
Abstract
Intensive care physicians may assume the primary care of patients with transplant-associated thrombotic microangiopathy (TA-TMA), an uncommon but potentially critical complication of hematopoietic stem cell transplants (HSCTs) and solid organ transplants. TA-TMA can have a dramatic presentation with multiple organ dysfunction syndrome (MODS) associated with high morbidity and mortality. The typical presenting clinical features are hemolytic anemia, thrombocytopenia, refractory hypertension, proteinuria and worsening renal failure. Intestinal involvement, with abdominal pain, nausea and vomiting, gastrointestinal bleeding, and ascites are also common. Cardiopulmonary involvement may develop from various causes including pulmonary arteriolar hypertension, pleural and pericardial effusions, and diffuse alveolar hemorrhage. Due to other often concurrent complications after HSCT, early diagnosis and effective management of TA-TMA may be challenging. Close collaboration between ICU and transplant physicians, along with other relevant specialists, is needed to best manage these patients. There are currently no approved therapies for the treatment of TA-TMA. Plasma exchange and rituximab are not recommended unless circulating factor H (CFH) antibodies or thrombotic thrombocytopenic purpura (TTP; ADAMTS activity < 10%) are diagnosed or highly suspected. The role of the complement pathway activation in the pathophysiology of TA-TMA has led to the successful use of targeted complement inhibitors, such as eculizumab. However, the relatively larger studies using eculizumab have been mostly conducted in the pediatric population with limited data on the adult population. This review is focused on the role of intensive care physicians to emphasize the clinical approach to patients with suspected TA-TMA and to discuss diagnosis and treatment strategies.
Introduction
The Center for International Blood and Marrow Transplant Research (CIBMTR) reports over 8000 allogeneic and 11,000 autogenic HSCTs in the United States per year. 1 Although infections and graft-versus-host disease (GVHD) have historically been the major contributors to transplant-related nonrelapse mortality,2,3 transplant-associated thrombotic microangiopathy (TA-TMA) has increasingly become recognized as an independent entity with incidence rates of 8.2% to 39%.4–7 It is characterized by the development of post-transplant hemolysis with schistocytes, thrombocytopenia, and organ dysfunction. Kidneys are the most common organs to become involved; intestinal involvement is also recognized. 8 The intensive care unit (ICU) is typically required because TA-TMA often progresses to multiorgan dysfunction syndrome (MODS) and has a mortality rate of 50% to 90%.4,9
TA-TMA is most commonly associated with allogeneic HSCTs, but it has also been reported after autologous stem cell transplants 10 and solid organ transplants.11–13 Children receiving tandem autologous stem cell transplants for neuroblastoma seem to be at high risk of developing TA-TMA. 10 The clinical manifestation can range from mild anemia and thrombocytopenia to severe MODS and death. 14 The introduction of novel agents in high-risk TA-TMA, such as the complement inhibitor eculizumab, has been associated with favorable outcomes with one study showing survival rates of 52% at 13.5 months.15,16 Another promising emerging therapeutic agent is narsoplimab (OMS721), a mannan-binding lectin-associated serine protease-2 (MASP-2) pathway inhibitor. 17 The incidence and mortality rates of TA-TMA are not well defined due to a lack of standard diagnostic criteria, under-recognition of the disease, and different treatment practices especially in critically ill patients who often have concurrent infections, graft-versus-host-disease (GVHD), or other complications of transplant. Large prospective trials are lacking, raising the need for an expert consensus on diagnostic and treatment algorithms. Recent comprehensive reviews on TA-TMA have been published8,18; however, this review focuses on the issues critical for intensive care medicine.
Pathophysiology
The pathophysiology of TA-TMA is multifactorial and complex and remains incompletely understood. Unlike in other thrombotic microangiopathies, there is no one inhibitor or protein deficiency that explains TA-TMA. We instead consider TA-TMA as a syndrome that develops after transplantation with multiple possible inciting events leading to different clinical features and outcomes.
The central event in the pathogenesis of TA-TMA is believed to be endothelial injury and the subsequent activation of procoagulant factors, immune effector cells, and the complement cascade that ensues. This theory was first supported by direct visualization of the damaged endothelium in patients with suspected TA-TMA with scanning electron microscopy. 19 Patients with TA-TMA have also been found to have significantly increased serum levels of markers of endothelial injury such as soluble vascular cell adhesion molecular-1, tissue-plasminogen activator-plasminogen activator inhibitor complex, thrombomodulin, and suppression of tumorgenicity 2 (ST2).20–22 Endothelial injury results in the release of interleukin-8, neutrophil extracellular traps, and complement activation. 23 Activation of the complement cascade results in elevated levels of C3b, leading to the formation of the membrane attack complex (MAC) and further endothelial damage.7,24,25 The damaged endothelium also leads to the release of tissue factor, which binds to factor VIIa and von Willebrand factor, and leads to platelet activation and microthrombi formation. Depletion of nitric oxide is also believed to play a crucial role in the development of the prothrombotic state and platelet microthrombi seen in TA-TMA. 26
One possible theory of why TA-TMA develops after a transplant is explained by the “three-hit hypothesis,” which states that multiple hits or risk factors are necessary for a patient to develop TA-TMA (Figure 1). 27 Several intrinsic risk factors can make an individual susceptible to developing TA-TMA (first hit). Then, the intensive chemotherapy and total body irradiation (TBI) used for conditioning are believed to be significant inciters for endothelial damage (second hit).28–31 Following endothelial injury, a third and final hit is thought to be necessary to develop the clinical manifestations seen in TA-TMA, 27 which may be from a variety of causes such as use of calcineurin inhibitors, GVHD, or infections.
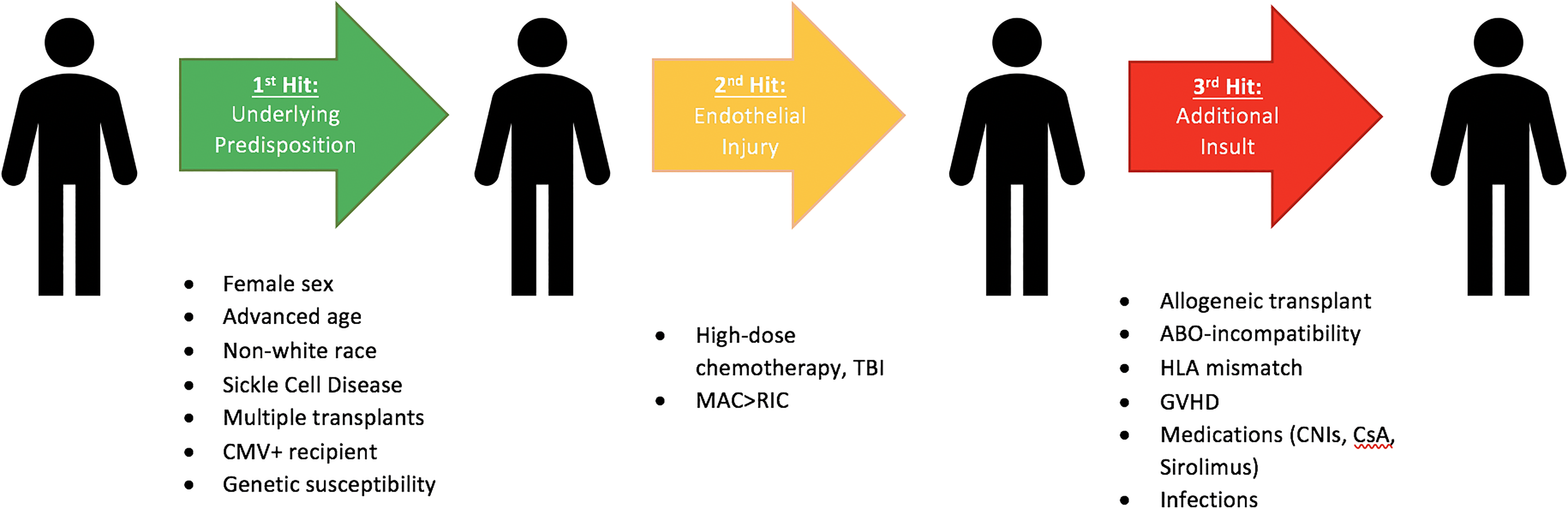
The three-hit hypothesis depicts the development of transplant-associated thrombotic microangiopathy (TA-TMA) and the risks or “hits” that predispose patients. Abbreviations: CMV, cytomegalovirus; CNI, calcineurin inhibitors; CsA, cyclosporine A; GVHD, graft-versus-host disease; HLA, human leukocyte antigen; MAC, myeloablative conditioning; RIC, reduced intensity conditioning; TBI, total body irradiation.
Risk Factors
Risk factors associated with TA-TMA can be categorized into intrinsic risk factors that are present prior to the transplant and risk factors that develop due to the transplant.
Intrinsic Risk Factors (Present Before the Transplant)
Females seem to be at increased risk of developing TA-TMA based on multiple reports, although the reason is unclear.32–35 Additionally, nonwhite patients, particularly African Americans, are more likely to develop TA-TMA and have a more severe disease with high mortality.36,37 Interestingly, these demographics are similar to other TMAs with a female predominance in both complement-mediated TMA (CM-TMA) and TTP, and increased incidence in black patients in TTP.38,39 Advanced age is also a risk factor.32,34,40,41 One large study found that although adults and children ≤18 years old had similar rates of developing TA-TMA, adults were more likely to have severe disease. 9 Another study found that older adults ≥50 years old were significantly more likely to develop TA-TMA than those <50 years old (HR 5.17, P = .004). 41 One study found that patients with sickle cell disease are more likely to develop TA-TMA compared to those without sickle cell disease (13% vs 2%) after adjusting for multiple variables. 42 Additionally, genetic susceptibilities from either the donor or recipient can predispose an individual to TA-TMA. A prospective study of 77 patients undergoing HSCTs found that 65% who developed TA-TMA had gene variants typically associated with CM-TMA compared to only 9% who did not develop TA-TMA. 36 There was a higher number of gene variants in nonwhite patients, which may explain the higher incidence of TA-TMA in African Americans. 36 Another study demonstrated that complement regulatory gene variants can also be transferred from the donor to the recipient. 43 CMV-positive serology of the recipient is also a potential risk factor. 44
Transplant-Related Risk Factors
Patients undergoing allogeneic HSCTs are significantly more likely to develop TA-TMA than those undergoing autologous HSCTs. 45 ABO incompatibility and human leukocyte antigen (HLA) mismatch are risk factors and may account for the increased rates of TA-TMA in allogeneic transplants.31,44,46 Prior history of transplant or tandem transplants also predispose patients to TA-TMA. 37 The type of conditioning regimen also matters as myeloablative conditioning is associated with higher rates of TA-TMA than reduced intensity conditioning. 47 Acute GVHD along with agents used for GVHD prophylaxis such as cyclosporine A and tacrolimus especially in combination with sirolimus are also potential triggers.30,40,46,48,49 Patients with steroid-refractory acute GVHD and grade 2 or higher acute GVHD are more at risk. 50 Several studies have found elevated serum markers of endothelial damage and membrane attack complex, such as sC5b-9, BBPlus, and ANG-2, at the onset of acute GVHD and concurrent development of TA-TMA.41,51 Additionally, survival is worse in patients who have both acute GVHD and TA-TMA compared to patients with acute GVHD or TA-TMA alone (median OS 5.6 months vs 55.4 months vs 7.6 months, P < .0001). 50 Lastly, active infections, such as cytomegalovirus, adenovirus, BK virus, and invasive aspergillosis have also been associated with endothelial injury and TA-TMA.30,31,52–54
Clinical Features
Most cases of TA-TMA occur within 100 days of HSCT, with one large study showing the onset between 9 and 721 days.44,55,56 Endothelial dysfunction leads to inflammatory and coagulation responses and can potentially affect any organ system (Figure 2), the kidneys being the most commonly involved.55–57 TA-TMA can also have a more dramatic presentation with MODS associated with high morbidity and mortality.45,58,59 Clinicians must therefore maintain a high index of suspicion for TA-TMA if any of the screening clinical or laboratory parameters indicate TA-TMA.
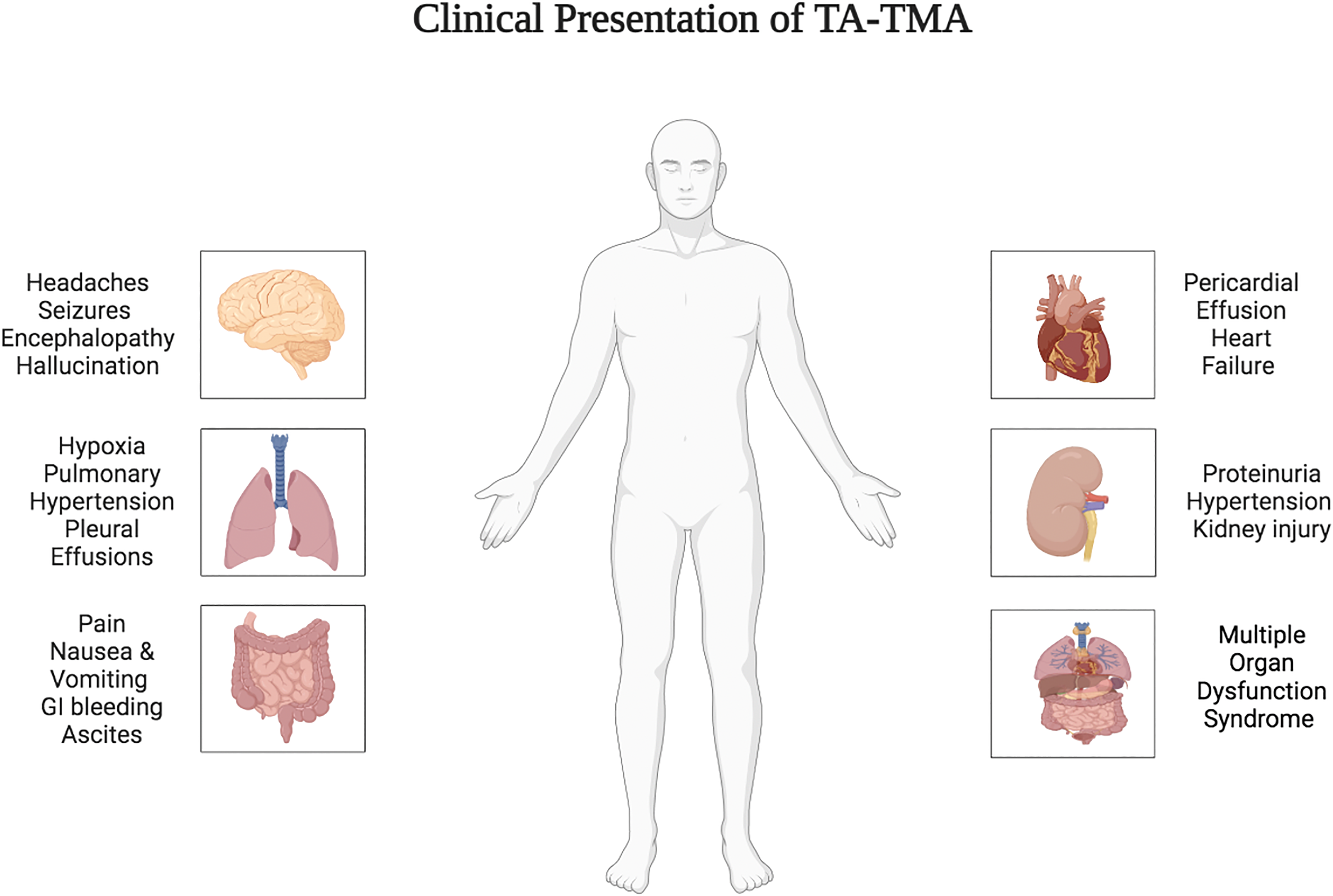
Clinical manifestations of TA-TMA by the organ system.
Renal Manifestations
Hypertension and proteinuria have been identified as early biomarkers of TA-TMA onset, present up to 14 days prior to the diagnosis. 60 Although new onset of hypertension can be common after transplantation from the use of calcineurin inhibitors or steroids, refractory hypertension or the need for multiple blood pressure medications should prompt evaluation for TA-TMA. In one small study, patients with TA-TMA were found to require a median of 6 (3-8) blood pressure medications for their hypertension. 60 In contrast, creatinine elevation is considered a late marker and reliance on the creatinine value alone can lead to a missed diagnosis. 7 Renal dysfunction has also been implicated as a poor prognostic indicator in patients with TA-TMA. 7 Renin–angiotensin–aldosterone system (RAAS) activation may also lead to electrolyte derangements such as hypokalemia. 61 Furthermore, proteinuria may lead to depletion of intravascular volume and cause systemic edema. In critically ill patients, a decreasing urine output along with low albumin levels can indicate a worsening course in the disease process.
Gastrointestinal
The presence of severe abdominal pain, nausea, vomiting, gastrointestinal bleeding, and ascites should raise suspicion for intestinal TMA (iTMA). Intestines are the second most frequently affected organ in TA-TMA accounting for up to 53% of patients in one study. 62 iTMA is associated with poor survival in HSCT patients and is often preceded by a diagnosis of GVHD. 63 Frank gastrointestinal bleeding or ileus may be the only obvious manifestations in a critically ill patient. When circulatory collapse occurs along with a significant decline in hemoglobin, hemorrhagic shock needs to be considered.
Cardiopulmonary
Cardiopulmonary manifestations of TA-TMA usually present with respiratory distress and hypoxemia because of underlying pulmonary arteriolar hypertension (PAH) and diffuse alveolar hemorrhage (DAH). Chest pain, dyspnea and tachycardia may be the initial symptoms and hypoxia may follow thereafter. DAH may additionally present with hemoptysis and a drop in hemoglobin. Prompt diagnosis is essential due to high mortality rates. 64 Endothelial injury in pulmonary vasculature can also lead to progressive right ventricular dysfunction. 65 In a prospective study performed by Lerner et al, up to 45% of patients diagnosed with TA-TMA had evidence of pericardial effusions on echocardiogram with one-third of these patients having moderate-severe effusions. 66 Recurrent pericardial effusions after medical or surgical interventions should raise suspicion for underlying TA-TMA. 67
Neurologic
While neurological toxicity is frequently associated with other TMAs (like TTP and complement-mediated TMA), it is not commonly reported in TA-TMA. 68 Neurological symptoms, including seizures and mental status changes, can indicate the presence of cerebral vasculopathy leading to intracranial hemorrhage, iron deposition, and posterior reversible cerebral encephalopathy. 68 A pediatric case with TA-TMA-associated refractory epileptic seizures and permanent neurological deficits has also been described in the literature. 69 Sickle cell disease is associated with chronic inflammation and endothelial dysfunction, which may make these patients especially susceptible to cerebral vasculopathy leading to posterior reversible cerebral encephalopathy after HSCT. 70
Multiorgan Dysfunction Syndrome
TA-TMA can often progress quickly to severe MODS requiring escalation of care in an intensive care unit. MODS may include one or more of the following: >50% reduction in glomerular filtration rate; a need for invasive or noninvasive positive pressure ventilation for 24 hours or more; pulmonary hypertension diagnosed by cardiac catheterization or echocardiogram; significant pericardial effusion requiring medical or surgical intervention; severe hypertension requiring multiple antihypertensives; seizures or altered mentation; gastrointestinal bleeding or strictures requiring an intervention. Severe organ dysfunction is often irreversible at this point and morbidity and mortality rates are high. Early detection and treatment are thus needed.
TMA After Solid Organ Transplantation
Thrombotic microangiopathy as a complication of tacrolimus therapy has been described in 4 individuals who received orthotopic liver transplants at the Western Australian Liver Transplantation Service from May 1994 to December 2010. All patients improved clinically with early discontinuation of tacrolimus and use of plasma exchange in 3 patients. 71 However, TA-TMA is also now recognized as a distinct entity in solid-organ transplant patients with complement activation as the main driving factor. 72 In a study of 129 patients who underwent liver transplants, ABO incompatibility was an independent risk factor for TA-TMA with a considerably higher incidence than the overall group (37.9% vs 10.1%). 73 The majority of cases occur after renal transplantation but some cases of TA-TMA have also been reported after liver, lung, and intestinal transplant.74–76 Prior to the complement inhibitor therapy era, mortality rates were high. 77 A meta-analysis described 17 solid-organ and 9 HSCT patients who developed TA-TMA and were subsequently treated with eculizumab. 72 The median interval to diagnosis (10 vs 68 days) and treatment (22 vs 150 days) with eculizumab was much shorter in solid-organ patients when compared to the HSCT patient cohort. Solid-organ transplant patients were also older on average (35 vs 7 years). Even though fewer patients received induction therapy and other treatment modalities like plasma exchange, all solid-organ transplant patients experienced complete resolution after eculizumab. This may suggest the importance of early diagnosis and treatment initiation while adding to the data on the successful use of eculizumab in adult patients with TA-TMA.
Screening for TA-TMA
Within the first 100 days after HSCT, patients may be in the ICU for a variety of early and late complications. 78 It may be particularly difficult to recognize TA-TMA in these patients due to multiple derangements in their labs and clinical picture. Following an established algorithm to screen for TA-TMA is therefore recommended. 45 An expert consensus panel from 4 international transplant societies recently published guidelines recommending screening practices for TA-TMA in all patients within the first 100 days of allogeneic HSCT and autologous HSCT in recipients with an underlying diagnosis of neuroblastoma. 18 Weekly CBC, LDH, random urine protein to creatinine ratio (rUPCR), blood smear for schistocytes, and blood pressure measurements should be obtained. 18 A positive screen of 3 or more of the following features indicates further testing: anemia, thrombocytopenia, elevated LDH, schistocytes, refractory hypertension, and proteinuria. 18 An organ system-based evaluation is needed to rule out other differential diagnoses, including but not limited to infections, drug or radiation-induced toxicity, GVHD, hepatic sinusoidal obstruction syndrome (SOS), disseminated intravascular coagulation (DIC), TTP, and engraftment syndrome 8 (Figure 3).
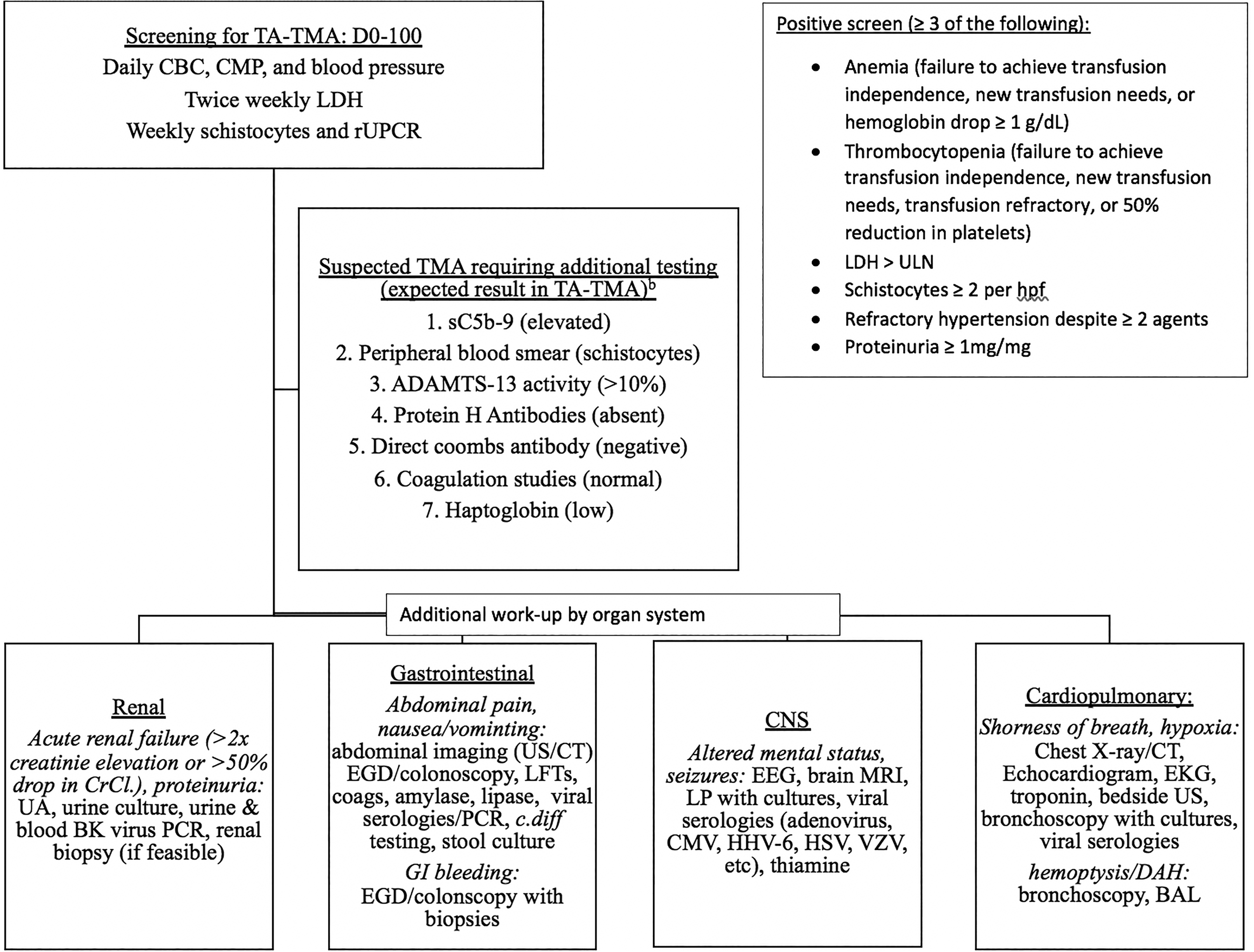
TA-TMA screening and initial evaluation by the affected organ systems in the critical care patient. Abbreviations: BAL, bronchoalveolar lavage; BP, blood pressure; CBC, complete blood count; c.diff, clostridium difficile; CMP, comprehensive metabolic panel; CMV, cytomegalovirus; coags, coagulation studies; CT, computed tomography scan; DAH, diffuse alveolar hemorrhage; EEG, electroencephalogram; EGD, esophagogastroduodenoscopy; EKG, electrocardiogram; HHV, human herpesvirus; hpf, high powered field; HSV, herpes simplex virus; LDH, lactate dehydrogenase; LFT, liver function tests; LP, lumbar puncture; MRI, magnetic resonance imaging; PCR, polymerase chain reaction; rUCR, random urine protein-creatinine ratio; UA, urinalysis; ULN, upper limit of normal; US, ultrasound; VZV, varicella zoster virus.
Diagnostic Criteria and Risk Stratification
Histological diagnosis remains the gold standard for establishing the diagnosis of TA-TMA 79 ; however, among ICU patients with suspected TA-TMA, histologic diagnosis through measures such as renal biopsy or endoscopy may prove hazardous or impractical. Therefore, given the importance of early and expeditious diagnosis of TA-TMA, it is essential to maintain a high index of suspicion for TA-TMA when cardinal findings such as hypertension with renal failure develop in this patient population. The relatively unique combination of recalcitrant or refractory hypertension in the setting of multiorgan system dysfunction may help to distinguish TA-TMA from more common infectious complications of HSCT which typically manifest as inappropriate vasodilation and hypotension. Therefore, when escalating hypertension occurs in the setting of progressive organ dysfunction following HSCT, TA-TMA should be further investigated as a possible diagnosis.
Over the last 2 decades, multiple clinical criteria have been proposed to help physicians in diagnosing TA-TMA in HSCT patients (see Table 1). The older proposed criteria by the Bone Marrow Transplant Clinical Trials Network (BMT-CTN) and the International Working Group of the European Group for Blood and Bone Marrow Transplantation (IWG) have been replaced by the more recent and novel criteria.7,55–57,80,81 A retrospective analysis recognized the limited sensitivity of the BMT-CTN and IWG criteria based on their need for abnormal serum creatinine and the presence of more than 4% schistocytes, respectively. 82 Furthermore, higher haptoglobin levels have been associated with poor survival in TA-TMA patients, thus questioning the inclusion of low haptoglobin in the diagnostic criteria. 7 Two of the criteria also require a negative Coombs test as a diagnostic criterion.55,81 Although a positive Coombs is not expected in patients with TA-TMA, there are many reasons why a patient may have this lab abnormality after HSCT; therefore, a positive Coombs alone should not exclude the diagnosis of TA-TMA. The diagnostic criteria put forth by Uderzo and Jodele et al established the importance of identifying proteinuria and hypertension as early markers of TA-TMA.7,81 The role of complement in the pathophysiology of TA-TMA is also highlighted by the inclusion of elevated sC5b-9 levels.7,81
Different Available Diagnostic Criteria for TA-TMA. Abbreviations: BMT-CTN, Bone Marrow Transplant Clinical Trials Network; IWG, International Working Group of the European Group for Blood and Bone Marrow Transplantation; COH, City of Hope; CTN, blood and marrow transplant clinical trials network; HPF, high-power field; LDH, lactate dehydrogenase; TA-TMA, transplant-associated thrombotic microangiopathy.
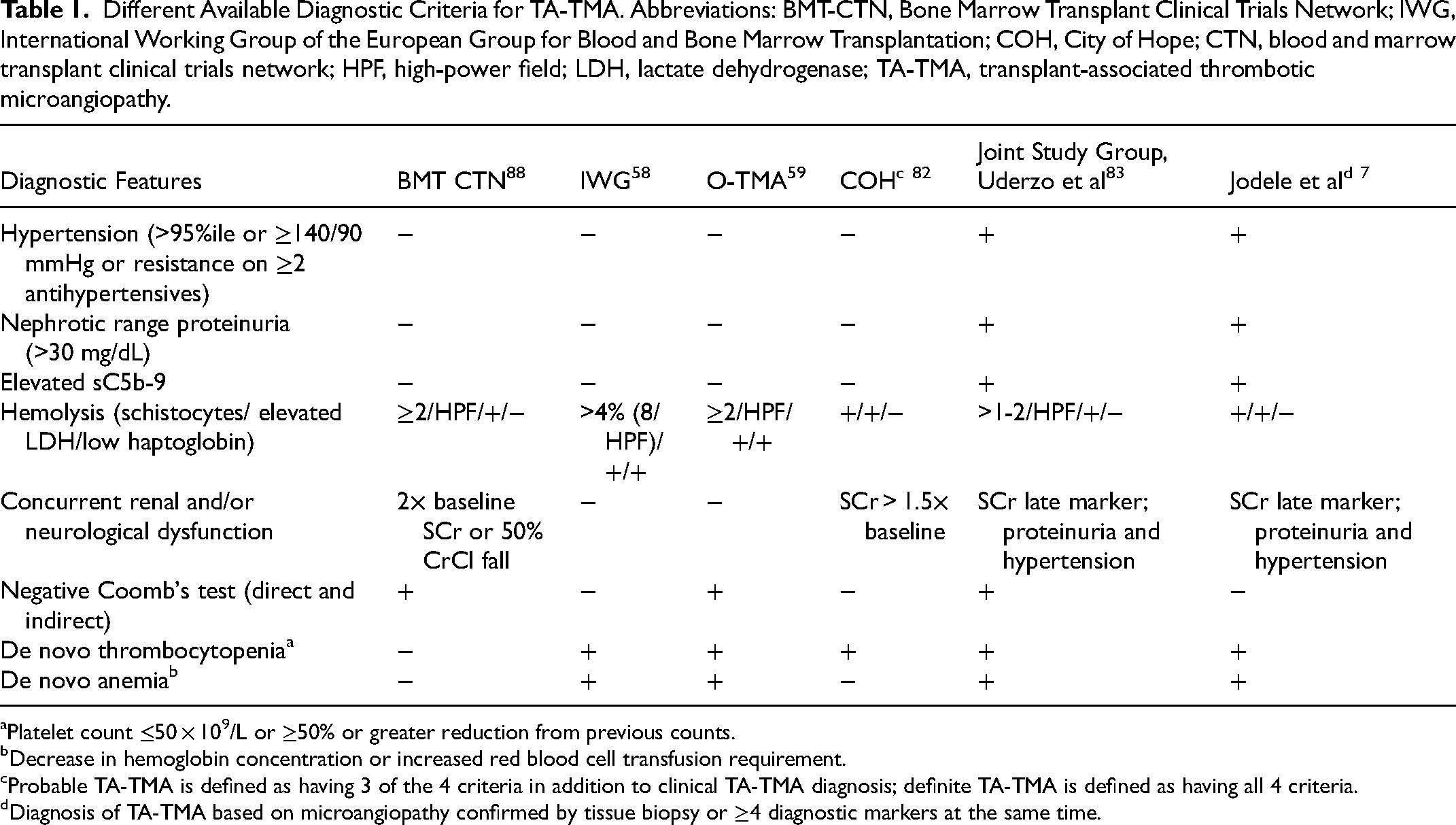
Platelet count ≤50 × 109/L or ≥50% or greater reduction from previous counts.
Decrease in hemoglobin concentration or increased red blood cell transfusion requirement.
Probable TA-TMA is defined as having 3 of the 4 criteria in addition to clinical TA-TMA diagnosis; definite TA-TMA is defined as having all 4 criteria.
Diagnosis of TA-TMA based on microangiopathy confirmed by tissue biopsy or ≥4 diagnostic markers at the same time.
The Jodele criteria are the most useful because they do not rely on any one clinical criterion and all criteria do not have to be met at the same time point. It requires at least 4 of 7 criteria to be met on 2 different time points within 14 days including anemia, thrombocytopenia, LDH ≥ upper limit of normal (ULN), schistocytes, hypertension, sC5b-9 ≥ ULN, and rUPCR ≥ 1 mg/mg. An expert consensus panel modified the Jodele criteria to include additional definitions of anemia and thrombocytopenia. 18 An important limitation of the Jodele criteria is that was developed and studied in children and young adults and so its utility in older adults is not well defined. It also requires sC5b-9 testing which is not widely available. For many centers, it is a send-out test that may take days or weeks to come back, or they may not have the test at all. As measuring sC5b-9 levels has become more important in the diagnosis, prognosis, and monitoring during treatment in TA-TMA, transplant centers should have this test readily available to prevent delays in diagnosis and treatment. Figure 4 shows the fully modified Jodele criteria recommended by the consensus panel of experts from 4 international transplant societies.18,64
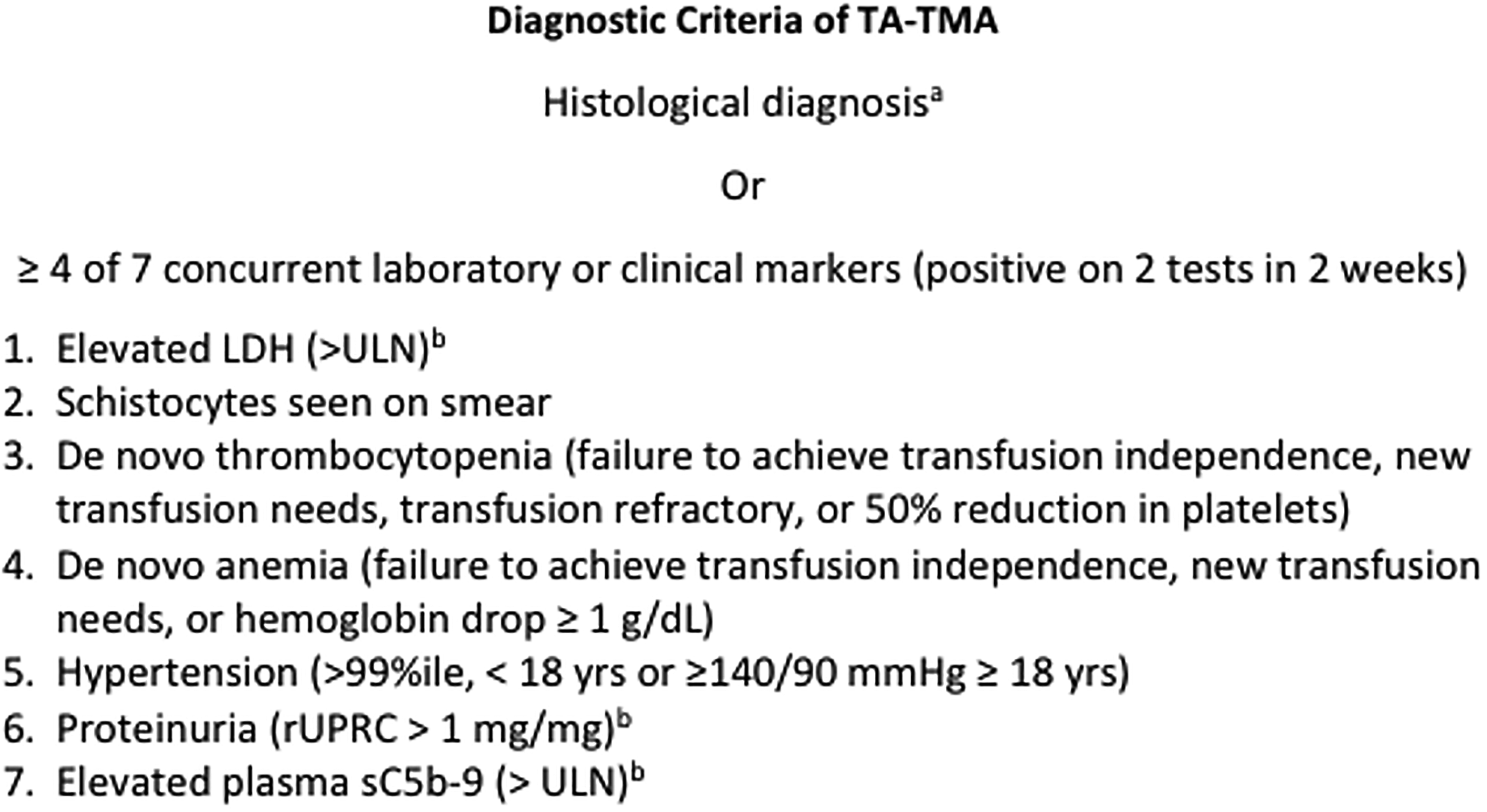
Fully modified Jodele criteria for TA-TMA recommended by the consensus panel of experts from 4 international transplant societies. a Characterized by mucosal hemorrhages, loss of glands, intraluminal schistocytes, intraluminal fibrin, intraluminal microthrombi, endothelial swelling, endothelial separation from the membrane, and total denudation of mucosa. b High-risk features (also include organ dysfunction, concurrent grade 2-4 acute graft-versus-host disease or viral infections). Abbreviations: LDH, lactate dehydrogenase; rUCR, random urine protein-creatinine ratio; ULN, upper limit of normal.
Patients were previously classified as having high-risk TMA in the presence of either both proteinuria (>30 mg/dL) and elevated serum C5b-9 (>244 ng/mL) or one of these with evidence of organ dysfunction. 83 The recent expert consensus expanded the definition of high risk to include the presence of any of the following: rUPCR (>1 mg/dL), elevated sC5b-9, organ dysfunction, LDH ≥ 2 times ULN, concurrent grade II-IV GVHD, or concurrent infections. 18 Patients who are critically ill in the ICU will meet these criteria and will likely benefit from early complement inhibitor therapies. 59
Treatment Strategies
By the time patients with TA-TMA require intensive care, they may unfortunately be relatively late in the disease course. TA-TMA may progress quickly to severe MODS, so early supportive care, infection management, and stabilization of the patient are of paramount importance. 59 Withdrawal of calcineurin inhibitors or sirolimus should be considered as they can exacerbate TA-TMA,55,84–87 but this may be challenging if concurrent aGVHD is present. Immunosuppressive medication decisions should be made in coordination with the transplant team. Currently, there are no therapies approved by the Food and Drug (FDA) for the treatment of TA-TMA. Patients considered high-risk as defined above should be strongly considered for early intervention on clinical trial if available or with off-label complement inhibitors. Once patients progress to the later stages of TA-TMA, treatment may fail to reverse the process of organ damage and outcomes are poor. 16 Due to a lack of consensus on how to treat these patients, algorithms have been proposed by some groups.8,27,88 Here, we review treatment considerations in the ICU setting.
Hemodynamic Considerations
Control of Blood Pressure
The frequent combination of impaired renal function and compromised intestinal integrity or bleeding seen with TA-TMA in the ICU have the potential to make blood pressure management more challenging. If there is a concern for GI involvement or frank evidence of GI bleeding, the use of the enteral route of medication administration may not be practical and therefore antihypertensive therapy may need to be administered by the intravenous route. Additionally, the propensity for renal involvement of patients admitted to the ICU with TA-TMA can make the choice of an antihypertensive agent difficult. While there is reason to believe that endothelial injury may lead to activation of the RAAS, 89 use of angiotensin-converting enzyme (ACE) inhibitors in critically ill patients is often problematic due to the risk of further decline in renal function and the potential for electrolyte derangements such as hyperkalemia. The limited intravenous options (enalapril only) in this class of drugs pose further challenges to safe and effective blood pressure control with these agents. Angiotensin receptor blockers (ARB) are another consideration; however, similar challenges regarding renal function impairment, electrolyte disturbances, and lack of IV formulation arise. Calcium channel blockers offer a reasonable alternative as these agents are considered safe in the setting of impaired renal function and are not typically associated with electrolyte derangements. Furthermore, there are multiple intravenous dihydropyridines available such as nicardipine and clevidipine which can be titrated as a continuous infusion in the ICU setting for more resistant hypertension. If there is a reason to suspect elevated pulmonary arterial pressures or right ventricular strain, choosing antihypertensive agents that also function to reduce afterload may be beneficial. The proteinuria that is characteristic of TA-TMA nephropathy has the potential to reduce serum oncotic pressure and lead to loss of circulating volume from the intravascular space. Caution should therefore be exercised with diuretic use as these agents may produce detrimental depletion of intravascular volume and further decline in renal function. Lastly, if there is a concern for the involvement of the pulmonary vasculature or right ventricular dysfunction, nitrates should be avoided when managing blood pressure due to right ventricular preload dependence in these circumstances.
Pulmonary Arteriolar Hypertension
The development of PAH due to microangiopathic insult to the pulmonary vasculature is a well-described complication of TA-TMA and mortality among these patients is unfortunately high.45,90 As with any type of pulmonary hypertension, right heart catheterization would be considered the gold standard for confirmatory diagnosis when pulmonary involvement of TA-TMA is suspected. If placement of an indwelling pulmonary artery catheter for invasive hemodynamic assessment is feasible within the ICU setting, this additional measure may prove helpful. However, noninvasive assessment with Doppler echocardiography is often more readily available. In the acute setting, the presence of pericardial effusion, enlargement of the right atrium, and degree of septal displacement all portend a poor prognosis. 91
Pericardial Effusion
Accumulation of fluid within the pericardial space is another important manifestation of TA-TMA in critically ill patients. 66 HSCT patients with TA-TMA are more likely to have pericardial effusions requiring intervention such as pericardiocentesis or pericardial window in the first 100 days following transplant than HSCT patients without TA-TMA. 45 Unfortunately, the clinical presentation and symptomatology associated with pericardial effusion are often vague and nonspecific, which makes prompt and early detection important. Complaints such as chest discomfort or dyspnea and findings such as unexplained tachycardia or enlargement of the cardiac silhouette on routine chest x-rays should trigger an expedited echocardiographic assessment. Point-of-care ultrasound (POCUS) assessment has also been shown to be fast and effective in the diagnosis and treatment of clinically significant pericardial effusion. 92 Thus, if there is suspicion of pericardial effusion in a critically ill HSCT patient with known or suspected TA-TMA, bedside ultrasound can often be employed as an efficient diagnostic tool. If pericardial effusion is detected, additional findings such as diastolic right ventricular collapse, systolic right atrial collapse, and dilation of the IVC with absent respiratory variation may indicate tamponade physiology and the need for emergent intervention. 93
Fluid Management Considerations
When caring for a critically ill patient with TA-TMA, there is the potential for right ventricular performance to be significantly impacted by fluctuations in both preload and after-load. Fluid management therefore becomes quite challenging depending upon the extent of organ systems involved. For instance, if pulmonary involvement of TA-TMA has led to increased pulmonary arterial pressures or right ventricular dysfunction, caution should be exercised to avoid overly aggressive IV fluid administration as excessive preload in these circumstances may precipitate right ventricular failure. Conversely, if gastrointestinal involvement of TA-TMA has led to clinically significant blood loss, there is also the potential for intravascular volume depletion, leading to a decline in right ventricular preload and subsequent drop in RV output. The degree and severity of renal impairment associated with TA-TMA will also have major implications for fluid management strategies in the ICU. Patients may have difficulty mobilizing fluid from the extravascular spaces due to urinary protein loss and are therefore at risk of intravascular volume depletion. Fluid shifts secondary to the nephrotic state may also contribute to loss of intravascular volume. Furthermore, if declining renal function leads to dropping urine output, the patient may quickly become volume-overloaded, and hemodialysis may be needed.
Respiratory Failure and Ventilatory Support
The spectrum of pulmonary complications related to TA-TMA is quite broad. In addition to the pulmonary vasculopathies discussed previously, DAH is another well-known complication of TA-TMA. Both conditions, whether occurring independently or concomitantly, can cause hypoxemia and respiratory failure. Alveolar hemorrhage may occur for a variety of reasons following HSCT including infection, drug toxicity, GVHD, thrombocytopenia, and other coagulopathies. Accepted criteria for diagnosis of DAH include radiographic evidence of diffuse alveolar infiltrates, increased alveolar to arterial oxygen gradient, the presence of a restrictive ventilatory defect, absence of infectious etiology, and progressively bloody effluent from sequential alveolar lavage. 94 This condition may be an under-recognized facet of TA-TMA as autopsy studies suggest that as much as 24% of pediatric patients who died of TA-TMA have postmortem evidence of DAH and that among those patients with TA-TMA associated DAH, mortality can be as high as 100%. 95 Depending upon the degree of hypoxemia, patients manifesting DAH often require intubation and mechanical ventilatory support. HSCT patients with TA-TMA are more likely to require ventilatory support. 45 The presence of a secure airway may help facilitate bronchoscopic evaluation if respiratory status remains tenuous. Following intubation, a low tidal volume strategy may be appropriate if there is evidence of diffuse alveolar injury and refractory hypoxemia. Furthermore, higher tidal volumes may produce higher intrathoracic pressures which can subsequently lead to a decline in right ventricular performance through increased transmural pressure (defined as pulmonary arterial pressure minus intrathoracic pressure). 96 Positive end-expiratory pressure (PEEP) can be utilized to help augment alveolar recruitment in the setting of DAH with associated hypoxemia. However, PEEP has the potential to increase pulmonary vascular resistance (PVR) and decrease right ventricular preload, which can be detrimental in the setting of TA-TMA-associated PAH. Thus, the detrimental interplay between pulmonary arterial vasculopathy and DAH can prove fatal if hypoxia and associated vasoconstriction are allowed to progress. The primary role of mechanical ventilation in TA-TMA is to help mitigate this vicious cycle through alveolar recruitment and protective ventilation strategies and to facilitate the completion of necessary diagnostics if possible.
Pleural Effusions
Pleural effusions are common following HSCT, occurring in up to 9.9% of transplant recipients in 1 year and are known to occur for a variety of reasons including infection, hypervolemia, and GVHD among others. 97 TA-TMA appears to represent a significant risk factor for pleural effusion requiring intervention, as it occurs more frequently in HSCT recipients with TA-TMA than among HSCT patients without TA-TMA. 45 While routine chest x-ray and CT imaging can detect relatively small pleural effusions, bedside ultrasound remains a quintessential tool for fast and effective management of pleural effusions in the ICU. The ability to image the pleural space at the bedside and in real time makes ultrasound a preferred modality for monitoring pleural effusions and determining the feasibility of drainage. This is particularly true with critically ill patients for whom repositioning or transport out of the ICU is not feasible. Thoracic ultrasound assessment of pleural fluid volume has been shown to correlate with CT imaging 98 and has been shown to have vastly superior sensitivity and specificity to routine chest radiography in the detection of pleural effusions as well as other parenchymal abnormalities.
Therapeutic Options
Therapeutic Plasma Exchange and Rituximab
As we gain a better understanding of the pathophysiology of TA-TMA, it is evident that it is not primarily an autoantibody-driven process. TTP with severe ADAMTS13 deficiency is extremely rare in these patients.99,100 As a result, therapeutic plasma exchange (TPE) has fallen out of favor as the treatment of choice. 101 In multiple studies, treatment with TPE has demonstrated that it has a low response and a high mortality rate. 55 A large retrospective study involving 82 patients with TA-TMA from the University People's Hospital demonstrated a response rate to TPE of 52.8%. Overall survival was only 20% at 100 days and 15% at 1 year. Those with higher grade GVHD of III-IV compared to 0-II were associated with a worse response. 102 Similarly, another large study of 121 patients treated with TPE demonstrated a 37% response rate with a mortality rate of 79%. Some studies have even shown that TPE may be detrimental to patient outcomes.37,55
The role of rituximab, an anti-CD20 monoclonal antibody, has similarly been elucidated to eliminate autoantibodies which may develop in other subtypes of TMA.103,104 Most studies which have historically suggested rituximab as a beneficial treatment option for TA-TMA had low ADAMTS13 which brings their initial diagnosis into question. 105 TPE and rituximab may be useful in the setting of circulating factor H (CFH) autoantibodies or if TTP has been diagnosed with an ADAMTS13 level of 10% or less. 106 Therefore, it is important to test for CFH antibodies and ADAMTS13 activity and inhibitor levels as soon as thrombotic microangiopathy is suspected. While waiting for these tests to result, clinical judgment should be used. Although generally not recommended in TA-TMA, it may be reasonable to initiate these therapies if the patient is at high risk for autoimmune TMA, such as if they have a history of TTP or CFH autoantibodies or systemic lupus erythematosus (SLE).
Eculizumab
The terminal complement blocker, eculizumab, was studied as a first-line treatment for high-risk TA-TMA in a cohort of 64 pediatric patients with high-risk TA-TMA. 16 Patients were considered high risk if they had elevated soluble terminal complex activity (sC5b-9) and nephrotic range proteinuria (≥30 mg/dL on 2 occasions or random urine protein/creatinine ratio ≥2 mg/mg). It is noteworthy that this is the only large prospective trial evaluating the benefit of eculizumab in patients with TA-TMA. The study showed a response rate of 64% and survival of 66% 1 year after HSCT which is much better compared to historical outcomes. Higher sC5b-9 prior to treatment initiation was associated with poor responses and survival. The presence of end-organ damage and intestinal bleeding appeared to correlate with poor response to eculizumab. Overall response rates have also exceeded 50% in other smaller studies including in adult cohorts.107–110
While smaller retrospective studies had administered the dose used for CM-TMA (weekly induction with 900 mg for 4 weeks, followed by 1200 mg biweekly in adults ≥40 kg), Jodele et al recognized the variability in eculizumab's clearance and the need for dynamic dosing in individuals with TA-TMA requiring eculizumab trough levels and CH50 monitoring.16,111 Using this approach, initial dosing should be weight-based with patient's weight <10 kg, 10-39 kg, and ≥40 kg receiving 300 mg, 600 mg, or 900 mg IV doses, consecutively. If sC5b-9 is elevated, a loading dose should initially be given every 72 h with a goal of reaching eculizumab trough levels ≥100 μg/mL, CH50 suppression <10%, and normalization of sC5b-9 or ≥5 doses. Subsequently, or if sC5b-9 is normal from the start of therapy, doses should be given weekly for at least 4 weeks followed by maintenance every 1 to 2 weeks, followed by a taper. Discontinuation of therapy should be considered when a patient is at the lowest taper dose (300 mg for patients 10-20 kg and 600 mg for >20 kg) for 2 cycles and has sustained normal sCb5-9 with no signs of hematological TA-TMA or MODS. 16
Complement-blocking therapies are associated with a high risk of infections with encapsulated bacteria. It is extremely important to administer vaccination along with antibiotic prophylaxis against Neisseria meningitides at the time of initiating eculizumab. 112 As HSCT patients may not respond to vaccination early post-transplant, antibiotic prophylaxis should be continued as per transplant institutional standards. Because of these risks, the Food and Drug Administration has mandated Solaris® (eculizumab) to implement the Risk Evaluation and Mitigation Strategy (REMS) program requiring certification of all providers administering eculizumab. 113
MASP-2 Inhibitor
The mannan-binding lectin-associated serine protease-2 inhibitor (MASP-2), narsoplimab (OMS721), is a novel selective complement inhibitor, which does not interfere with acquired or adaptive immunity. In a single-arm phase II study by Khaled et al, narsoplimab administered intravenously once weekly for a duration of 4 to 8 weeks demonstrated a durable response rate of 61%, defined by an improvement in labs and clinical status. 17 The study also demonstrated a 94% survival among responders at day 100. The adverse effects experienced by the study participants were not unusual for this high-risk immunocompromised population. 17
Defibrotide
Defibrotide is a polydeoxyribonucleotide with properties that can induce vasodilatation and lead to a reduction in vascular endothelial inflammation and macroangiopathic thrombosis, currently approved for the treatment of sinusoidal obstruction syndrome (SOS) in the United States. 114 Multiple studies that have studied TA-TMA patients treated with defibrotide (with or without other therapies) indicate a reassuring resolution rate of more than 60%.107,115,116 Bohl et al, however, observed that these initial response rates were not long-lasting and mortality rates continued to be high. 107 One small case series of 3 patients demonstrated a 100% response using low-dose defibrotide (<10 mg/kg/dose) in the treatment of TA-TMA. 117 This strategy may be considered for further study as a lower-cost option.
Current Clinical Trials
Consideration of clinical trials if available is strongly recommended for all patients diagnosed with TA-TMA. There are several ongoing multi-institutional clinical trials currently enrolling patients. Ravulizumab, a long-acting monoclonal antibody against C5, is currently under study in a phase III, randomized, multicenter trial for adults and adolescent patients (ClinicalTrials.gov NCT04543591) and in a phase III, single-arm study in pediatric patients (ClinicalTrials.gov NCT04557735) experiencing TA-TMA. Nomacopan (rVA576) is another second-generation C5-inhibitor currently enrolling pediatric patients with TA-TMA in an open-label, uncontrolled, multicenter study (ClinicalTrials.gov NCT04784455). Pegcetacoplan is a C3 inhibitor which is under investigation in a phase II clinical trial to evaluate its pharmacokinetics, pharmacodynamics, efficacy, and safety in patients with TA-TMA (ClinicalTrials.gov NCT05148299).
Conclusion
TA-TMA in the ICU patient can be challenging to recognize, diagnose, and treat. Refractory hypertension with multiorgan dysfunction may be a unique clinical presentation to alert the critical care physician of TA-TMA as a potential diagnosis. Stabilizing the patient while providing supportive care and early intervention with complement inhibitors are the cornerstones of treatment. Several large clinical trials utilizing promising next-generation complement inhibitors are currently underway.
Footnotes
Authors’ Disclosures
Ryo Nakamura—Omeros—consultancy and institutional research support (multicenter retrospective data collection project) and participating as a site PI for NCT05148299 by SOBI/Appelis. Azra Borogovac- Prime Education, LLC -honorarium.
The other authors have no disclosures or acknowledgments.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.