
Abstract
Keywords
Introduction
Community-acquired pneumonia (CAP) is a highly prevalent acute lung infection associated with significant disease burden and healthcare consumption. With approximately 1.5 million inpatient admissions per year, CAP is the second most common cause of hospitalization and the most common infectious cause of death in the United States.1–3 In the realm of critical care, CAP contributes to a significant portion of intensive care unit (ICU) admissions, and is associated with high mortality and ventilator requirement.4–7
Acute respiratory distress syndrome (ARDS), a noninfectious inflammatory lung injury, contributes to an even larger portion of ICU admissions compared to CAP and is similarly associated with high mortality and ventilator requirement.8,9 One study across 50 countries noted a 10.4% prevalence of ARDS among thousands of ICU patients, and that patients with ARDS accounted for 23.4% of all patients requiring mechanical ventilation. 10 While pneumonia is a common etiology of ARDS,7,11 there is limited prior literature assessing the incidence, risk factors, and outcomes among patients with CAP who develop ARDS. In this study of patients hospitalized with CAP, we investigated patients who did and did not develop ARDS during hospital admission to identify predictors of ARDS and assess the impact of ARDS on hospital outcomes in patients with CAP.
Methods
Data Sources
This study was approved by the Duke University Institutional Review Board (IRB number: Pro00108689). Patient data was retrieved from the Premier Healthcare Database (Charlotte, NC) between January 2016 and March 2020. The Premier Healthcare Database contains discharge information from 10 million patient encounters and is compliant with the Health Insurance Portability and Accountability Act. This service-level, all-payer database is large, geographically diverse, and hospital-based. It includes patient demographic characteristics, disease states, and a time-stamped log of billed items. 12
Population and Setting
We included adult patients who had a principal diagnosis of pneumonia (International Classification of Disease, Tenth Revision, Clinical Modification [ICD-10-CM] codes J13, J14, J15.x, J16.x, J17.x, J18.x, and J69.0) or a secondary diagnosis of pneumonia paired with a principal diagnosis of respiratory failure or sepsis. 13 Patients were included if they were adults (age ≥18), had a charge for chest imaging (X-ray image or computed tomography), were mechanically ventilated within 2 days of admission, and were started on antimicrobial treatment within 2 days of admission. 14 We selected for patients who were mechanically ventilated to compare patients with CAP with similar severity of initial illness, whether or not they ultimately developed ARDS (ICD-10 code J80). Patients were excluded if they were transferred from another hospital, had a diagnosis of cystic fibrosis, or were discharged within 2 days of admission.
Study Design, Exposure, Outcomes, and Covariates
This was a retrospective cross-sectional cohort study. ICD-10-CM diagnosis codes were used to identify patients who developed ARDS. The primary outcome was in-hospital mortality, comparing cohort patients who did and did not develop ARDS. Secondary outcomes included length of stay (LOS), mechanical ventilation days, days in the ICU, and total cost. Covariates included demographics (age, sex, and race), baseline comorbidities (hypertension, congestive heart failure, valvular disease, peripheral vascular disease, paralysis, other neurological disorders, chronic pulmonary disease, diabetes, hypothyroidism, renal failure, liver disease, peptic ulcer disease, acquired immune deficiency syndrome, arthritis, coagulopathy, obesity, weight loss, fluid and electrolyte disorders, chronic blood loss anemia, deficiency anemia, alcohol use, drug use, psychoses, and cancer) using the binary Elixhauser's comorbidity indicator, 15 hospital characteristics (number of beds, teaching hospital, and location), and management (vasopressor use within 2 days of admission, dialysis within 2 days of admission).
Statistical Analysis
All continuous data were expressed as either means with a standard deviation or medians with an interquartile range. Categorical data were expressed as percentages. Using a multilevel logistic regression model, we estimated the odds ratios of hospital mortality. For continuous outcomes, we used generalized estimating equations with a negative binomial distribution and log link. The model had random intercepts for individual hospitals to account for clustering within hospitals, adjusting for the covariates noted above. Statistical significance was set at P = .05. All analyses were conducted using SAS version 9.4 (SAS Institute).
Results
Demographic and Clinical Characteristics of the Study Population
There were 472 820 patients with ICD-10-CM codes for pneumonia identified in the premier healthcare database (PHD) (Figure 1). Of these, 72 107 patients met criteria for the final cohort, and 1924 (2.7%) of these patients developed ARDS. Comparing the ARDS versus no ARDS cohorts, notable patient characteristics are as follows, respectively: 49.9% versus 51.9% male, 73.6% versus 73.2% White, 14.6% versus 15.6% Black, 28.7% versus 39.2% history of congestive heart failure, 30.2% versus 45.4% history of chronic pulmonary disease, 15.3% versus 23.2% history of renal failure, 4.5% versus 3.4% history of arthritis, 17.4% versus 12.6% history of coagulopathy, 58.1% versus 57.3% history of fluid and electrolyte disorders, and 52.8% versus 40.0% initiation of vasopressors within 2 days of admission (Table 1).
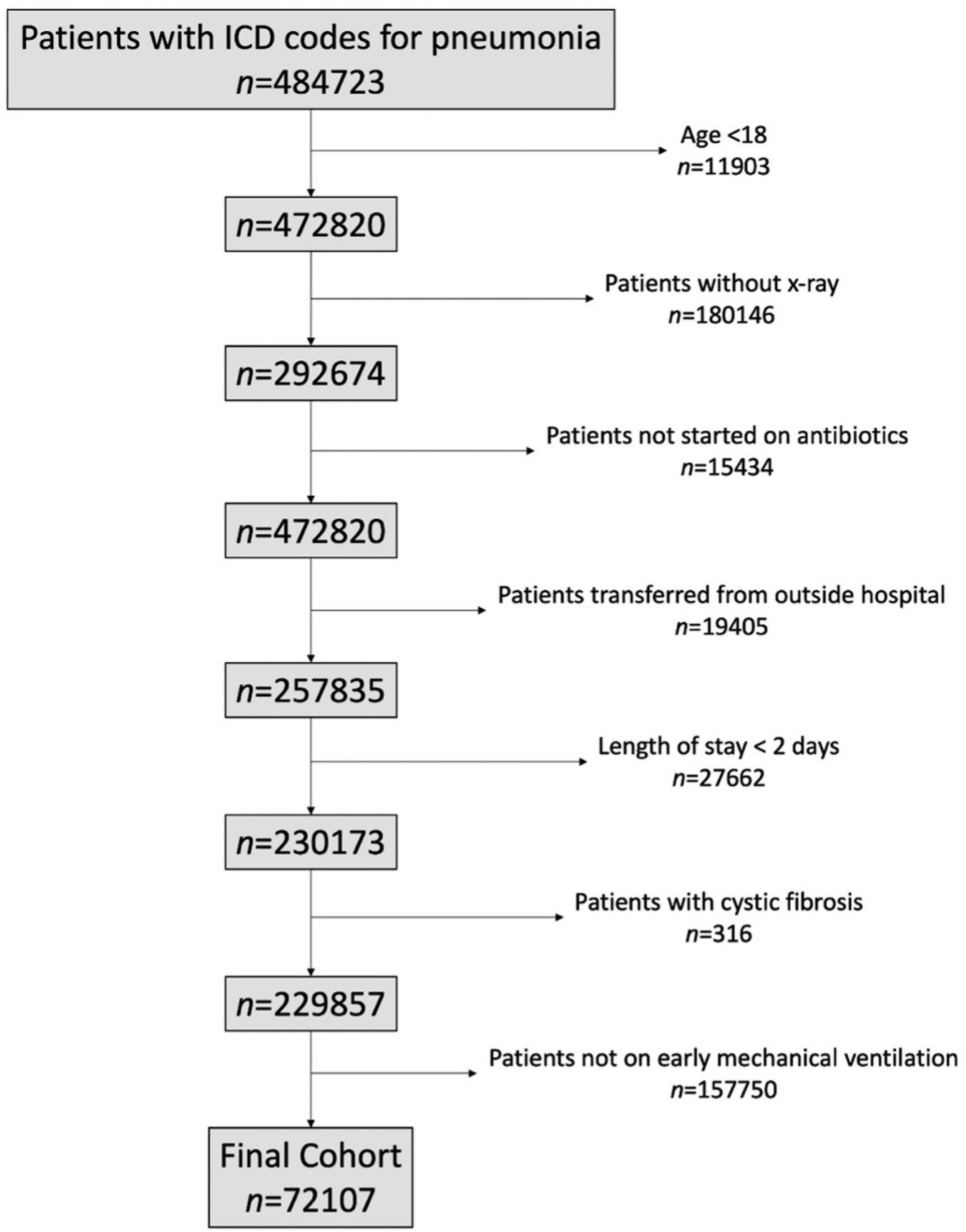
Final cohort based on inclusion and exclusion criteria.
Patient Characteristics Among Patients With Community-Acquired Pneumonia With and Without ARDS.
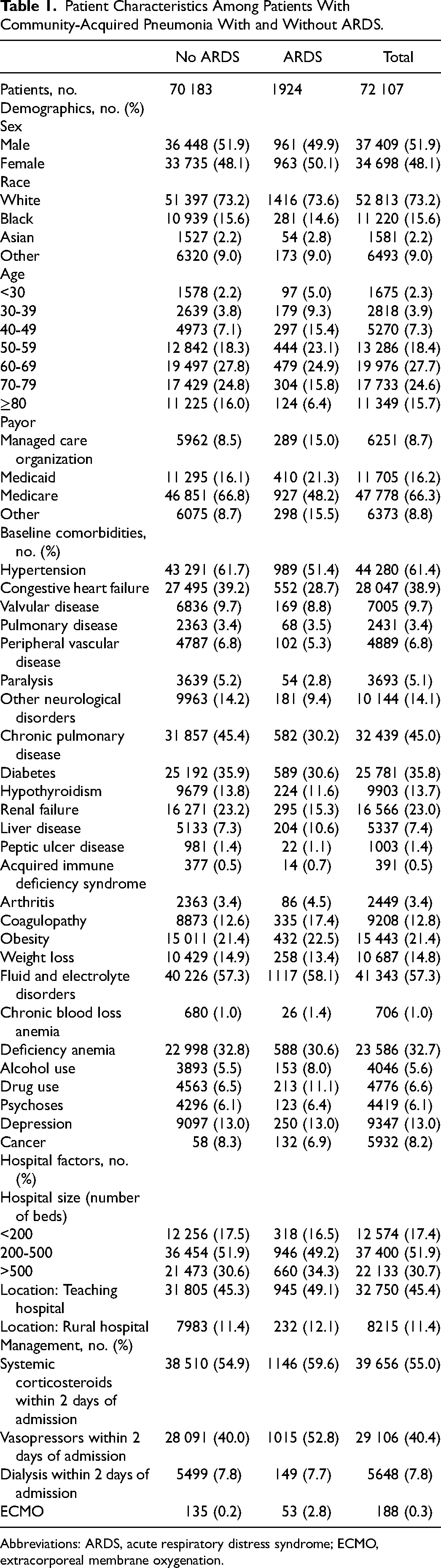
Abbreviations: ARDS, acute respiratory distress syndrome; ECMO, extracorporeal membrane oxygenation.
Outcomes in ARDS
Hospitalized patients who developed ARDS had higher mortality rates (n = 648, 33.7%) than those that did not (adjusted odds ratio (aOR) 2.40; 95% CI 2.16-2.66). The Kaplan-Meier statistic showed that the survival probability at 30 days of hospitalization was higher for patients without ARDS compared to those with ARDS (logrank test: P-value <.0001) (Figure 2).
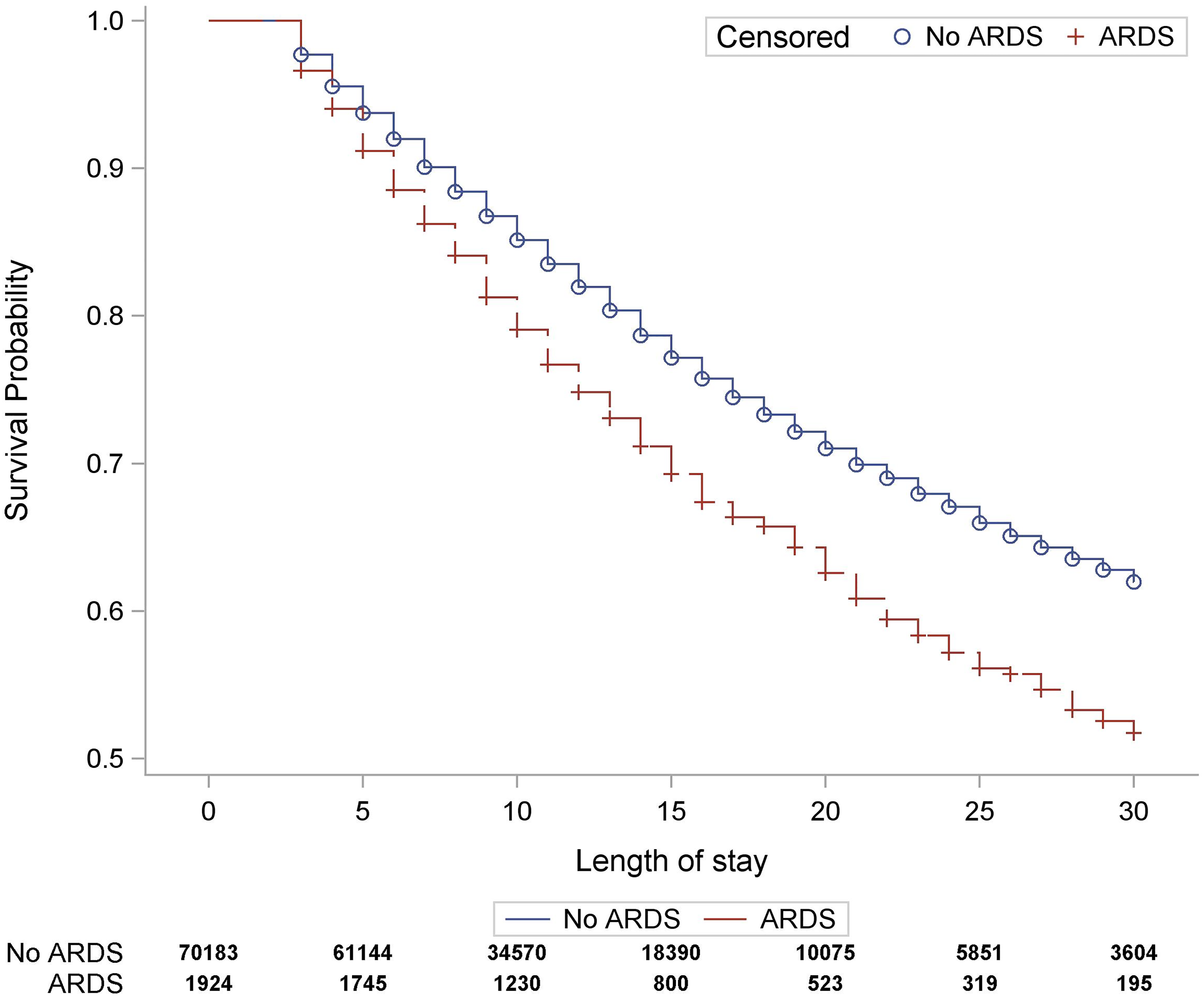
Kaplan-Meier curve depicting the survival probability of hospitalized patients who did and did not develop ARDS. Abbreviation: ARDS, acute respiratory distress syndrome.
Patients with ARDS also had longer median LOS (13 vs 9 days; adjusted incident rate ratio [aIRR] 1.24; 95% CI 1.20-1.27), days on mechanical ventilation (8 vs 5; aIRR 1.54; 95% CI 1.48-1.59), and days in the ICU (9 vs 5; aIRR 1.51; 95% CI 1.46-1.56) than patients who did not develop ARDS. Furthermore, median total cost of hospitalization was significantly higher in the ARDS cohort ($46 459 vs $29 441; aIRR 1.50; 95% CI 1.45-1.55) (Table 2).
Outcomes Among Patients With Community Acquired Pneumonia With and without ARDS.
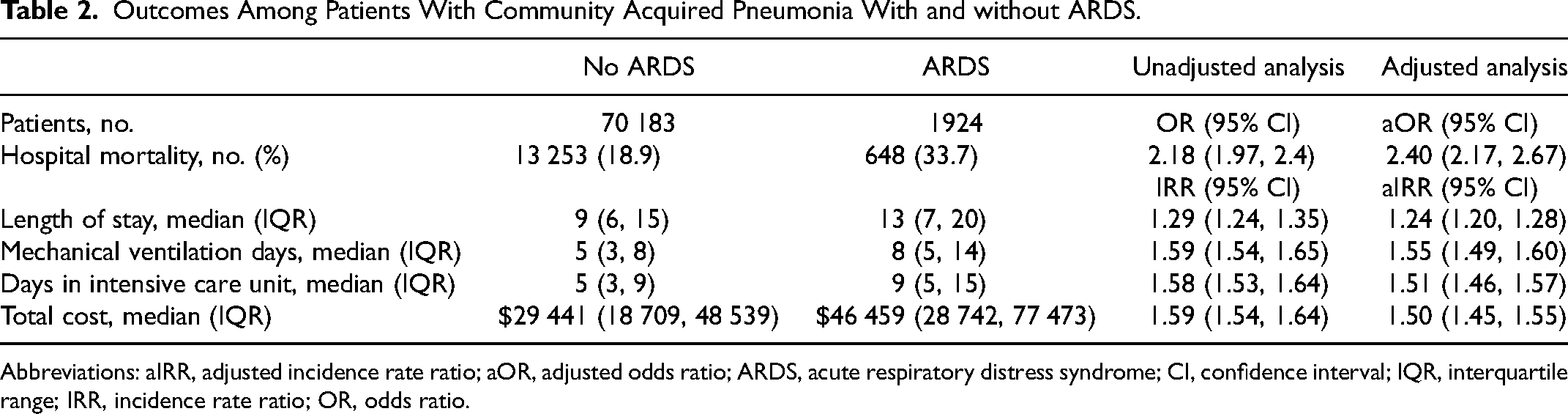
Abbreviations: aIRR, adjusted incidence rate ratio; aOR, adjusted odds ratio; ARDS, acute respiratory distress syndrome; CI, confidence interval; IQR, interquartile range; IRR, incidence rate ratio; OR, odds ratio.
Factors Associated With ARDS
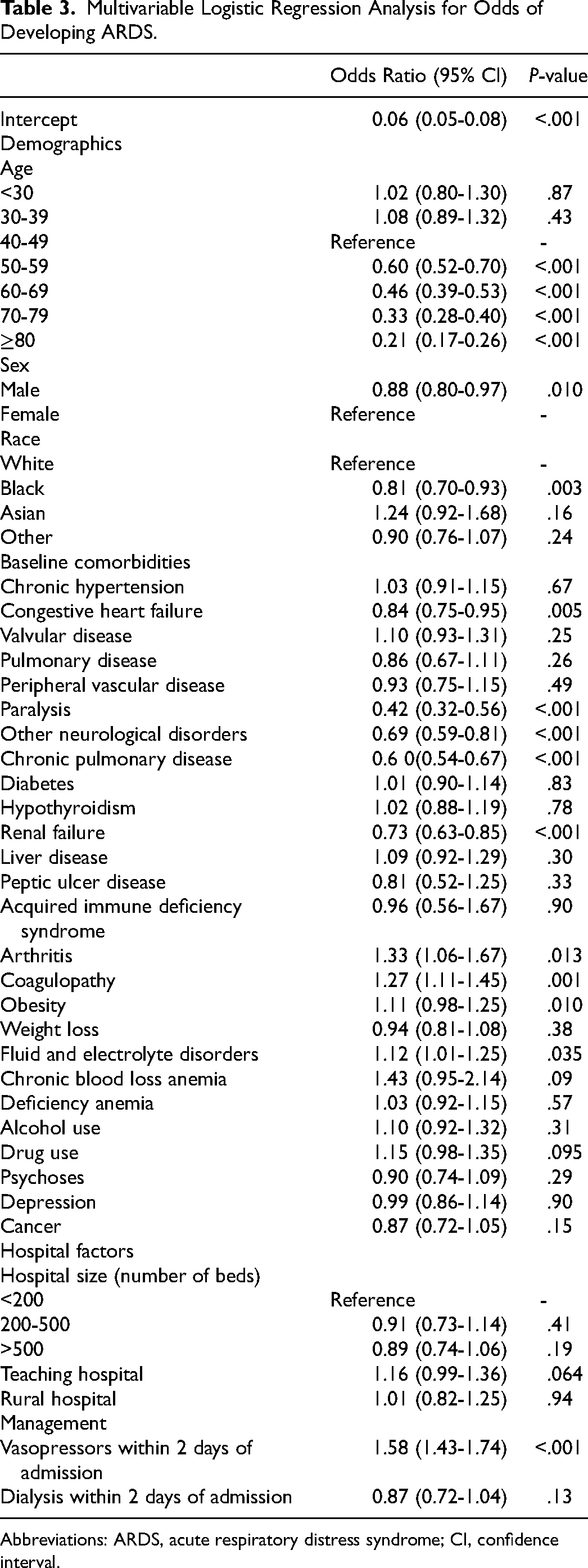
Several factors were associated with the development of ARDS. These included arthritis (OR 1.33; 95% CI, 1.06-1.67; P = .0135), coagulopathy (OR 1.27; 95% CI, 1.11-1.45; P = .0006), fluid and electrolyte disorders (OR 1.12; 95% CI, 1.01-1.25; P = .0349), and vasopressor use within 2 days of admission (OR 1.58; 95% CI, 1.43-1.74; P < .0001; Table 3). Several factors were associated with a decreased risk of ARDS. These included age 50-59 (OR 0.60; 95% CI, 0.52-0.70; P < .0001), age 60-69 (OR 0.46; 95% CI, 0.39-0.53; P < .0001), age 70-79 (OR 0.33; 95% CI, 0.28-0.40; P < .0001), age ≥ 80 (OR 0.21; 95% CI, 0.17-0.26; P < .0001), male sex (OR 0.88; 95% CI, 0.70-0.93; P = .0096), Black race (OR 0.81; 95% CI, 0.70-0.93; P = .0028), congestive heart failure (OR 0.84; 95% CI, 0.75-0.95; P = .0051), chronic pulmonary disease (OR 0.60; 95% CI, 0.54-0.67; P < .0001), renal failure (OR 0.73; 95% CI, 0.63-0.85; P < .0001), paralysis (OR 0.42; 95% CI, 0.32-0.56; P < .0001), and other neurological disorders (OR 0.69; 95% CI, 0.59-0.81; P < .0001) (Table 3).
Multivariable Logistic Regression Analysis for Odds of Developing ARDS.
Abbreviations: ARDS, acute respiratory distress syndrome; CI, confidence interval.
Discussion
In this retrospective cross-sectional cohort study, we found that development of ARDS after CAP was associated with worse in-hospital outcomes and higher cost of treatment. We also identified several factors, including treatment practice, demographics, and baseline comorbidities that were either predictive of or protective against the development of ARDS after CAP.
Our study contributes to existing work as an analysis of a large patient population with CAP and ARDS. CAP and ARDS are both associated with frequent hospitalization, ICU admission, mechanical ventilation (MV) requirement, high mortality, and significant resource utilization.7,8,10,16 Outside of mortality, there is limited data examining risk factors for and outcomes in patients who develop ARDS in the setting of CAP. We found that mortality, hospital LOS, ICU LOS, and number of days on MV were all higher in the ARDS cohort. In our study, ARDS patients had a 33.7% in-hospital mortality. Most literature typically demonstrates a mortality between 30% and 40% in ARDS across etiologies (eg, sepsis, trauma, and pneumonia).10,17–21 There is also evidence that mortality increases significantly with increasing severity, with one study indicating that patients with moderate ARDS had an in-hospital mortality of 31.8% while patients with severe ARDS had a 60% in-hospital mortality. 22 In-hospital mortality in CAP is more variable, ranging as wide as 4% to 66%23–26 but is generally lower than mortality in patients with ARDS, likely due to its more variable severity when compared to ARDS. More specific to our study's patient population, Toba et al and Sirvent et al also found higher mortality in patients with CAP who developed ARDS versus not,27,28 while Cilloniz et al found no significant differences in mortality or length of hospitalization between patients with CAP who did and did not develop ARDS. 29 In a study of ARDS in patients hospitalized with SARS pneumonia (pre-COVID-19), Chen et al found that mortality was higher in patients who developed ARDS versus not. 30 Our data is therefore consistent with the majority of existing literature that indicates development of ARDS is associated with worse outcomes in pneumonia patients.
In addition to increased mortality and longer time on intensive treatment, patients who developed ARDS after CAP had significantly higher total cost of hospitalization than those who did not. Given that all patients in our study required aggressive treatment, including at least MV and antimicrobial therapy, it is noteworthy that cost of treatment was still much higher in patients with ARDS. To our knowledge, no prior literature has made a similar comparison, but there is data that development of ARDS prolongs ICU stay and hospitalization cost in critically ill trauma patients. 31 The fact that patients with ARDS spent more days in the ICU and on MV likely contributes to the differences in costs.32,33 Additionally, patients with ARDS were more likely to have had early vasopressor initiation during hospitalization. Although we do not have data on differences in total vasopressor use between cohorts, it is plausible that patients with ARDS had greater pressor requirement, which may contribute to differences in cost. Notably, while there is evidence that vasopressor costs are rising, 34 recent literature in septic shock suggests use of vasopressors is a relatively minor contributor to total hospitalization cost. 35 Time spent in the ICU and on MV are likely much more substantial contributors to cost differences.
We found that early vasopressor initiation being associated with increased ARDS risk is most consistent with prior literature. While we do not have data on vasopressor indications in our patients, it is likely that many patients hospitalized with severe CAP had septic shock, 36 and sepsis is the most common risk factor for ARDS. 37 Given the well-documented association between shock and mortality, 38 the higher rate of early vasopressor initiation in the ARDS cohort suggests that a higher incidence of early shock likely contributed to the higher mortality compared to the no ARDS cohort. We also found that arthritis was associated with increased ARDS risk. While there are individual case reports demonstrating development of severe ARDS in patients with arthritis who received tumor necrosing factor (TNF)-targeting therapies,39–41 there is no conclusive evidence that arthritis increases ARDS risk. TNF-α is a known inflammatory mediator in patients with rheumatoid arthritis 42 and may play a role in the development of ARDS,43,44 but we found no studies larger or more comprehensive than the above case reports that associated arthritis, TNF activity, or anti-TNF therapy with ARDS.
Our findings regarding history of congestive heart failure (CHF), renal failure, and chronic pulmonary disease being associated with decreased ARDS risk are also of interest. Chronic pulmonary disease and CHF are risk factors for the development of CAP,45–48 and there is evidence that a history of renal disease is also a risk factor. 45 While there is little data directly examining CHF or renal failure as risk factors for ARDS, chronic obstructive pulmonary disease is prevalent in patients with ARDS, 10 and chronic pulmonary disease is associated with ARDS in patients admitted for trauma and sepsis.49,50 It is unclear why our results demonstrated that comorbidities that are commonly associated with increased CAP risk were associated with lower risk of developing ARDS after CAP. One possible explanation is that these comorbidities confounded diagnosis of ARDS. Exclusion of cardiogenic pulmonary edema is part of the Berlin criteria, 51 and differentiation of ARDS from CHF can be challenging, 52 which may explain why patients with CHF were less likely to be diagnosed with ARDS. As the presence of pulmonary infiltrates on imaging is another component of the Berlin criteria, pulmonary edema from CHF or volume overload in renal failure may confound diagnosis of ARDS. 53 It is also possible that it was more difficult to diagnose ARDS due to pre-existing pulmonary disease, and potentially further complicated by pulmonary infiltrates from CAP in our patients. The literature examining ARDS risk specifically in patients with CAP is limited. Many of the comparative studies examined in this discussion come from literature in ARDS after trauma and sepsis.31,49,50 ARDS has several etiologies, and the factors that may predispose patients with CAP to developing ARDS may differ greatly from other patient populations at high risk for ARDS. While this study describes factors that may affect ARDS risk in patients with CAP, it also highlights the need to further explore factors that impact the development of ARDS in patients hospitalized with CAP.
This study has limitations. First, this was a retrospective study. Second, covariates were based on definitions from the Elixhauser comorbidity index, meaning that for some covariates (eg, arthritis and coagulopathy), we cannot specify the exact nature of the comorbidity that was associated with increased or decreased ARDS risk (eg, rheumatoid vs osteoarthritis, disseminated intravascular coagulation vs antiphospholipid syndrome). Third, some patients were admitted with primary diagnosis of CAP while others were admitted with primary diagnosis of respiratory failure or sepsis with secondary diagnosis of CAP. Based on severity of CAP and overall illness at presentation, patients may have developed ARDS in the setting of multiple factors, not just CAP which was the focus of this study. However, our inclusion criteria ensured that only sick patients requiring mechanical ventilation were included in our analysis, regardless of primary diagnosis. Fourth, although we included only sick patients in our study, we were not able to account for certain parameters of ARDS severity (eg, P/F ratios, PEEP) or CAP severity (eg, real-time laboratory findings, vital signs). However, our models accounted for demographics, comorbidities, and vasopressor use, and all included patients required mechanical ventilation. Fifth, the PHD reflects inpatient data for the pertinent admission, meaning that relevant data on previous antimicrobial therapies, inhaled corticosteroid use, and immunosuppressive therapy (eg, for rheumatoid arthritis) was not available. Sixth, given that ARDS and CAP were identified by diagnosis codes, we were unable to identify the laterality or number of lobes affected in each instance of pneumonia. Seventh, our study did not adjust for use of sedation or prone positioning, as this data was not available in the PHD. Eighth, we acknowledge that ARDS is frequently underrecognized, and that relying on diagnosis codes may have affected our interpretation of clinical outcomes in patients who did or did not develop ARDS after CAP.
In conclusion, in patients hospitalized with CAP, development of ARDS led to higher mortality, longer hospitalization, more days in the ICU, more days on mechanical ventilation, and higher hospitalization cost. Development of ARDS was typically predicted by early vasopressor initiation, arthritis, baseline coagulopathy, and fluid and electrolyte disorders. Meanwhile, older age (≥ 50), male sex, Black race, and history of congestive heart failure, chronic lung disease, renal failure, paralysis, and other neurological conditions were protective against development of ARDS. Further research is needed to evaluate risk factors for ARDS in patients with CAP.
Footnotes
Authors’ Contributions
Study design performed by GK, YA, KR, VK, and TO. Data collection and analysis performed by VK and TO. Literature search and manuscript preparation performed by PP, AP, VK, and TO. The manuscript was reviewed by all authors. This study was conducted by the Critical Care and Perioperative Population Health Research (CAPER) Unit, Department of Anesthesiology, Duke University Medical Center, Durham, North Carolina
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. Informed consent was not sought for the present study because of the retrospective nature of the study involving collection of several data points from deidentified large hospital databases.