level to the biological sleep-wake cycle, and effect of shift work. The nighttime effect of alarms and other sleep disruptors can also affect patients and precipitate agitation or delirium.2,12,19,35–37
Patient Characteristics
Medical ICUs traditionally have the highest rates of UE.14,15 Data from a national prevalence study reports 23.4 episodes of UE in MICUs per 1000 ventilator days. 14 Approximately 9.5–15% of all ventilated patients in the MICU experience UE.14–16 Male gender and chronic obstructive pulmonary disease (COPD) have been reported among the demographic risks. 38 Patients ventilated in Medical ICU often have complex chronic medical conditions, which result in prolonged ventilation and increased risk for UE. UE for the Surgical ICU (SICU) is reported at 1.41 episodes per 100 ventilator days, 17 or 6.8 episodes per 1000 ventilator days 14 which is lower than the MICU cohorts. Specific to the SICU, age, sedation scale scores, need for reintubation, ICU nurse experience, and location of staff at the time of UE, criteria for extubation have been suggested21,39; however, significant predictors were the use of restraints, decreased sedation, 21 and meeting criteria for extubation. 39 Among patients who experienced UE, 87% were physically restrained, 21 with reported low sedation levels (mean RASS = 2.42) preceding the UE. Most patients (64%) met the criteria for planned extubation and did not require re-intubation, 39 suggesting readiness for planned extubation. The larger body of literature obtained from medical-surgical or “mixed/general” ICUs confirms similar findings. More variables were included as potential risk factors for mixed ICUs owing to the high number of studies in the mixed ICU setting. The additional variables were admission diagnosis, APACHE II score, ICU and hospital LOS, days of mechanical ventilation, ventilator settings, nosocomial infection laboratory values, medication types, and body mass index.3,13,20,29
Clinical Outcomes After Unplanned Extubation
After an UE, reintubation is not always required but portends worse outcomes. Reintubation depends on the patient's clinical condition and is needed in 43%–63% of the cases.7,8,40 Patients with UE during MV weaning have a lower reintubation rate.7,8 Irrespective of the cause of UE, there are adverse consequences for the patient and the hospital. Patients who experience UE may have higher rates of hospital mortality which can be related to additional costs associated with the severity of the injury, the need for reintubation, and underlying chronic diseases. 17 Older age, male gender, lower RASS score at the time of UE, not being on a weaning trial at the time of UE, and being intubated initially for acute hypoxic respiratory failure were all associated with an increased risk of requiring re-intubation after UE.19,30,66 Patients who experience accidental UE have a higher incidence of nosocomial pneumonia (27.6% v 13.8%, p = .002), 8 longer duration of mechanical ventilation, and increased length of stay (LOS).17,29 Accidental UEs were associated with an increased risk of requiring re-intubation compared to deliberate UEs. These patients were also more likely to suffer from hospital-acquired pneumonia.8,31 UE is associated with increased mortality; however, this seems to be primarily derived from the subset of patients that fail UE. A prospective cohort study found that patients who required reintubation had a higher mortality rate than patients who tolerated UE (54.5% vs 5.9%, p = .007). 8 Thille et al. found similar results with increased ICU mortality among patients who failed UE (50% vs 5%, p < .01). 31 A retrospective cohort study in Chi Mei Medical Center found a higher prevalence of higher APACHE scores before UE, higher respiratory rate before UE, uremia, liver cirrhosis, and malignancy among patients who did not survive UE compared to patients that survived UE. 9
UE can damage the larynx and cause airway complications because the tube is removed while the cuff is still inflated, which can also precipitate bronchospasm, or lead to aspiration.17,18 These complications can make re-intubation more difficult if necessary. Hypoxemia, hemodynamic instability, hypotension, brain damage, cardiac arrest, and even death if inadequate ventilation occurs. 18 In patients who are ready for planned extubation or are undergoing weaning, the occurrence of UE does not always lead to re-intubation.8,16 Those who do not require re-intubation experience reduced mechanical ventilation and weaning duration.3,8,12,16,25,39 Only 45% of patients who self-extubate require re-intubation. The need for reintubation after UE adversely impacts outcomes.8,41 Patients requiring re-intubation have a significantly higher rate of developing pneumonia, experiencing increased ICU or hospital length of stay or mortality than those successfully self-extubated.8,13,41 It is doubtful that the re-intubation process causes the increase in-hospital mortality but it is likely the interaction between the UE event and premorbid conditions. Apart from affecting clinical outcomes, the requirement for reintubation can lead to higher hospital expenses, regardless of the direct costs of longer stays in the ICU or prolonged use of mechanical ventilation. 21 The estimated additional cost in pediatric patients was approximately $36,000 42 and is likely higher in adult patients due to the multiple comorbidities that accompany the need for mechanical ventilation and other hospital charges (pharmacy, lab, and diagnostic charges). 41
Prevention of Unplanned Extubations
Agitation Management
Most studies cited agitation or inadequate sedation as risk factors for UE.3,12,15,20,21,29 Therefore, we recommend identifying and correcting the cause of agitation, which is often precipitated by pain or delirium.43–45 The prevalence of delirium in the ICU ranges from 20% to 80%46–48 and is related to sleep deprivation, older age, restraints, abnormal lab values, medications, infection, and respiratory complications. 44 The treatment for delirium is mainly by prevention, early recognition, interdisciplinary and pharmacologic protocols, increased nursing presence, and short-acting sedation when necessary.44,45,49,50,65 While none of the studies directly linked UE to delirium, a quality analysis of risk factors at the time of UE by Kerckhoffs et al., using bow tie analysis methods, identified delirium as a critical factor present in most UE cases, 50 raising the possibility that the agitation reported in other studies may be reflective of agitated delirium. Routine screening using validated delirium screening tools would aid in the early detection and management of delirium. It would provide a standardized method for future trials to explore the relationship between delirium and UE. Reducing pain and delirium may portend better outcomes, as both are prevalent in patients with UE. 35
Sedation and Physical Restraints
When sedation protocols and physical restraints were combined with other interventions, reductions in UE were observed. A quality improvement project conducted in a hospital in Singapore employed the PEST model with a resultant decrease in UE by 50%. 51 The model incorporates sedation protocols with a goal RASS score of 0 to −2 and requires daily assessment of physical restraints by a provider with re-ordering restraints daily. Implementing protocoled sedation strategies has been associated with positive outcomes. Li et al. found that administering sedation through a protocol that incorporates regular assessment of pain and delirium and providing daily sedation holidays is associated with a shorter duration of mechanical ventilation, shorter ICU stay, and lower incidence of delirium than controls. 52 Although the study did not find a statistically significant reduction in UE, there was a trend toward a lower incidence. 52
Integration of Weaning Protocols
Protocol-directed weaning is beneficial for decreasing ventilator days, time to wean from mechanical ventilation, and ICU LOS. 53 A systematic review that included 2434 patients from 17 trials compared the effect of using the standardized weaning protocol on the total duration of mechanical ventilation. Results showed that a protocolized weaning approach reduced the mean duration of mechanical ventilation by 26% (95% CI 13% to 37%, p < .0002). Weaning time was reduced by 70% (95% CI 27% to −88%, p = .009), and ICU LOS was reduced by 11% (95% CI 3% to 19%, p = .01). In a prospective cohort study, Jarachovic et al., concluded that the use of weaning protocols was associated with a significant reduction in the rate of UE. 16 Their findings specifically identified weaning protocols as an essential factor for reducing UE; patients who had weaning protocols ordered and followed were least likely to experience UE (p = .02). 16 A separate quality improvement initiative demonstrated an overall decrease in the number of UE (from 5.2% to 0.9%) after implementing weaning protocols as the standard of care. 54 Implemented protocolized weaning to help reduce UE risk while reducing MV time and ensuring timely extubation.16,53
Securing the Endotracheal Tube and Preventing Near Misses
The distance of the endotracheal tube to the carina is associated with an increased risk of UE. A distance of more than 5 cm has been shown to increase the risk for UE.30–32 Furthermore, ET tube securement devices and methods have been a frequent topic of debate.55–58 However, the impact on UE and facial ulcers remains has not been consistent.57,59–61 Therefore, we do not recommend a specific securement method. Still, we recommend standardization of securement methods and techniques while implementing routine monitoring the integrity of the tube securement device and maintaining a distance to the carina <5 cm. This can be accomplished through education and multidisciplinary accountability. Increased surveillance might be more impactful during the night shift.
Nursing Strategies
Variability in nursing care affects the incidence of UE. Many studies have shown nursing experience to affect the incidence of UE. Workload and nurse/patient ratio has been frequently cited as risk factors for UE.1,24 Optimizing the nurse workload will likely reduce the incidence of UE, as patients with a high risk for UE will have more time for provider presence at the bedside. The addition of one additional nurse per patient day can result in a 51% decrease in UE, while a reduction in nursing workload could result in a 45% decrease in UE.62,63 Maintaining a patient-to-nurse ratio of 2:1 or less is likely to achieve this impact. Time of the day is another factor contributing to the risk of UE, as UE frequently occurs on the night shift and during shift changes when no nurse is at the bedside.12,13,21,38,64
Furthermore, methods to identify high-risk patients for UE are necessary to yield the desired outcome. In a QI project conducted by Chao, Chien-Ming, et al., a task force was introduced in addition to several other interventions to identify patients at high risk for UE. 65 Additionally, a system of event review and debriefing was introduced to evaluate every UE and identify shortcomings. 65 Both interventions, along with several other multidisciplinary interventions, resulted in a reduction in UE from 9 events/1000 ventilator days to 1.36 events / 1000 ventilator days. 65 Similar strategies involving evening rounds and identifying patients at high risk for UE were implemented in other QI projects, yielding similar results. 66 We recommend implementing a practice where patients with an increased risk of UE are regularly identified to prevent UE.
Summary
UE is a frequent occurrence in the ICU that is associated with various modifiable and non-modifiable risk factors. UE is associated with adverse outcomes for patients and additional costs to hospitals. We recommend a multidisciplinary approach, including using validated protocols for sedation and weaning and an effort to minimize near misses to reduce the risk of UE.
Footnotes
Authors’ Contribution
AA, RP, and MAT contributed to the Literature search, Manuscript preparation, and Review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article