
Abstract
Introduction
Family-centered rounds (FCR) are a multidisciplinary and inclusive approach to daily patient care in the intensive care unit (ICU).1,2 The Society of Critical Care Medicine highlights FCR as a key aspect of a comprehensive and evidence-based family support approach in the ICU. 2 Adequate communication during ICU admission is critical as family members are at significant risk for depression, anxiety, and posttraumatic stress disorder after their loved one's admission.3,4 FCR has been shown to reduce the risk of psychological comorbidities of family members, improve the quality of communication between providers and families, and improve overall family satisfaction levels.5,6 Additionally, FCR may improve ICU clinician time management by decreasing the need for family updates throughout the day 7 and decreasing rounding time,8,9 decrease length of stay, and decrease overall ICU costs.5,10
When the COVID-19 pandemic forced hospital visit limitations, clinicians adapted new ways to support family members through utilization of virtual modalities. 11 Virtual meetings and updates quickly became a primary modality for family communication,12–14 and virtual FCR was introduced. While in-person FCR has been a standard practice in many pediatric and adult ICU settings,2,15 few studies support the use and efficacy of virtual technology for FCR, especially in acute care settings such as the cardiac ICU. Because of the lack of data and rapid uptake of virtual technology during the COVID-19 pandemic, this quality improvement study aimed to understand family members’ perceptions of virtual FCR in a cardiovascular critical care setting. The cardiac ICU at the study hospital provided a unique setting for virtual FCR by compiling a diverse interdisciplinary team of social workers, case managers, nurses, and physicians. Rounds were completed using a dedicated device with video and audio capabilities. The primary outcome of this quality improvement project was to explore family members’ perceptions of the benefits and barriers of virtual FCRs. It was hypothesized that family members would highly rate the quality of communication.
Materials and Methods
This pilot quality improvement study included adult family members of previously admitted cardiac ICU patients who participated in at least one session of virtual FCR between April 2020 and June 2021 at Massachusetts General Hospital (MGH). MGH is a 999-bed urban quaternary care general hospital, where the cardiac intensive care units include 34 beds in both traditional cardiac surgical intensive care unit and cardiac medical intensive care unit. During this study, a dedicated cardiac intensivist experienced in FCR-led daily bedside rounds in the unit. A total of two cardiac intensivists participated when they were attending in the cardiac ICU.
FCR was conducted with the nurse or attending intensivist contacting the patient representative immediately prior to initiating rounds. Contact was made with a dedicated tablet device with Zoom capability. If this modality was not available, telephone was used. After contacting the representative, the intensivist introduced the team members (typically an intensivist, nurse, and nurse practitioner) and then rounds proceeded with the responding clinician's review of data and events, examination of the patient, and then verbalization of the daily plan. If multiple family members were listed in the electronic medical record, the primary decision maker was contacted first with the option to participate voluntarily. If the primary family contact declined, the secondary family member was contacted and given the opportunity to participate. Therefore, for each patient admitted to the ICU only one surrogate participated in the study. The Mass General Brigham Institutional Review Board approved this study (Virtual Family Centered Rounds in the Heart Center Intensive Care Unit #2020P002532 on 08/21/20 deemed exempt) prior to initiation. The study was in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975.
Family members or surrogates of admitted cardiac ICU patients were contacted via telephone after hospital discharge and were asked to complete a phone survey. The phone survey included an opening and closing script for both the verbal consent and introduction to the questions. Methodology for follow-up call timing varied. Once a patient's family member participated in virtual FCR, they were subsequently contacted post-discharge. Some patients remained in the hospital for weeks and some required inpatient rehabilitation. Those patients’ families were contacted weeks after the FCR participation (given hospital non-ICU days and rehabilitation days). Study investigators called primary family members beginning at 1-week post-discharge. Families were called up to three times (at least 1 day intervals) and if no response was obtained after three attempts, efforts were stopped.
The questionnaire included a modified Patient Perception of Patient Centeredness (PPPC) survey utilizing the unipolar scale from 1 to 4. 10 Scores of 1 corresponded with a higher level of care while a score of 4 corresponded with a lower level of care. The PPPC survey is a validated survey which has been previously adapted to study the impact of a family support intervention on family member/family satisfaction.10,16 While initially developed in the outpatient setting for patients’ experience, the PPPC aimed to address a patient's experience with their disease, common ground with the provider, patient–doctor relationship, and perception of whole-person care. 16 To best apply to our study population, we modified the existing 14-item PPPC 17 survey by rewording the questions to be more directed toward family members versus the patients themselves, and to be more applicable to the inpatient setting. Three questions which were specific to the patient's experience (not the family members) were also omitted. Three qualitative questions were also administered to assess the family member's experience, as detailed in Table 1. Information on the relationship to the patient and the number of days the respondent participated in virtual FCR was collected. Patient demographics (age, sex, race/ethnicity, reason for admission) and outcomes data (length of ICU and hospital stay and discharge disposition) were abstracted from the medical records. Survey data were collected directly into an electronic password-protected Research Electronic Data Capture (REDCap) database for analysis. Both complete and incomplete questionnaires were included in the analysis. Incomplete questionnaires occurred when family members felt that they were unable to provide an answer for certain questions but felt comfortable answering other parts of the questionnaire.
Survey Questions.
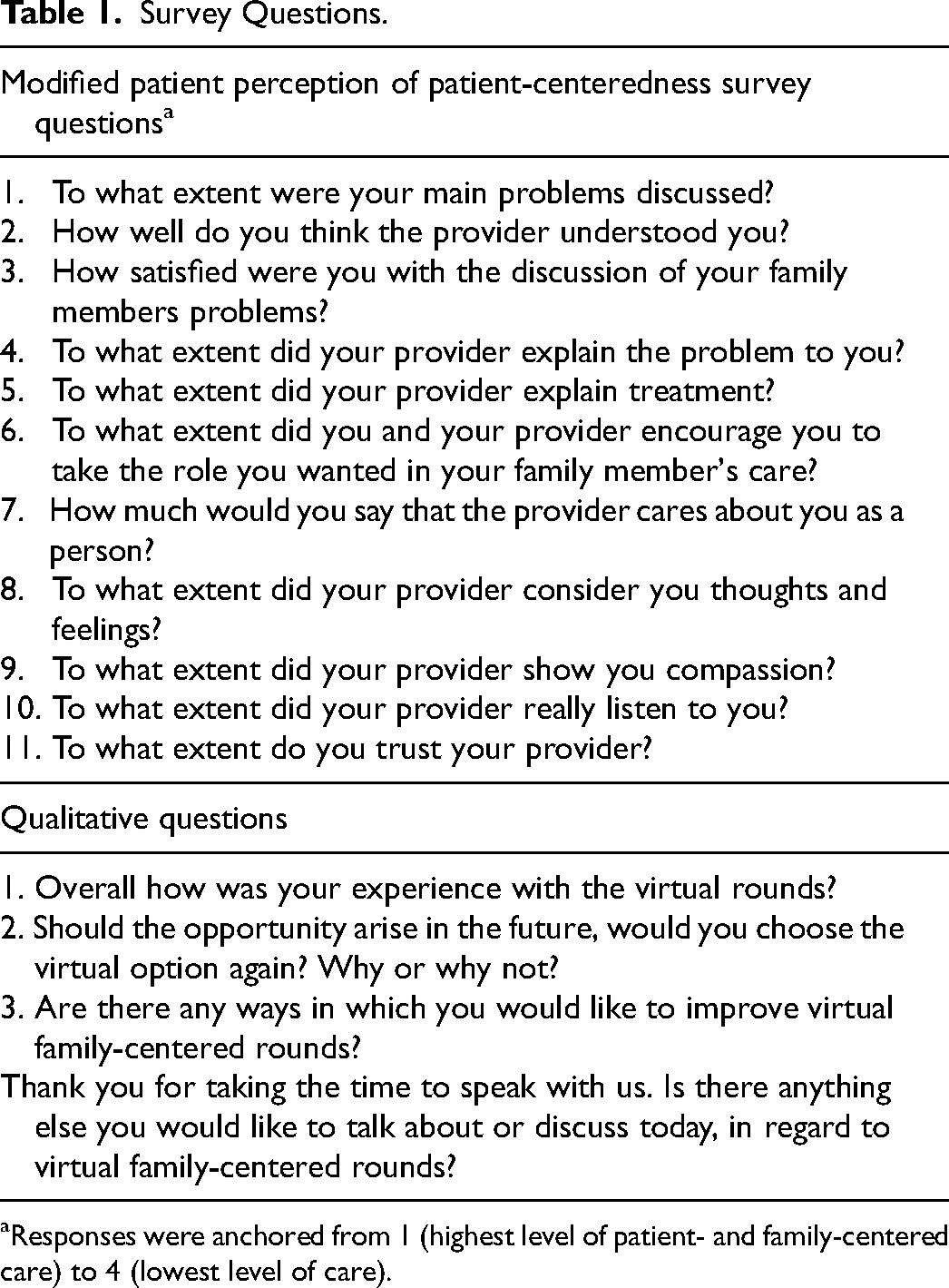
Responses were anchored from 1 (highest level of patient- and family-centered care) to 4 (lowest level of care).
Statistical Analysis
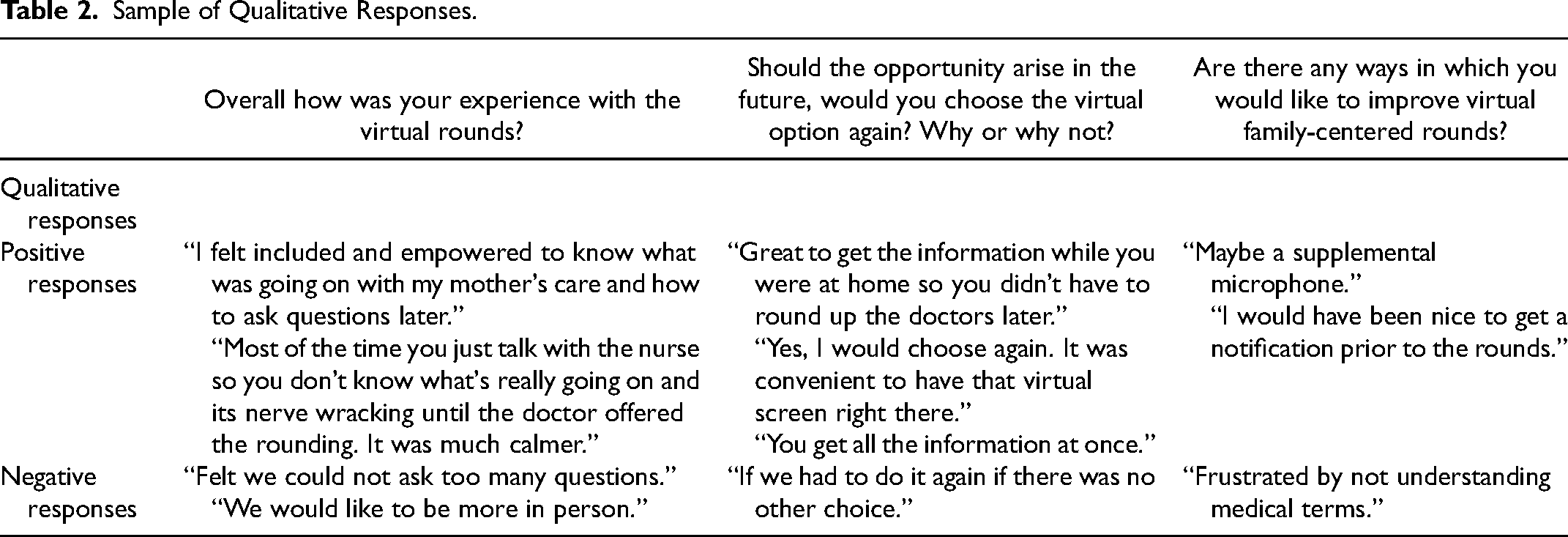
Given the descriptive nature of the analysis, continuous values are presented as mean ± standard deviations or median (interquartile range [IQR]) depending on the distribution of the data. Normality was assessed using the Shapiro–Wilk test and confirmed by visually inspecting the data. Categorical data are presented as frequency counts and proportions. Differences between those who did and did not participate in the survey were assessed using a Wilcoxon Rank Sum Test, chi-square, or Fisher's Exact Test. Two-sided p-values < .05 were considered statistically significant. Samples of qualitative responses sorted based on the study staff's perception of whether the feedback was positive or negative are shown in Table 2. Sample size was dependent on enrollment and participation in virtual FCR during the reported time period. A prespecified number of responses was not required and instead, all surrogates who consented over this time period were included. All descriptive statistics were generated using SAS 9.4 (SAS Institute Inc., Cary, NC).
Sample of Qualitative Responses.
Results
Over the course of the study period, a total of 82 family members participated in virtual FCR, of whom 29 completed a post-discharge phone questionnaire, resulting in a response rate of 35.4%. Reasons for non-response included the inability to contact the family or participants declining. Baseline demographic data for patients is included in Table 3. Among the patients whose family members participated in virtual FCR, 70.7% were non-Hispanic White, 8.5% were non-Hispanic Black, 11.0% Hispanic, and 9.8% other or nonidentified. Of the eight male partners who participated in virtual FCR, none opted to complete the survey. Additionally, only one of the family members of the 11 patients who died in the hospital elected to complete the survey.
Demographics.
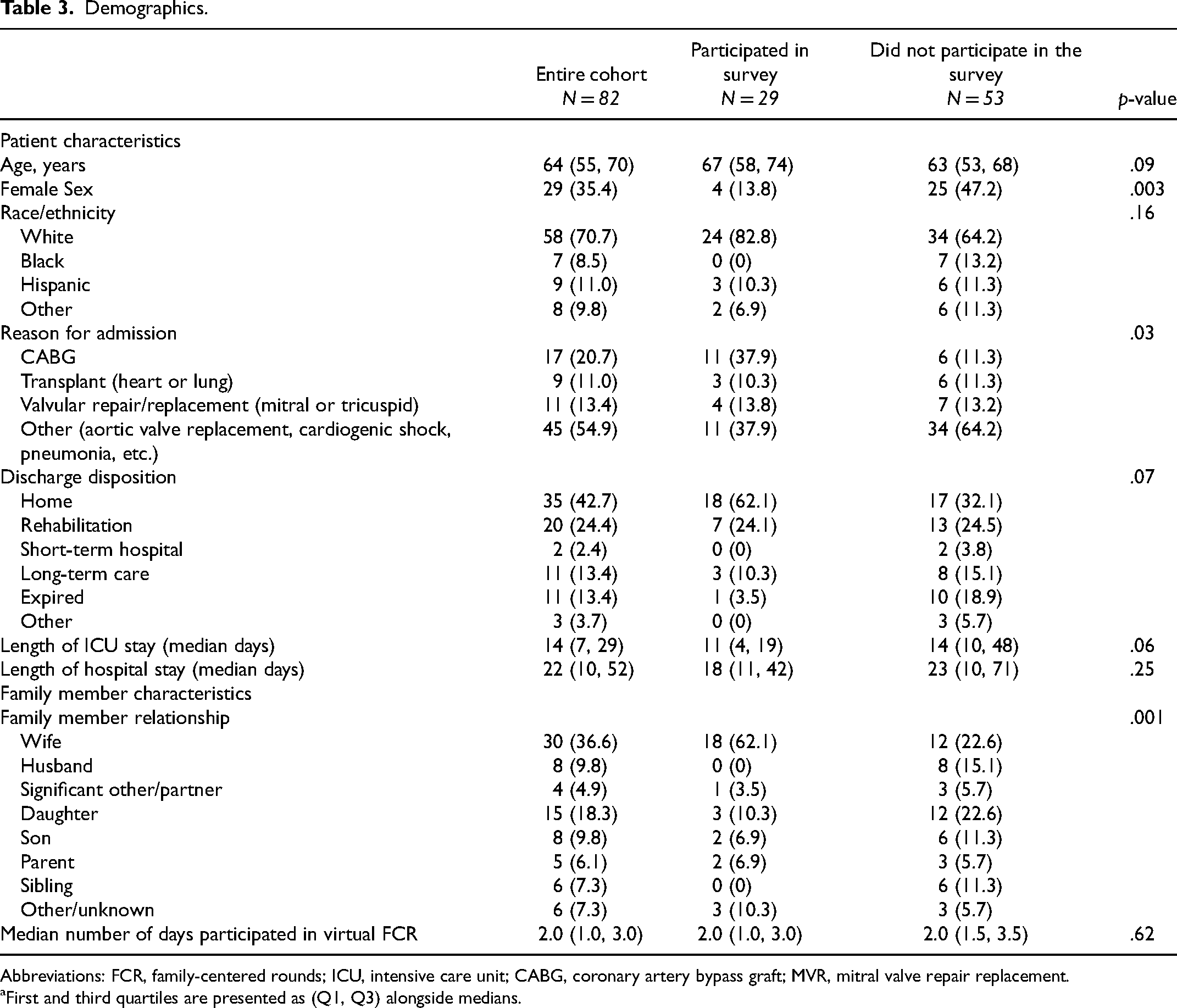
Abbreviations: FCR, family-centered rounds; ICU, intensive care unit; CABG, coronary artery bypass graft; MVR, mitral valve repair replacement.
First and third quartiles are presented as (Q1, Q3) alongside medians.
The majority of ICU patients were male (n = 53) and had a median age of 64 years (IQR 55, 70). The most common reason for admission to the ICU was other (n = 45) which included a variety of ICU conditions such as pericarditis, pneumonia, cardiogenic shock, etc. Most patients were discharged home or home with services (42.7%), followed by rehabilitation (24.4%), long-term care (13.4%), or deceased (13.4%). Patients’ wives (n = 18) most commonly completed the questionnaire, followed by their children (daughter n = 3, son n = 2).
Across all questions in the survey, more than 75% of the respondents perceived the highest level of care in trust, communication, relationship, and compassion with their provider (Figure 1). Notably, 96% of respondents perceived the highest level of care in trust. The next highest categories covered explanation of information with 88% perceiving the highest level of care and understanding with their provider with 89%. The responses regarding role responsibility and caring as a person had scores of 78% and 76%, respectively. A representative sample of responses is shown in Table 2 highlighting both negative and positive responses from the qualitative questions.
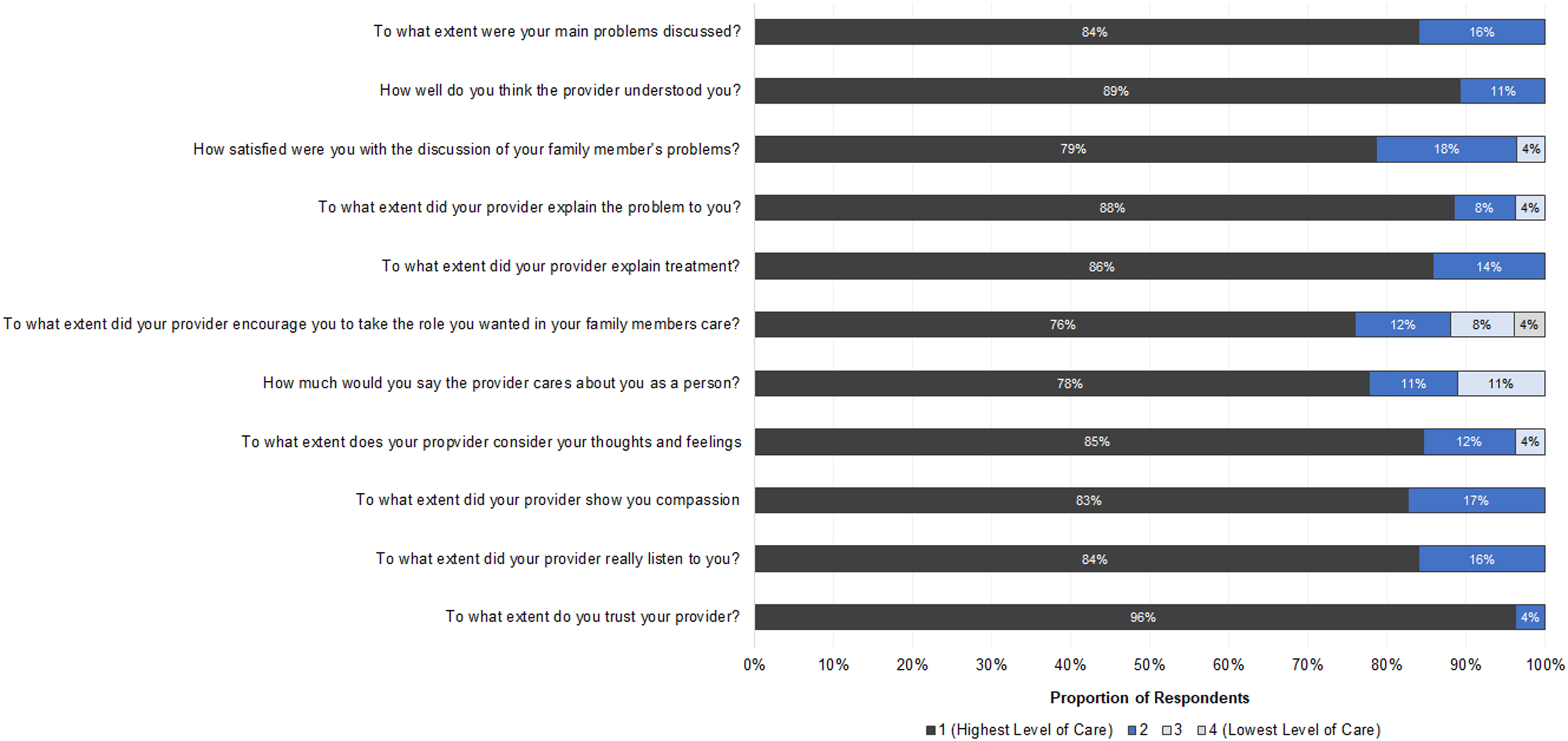
Survey results.
Discussion
To our knowledge, this quality improvement study is the first to explore the role of virtual FCR in a cardiac ICU. We discovered that family members positively rated the quality of communication associated with virtual FCR. Most family members valued the treatment explanations provided and invitation to participate in care. A minority of family members felt overwhelmed with medical language used during virtual FCR as highlighted in the qualitative responses (Table 2).
The survey results support the use of a virtual FCR format, an important component of evidence-based family-centered care. A study at the Medical College of Wisconsin evaluating the efficacy of virtual FCR in pediatrics found that families felt more involved and felt it “extremely important to be included on rounds” specifically in regards to nonverbal communication such as resident body language and inclusion over the screen. 14 However, there remains a paucity of data on the utilization of virtual FCR in the cardiac ICU. Our quality improvement study explores the potential benefits of virtual FCR and may serve as foundation to evaluate virtual FCR in a clinical trial setting.
The novelty of telemedicine has given clinicians the opportunity to engage with and include multiple family members without geographical constraints. For example, some of the qualitative responses highlighted how beneficial it was for families to be able to participate from home where they would not have been able to otherwise participate due to work or transportation constraints. There were times where family members were able to connect while out of state, and in some cases out of the country. This opens the door for improved communication and engagement with key stakeholders without the limitation of location or distance. With the increase in reliance on telemedicine, virtual FCR allows for novel ways to incorporate the patient-centered model in practice. The positive findings in this study are in line with SCCM guidelines to provide “flexible family presence at the bedside” and “implement routine interdisciplinary family conferences to improve communication and trust.” 2 This study highlights the benefits of video conferencing and the need for structured communication as a part of COVID-19 family-centered care initiatives. 18 Overall, a FCR approach has been shown to improve shared decision-making among the care team. 19 FCR allows family members to be present in real-time during key decision-making points rather than being consulted afterward or only in limited situations.
One of the barriers to virtual FCR mentioned in this study was family dissatisfaction with taking an active role in a patient's care. We theorize that while family members overall feel virtual rounds are a positive experience to communicate information, they may feel slightly less able to take an active role in their care given the lack of physical contact in a virtual format as well as the challenges with utilizing video conferencing technology. Another recent study in a pediatric ICU—specifically regarding virtual hybrid rounds—highlighted various issues with limitations in audio and visual quality of rounds. 20 As done in our study, we created a streamlined approach to assisting patients and logging in which may obviate some difficulties and discomforts patients and clinicians experience. A virtual format is still relatively novel for many and being able to take an active role in their family member's care requires comfort with the virtual format during a stressful time. Further investigation would be needed to better understand if general discomfort with the format has eased as people adapt to virtual platforms.
This study has several limitations. First, we modified a previously validated PPPC survey to adapt its use on family members. Additionally, the small sample size, high likelihood of selection bias in respondents, and low response rate over a long-time frame make it difficult to generalize to other ICUs. Furthermore, since only two cardiac intensivists were experienced in FCR, the study was limited to weeks when they were on clinical service. There is likely a positive response bias in those who had better experiences were more likely to respond, or that responses may be biased based off the proximity between the survey completion and the ICU stay. Due to the fact that we did not have a control group to compare and rate their experience with the cardiac ICU, it is hard to ascertain how this might affect our results. Given the high positivity in responses we suspect a ceiling effect which is a common occurrence and limitation in patient surveys. We also were limited in communicating with family members who were not comfortable in using the virtual teleconferencing software.
Conclusion
Our study showed that ICU patient family members positively rated the quality of communication associated with virtual FCR. The results support providing an option for virtual FCR for ICU families, which is in alignment with current patient and family-centered care guidelines. Further investigation is needed to address and understand barriers and benefits of FCR.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Mongan Institute at Massachusetts General Hospital which supported Paolo Ramirez.