
Abstract
Introduction
Minimization of exposure to sedative agents is an important metric for any contemporary intensive care unit (ICU). 1 Unfortunately, during the early phases of the coronavirus disease-2019 (COVID-19) pandemic, many healthcare systems struggled with implementing existing sedation protocols. The reasons for these deviations were multifactorial, and included concerns around transmissibility, the high severity of disease, and the high patient volumes that overwhelmed systems. 2 Similar to literature from the pre-COVID era, 3 exposure to higher doses of sedatives to ensure deeper levels of sedation has been recognized as a strong independent predictor of mortality in COVID-19 patients. 4 Subsequent studies have further tried to understand the impact of the choice of different sedative agents on ICU-specific outcomes including mortality,5,6 duration of mechanical ventilation,6,7 and the incidence of delirium. 8 Unfortunately, most of these analyses were retrospective and categorized patients based on the primary sedative agent provided despite many patients receiving polypharmacy.5,7,8 This analytic approach without controlling for patient and disease severity variables may lead to misleading results and mask the true impact of the pharmacological agents under investigation. 9 Our objective was to investigate and elucidate the patterns of bedside sedation practices throughout four successive COVID-19 waves within a prominent US health system. Additionally, we assessed the influence of specific sedatives and analgesics on patient mortality across the COVID pandemic.
Materials and Methods
This was a retrospective cohort study with data collected from seven hospitals within a major healthcare system in Northeast Ohio. The study included all patients aged ≥18 years admitted to a medical ICU (MICU) with COVID-19 adult respiratory distress syndrome (ARDS) and requiring invasive mechanical ventilation (IMV). Real-time polymerase chain reaction (PCR) through nasal swabs was the standard of care in diagnosing SARS-CoV-2 virus in our health system. Patients were excluded if they were less than 18 years old, pregnant, or admitted to surgical, trauma, or cardiology ICU. All eligible patients admitted during the study period were included in the analysis. Patients were categorized based on the intubation day into four COVID-19 waves: first wave: March 1, 2020-May 31, 2020; second wave: June 1, 2020-October 15, 2020; third wave: October 16, 2020-February 28, 2021; and fourth wave: March 1, 2021-December 31, 2021. Data including demographics (age, gender, race, body mass index [BMI]), clinical characteristics (Acute Physiology and Chronic Health Evaluation [APACHE] III score, comorbidities, and ARDS severity according to the Berlin definition, 10 number of vasopressors), sedation requirements (number of sedatives per patient, type of sedative agent, and type of analgesic agent), and clinical outcomes (IMV duration in days, ICU length of stay [LOS], hospital LOS, and alive at hospital discharge) were extracted from the electronic health records (EHR) and internal clinical registry. Five percent of the ARDS severity data were initially missing and required a manual chart review for extraction to confirm that no data points were left unaccounted for by the end.
Normally distributed continuous variables were presented as mean and standard deviation (SD), and a one-way analysis of variance (ANOVA) test was used to examine the differences between the four groups. Nonnormal distributed data were presented as the median and interquartile range (IQR), and the Kruskal–Wallis test was used to examine the groups’ differences. Categorical variables were presented as counts and percentages, and the chi-square test or Fisher exact test was used to detect the significant differences between groups. Patients were considered to have received the sedative agent infusion if they received it for 20% or more of the total sedation time, to eliminate any infusions used for transient periods. An alluvial diagram was used to illustrate the temporal flow for each ARDS severity to different sedative agent groups and ultimately ending at the patient's final disposition (hospital survival vs death).
A multivariable logistic regression analysis was conducted to identify clinical variables independently associated with mortality considering various factors such as demographics (age, gender, race, BMI), comorbidities (hypertension, diabetes, obstructive lung disease, dialysis, coronary artery disease, dementia, transplant, malignancy, malnutrition, liver disease, stroke), and clinical factors (APACHE III, ARDS severity, and number of vasopressors). The selection of these covariates was based on a combination of clinical expertise, variables previously documented in the literature, 11 and the practicality of extracting the data. The study then examined the impact of different sedative and analgesic agents on mortality by entering the outcome probability in a second model, along with the total infused dosage. The aim was to observe the change in Nagelkerke R2 from the first to the second model. We conducted an assessment of regression assumptions, including linearity, the absence of multicollinearity, and the presence of outliers without violations. All statistical analyses were performed using R programming language version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/) with P level < 0.05 considered statistically significant. The study was reviewed and approved by the institutional review board (IRB) of the Cleveland Clinic Foundation (CCF-IRB # 14-1431). All procedures were in accordance with the ethical standards of the institutional IRB and with the Helsinki Declaration of 1975. Informed consent has been waived by the IRB due to the retrospective, non-interventional nature of the study. Our study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting. 12
Results
From March 2020 to December 2021, a total of 2394 patients required IMV due to COVID-19 ARDS in the included MICUs. Demographics, clinical characteristics, sedative requirements, and clinical outcomes are summarized in Table 1. The fourth wave accounted for the largest number of patients, comprising 44.8% of the total cases. During the fourth wave, patients exhibited a lower average age of 61 years (SD 15) and a lower percentage of males at 55%, in contrast to the average ages and male percentages observed in the preceding waves (first to third waves), which were 65 years (SD 13) and 62%, 65 years (SD 16) and 63.5%, and 68 years (SD 13) and 60.6%, respectively. The differences were statistically significant with P-values of <0.001 for age and 0.011 for male percentage. Hypertension emerged as the predominant comorbidity across all waves, reaching its peak prevalence during the third wave (88.1%), significantly higher than the prevalence in the other waves (ranging from 79% to 86.9%; P < 0.001). Diabetes mellitus (DM) and chronic obstructive pulmonary disease (COPD) displayed analogous patterns, with their highest prevalence recorded during the third wave (57.1% and 39.4%, respectively), contrasting with lower prevalence rates in other waves (DM 50%-53.8%, P = 0.024; COPD 30%-35%, P = 0.001). Similarly, coronary artery disease (CAD) reached its zenith during the third wave at 20.1%, whereas the prevalence in other waves ranged from 12.7% to 17.3%, signifying a significant difference (P = 0.001). The APACHE III score at admission did not show a statistically significant difference among the groups, with scores of 66.6 (SD 23.6), 68.9 (SD 23.6), 65.8 (SD 22.7), and 66.82 (SD 23.78) for the respective COVID-19 wave groups first to fourth; P = 0.37. ARDS severity exhibited a temporal increase from the first wave to the fourth wave, with rates of 22.4, 22.9, 27.2, and 34.3%, respectively (P < 0.001).
Demographics, Clinical Characteristics, Sedative Requirements, and Clinical Outcomes Over the Four COVID-19 Waves.
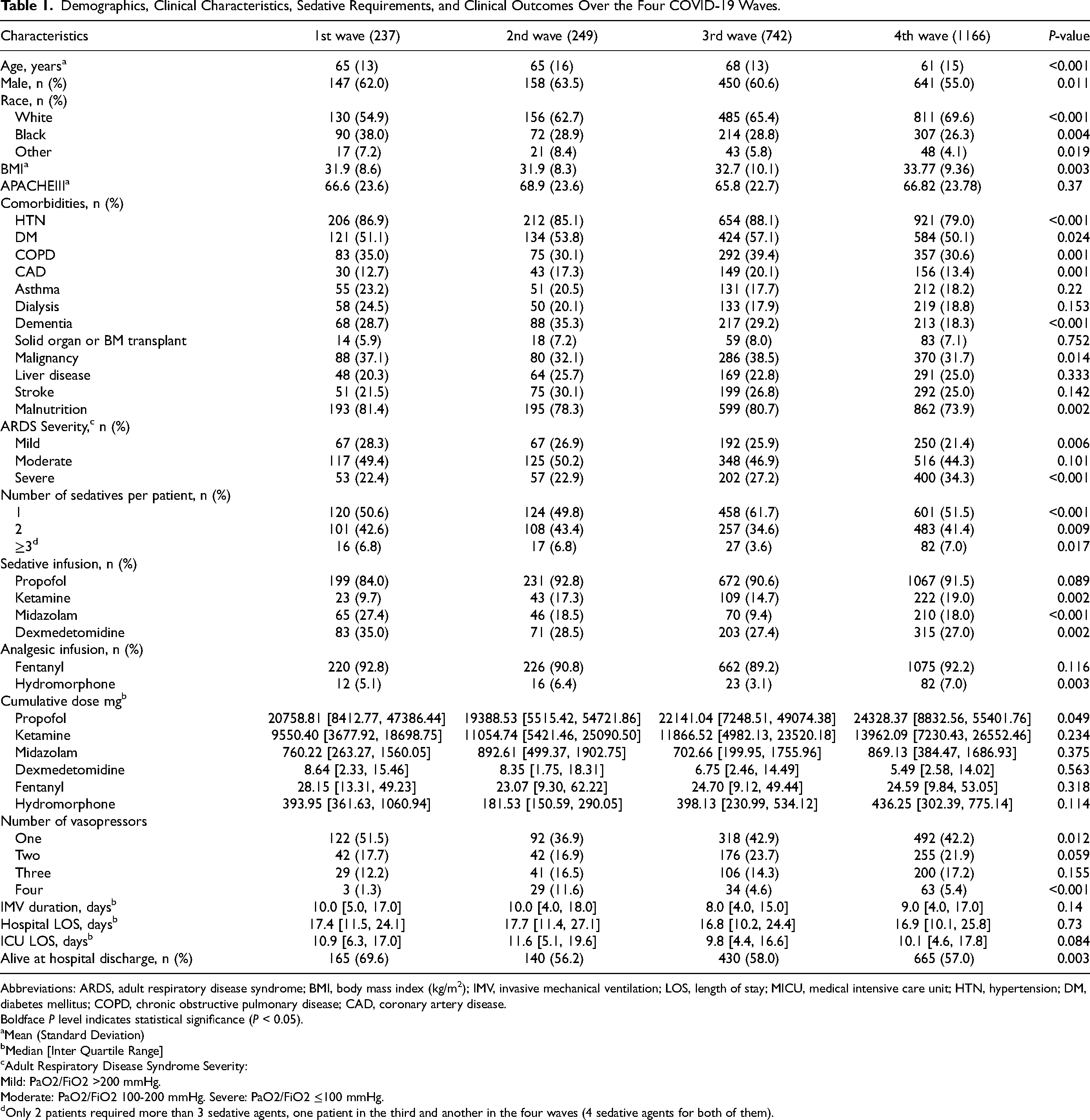
Abbreviations: ARDS, adult respiratory disease syndrome; BMI, body mass index (kg/m2); IMV, invasive mechanical ventilation; LOS, length of stay; MICU, medical intensive care unit; HTN, hypertension; DM, diabetes mellitus; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease.
Boldface P level indicates statistical significance (P < 0.05).
Mean (Standard Deviation)
Median [Inter Quartile Range]
Adult Respiratory Disease Syndrome Severity:
Mild: PaO2/FiO2 >200 mmHg.
Moderate: PaO2/FiO2 100-200 mmHg. Severe: PaO2/FiO2 ≤100 mmHg.
Only 2 patients required more than 3 sedative agents, one patient in the third and another in the four waves (4 sedative agents for both of them).
Propofol consistently remained the predominant sedative agent across all waves, accounting for 84, 92.8, 90.6, and 91.5% of cases, respectively (P = 0.089). Ketamine use increased with each subsequent wave (first [9.7%], second [17.3%], third [14.7%], and fourth [19%]; P = 0.002). Midazolam use varied throughout the waves and fluctuated after the first wave from 27.4% to 9.4% in the third wave and 18% in the second and fourth waves (P < 0.001). Less utilization of dexmedetomidine was noticed after the first wave and continued to decrease from 35% to 27-28% in subsequent waves (P = 0.002). There was a significant change in the use of sedation across the different waves, especially in moderate and severe ARDS where ketamine use replaced midazolam over time (Figure 1). Only a limited number of patients received more than two sedative agents, and this was notably less common during the third wave (3.6%) compared to the other waves (7%) (P = 0.017). However, it is worth noting that there was significant heterogeneity in drug use within this patient cohort (see Figure 1). Among the analgesic medications, Fentanyl was the primary agent in all four waves, with usage rates of 92.8, 90.8, 89.2, and 92.2%, respectively (P = 0.116). In contrast, the use of Hydromorphone was notably lower during the third wave at 3.1% compared to the first (5.1%), second (6.4%), and fourth (7%) waves, respectively (P = 0.003). The cumulative medication doses were assessed across the four COVID-19 waves. Among sedative agents, propofol (8412.77 to 47,386.44 mg), ketamine (3677.92 to 18,698.75 mg), midazolam (263.27 to 1560.05 mg), and dexmedetomidine (2.33 to 15.46 mg) displayed varying median cumulative doses. Propofol exhibited significant differences across waves (P = 0.049), while ketamine, midazolam, and dexmedetomidine remained relatively stable with no significant differences observed (P = 0.234, P = 0.375, and P = 0.563, respectively). In contrast, the analgesic medications, fentanyl (13.31 to 49.23 mg) and hydromorphone (150.59 to 1060.94 mg), exhibited consistent cumulative doses, with no significant variations noted (P = 0.318 and P = 0.114, respectively). The median duration of IMV across the four COVID-19 waves ranged from 8.0 to 10.0 days (P = 0.14). The median ICU LOS exhibited a consistent pattern across the four COVID-19 waves, ranging from 9.8 to 11.6 days, with no statistically significant variations observed (P = 0.084). Similarly, the median hospital LOS also remained relatively consistent, ranging from 16.8 to 17.7 days, with no significant differences noted among the waves (P = 0.73). The mortality rates exhibited a statistically significant increase following the first wave, with rates of 30.4, 43.8, 42.0, and 43.0%, respectively (P = 0.003).
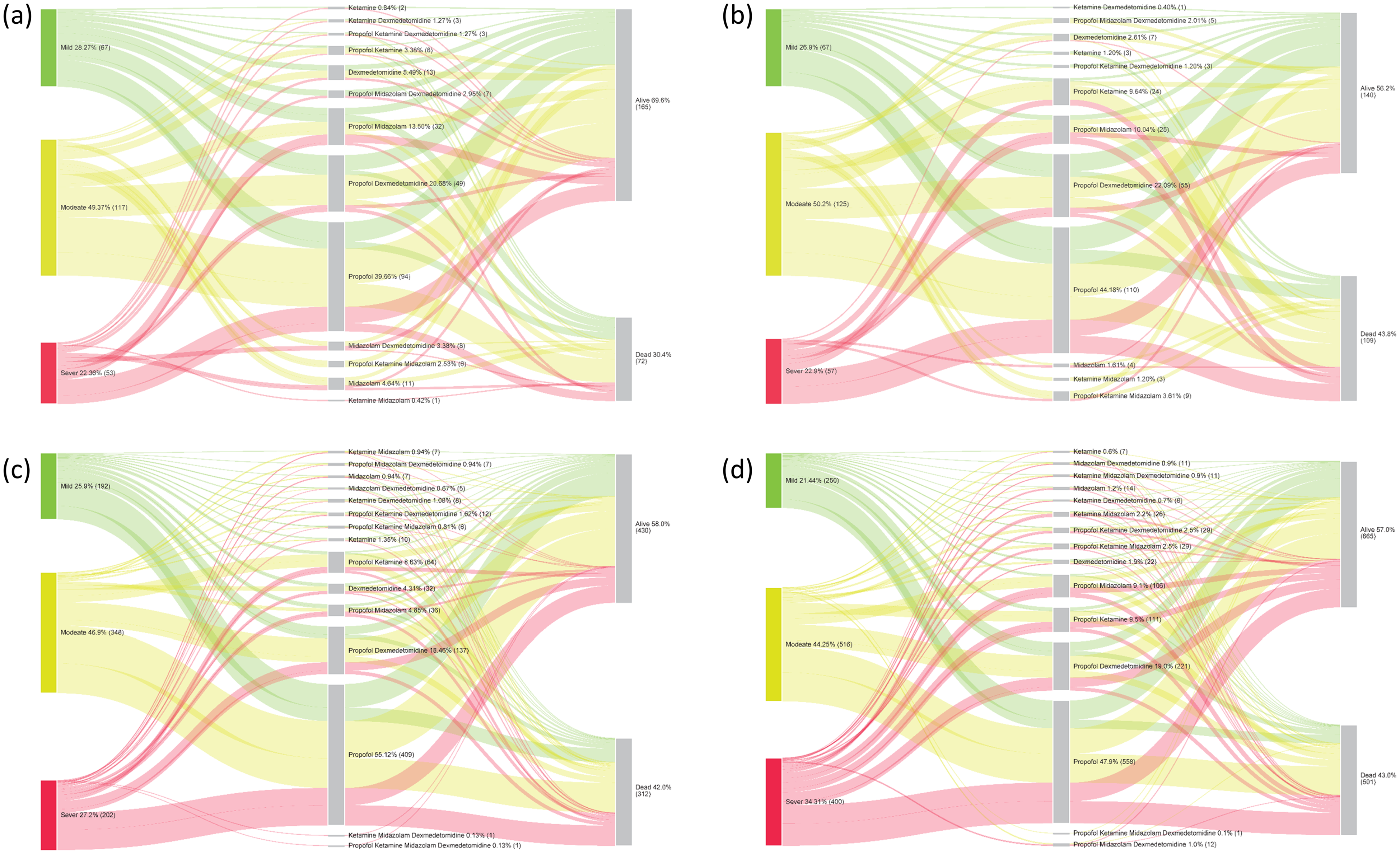
Alluvial diagram showing the movement of patients from ARDS severity and sedation regimen to alive status at hospital discharge: (a) first wave: March 1, 2020-May 31, 2020; (b) second wave: June 1, 2020-October 15, 2020; (c) third wave: October 16, 2020-February 28, 2021; (d) fourth wave: March 1, 2021-December 31, 2021. *The alluvial diagram is a flow diagram representing clusters of data categorized on the left based on ARDS severity, diverging and meeting in the middle of the diagram based on the sedation regimen, and finally ending and at the patient's discharge status. The height of each category block represents the size of the cluster of data represented within.
In our initial regression analysis, several factors emerged as noteworthy predictors of the mortality outcome. Advancing age was associated with an increased risk (adjusted odds ratio [aOR] = 1.059 [95% confidence interval (CI) 1.049-1.069]; P < 0.001]. Patients from racial backgrounds other than black or white exhibited a lower risk (aOR = 0.576 [95% CI 0.392-0.848]; P = 0.005), while patients on dialysis had a reduced risk (aOR = 0.751 [95% CI 0.575-0.982]; P = 0.036). Similarly, individuals with dementia displayed a lower risk (aOR = 0.578 [95% CI 0.451-0.739]; P < 0.001), as did malnourished patients (aOR = 0.624 [95% CI 0.485-0.803]; P < 0.001). In terms of clinical factors, severe ARDS emerged as a significant predictor (aOR = 1.437 [95% CI 1.082-1.908]; P = 0.012). The COVID-19 wave demonstrated a significant role, with patients in the second wave facing an increased risk compared to the first wave (aOR = 1.585 [95% CI 1.013-2.479], P = 0.044), and those in the third wave also exhibiting a heightened risk (aOR = 1.508 [95% CI 1.031-2.207], P = 0.034). However, the impact was most pronounced in the fourth wave, where patients experienced a notably higher risk compared to the first wave (aOR = 2.147 [95% CI 1.370-3.365], P = 0.001). Additionally, the number of vasopressors administered demonstrated a strong association with the risk of the mortality outcome, with progressively higher odds for each additional vasopressor: one vasopressor (aOR = 2.522 [95% CI 1.725-3.687]), two vasopressors (aOR = 7.489 [95% CI 5.008-11.199]), three vasopressors (aOR = 13.093 [95% CI 8.544-20.064]), and four vasopressors (aOR = 31.636 [95% CI 17.603-56.856]) (all P < 0.001). The first model R2 = 34%.
In a subsequent regression analysis, the clinical factors that exhibited statistical significance in the initial model continued to maintain their statistical significance in the second model. However, the variable “second wave versus first wave” which showed significance in the first model (aOR 1.585, 95% CI 1.013-2.479, P = 0.044), lost its significance (aOR 1.548, 95% CI 0.983-2.436, P = 0.059) after incorporating the cumulative sedative and analgesic medication dose in milligrams. Among these sedatives, dexmedetomidine demonstrated a decrease in the odds of mortality (aOR = 0.955 [95% 0.940-0.970]; P < 0.001), while propofol, ketamine, and midazolam did not contribute significantly to the risk of mortality in our model (aOR = 1 [95% CI 1-1]; P > 0.05). Notably, the addition of sedative and analgesic medications in the second model yielded only a marginal improvement in R² by 1.6%, bringing it to 35.6%. Table 2 summarizes the two regression model results and provides a comprehensive overview of the aOR for all variables incorporated in both models.
Multivariable Regression Analysis Assessing the Relationship Between Clinical Predictors and Hospital Mortality.
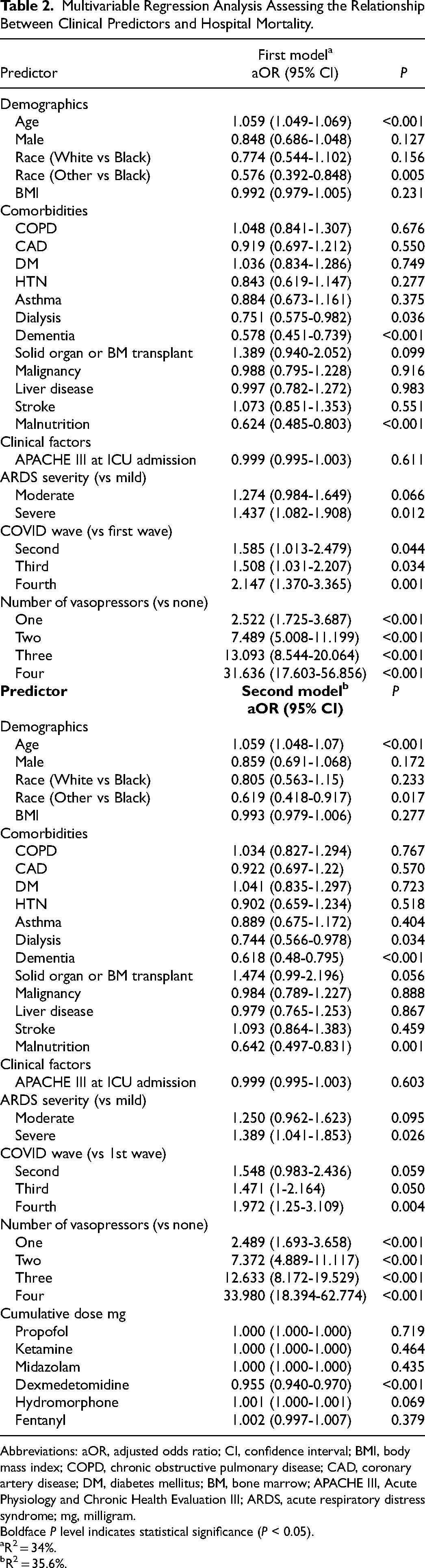
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; BMI, body mass index; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; DM, diabetes mellitus; BM, bone marrow; APACHE III, Acute Physiology and Chronic Health Evaluation III; ARDS, acute respiratory distress syndrome; mg, milligram.
Boldface P level indicates statistical significance (P < 0.05).
R2 = 34%.
R2 = 35.6%.
Discussion
Our study highlights the heterogeneity in practice related to the use of sedatives and analgesics during the COVID-19 pandemic. This study further indicates the differences in sedation practices and varying use of sedative and analgesic agent combinations during the different COVID-19 waves. Propofol remained the sedative agent of choice across all four waves, but we noticed an uptrend in the use of ketamine and a downtrend in the use of midazolam and dexmedetomidine after the first wave. Our study also highlights that in a hierarchical model after adjusting for the severity of disease, comorbidities, the choice and dose of a sedative, sedation did not impact the risk of mortality.
In the early stages of the pandemic, the Society of Critical Care Medicine (SCCM) endorsed the use of the ABCDEF liberation bundle for critically ill patients with COVID. 13 The ABCDEF bundle includes: Assess, Prevent, and Manage Pain (A), Both Spontaneous Awakening Trials (SAT) and Spontaneous Breathing Trials (SBT) (B), Choice of analgesia and sedation (C), Delirium: Assess, Prevent, and Manage (D), Early mobility and Exercise (E), and Family engagement and empowerment (F). This bundle, with a decades-long track record, was recommended due to its known advantages in reducing ICU mortality, occurrence of coma, delirium, ICU readmissions, and increase discharges to nursing or rehabilitation facilities. 14 Also this guideline remained consistent with the pre-pandemic recommendations of using propofol and dexmedetomidine as first-line options due to their rapid onset and short duration of action but with potential side effect of hemodynamic instability. Subsequently, midazolam and lorazepam were recommended as second and third agent respectively, primarily owing to their relatively longer half-life and clearance affected by hepatic and renal dysfunction, which could lead to prolonged coma and delirium after cessation. 13 Despite the recommendations, the utilization of sedative agents, especially ketamine, experienced variations during the pandemic. Ketamine, originally designated by the SCCM guidelines as a third-line analgesic after fentanyl and hydromorphone, was explored for its potential benefits as a sedative adjunct to spare propofol, with a reduced impact on hemodynamics.15,16 This deviation from the guidelines recommendations was noticeable in a real-world practice reported by 68 ICU physicians who participated in a national-level survey, where half of the respondents reported increased usage of ketamine and benzodiazepines compared to pre-pandemic practices with target of deeper sedation and less utilization of daily SAT and SBT. 17 Additionally, a multinational prevalence study conducted across 54 countries, involving 1229 patients in 135 ICUs, revealed that half of the study population did not strictly adhere to the sedation recommendations outlined in the bundle. 18
While the benefits of adhering to the ABCDEF bundle during the pandemic remain underexplored, and there is no concrete evidence to suggest that non-compliance with sedation choices leads to worse outcomes, the real-world deviation from these recommendations is intriguing. It may be a clinical response to changes in clinical factors, which are not comprehensively documented in the literature. Furthermore, this preference for newer medications over the older recommendations raises questions about their comparative effectiveness in prolonged and severe diseases like COVID-19. Few studies have described sedation practices overtime during the COVID-19 pandemic. Balakrishna et al 19 reported their practice over 10 days for 86 patients on IMV during the first month of the pandemic. They described a practice that was similar to ours with propofol being the most commonly utilized medication for sedation followed by dexmedetomidine. They reported ketamine as their third most commonly utilized agent, whereas our study showed midazolam and dexmedetomidine use exceeded ketamine in the first wave. Ketamine use subsequently increased after the first wave in our study which likely indicates increased familiarity with its use by providers over time and an attempt to avoid benzodiazepines due to the known increased risk of prolonged IMV duration, delirium, and ICU length of stay. 20 Dexmedetomidine use decreased after the first wave which is likely explained by a change in our practice of not intubating mild COVID-19 cases early, a practice that was common at the beginning of the pandemic due to concerns of transmission. 21 More importantly, our study highlights that the heterogeneity in practice increases with the severity of hypoxemia, and once more than 3 sedative agents are used, there is a significant impact on provider preferences. Studies conducted at comparable institutions have revealed a correlation between a higher dose of sedatives and increased hospital mortality, as demonstrated by Wongtangman et al 4 However, it can be argued that this correlation is due to the severity of the patients’ illnesses progression, which led the medical teams to induce deeper sedation. Although the author used propensity score matching to compare COVID-19 patients on invasive mechanical ventilation to non-COVID-19 patients, the absence of matching for sedation levels or daily subjective and objective measures of disease severity may lead to misleading conclusions as well. Our findings closely correspond to work published before the COVID-19 pandemic. Similar to the current study, Hu et al 22 showed that after adjusting for nearly identical clinical factors (age; sex; ethnicity; weight; height; APACHE III score; oxygenation index; alveolar-arterial oxygen difference; patient characteristics at discharge; hospital characteristics like number of beds, teaching, and geographic location), a significant mortality benefit was associated with dexmedetomidine when compared to both propofol (aOR 0.58 [0.42-0.79]; P < 0.001) and midazolam (aOR 0.52 [0.40-0.68]; P < 0.001), while midazolam compared to propofol was not significant (aOR 1.23 [0.96-1.57]; P = 0.10). We are uncertain whether the observed mortality benefit associated with dexmedetomidine, as reported in our study and by Hu et al 22 is due to milder disease severity in the treated patients. This ambiguity arises from the fact that dexmedetomidine, being a relatively light sedative, may not suffice in situations where higher post-end-expiratory pressure (PEEP) is needed, primarily due to the patient's comfort requirements. 23 Circulatory shock and the escalated requirement for vasopressors were the primary factors influencing mortality in our mechanically ventilated COVID-19 patient cohort. This aligns with the widely recognized role of circulatory shock as a leading cause of death in ARDS patients, compounded by the impact of invasive mechanical ventilation on the right ventricle, pulmonary hypertension, and sepsis-induced tissue demands. 24 The potential overdiagnosis of subtle malnutrition, a significant factor in reimbursement in the US, may have contributed to a high proportion (70-80%) of patients being diagnosed with malnutrition, possibly leading to reduced mortality odds in this group. Future research should carefully consider diagnosis criteria and malnutrition severity. There is a lack of existing literature that investigates the connection between dementia or the need for dialysis and mortality in COVID-19 patients requiring IMV. Therefore, it remains uncertain whether our observed lower mortality risk is a genuine result or influenced by unaccounted confounding factors.
The question of which sedative agent could achieve the targeted sedation level while yielding better outcomes, such as improved neurologic recovery and reduced mortality, remains unanswered in the literature. Studies assuming the superiority of an agent and the belief that a higher total dose would have less detrimental effects are challenged by our regression analysis. Our results indicated that clinical factors explained 34% of the mortality, while adding the total sedative and analgesic dosage only increased the explanation by 1.6%. This aligns with logical reasoning, given that the purpose of sedation is to facilitate the treatment of the disease process. Prolonged exposure to sedative and analgesic agents is often a consequence of a deterioration in the clinical condition, especially when the ABCDEF bundle is not followed appropriately. Within our healthcare system, we have fostered a culture of rigorous adherence to the ABCDEF bundle recommendations well before the pandemic, which might have helped to avoid unnecessary deep sedative and analgesic exposure during the pandemic and allowed a better opportunity to study their true effect on mortality. However, it is essential to note that the absence of discrete data in our EHR to reflect compliance with ABCDEF recommendations could introduce limitations to our certainty in reaching this conclusion. In summary, our analysis reveals notable diversity, intermingling, and excessive use of sedatives in our sedation protocols during the COVID-19 pandemic, despite current guidelines suggesting that strategies targeted to minimize sedation during ICU stay should be favored. 20 While potential reasons for this may include the severe and prolonged nature of the illness and isolation precautions that limit frequent assessment and titration, a superiority analysis for any particular sedative agent would pose significant challenges and high risk of bias. Furthermore, our analysis contributes to a better understanding of potential factors associated with mortality in a sample of critical COVID-19 patients, providing a unique opportunity for targeted interventions aimed at improving patient outcomes. Our study's strengths lie in its multicenter design, substantial sample size, comprehensive data collection regarding sedation dosages, and the utilization of a multivariable regression model to account for available covariates. However, our study has certain limitations. It is retrospective in nature, and it lacks adequate daily subjective variables such as the Richmond Agitation-Sedation Scale (RASS) score for assessing sedation levels. Additionally, we were without objective clinical variables like daily vital signs, information on exposure to antibiotics or steroid medications, as well as data related to the use of extracorporeal membrane oxygenation (ECMO) and complications during ICU stays, such as delirium or the need for tracheostomy. Additionally, the lack of balance in demographics and baseline clinical characteristics across the four study cohorts may potentially result in selection bias. However, building a regression model to control the available baseline variables indicated that the different sedative and analgesic agents did not contribute significantly to the mortality. Further research should consider using multivariable regression analysis to account for relevant baseline characteristics, daily clinical interventions, and disease severity which is necessary to comprehend the potential benefits of one sedative compared to others. Another significant finding from our study concerning clinical practice is the recommendation for healthcare systems to incorporate clinical decision-support tools with multiple sedation protocols into their EHR systems. This step is essential for ensuring standardized practices and facilitating data extraction for future research. By proactively addressing this issue in non-pandemic periods, there is an opportunity to develop diverse protocols that mirror various clinical and logistical considerations. This proactive approach can alleviate the strain on healthcare professionals and enhance preparedness for potential future pandemics. The promising potential for a mortality benefit associated with the use of dexmedetomidine in light sedation warrants consideration as a means to prevent deep sedation and aligns with the recommendations of the ABCDEF liberation bundle. Further studies are required to confirm our results in the critical COVID-19 population, to provide a basis for helping to guide future sedation practices in these patients.
Conclusion
The mortality in critically ill patients was mostly driven by the severity of illness and the choice of sedation might have minimal impact when other factors are controlled. The current study highlights the need for standardized sedation protocols during the COVID-19 pandemic and emphasizes the challenges of future analyses to assess the impact of sedation practices on patient outcomes.
Footnotes
Acknowledgments
None
Authors’ Contributions:
M.A. contributed to conceptualization, data curation, methodology, validation, writing – original draft, and writing – review and editing. X.W. contributed to formal analysis, software, and writing – review and editing. H.T. contributed to methodology, data curation, and writing – review and editing. G.L.S. contributed to methodology, data curation, and writing – review and editing. F.A. contributed to conceptualization, data curation, methodology, resources, and writing – review and editing. A.D. contributed to conceptualization, data curation, methodology, resources, supervision, and writing – review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
Study approved by Cleveland Clinic Institutional Review Board (IRB) and consent has been waived by the IRB.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.